
Abstract
Purpose
To define the management of patients undergoing cataract surgery.
Setting
Panel of experts on cataract surgery and members of the Italian Association of Cataract and Refractive Surgery (AICCER) participated in the Delphi study.
Design
A restricted panel of experts defined the statements concerning the topic and identified a larger panel of experts who voted the statements. The statements concerned a series of practical issues concerning the management of patients undergoing cataract surgery.
Methods
An initial web round-table served to develop the statements. The larger panel was constituted by 15 experts which anonymously voted the statements, presented in a web platform, using a 5- point Likert scale. Consensus was defined as at least 80% of agreement.
Results
All participants completed the questionnaire. Globally, the total percentage of agreement of all statements was 90.4%. The total mean score was 4.5. Score 4 and score 5 accounted for the 27% and the 68% of the total votes, respectively.
Conclusions
The participants felt they could largely agree with and approve the statements proposed by the board. In addition, the Delphi study identified some points that are highly shared and endorsed. In particular, a new model approach can be based on a seven-day course using a fixed high-potency corticosteroid combination with a broad-spectrum antibiotic. At the end of this cycle, the patient should be re-evaluated in some way to continue any treatment in the most appropriate and personalized way possible.
Introduction
Cataract is a prevalent disease worldwide. 1 The present surgery procedure, based on phacoemulsification and clear corneal incision, has made cataract surgery the most common elective surgery in the western world.2,3
However, it has to be underlined that the operation results in the development of an inflammatory response, and the surgical wound is potentially at risk of infection until it heals.4–7 As a result, the management of patients undergoing cataract surgery consists of two cornerstones: prevention of ocular infection and inflammation dampening.8–10 Consistently, the guidelines on cataract surgery underscored the relevance of an adequate management of patients.8–11
Nevertheless, there has yet to be a complete consensus on several practical aspects, mainly concerning the duration of antibiotic prophylaxis and anti-inflammatory therapy and the choice of the medications. Consequently, the current behavior of several surgeons is usually based on empiric grounds. 12 In this regard, the Italian Association of Cataract and Refractive Surgery (AICCER) promoted a survey among its members. 13 The aim was to evaluate the current practice in managing patients undergoing cataract surgery through a questionnaire.
The results obtained reflected what was daily practiced in real life. Most ophthalmologists implemented preoperative prophylaxis using various products, including antiseptics, topical antibiotics, NSAIDs, and artificial tears. During the perioperative phase, 60% of participants also used intracameral antibiotics, artificial tears, and corticosteroids, while 40% used topical antibiotics. After surgery, several products were prescribed, even simultaneously. NSAIDs (88%) and fixed antibiotic-corticosteroid combinations (87%) were the most commonly used drugs. These medications were prescribed for at least two weeks by more than 80% of physicians. In addition, almost all participants scheduled the first visit the day after surgery. In contrast, a second visit was scheduled after one week by more than 40% of physicians and after two or more weeks by half of the participants. Accordingly, this survey highlighted a discrete inconstancy among Italian ophthalmologists in managing patients undergoing cataract surgery.
Therefore, based on the results provided by this survey, the AICCER executive board decided to validate, with a Delphi method approach, a series of recommendations able to contribute to improving the management of patients undergoing cataract surgery. The aim of this consensus document is to give guidance on approaches capable to relieve ocular inflammation and prevent infection, limiting the occurrence of adverse events and antimicrobial resistance.
Materials and Methods
Design
This study considered the Delphi method to define a series of statements about managing patients undergoing cataract surgery. Delphi study represents an indirect, anonymous, iterative process (such as repetitive among participants) finalized at achieving consensus among experts on specific topics, mainly concerning patient management and pharmacological therapy. 14 This methodology has various applications in different healthcare research fields, like policy analysis, education, and technology assessment, but it has been proven to be useful to develop consensus statements regarding disease management and pharmacological approaches. 15
The Delphi process used for this study consists of 3 phases: i) the explorative phase: which aims at objective and topic definition, to be evaluated by the scientific board, and the expert panel identification; ii) the analytic phase, which aims at the elaboration of statements, through the gathering of evidence and opinion by the scientific board; and iii) evaluation phase which consisted in an analysis of concordance level from experts’ panel to proposed statements.
