
Abstract
Purpose
To describe the role of multimodal imaging in a case of coexisting pachychoroid diseases
Case description
We report a case of a 43 year old lady with coexistent central serous chorioretinopathy (CSC) and pachychoroid neovasculopathy (PNV) in the same eye which posed a diagnostic challenge. Fundus examination showed neurosensory detachment (NSD) at the macula along with retinal pigment epithelial alterations. Optical coherence tomography (OCT) showed a shallow pigment epithelial detachment and OCT angiography showed the presence of vascular network in outer retina choriocapillaris slab suggesting a diagnosis of PNV. However, fundus fluorescein angiography (FFA) showed a smoke stack leak adjacent to the site of vascular network. Focal laser photocoagulation of the leaky point resulted in resolution of NSD pointing towards a diagnosis of CSC.
Conclusion
This case emphasises the role of multimodal imaging in identifying the source of leak in coexistent pachychoroid spectrum diseases.
Keywords
Introduction
Pachychoroid spectrum diseases includes pachychoroid pigment epitheliopathy (PPE), central serous chorioretinopathy (CSC), pachychoroid neovasculopathy (PNV), focal choroidal excavation (FCE), polypoidal choroidal vasculopathy (PCV) and peripapillary pachychoroid syndrome. 1 These conditions are believed to represent different manifestations of a common pathogenic process, as overlapping features have been observed, and progression from one to another has been described. 2 Here we present a case of coexisting PNV and CSC in the same eye identified by multimodal imaging.
Case report
A 43 years old female presented with gradual progressive diminution of vision in the right eye for 4 months. She was healthy with no systemic illness and no history of corticosteroid usage in the past. Her best corrected visual acuity (BCVA) in the right eye was 6/12 and in the left eye was 6/6. Intraocular pressure was 20 mm of Hg and 14 mm of Hg in the left eye. The anterior segment examination was within normal limits in both the eyes. On fundus examination, retinal pigment epithelial abnormalities and subretinal fluid was noted at the macula in the right eye (Figure 1(a)). Swept source optical coherence tomography (OCT) using DRI OCT Triton plus showed subretinal fluid (SRF) along with a shallow irregular hyperreflective pigment epithelial detachment (PED). Beneath the PED, the choroid was thick (397microns) with pachyvessels and attenuated choriocapillaris (Figure 1(b)). OCT angiography (OCTA) using DRI OCT Triton plus revealed a vascular network at the sub RPE level (Figure 1(c) and (d)). The diagnosis of PNV was considered. However, considering the possibility of inactive neovascular network, fundus fluorescein angiography (FFA) was performed. It revealed a focal hyperfluorescence in early venous phase (Figure 2(a)) which increased in size and intensity in a smoke stack pattern typical of acute CSC (Figure 2(b) and (c)). The leak was 606 microns away from the centre of foveal avascular zone. The area corresponding to the vascular network detected on OCTA was seen as an area of stippled hyperfluorescence on FFA with no leak. Fundus autofluorescence showed few smaller areas of hypoautofluorescence and a larger area of hyper-autofluorescence corresponding to SRF (Figure 2(d)). FFA of the left eye revealed an area of stippled hyperfluorescence which increased in intensity in the late phase with no increase in size. A diagnosis of coexistent acute CSC and inactive PNV was considered in the right eye. Focal laser was performed using the 532 nm double frequency Nd: YAG laser over the site of leak (Spot size: 50 microns; Power: 50 mW; duration: 100 milliseconds; number of spots- 3). At 1 month follow up, SRF resolved completely (Figure 3). Best corrected visual acuity in the right eye improved to 6/9.
