
Abstract
Age-related macular degeneration (AMD) is one of the leading causes of vision loss and blindness in older adults. Given the aging population in developed countries and the increased participation of older adults in the labour market, this paper aims to understand the impact of AMD on workplace productivity. Economic studies, comparative studies, observational studies, cohort studies, case series, randomized control trials, clinical trials, multicenter studies from MEDLINE, EMBASE, and CINHAL, as well as grey literature, were systematically searched to obtain all relevant literature. Duplicate records were removed, and two independent reviewers screened records for relevance. After screening, a risk of bias assessment was carried out. Data were extracted and a meta-analysis was performed using STATA 15.0. Fixed-effect and random-effect models were computed based on heterogeneity. Seven studies consisting of 3,060,864 subjects from 5 different countries were included in this systematic review. Mean wages lost due to impaired work productivity ranged from $1,395 to $55,180. The mean unemployment rate attributed to AMD ranged from 5.50% to 77.00%. Meta-analysis results indicated a significant unemployment rate (SMD = 0.44, CI: [0.27, 0.62]). Patients with AMD experience impaired work productivity as demonstrated by the wages lost and significantly higher rates of unemployment.
Keywords
Introduction
Age-related macular degeneration (AMD) is a chronic degenerative disorder of the retina that gradually leads to central vision loss. Among older adults, late-stage AMD is a significant cause of permanent vision loss and blindness, globally. 1 The estimated worldwide prevalence of late-stage AMD is approximately 0.37%. 2 Unfortunately, the prognosis for AMD is poor, with rapid progression towards legal blindness (defined as visual acuity worse than 20/200) within three months of diagnosis, and 77.6% of patients becoming legal blindness within three years. 3 It is projected that the number of individuals with late-stage AMD will increase by 86% from 2014 to 2040, with a total of 9.92 million cases worldwide. 2
Understanding the effects of AMD on both patients and society is essential. While the impact on visual function has been extensively studied, the consequences of AMD-related vision loss and blindness extend beyond just vision issues.4–7 Previous research has indicated that individuals with AMD experience a significant decline in their quality of life, increased utilization of healthcare resources, and incur greater economic costs in comparison to matched controls.8,9
Effective treatment for neovascular AMD (nAMD) requires regular anti-VEGF injections and frequent clinic visits for fundus examination and optical coherence tomography. Patients typically spend an average of 12 h per visit, with 22% requiring a caregiver to take time off from work for transportation. 10 The indirect costs of AMD, such as loss of work productivity for the patient and caregivers, as well as decreased productivity due to premature mortality and time away from work, must also be taken into consideration. 11
It is important to understand the relationship between work productivity in patients with AMD and its effects on presenteeism (lost productivity that occurs when employees are not fully functioning in the workplace because of an illness, injury, or other condition) and absenteeism (habitual absence from work). At present, a comprehensive summary of all the primary research related to the indirect costs of AMD, especially its impact on work productivity is limited. Therefore, we aim to conduct a systematic review and meta-analysis, to characterize the relationship between AMD and workplace functioning as well as its associated economic burden.
Methods
Search strategy
This systematic review protocol adheres to the guidelines outlined in Appendix A of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). MEDLINE, EMBASE, and CINAHL databases were comprehensively searched from their inception until January 27th, 2022 to identify eligible studies. The search strategy used is described in detail in Appendix B. In addition, grey literature searches were also conducted, which included ClinicalTrials.gov, ProQuest Dissertations and Theses Global (ProQuest). Relevant poster presentations and abstracts from conferences of The Association for Research in Vision and Ophthalmology, American Academy of Ophthalmology, and Canadian Ophthalmological Society were manually searched to identify any relevant information. Further details on grey literature searches can be found in Appendix B.