A group of 9 experts (six ophthalmologists and one microbiologist) constituted the scientific board, appointed to design and overview the study and identify a panel of expert participants to vote on the statements. Namely, the scientific board selected a panel of 15 eye surgeons, with proven experience in cataract surgery.
The scientific board discussed and approved 18 statements concerning the main topics (rationale, disease management, treatment of patients undergoing cataract surgery) and singled out the literature and personal practice.
Statements were uploaded to a dedicated online platform to be anonymously voted by the panel of 15 experts using a ranking scale such as 5-point Likert scale (1 = strongly disagree; 2 = disagree; 3 = undecided; 4 = agree; 5 = strongly agree). The rankings were summarized and shared with the Scientific board. In our study, we defined an agreement level of 80% for 4 + 5 scores. In light of the results, additional cut-off levels of agreement were explored: regarding score 4 + 5 a stricter agreement level of 90% was considered as well, while the same cut-off levels were evaluated for score 5.
The median of achieved scores was calculated together with the standard deviation (SD) and statistical analysis was performed with R software.
Statements
The statements’ preparation consisted of summarizing evidence provided by the most relevant and updated literature on each item concerning the rationale, disease, and treatment. A non-systematic literature search was performed in databases (PubMed, Scholar) to identify relevant scientific evidence to support statements. The scientific board discussed and approved 18 statements concerning the main topics (rationale, disease, treatment, and a final statement). The selection of evidence to support every single statement was performed on the base of the boards’ experiences and personal practice. Statements are presented in this section together with the evidence in their support.
The statements are reported in detail in the Supplemental material.
Results
All 15 participants completed the vote phase for all statements. Globally, the total percentage of agreement of all statements was 90.4%. On a Likert scale for agreement from 1 to 5 point, the total mean score was 4.5. The score 4 accounted for 27% of votes, while the score 5 accounted the 68% of votes. Detailed statistical findings of the voting process are summarized in Table 1
Summary of scores concerning the 18 statements.
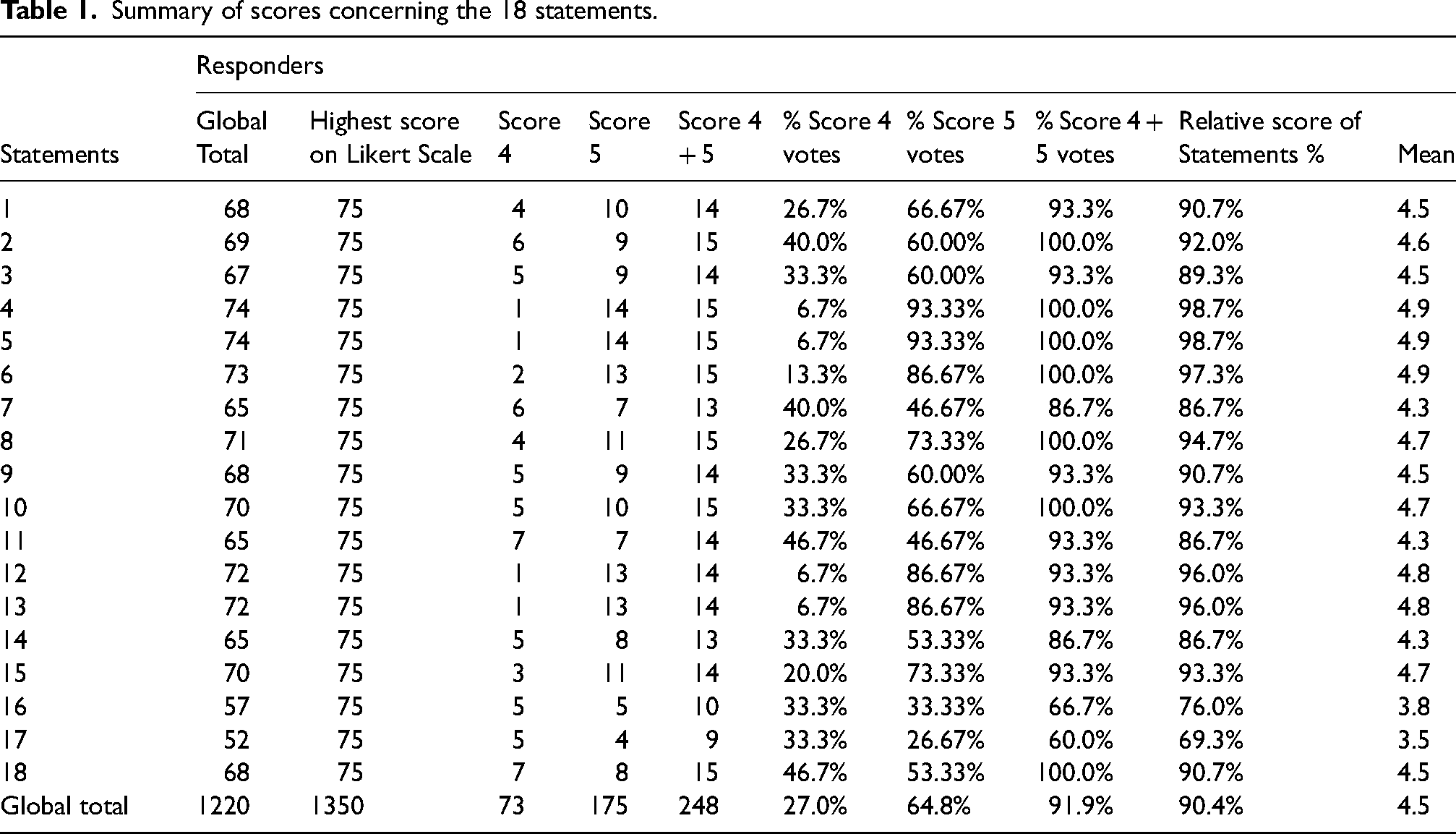
By applying the criteria for the definition of consensus (at least 80% agreement for 4 + 5 scores), 16 of the 18-statements proposed achieved the consensus level. The 2 statements that have not passed the agreement were statements 16 and 17, which achieved 66.7% and 60.0% of consensus respectively. For the statements that reached consensus percentage of concordance was 85–90% for 2 statements, 90–95% for 7 statements and 100% for 7 statements (Statements 2, 4, 5, 6, 8, 10, and 18). Considering the stricter cut-off of ≥ 90% for agreement level of 4 + 5, 14 statements have passed the cut-off.