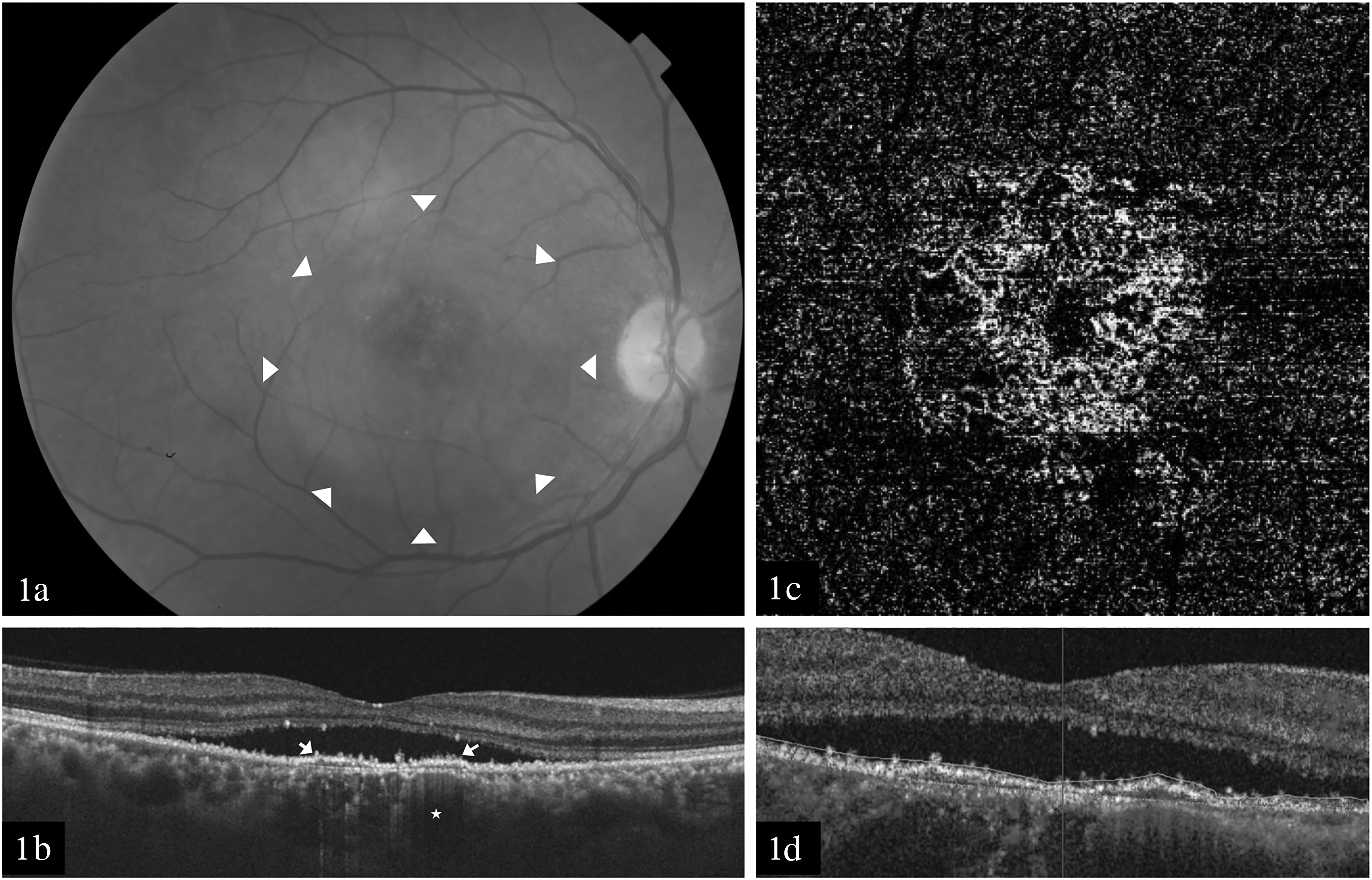
At presentation. (a) Colour fundus photograph of the right eye depicting retinal pigment epithelial abnormalities and subretinal fluid at the macula (arrow heads). (b) OCT image showing the presence of subretinal fluid along with a shallow irregular hyperreflective PED (arrows). The choroid beneath the PED is thicker with dilated Haller's layer vessels (arrow) and loss of choriocapillaris. (c) En face OCTA image showing the vascular network in outer retina choriocapillaris slab.1D: Cross sectional OCTA image through the lesion showing the presence of a flow signal within the PED (arrow).
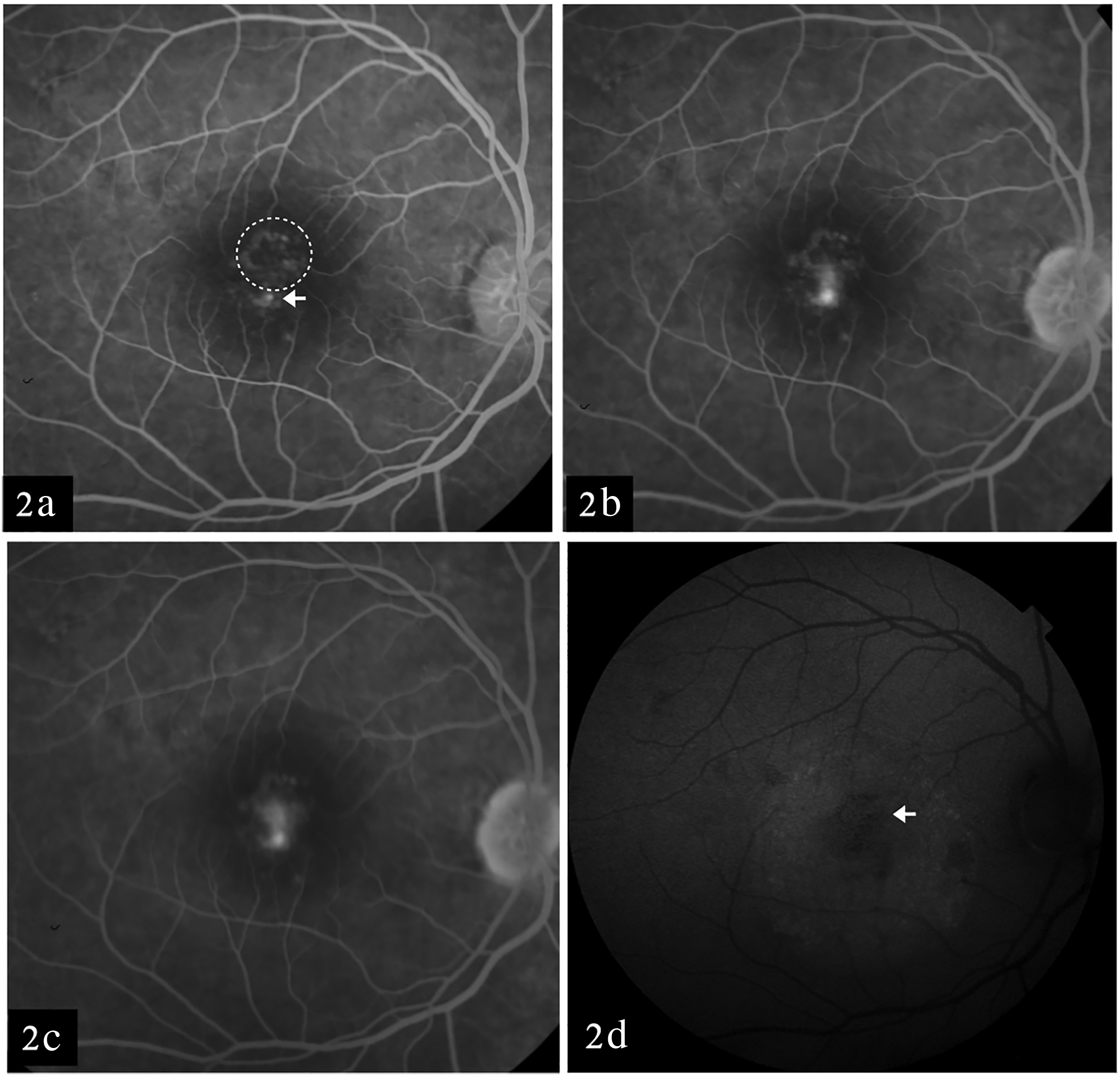
Early venous phase showing stippled fluorescence (dotted circle) with a spot of hyper fluorescence (arrow). (b) The spot of hyper fluorescence increases in size and intensity in late venous phase. (c) Smoke stack appearance of the leak in the late phase. (d) Fundus autofluorescence of right eye showing few smaller areas of hypoautofluorescence corresponding to PED (arrow) and a larger area of hyper-autofluorescence corresponding to SRF.
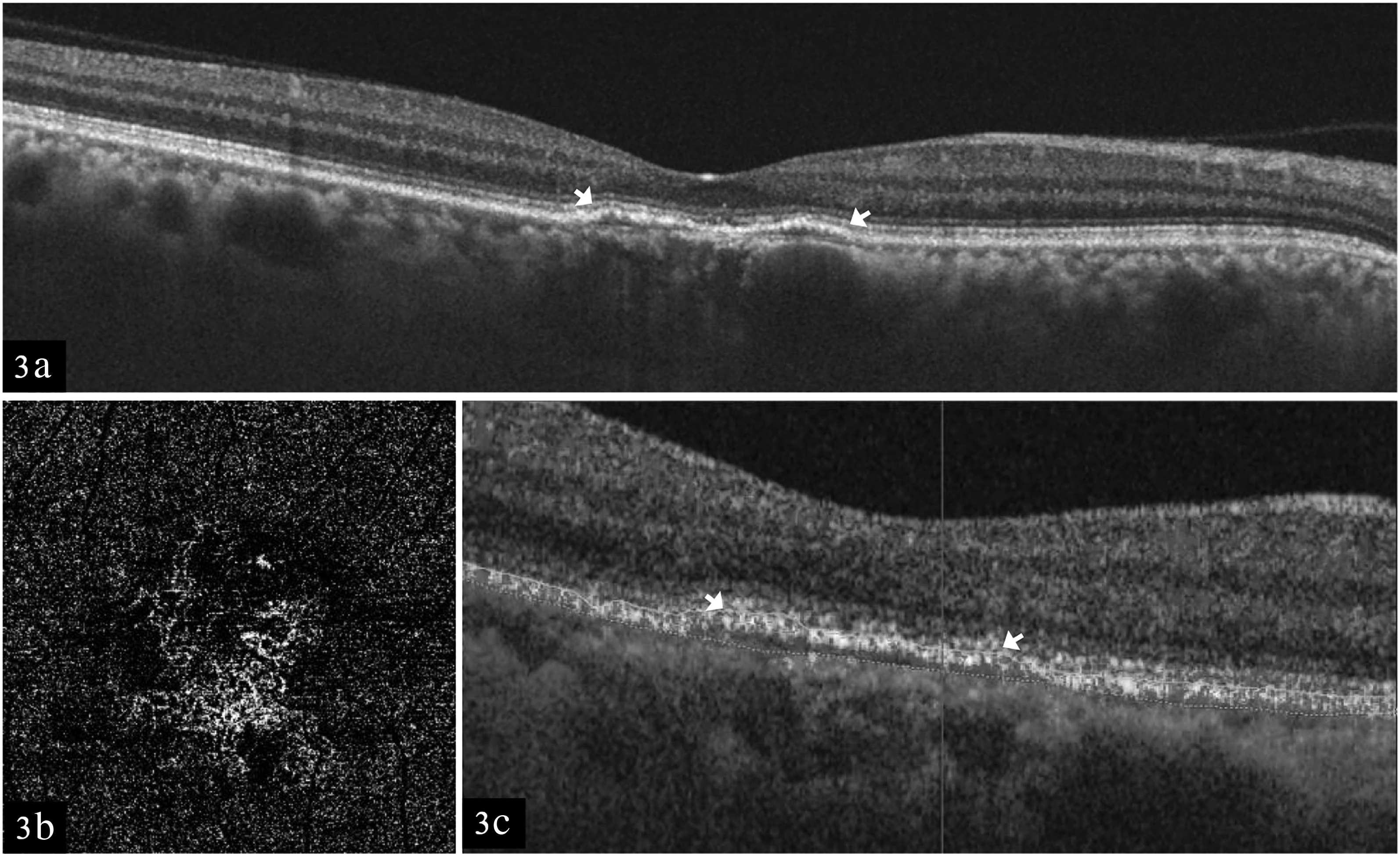
At 1 month follow up. (a) OCT scan showing the resolution of fluid with persistence of PED (arrows). (b) En face OCTA image showing the persistence of the vascular network. (c) Cross sectional OCTA image showing the flow signal within the PED (arrows).