Inclusion criteria
Studies were included if they were focused on human subjects who were adults 18 years and older with AMD. There was no distinction made between dry AMD and wet AMD. The association between diagnosis and treatment of AMD and workplace productivity was evaluated using outcome measures such as unemployment rate, lost wages lost due to reduced salaries or missed work, and total wage lost. Included articles encompassed a variety of study types, such as cohort studies, case series, economic studies, comparative studies, observational studies, randomized control trials, clinical trials, and multicenter studies.
Exclusion criteria
We excluded certain types of articles such as review articles, case reports, systematic reviews and meta-analyses, letters to editors, and commentaries. Conference abstracts were included if they had sufficient study details and data. The review only included articles in English as translations of non-English articles may have caused inconsistencies. There were no restrictions on the publication year or location of the studies.
Study selection
The process of compiling the relevant literature involved a multi-step screening process. The database search results were imported into Covidence, which also conducted an automatic duplicate check. The first level of screening involved a review of the titles, the second level involved a review of the abstracts, and the third level involved a full-text review of the articles.
Two reviewers, E.T and M.N, independently assessed the articles at each level of screening, and any conflicts were resolved through discussion or mediation by a third reviewer if necessary. The percentage agreement between the two reviewers was calculated using Cohen's kappa coefficient, and a PRISMA flowchart (Figure 1) was created to display the number of studies included and excluded at each step of the screening process.