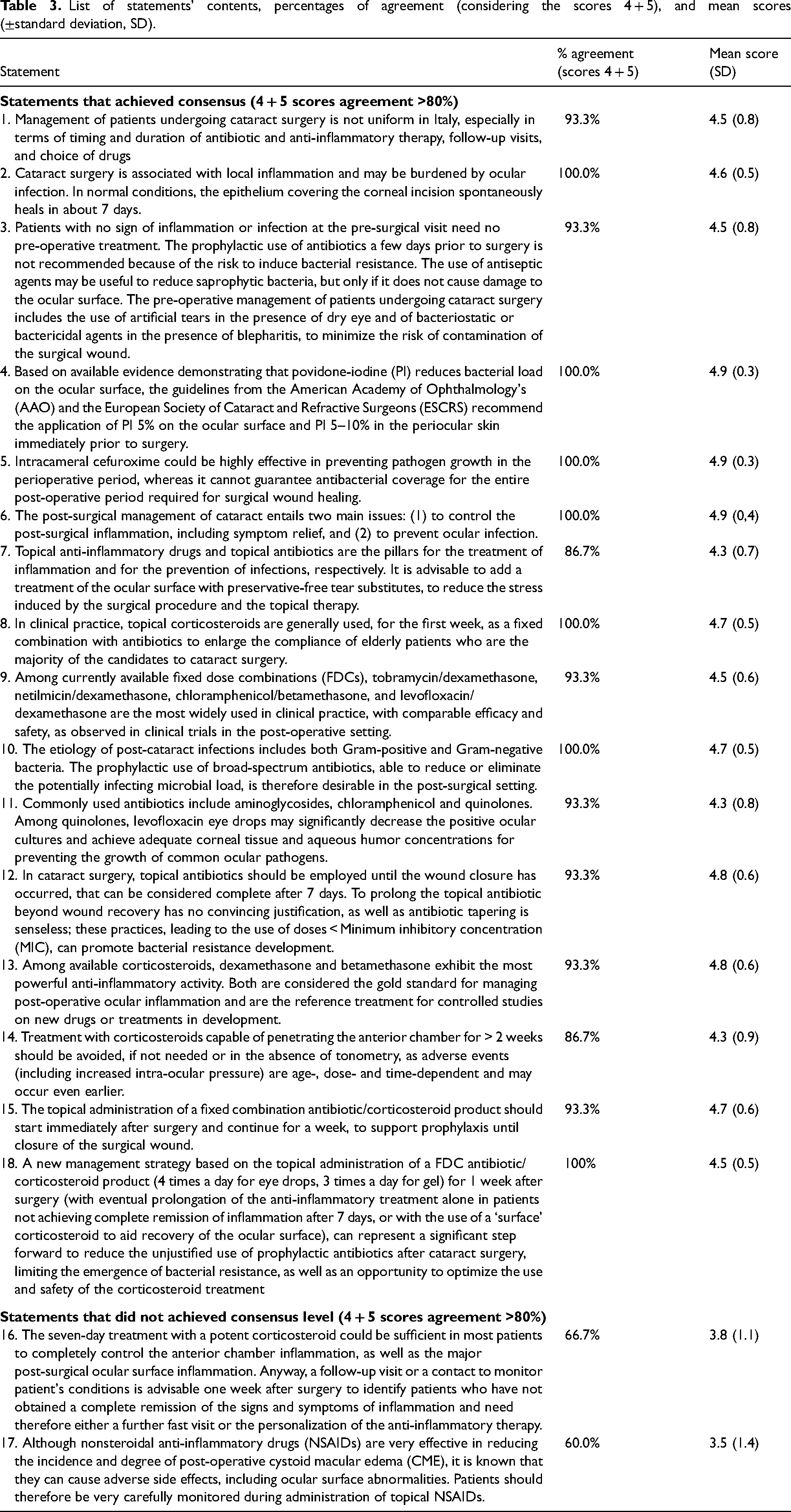
Table 2 shows the 16 statements with a cut-off of > 80% and 14 statements with a cut-off of >90% for 4 + 5 votes. Each single statement, the percentages of agreement considering the scores 4 + 5, and the mean scores are reported in Table 3.
Underlined in yellow statements exceeding the cut-off 4 + 5.

List of statements’ contents, percentages of agreement (considering the scores 4 + 5), and mean scores (±standard deviation, SD).
In the analysis for consensus defined with score of 5, three statements have passed the cut-off threshold of 80%, and two statements have passed the cut-off threshold of 90%.
Discussion
The management of patients undergoing cataract surgery is still uneven across Italy, as recently demonstrated by a survey promoted by AICCER. 13 For this reason, the executive board promoted the present Delphi study to enhance awareness of the importance of following standardized, evidence-based rules of practice.
The results of this Delphi study confirmed a high consensus concerning most of the statements, and in general, the mean score was very high, i.e., 4.5 on a 5-point item scale, as well as the mean percentage of assessment was 90.4%. Therefore, the global consideration of consensus was particularly elevated.
