
Abstract
Introduction
Tuberculosis can involve any organ in the body including ocular tissue of which the uveal tissue is most commonly infected. Choroidal involvement ranges from choroidal tubercles to granulomas. This is one of the few cases of a solitary choroidal granuloma with no other systemic symptoms in an immunocompetent child.
Method
A case report.
Results
A 12-year-old female, presented with diminution of vision in the left eye for a month. The anterior segment of her left eye was normal. A fundus examination revealed an isolated orangish-yellow choroidal mass, 4 DD in size, involving the posterior pole with overlying subretinal exudation. CT scan of the thorax showed large pulmonary, cervical and pancreatic lymph nodes, along with lytic lesions of the thoracic vertebrae. Excision biopsy of the cervical lymph nodes showed caseating granulomas with no e/o malignancies on histopathology. The patient was started on anti-tubercular therapy. Six months after the treatment, the lesion had reduced in size and her vision had improved.
Conclusion
Isolated choroidal tuberculomas can be present in eyes with little associated ocular inflammation and no other symptoms of systemic tuberculosis. High suspicion, early diagnosis and rapid initiation of medication are important for the treatment of ocular and systemic tuberculosis.
Keywords
Introduction
Tuberculosis, one of the most contagious infections has caused a high rate of mortality and it is responsible for almost 1.4 million deaths yearly. 1 Ocular tuberculosis has diverse manifestations and can involve any tissues of the eye and orbit. The uveal tissue is especially vulnerable owing to its rich vascularity. Choroidal involvement ranges from a solitary choroidal granuloma to multiple choroidal tubercles, a subretinal abscess or choroiditis. This is one of the few reported cases of a solitary choroidal granuloma with no other systemic symptoms in an immunocompetent child. It highlights the importance of a quick diagnosis and initiation of timely therapy.
Case report
A 12-year-old girl, presented with complaints of diminution of vision in her left eye for 1 month. She had no other complaints. The best corrected visual acuity in her right eye was 6/6 and the left eye was 1/60. On examination, her right eye was normal. The anterior segment of her left eye was normal. Fundus examination of her left eye showed a solitary, orangish- yellow subretinal lesion with fuzzy margins which was around 4 DD in size and was located at the posterior pole (Figure 1(a)). There was overlying subretinal fluid present. OCT of the left eye revealed a large choroidal elevation with compression of the overlying choriocapillaris and a neurosensory detachment. A distinctive feature of attachment between the retinal pigment epithelial–choriocapillaris layer and the neurosensory retina over the granuloma, known as the “contact” sign was evident on OCT (Figure 1(b)). BSCAN ultrasonography of the left eye showed a dome shaped choroidal lesion. The corresponding A- scan showed moderate internal reflectivity (Figure 1(c)).
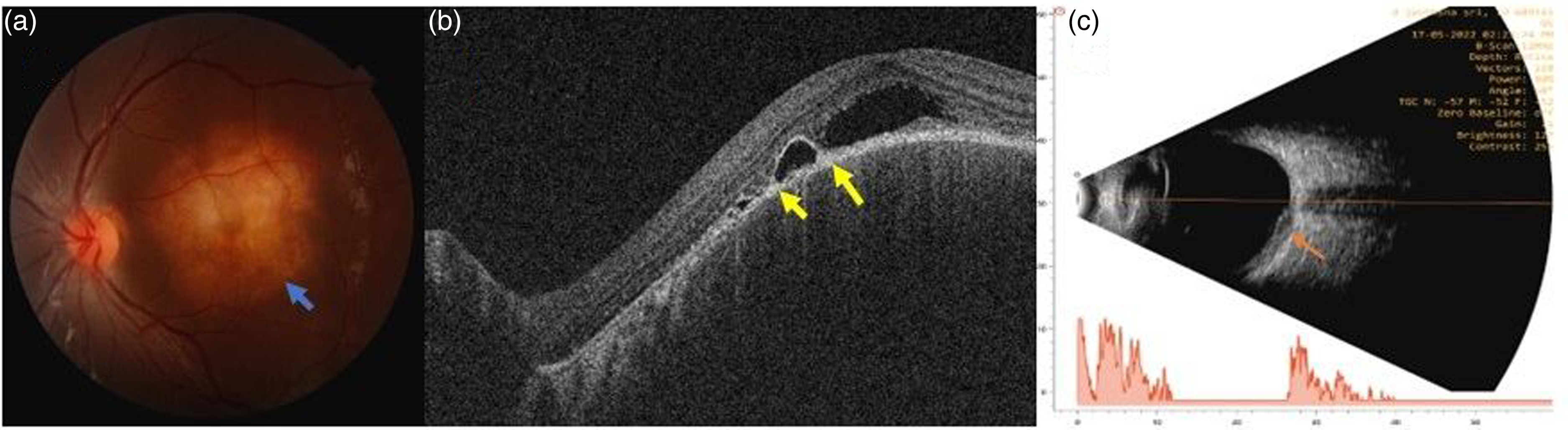
(a) Left eye fundus photo shows a yellowish- orange choroidal lesion, 4 DD in size with fuzzy margins, located at the posterior pole (blue arrow). (b) Left eye OCT shows a neurosensory detachment (NSD) and contact sign (yellow arrows). (c) Left eye Bscan showing a dome shaped choroidal lesion and the corresponding A-scan shows moderate reflectivity (orange arrow).