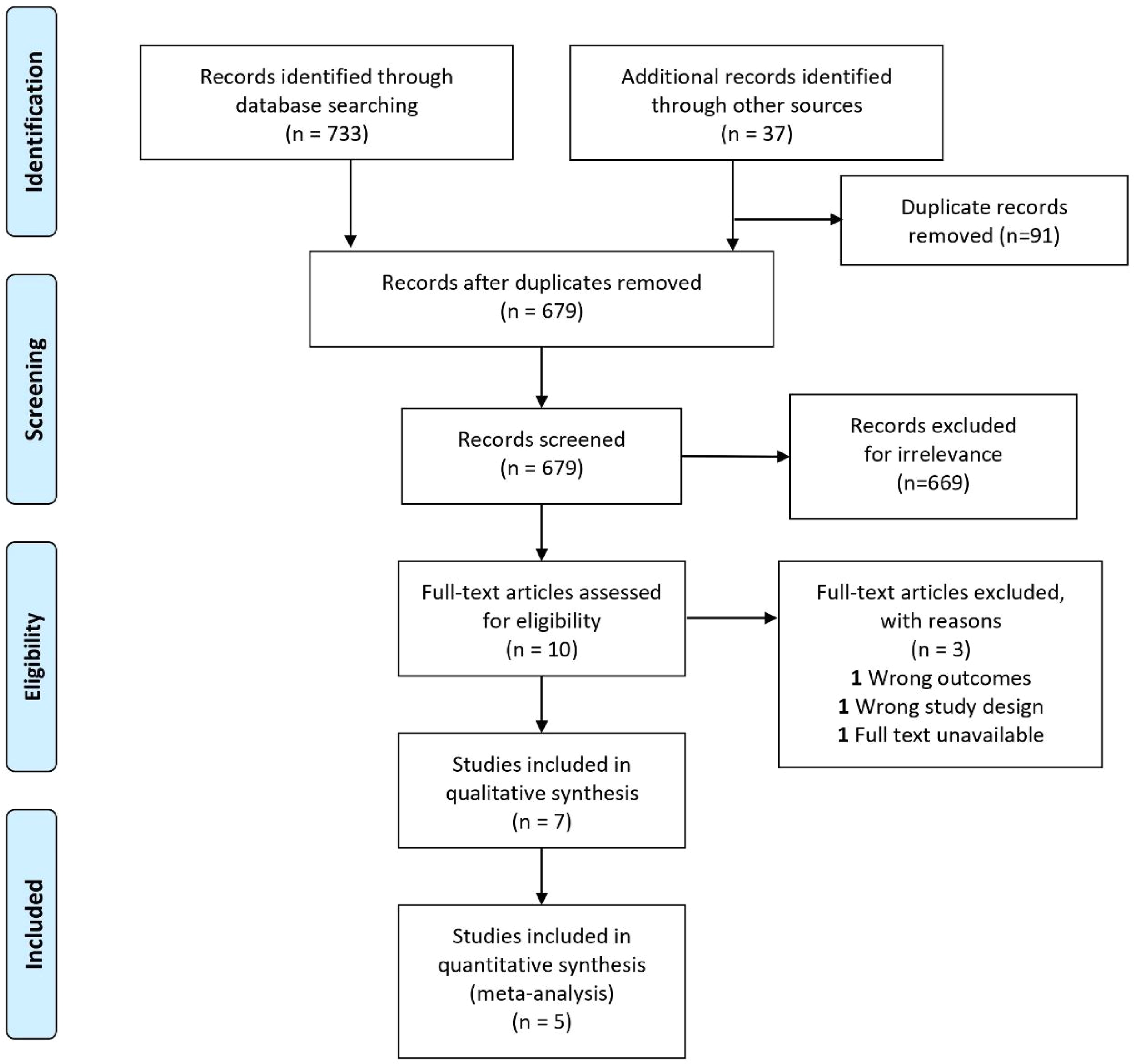
PRISMA flowchart for study identification and selection. The PRISMA flow diagram for the systematic review detailing the database searches, the number of abstracts screened and full-text articles reviewed for study eligibility, and reasons for exclusion.
Only articles that evaluated a minimum of 20 adult eyes and presented outcomes related to impaired work productivity, such as unemployment rate, lost wages, reduced salaries or missed work, and total wage loss were included in the full-text screening.
Risk of bias assessment
The modified Downs and Black checklist was used to assess the risk of bias in the studies. 12 Studies that scored over 20 were considered high quality, those with scores between 16 and 19 were considered medium quality, and those with scores below 15 were considered poor quality. The methodology was thoroughly checked for completeness. Due to limited evidence, none of the studies with lower quality were excluded from the analysis. The risk of bias assessment is described in detail in Appendix C.
Data collection process
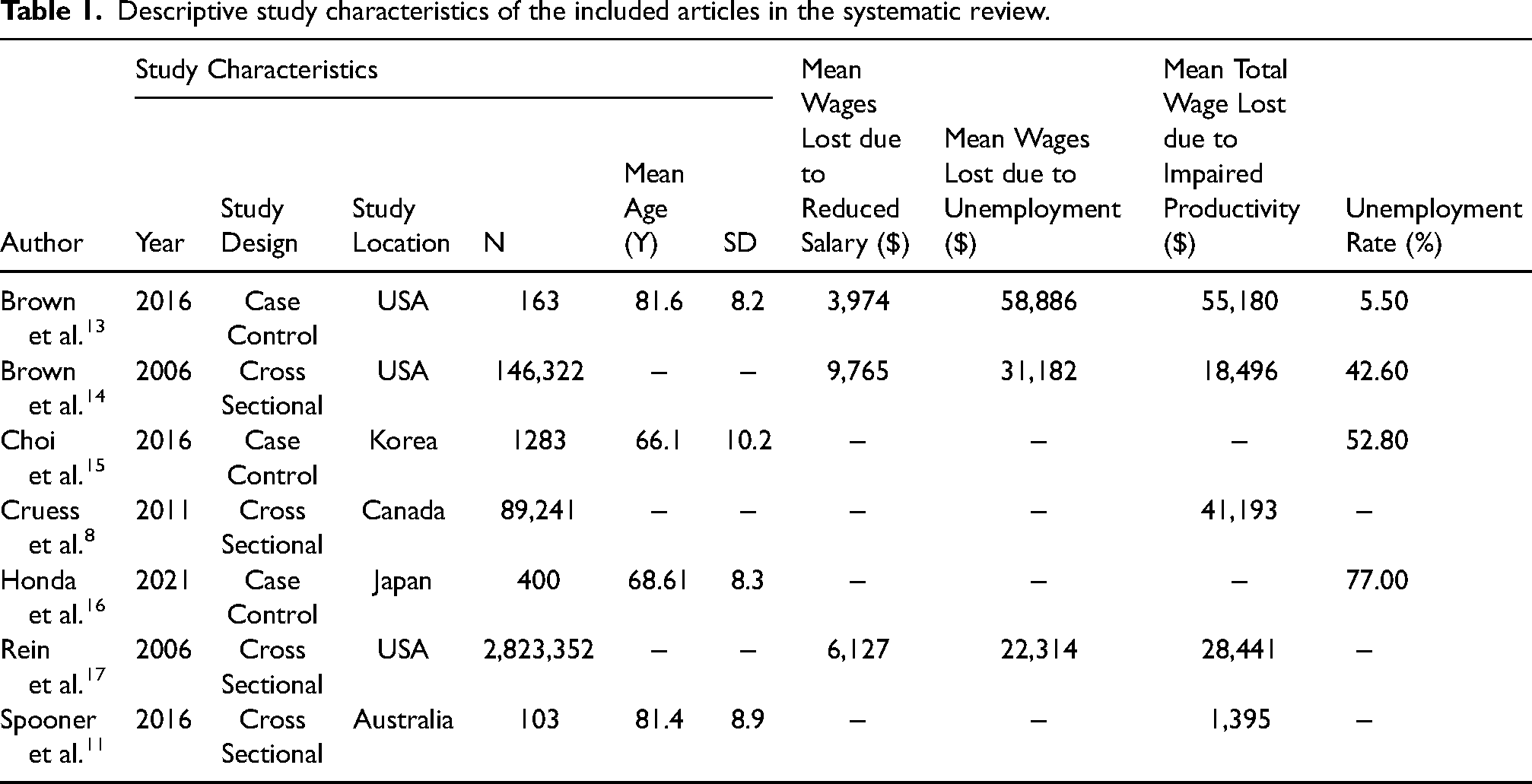
After the quality-check process, the study characteristics of 7 articles were extracted (Table 1). This included author, year of publication, study design, study location, sample size, mean lost wages due to reduced salary, unemployment rate, mean lost wages due to unemployment, and mean total productivity loss. A total of 4 articles were used for quantitative synthesis and 3 for qualitative analysis.