Only two statements (i.e., statement 16 and 17) reported a relatively low consensus grade, even if the percentages of the agreement were 66.7% and 60%, respectively, and 86.7% of participants attributed the vote 5 to these statements.
Statement 1 concerned the variable management across Italy; the consensus was very high, as 93.3% of participants scored 4 or 5 (mean score 4.5). Therefore, there is a shared understanding that this topic is controversial.
Statement 2 stated that cataract surgery is associated with inflammation and risk of infection until the wound has healed. The consensus was very high and was based on convincing literature evidence and personal experience by all participants.
Statement 3 concerned preoperative management. There was a high consensus about the need to use adequate products in selected patients as subjects without signs of inflammation or infection do not require any treatment.
Statement 4 regarded the use of povidone-iodine in 5% aqueous solution on ocular surface or 5–10% on periocular skin, immediately before surgery. The consensus about this statement was very high, as confirmed by 100% of agreement with scores 4 + 5 and a meaningful vote of 4.9. As a result, this procedure is well accepted and routinely practiced.
Statement 5 stated that intracameral cefuroxime is highly effective but for a short time, so infection prevention during the wound healing period is not guaranteed. Again, consensus about this statement was extremely high, as confirmed by 100% agreement with scores 4 + 5 and a meaningful vote of 4.9.
Statement 6 stated that the cornerstone of managing patients undergoing cataract surgery is controlling inflammation and preventing infections. As expected, the agreement on this statement was extremely high.
Statement 7, besides emphasizing the importance of using eye drops with corticosteroids and antibiotics, recommended using artificial tears to reduce surgical damage. The percentage of agreement was relatively high (86.7%). However, it depends on the formulation of the proposition. In fact, the statement encompassed two distinct concepts: on the one hand, the established use of antibiotics and anti-inflammatories, and on the other, the use of artificial tears. This last statement created some perplexity in some participants.
Statement 8 regarded the use of corticosteroids with antibiotics for the first week as a fixed combination to optimize treatment adherence. Consistently, the consensus was remarkably raised as the fixed combination is a widespread and shared practice.
Statement 9 proposed a substantial equivalence among fixed combinations. As a result, the agreement was fairly elevated. However, some participants only partially agreed about this assertion as they believe there is some difference among fixed combinations, mainly concerning efficacy.
Statement 10 advised the use of broad-spectrum antibiotics. Again, the agreement level was particularly elevated, underlined by 100% consensus and a high mean score.
Statement 11 declared the peculiarity of levofloxacin regarding microbicidal activity and adequate, effective concentration in ocular tissues. The agreement was high, even if not all participants expressed complete agreement.
Statement 12 concerned the duration of antibiotic prophylaxis (seven days) and the uselessness and even harmfulness of tapering antibiotic treatment. Again, the consensus was high, as documented by the raised mean score (4.8). In fact, there is widespread awareness that antibiotics, even topically, must be limited to a minimum time. Furthermore, even tapering may favor the emergence of resistant bacteria. Accordingly, this behavior reflects the recommendation of WHO on antibiotic stewardship. 16
Statement 13 underscored the relevance of dexamethasone and betamethasone as gold-standard corticosteroids to dampen ocular inflammation. Again, the consensus was high, as confirmed by the high mean score (4.8).
Statement 14 considered the duration of therapy with high penetrability topical corticosteroids in the routine cases that should not be longer than two weeks in most patients to minimize the risk of adverse events. Again, the consensus was high, with 86.7% of agreement and a mean score of 4.3.
Statement 15 stated that the fixed combination antibiotic/corticosteroid duration should start immediately after surgery and last one week. The consensus level was also high for this statement.
Statement 18 was mainly hinged considering the fixed combination schedule, which should be limited to the first week, eventually followed by a prolongation of anti-inflammatory treatment in low responders, using “surface” corticosteroids. The consensus was particularly elevated as the percentage of agreement (4 + 5) was 100%, and the mean score 4.5.