Systemic examination was normal. Human immunodeficiency virus (HIV) antibody, syphilis and hepatitis B and C serology were normal. Initial laboratory investigations showed an elevated erythrocyte sedimentation rate of 100 mm/ hr. A 20 mm induration was noted in the Mantoux test, which was strongly positive. On further enquiry, a single dose of BCG vaccine had been administered to her at birth. Her chest X-ray showed enlarged mediastinal and hilar lymphadenopathy. A CT scan of the thorax was performed which revealed cervical, mediastinal and retroperitoneal lymphadenopathy with central necrosis and encasement of mediastinal structures. There were lytic lesions of the T7 vertebra and manubrium sterni with involvement of the paravertebral tissues causing significant compression on the theca. The patient was referred to a pulmonologist where she was advised excision biopsy of the cervical lymph nodes under general anaesthesia. The histopathology report revealed caseating tuberculous lymphadenitis, with no evidence of malignancy.
She was started on anti-tubercular treatment in the form of four drugs i.e., isoniazid, ethambutol, pyrazinamide, and rifampicin for 3 months and isoniazid and rifampicin for 6 months. At the end of 6 months, her visual acuity had improved to 6/12 and the size of the choroidal tuberculoma had decreased (Figure 2(a)). An OCT of the left eye showed resolution of the subretinal fluid (Figure 2(b)).
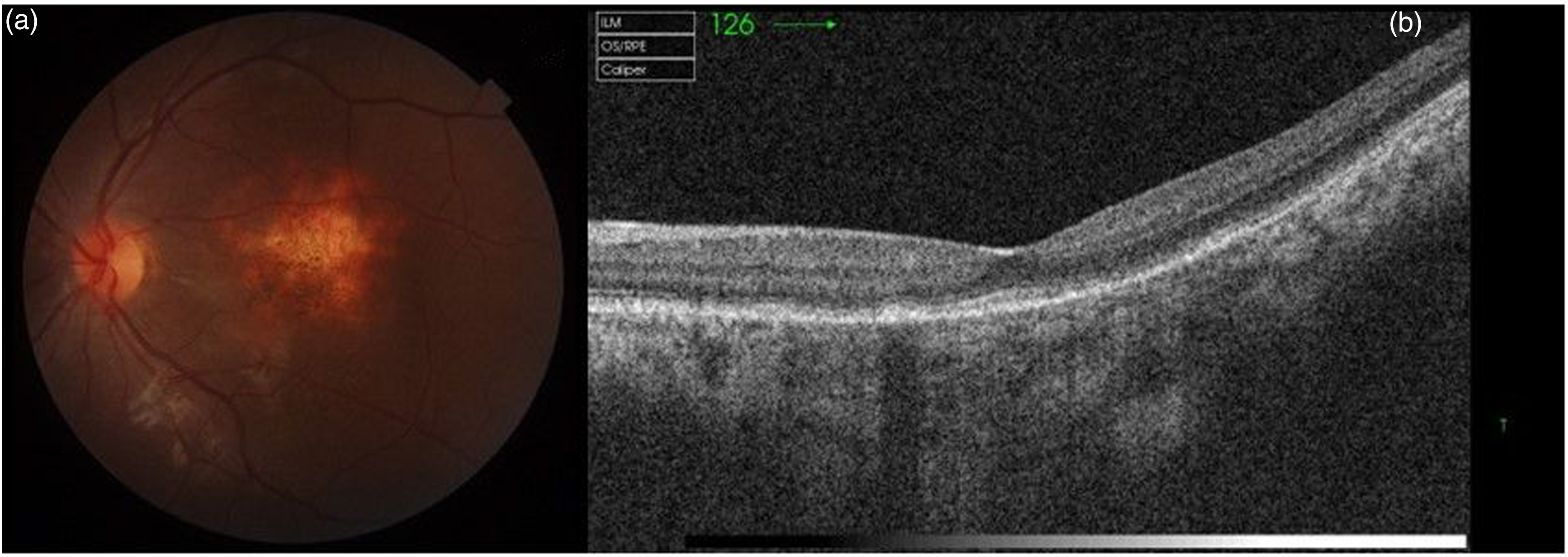
(a) Left eye fundus picture shows a reduction in the size of the choroidal lesion. Left eye OCT shows a complete resolution of the NSD and the contact sign.
Discussion
Although ocular TB is a rare event (1% of all cases of TB), it can occur with or without evidence of systemic TB and can involve any part of the eye. 2 The most common clinical presentation appears to be posterior uveitis, particularly multiple choroidal tubercles. Less commonly, intraocular TB may present as a large tuberculoma: generally located in the posterior pole. 3
Rarely, a tuberculoma may be the presenting sign in a patient with no evidence of systemic disease. Only a handful of cases have been reported as choroidal tuberculomas as the initial sign of systemic tuberculosis.3–7
Imaging techniques, such as fluorescein angiography and B-scan, can assist in excluding other diagnoses, especially intraocular tumours (e.g., melanoma) or infective abscesses. 2 Salman et al were the first to describe a distinctive OCT feature, of attachment between the retinal pigment epithelial–choriocapillaris layer and the neurosensory retina over the granuloma (“contact sign”). 8
Visual recovery and choroidal tuberculoma involution to a flat inactive scar can occur with proper and rapid diagnosis and treatment.
This is one of a few reported cases of a unilateral, solitary large choroidal granuloma as the only presenting feature of disseminated tuberculosis in an immunocompetent girl. Our patient had multiorgan involvement (ocular, lungs, cervical, retroperitoneal and pancreatic lymph nodes, vertebrae and manubrium sterni). Despite this, her presenting symptom was vision loss. This highlights the importance of keeping a low threshold to search for other foci of disease in such patients to initiate timely therapy.
Conclusion
Ophthalmologists should be aware that a choroidal tuberculoma may be the presenting sign of tuberculosis with or without systemic disease even in an immunocompetent patient. There should be a low threshold for a thorough systemic evaluation including imaging, especially in endemic countries. Early diagnosis and initiation of treatment can lead to a demonstrable reduction in inflammation and symptoms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Written informed consent for patient information and images to be published was provided by the patient's legally authorized representative.