Descriptive study characteristics of the included articles in the systematic review.
Statistical analysis
To conduct the meta-analysis, STATA 15.0 software from STATA Corporation in College Station, TX was used. The effect size, or treatment effect, was determined by the proportion, while the treatment effect was the unemployment rate among patients with AMD. To assess heterogeneity, the I2 value was employed to determine the degree of variation between studies due to heterogeneity rather than chance. Heterogeneity between studies was assessed using a chi-squared test to determine whether observed between-study differences were solely due to chance. Evidence of heterogeneity was indicated by a low p-value and a large chi-squared statistic relative to its degree of freedom. Based on heterogeneity, either fixed-effect or random-effects models were developed, and forest plots were generated. Funnel plots were also generated to evaluate publication bias.
Results
Search results
A total of 679 results were obtained from online databases and grey literature sources, with 91 duplicates identified and removed. Subsequent screening of titles and abstracts led to the exclusion of 669 articles, leaving 10 studies for full-text screening. Out of the 10 studies, 7 were eligible for data extraction, while the remaining 3 provided data using different measures that were not comparable to the other papers. Quantitative synthesis was performed on 4 studies, while the excluded studies were either deemed irrelevant or failed to progress past the screening stages. The Cohen's kappa coefficient for abstract and title screening and full-text screening were 23% and 78%, respectively.