On the other hand, only two statements did not achieve a valuable consensus level, such as >80% of 4 + 5 scores. Statement 16 proposed two different propositions. The first concerned the proposal of a new seven-day approach using a potent corticosteroid to reduce ocular inflammation quickly. The second declaration proposed a follow-up visit (or at least a contact) at seven days for monitoring the patient's condition. Unfortunately, the agreement was incomplete, as documented by the low mean score (3.8). However, 67% of participants expressed the vote 5. This relatively low acceptance may depend on the double proposition. In particular, a seven-day follow-up visit could be challenging to organize due to the elevated activity performed by cataract units, even if the contact could be performed by telephone or video call, as routinely used in UK.17,18 A reappraisal of organizational procedures certainly requires time and sufficient financial and personnel resources. Nevertheless, a follow-up visit seven days after surgery (also by phone or web) could allow to better personalize the management of patients and could rationalize the use of medications, avoiding adverse events and antibiotic resistance.
Statement 17 concerned the use of NSAIDs to prevent cystoid macular edema; in particular, it highlighted the need to monitor patients treated with this therapeutical option adequately. However, similarly to the previous statement, close monitoring of patients requires a considerable commitment that can only sometimes be fulfilled.
The strength of this study regards the robust approach of the Delphi method to validate a set of statements. Moreover, another point of strength is the panel selected by the AICCER board was particularly experienced in cataract surgery. Finally, the high consensus reached for most of the statements could give well-defined guidance, in particular for the proper pharmacological management of patients that underwent cataract surgery, in each preoperative, perioperative, and post-operative setting, with a particular focus on fixed-dose combination (FDC) management. The limitation of the study could be individuated in the relatively small number of participants and in the national location of the study, although these features corroborate the document as an answer to the Italian state-of-art landscape depicted in the previous survey. 13 Hopefully, the experience here reported on the Italian management of patients that underwent cataract surgery could be inspiring for other countries in order to achieve consistent and evidence-based management of these patients.
Conclusions
The management of patients undergoing cataract surgery is complex and requires thorough expertise. However, there is a need for a broader sharing of standardized procedures based on robust scientific evidence.
This Delphi study garnered a particularly high level of consensus as the average percentage of agreement was 90% and the average vote was 4.5 on a 5-point Likert Scale. Therefore, the participants felt they could largely agree with and approve the statements proposed by the board. In addition, the Delphi study identified some points that are highly shared and endorsed. In particular, a new model approach for post-operative therapy can be based on a seven-day course using a fixed high-potency corticosteroid combination with a broad-spectrum antibiotic. At the end of this cycle, the patient should be re-evaluated in some way to continue any treatment in the most appropriate and individualized manner possible.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231200996 - Supplemental material for Expert consensus on the management of patients undergoing cataract surgery: A Delphi study
Supplemental material, sj-docx-1-ejo-10.1177_11206721231200996 for Expert consensus on the management of patients undergoing cataract surgery: A Delphi study by Vincenzo Orfeo, Pasquale Aragona, Giovanni Alessio, Lorenzo Drago, Leonardo Mastropasqua, Scipione Rossi, Paolo Vinciguerra, Giorgio Ciprandi and Daniele Tognetto in European Journal of Ophthalmology
Footnotes
Acknowledgements
The authors would thank the Content Ed Net agency for the skillful support in organizing the study. The authors also would thank the Study Group on Cataract Surgery Management in Italy; Members: Stefano Gandolfi; Alessandro Franchini; Alessandro Mularoni; Simonetta Morselli; Emilio Pedrotti; Riccardo Sciacca; Vincenzo Scorcia; Marco Tavolato; Lisa Toto; Riccardo Vinciguerra. They participated to the Delphi evaluation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
The study was supported by an unconditioned grant from NTC Italy.
Ethical statement
N/A
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
N/A
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.