Discussion
The concept of pachychoroid disease has largely come forward due to advances in imaging techniques. The described clinical phenotype however is different for each disease within the pachychoroid spectrum, but with noticeable overlaps. PNV and CSC are considered to be distinct clinical entities within the pachychoroid spectrum. A diagnosis of PNV is considered in cases with the presence of type 1 CNV in absence of chronic CSC. 3 However, CNV is known to be a late complication of chronic CSC. In the pre-OCT era, classic or predominantly classic CNV which corresponds to type 2 CNV were described on FFA in cases with chronic CSC. 4 Nevertheless, OCT and OCTA based studies have noted higher incidence of type 1 secondary CNV in patients initially diagnosed as CSC. 4
In our case, OCT showed SRF and type 1 CNV. Though the initial diagnosis was PNV owing to the presence of type 1 CNV and focal areas of thickened choroid with dilated choroidal vessels beneath the CNV, FFA confirmed the diagnosis of acute CSC based on the typical smoke stack leak. Absence of leak from the area corresponding to type 1 CNV indicated that the CNV was quiescent. Focal laser therapy was considered based on the FFA which resulted in complete resolution of SRF. We considered this as first episode of acute CSC based on the absence of descending tracts and FAF abnormalities outside the area of SRF. As discussed earlier, secondary CNV is a known complication of CSC. However, coexistence of acute CSC and PNV is not reported. Both acute CSC and PNV are considered as distinct clinical entities of the pachychoroid spectrum. Pachychoroid is implicated to have effect on overlying RPE. This can lead to leak and accumulation of fluid as in CSC or can also lead to development of CNV. However the exact mechanism is not well established. Advances in OCT and OCTA enables the detection of quiescent CNV, which would have been missed in the pre- OCTA era. The use of FFA is declining due to availability of OCTA. Nonetheless this case emphasises the role of FFA in identifying the source of leak in coexistent pachychoroid spectrum diseases and aids in proper diagnosis and treatment.
Supplemental Material
sj-tiff-1-ejo-10.1177_11206721231187423 - Supplemental material for Role of multimodal imaging in coexistent pachychoroid spectrum disease
Supplemental material, sj-tiff-1-ejo-10.1177_11206721231187423 for Role of multimodal imaging in coexistent pachychoroid spectrum disease by Shubhra Sweta, Pradeep Sagar, Suchitra Biswal, Ravishankar HN and Parvathy PS in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical committee approval
Institute ethics committee approval was obtained in November 2022. Written informed consent was obtained from the patient.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.