Study characteristics
Out of the 7 studies that proceeded to the data extraction stage, the majority (n = 4) were cross-sectional studies, while the rest (n = 3) were case-control studies. The studies were conducted globally, with a particular emphasis on the United States of America. Most of the studies had large sample sizes, ranging from 103 to 2,823,352 participants,11,18 although not all studies reported the mean age of their subjects. However, the available data indicated that most participants were elderly, with a mean age ranging from 66.1 to 81.6 years.14,19 Mean wages lost due to a reduced salary (demotion at work, poor performance, lack of skills, fewer responsibilities, less time spent at work) ranged from $3,974 USD to $9,765 USD a year.14,20 Mean wages lost due to unemployment ranged from $22,314 USD to $58,886 USD a year.14,18 Mean unemployment rate attributed to AMD ranged from 5.50% to 77.00%.14,17
Publication bias
In Figure 2, the funnel plots for the unemployment rate among AMD patients are depicted. The studies are dispersed from the top left to the bottom right of the plot. The funnel plot contains fewer studies towards the bottom of the plot, indicating that small studies with non-significant results may not have been published. A visual assessment of the funnel plot does not show any evidence of asymmetry.
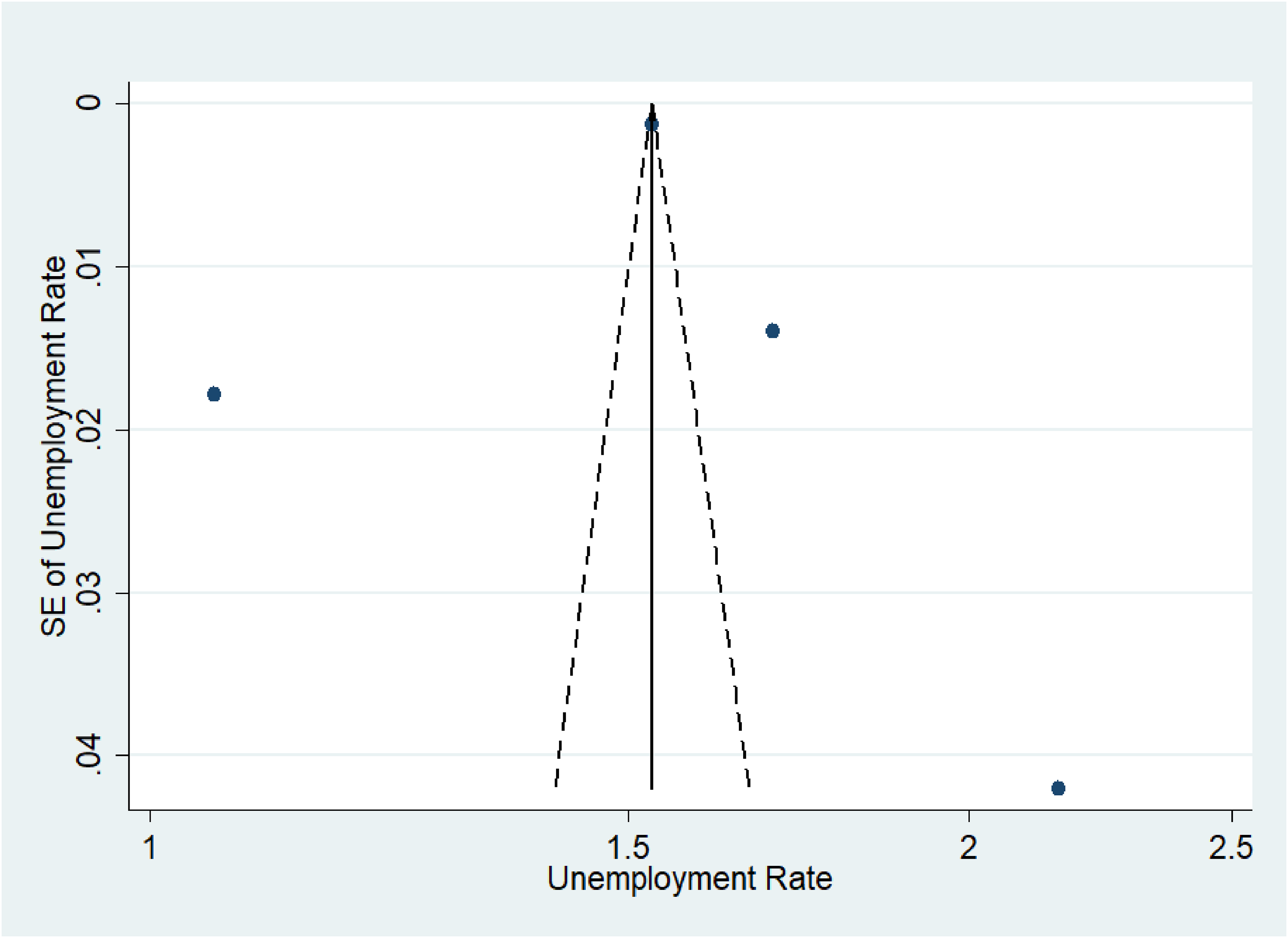
Funnel plot for included studies for the unemployment rate of AMD patients.
Impact on employment
Figure 3 summarizes the results for the unemployment rate of AMD patients. Four studies (172,996 subjects) considered the impact of AMD on the employment rate of the patients. All the studies showed a significant increase in the unemployment rate. However, there was significant heterogeneity (I2 = 99.5%, p = 0.0) observed among the studies that investigated the impact of unemployment. A significant increase in unemployment rate (SMD = 0.44, CI: [0.27, 0.62]) was detected among AMD patients. It should be noted that only four studies evaluated the impact of work productivity in AMD patients, indicating that further research is required to draw more definitive conclusions.
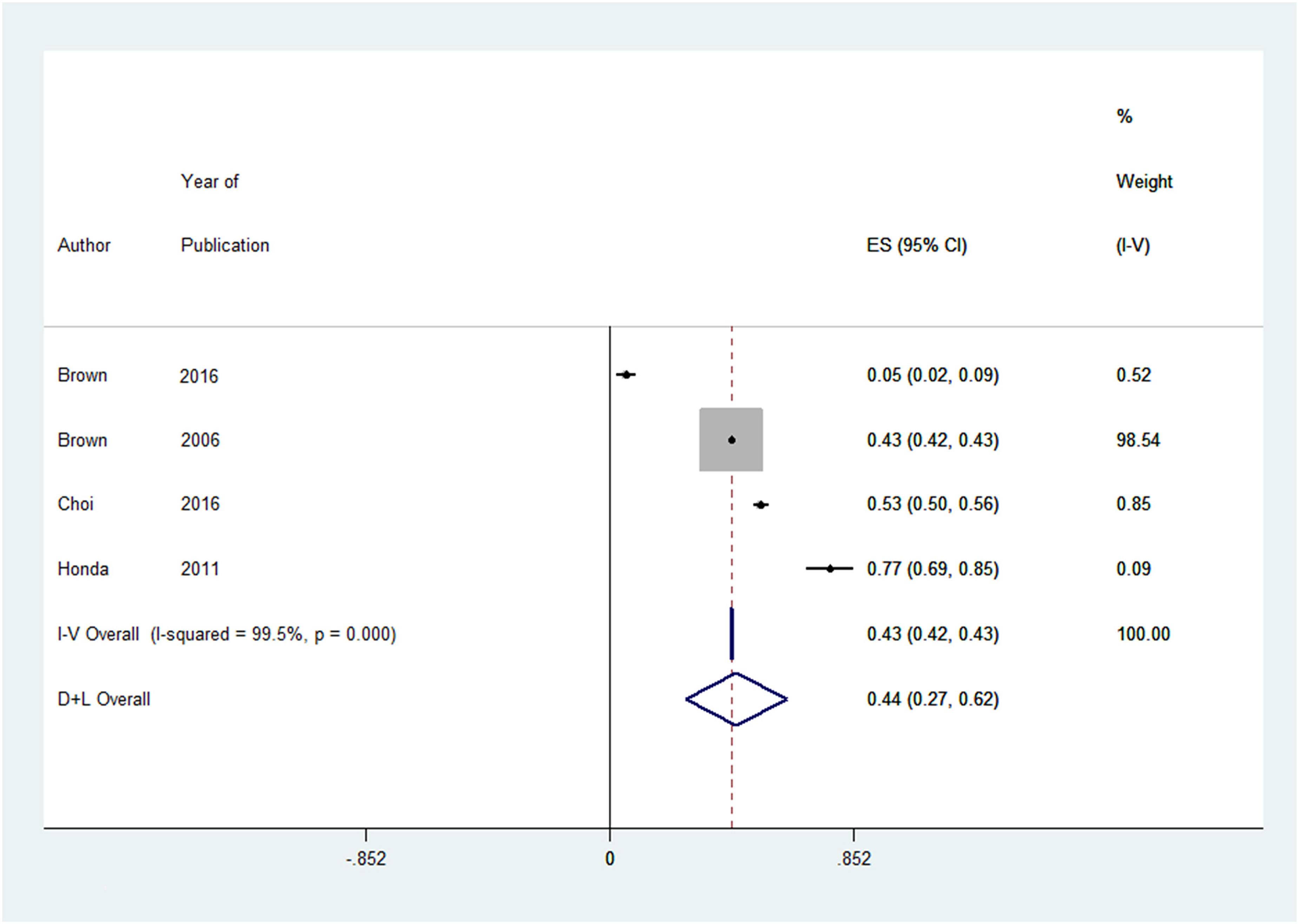
Forest plot analyses describing the association between age-related macular degeneration and unemployment included studies for the unemployment rate of AMD patients.
Discussion
The aging population in developed countries has led to an increase in labour market participation of older adults. 21 With AMD being one of the leading causes of legal blindness in the older populations in the world today, 22 it is crucial to understand how decreased visual acuity and quality of life caused by AMD directly relates to decreased work productivity and unemployment. However, it has been shown that physicians often underestimate the effects of AMD on productivity, income, and unemployment. 11
Mean ages ranged from 66.1 to 81.6 years14,19 which accurately reflects the population affected by AMD and indicates that the majority of individuals are around retirement age. Despite that, the shift in the increase in the participation of older adults in the labour market demonstrates that older adults still have a desire to work. Figure 3 shows that individuals with AMD are unable to work which is seen by the significantly higher unemployment rate. The total mean wages lost due to impaired productivity, either due to presenteeism or absenteeism ranged from $1,395 to $55,18011,14 which demonstrates the financial burden of AMD on individuals.
Disability leading to unemployment and impairments in work productivity have adverse consequences not only on an individual's personal finances but also on the global economy. Gross Domestic Product (GDP) can be calculated by adding the income of wages, rent, interest, and profits of all contributors to the production of goods and services within a country over a yearly period. 23 Studies predict that due to the economic burden of AMD, loss of wages and unemployment caused by the condition will consequently result in a decrease in GDP.8,14,18,20,24 It is essential to acknowledge that treating patients with AMD not only enhances their quality of life, but also contributes to the overall economic well-being of the country. This highlights the importance of maintaining a healthy and productive workforce to sustain the economy.
Individuals with visual impairment caused by AMD face significant challenges in securing employment, which is evidenced by the increased rate of unemployment.13,17,19 The financial burden of AMD is further exacerbated by additional expenses such as transportation costs, costs for caregivers, and healthcare costs.11,20
Patients with AMD often experience a decline in central vision while retaining peripheral vision. The loss of central vision caused by AMD significantly hinders an individual's ability to carry out tasks such as reading, writing, driving, using digital devices, and recognizing faces.4,5,15,16 This would impair an individual's ability to perform their job effectively and efficiently, leading to presenteeism, and lost productivity that occurs when employees are not fully functioning in the workplace because of an illness, injury, or other condition. Older adults with AMD and increased visual impairment have a higher incidence of falls and injuries, such as cuts, burns, or lifting injuries, compared to those with reduced visual acuity of the same age. 25 These issues could lead to absenteeism or habitual absence from work, and subsequent loss of work productivity.
Early detection and prompt treatment of AMD are crucial to maintain visual acuity and work productivity. Anti-VEGF injections for nAMD may have implications on work productivity, as demonstrated by studies conducted in the USA, Europe, and Japan. These studies showed that patients with nAMD visited their ophthalmologists more frequently compared to matched controls. 26 Another study also demonstrated increased absenteeism, meaning patients were more likely to be habitually absent from work, and increased presenteeism, meaning patients were less productive at work due to either their medical condition or medical treatment. 19 A different study observed the same association between higher frequency of visits to ophthalmologists and greater levels of absenteeism and presenteeism. 17 Frequent visits to the ophthalmologist can be a major inconvenience and cause time away from work, leading to increased absenteeism. Conversely, anti-VEGF injections can be associated with complications such as floaters, irritation and pain which can impair vision and make it difficult for individuals to complete their tasks at work effectively, leading to increased presenteeism. This implies that a higher number of appointments with an ophthalmologist can lead to increased levels of absenteeism and presenteeism, thereby negatively impacting the work productivity of nAMD patients. 17
The “Treat and Extend” regimen (TER) has received support from various studies and meta-analysis, as it has been shown to reduce the frequency of appointments, which can have a significant time burden for patients. It can also decrease the cost of appointments without negatively affecting visual function.27,28 A study by Gupta et al. found that the average direct costs for patients receiving intravitreal ranibizumab using TER were lower compared to those receiving monthly injections over a one-year period. 29
It is important to take into account the limitations of the study before drawing any conclusions. The quality of the selected studies varied greatly, and there was significant variation in their scores based on the modified Downs and Black checklist. Despite this, all studies were included due to the limited amount of evidence. The screening process excluded studies that were not available in English, as the screeners were only proficient in this language. This did not limit the location of the studies, so studies from around the world were included in the systematic review. However, conducting a meta-analysis of observational studies can be influenced by biases in the articles, such as other factors like education level, ethnicity, income, pre-existing health conditions, and medications.
The study also has some limitations to consider before drawing conclusions. One of the limitations was the inconsistency between the studies that analyzed the relationship between AMD and work productivity. The studies did not differentiate between wet and dry AMD, the degree of visual acuity loss, or whether the patients received treatment such as intravitreal injections or no treatment. To have a better understanding of the impact of AMD on work productivity, future studies could specifically examine measures like presenteeism and absenteeism. Another area of exploration could be to investigate if reducing the frequency of visits to the ophthalmologist and intravitreal injections through the “Treat and Extend” Protocol results in reduced wage loss and improved work productivity, without compromising efficacy and safety.
In conclusion, AMD negatively affects a patient's work productivity, causing decreased wages, and significantly higher rates of unemployment. With regards to future healthcare planning, it is important to be conscientious of how AMD can impair a patient's work productivity and the entailing economic consequences, especially considering the aging population, and shifting labour market.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231185808 - Supplemental material for The effects of age-related macular degeneration on work productivity: A meta-analysis
Supplemental material, sj-docx-1-ejo-10.1177_11206721231185808 for The effects of age-related macular degeneration on work productivity: A meta-analysis by Edward Tran, Manav Nayeni, Nirmit Shah and Monali S Malvankar-Mehta in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721231185808 - Supplemental material for The effects of age-related macular degeneration on work productivity: A meta-analysis
Supplemental material, sj-docx-2-ejo-10.1177_11206721231185808 for The effects of age-related macular degeneration on work productivity: A meta-analysis by Edward Tran, Manav Nayeni, Nirmit Shah and Monali S Malvankar-Mehta in European Journal of Ophthalmology
Supplemental Material
sj-docx-3-ejo-10.1177_11206721231185808 - Supplemental material for The effects of age-related macular degeneration on work productivity: A meta-analysis
Supplemental material, sj-docx-3-ejo-10.1177_11206721231185808 for The effects of age-related macular degeneration on work productivity: A meta-analysis by Edward Tran, Manav Nayeni, Nirmit Shah and Monali S Malvankar-Mehta in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.