
Abstract
Purpose
To evaluate preferred diagnostic tools and treatment decision-making factors in cases suspicious of mucous membrane pemphigoid (MMP) amongst ophthalmologists and cornea specialists.
Methods
Web-based survey, consisting of 14 multiple choice questions, posted to the Cornea Society Listserv Keranet, the Canadian Ophthalmological Society Cornea Listserv, and the Bowman Club Listserv.
Results
One hundred and thirty-eight ophthalmologists participated in the survey. Eighty-six percent (86%) of respondents were cornea trained and practiced in either North America or Europe (83%). Most respondents (72%) routinely perform conjunctival biopsies for all suspicious cases of MMP. For those who do not, fear that biopsy will exacerbate inflammation was the most common reason to defer investigation (47%). Seventy-one percent (71%) performed biopsies from perilesional sites. Ninety-seven percent (97%) ask for direct (DIF) studies and 60% for histopathology in formalin. Most do not recommend biopsy at other non-ocular sites (75%), nor do they perform indirect immunofluorescence for serum autoantibodies (68%). Immune-modulatory therapy is started following positive biopsy results for most (66%), albeit most (62%) would not let a negative DIF influence the choice of starting treatment should there be clinical suspicion of MMP. Differences in practice patterns as they relate to level of experience and geographical location are contrasted to the most up-to-date available guidelines.
Conclusion
Responses to the survey suggest that there is heterogeneity in certain practice patterns for MMP. Biopsy remains an area of controversy in dictating treatment plans. Identified areas of need should be targeted in future research.
Introduction
Mucous membrane pemphigoid (MMP) is an autoimmune disease that affects the mucous membranes of individuals typically older than 60-year-old.1 Oral mucosa is the primary affected area (90% of cases), and ocular mucosa is the main secondary area (61% of cases).2 About one-third of patients with oral mucosal manifestations will progress to have ocular manifestations.1,2 Ocular manifestations include chronic and progressive conjunctivitis and inflammation which can lead to complications including symblepharon, limbal stem cell deficiency, corneal ulceration and perforation, and blindness.3 While the etiology of MMP is not fully understood, there is evidence to support that it may be caused by a Type II hypersensitivity response to the basement membrane of conjunctival epithelium.4,5 The diagnosis and management of MMP present many challenges. In the field of ophthalmology, the differential diagnosis for cicatricial conjunctivitis is broad, which can delay the diagnosis and lead to irreversible corneal damage and blindness.6 Diagnostic work-up for MMP can last approximately 21 months.3 The early-stage disease can have non-specific findings, including dry eye symptoms, redness, and foreign body sensation, which can lead to the under-recognition of MMP.7 Conjunctival biopsies with direct immunofluorescence are helpful tools for diagnosis, however, biopsies may be inconclusive considering that the sensitivity of the diagnostic procedure is 40–50% and worsens with severe cicatrization.6–8 As such, the diagnosis requires a combination of diagnostic tests and clinical exams from a multidisciplinary team with sufficient knowledge and familiarity with the natural history of the disease to recognize it.8 Ocular MMP carries a poor prognosis and, if left untreated, MMP progresses in over 75% of patients.7 Approximately 30% of individuals affected with MMP with advanced conjunctival fibrosis become blind.9,10 Due to the systemic nature of the disease, an interprofessional team is essential.5 Medical management involves using a stepladder approach with systemic immunosuppression to limit the progression of conjunctival scarring.5 Despite these challenges, there is no consensus on the diagnosis or treatment algorithm specific for MMP that is used by all ophthalmologists. Clinical and diagnostic approaches tend to differ from center to center and no studies to date have scrutinized the preferred practice patterns in the diagnosis and management of cases suspicious of MMP. In addition, the relative rarity of this disease could contribute to a lack of applied international guidelines on its management. As such, the purpose of this study is to explore and understand the preferred diagnostic patterns for cases suspicious of MMP amongst ophthalmologists and cornea specialists and help identify common practice patterns.
Materials and methods
A unique questionnaire available in both English and French was distributed electronically to ophthalmologists and cornea specialists internationally using personalized invitations and list servers amongst the ophthalmology community including the Cornea Society Listserv Keranet, the Canadian Ophthalmological Society Cornea Listserv, and the Bowman Club Listserv. The questionnaire can be found in supplemental digital content 1.0. There was no financial incentive to participate. The inclusion criteria encompassed practicing ophthalmologists and cornea specialists, with a specific focus on ophthalmologists in North America and Europe. Residents and ophthalmology trainees were excluded from this study. The 3-min anonymous questionnaire was active for 8 consecutive weeks ending July 1,st 2022, on the Momentive platform. In total, three email reminders were sent to ophthalmologists during the second, fourth, and sixth weeks of the data collection period.
The online survey consisted of 14 multiple-choice questions. The questionnaire collected data regarding the demographics of the respondents, including the geographic area of practice, sub-specialization, years of experience, and the setting of practice. Information was also obtained regarding the MMP diagnosis patterns amongst ophthalmologists, including the reported yearly incidence of MMP or cicatrizing conjunctivitis in their practice and their diagnostic approach using biopsy and serology. Finally, ophthalmologists were asked about the management of MMP in their practice and the relationship between biopsy results and systemic immunomodulatory therapy.
Descriptive analysis was done using the Momentive platform and Microsoft Excel. A sub-group analysis based on the level of experience and the geographical location of respondents was performed using a two-tailed Z-score proportional analysis. Missing data was excluded. The study was approved by the ethics review board of the University of Montréal hospital center (CHUM) and was conducted in accordance with the Declaration of Helsinki.
Results
Demographic details
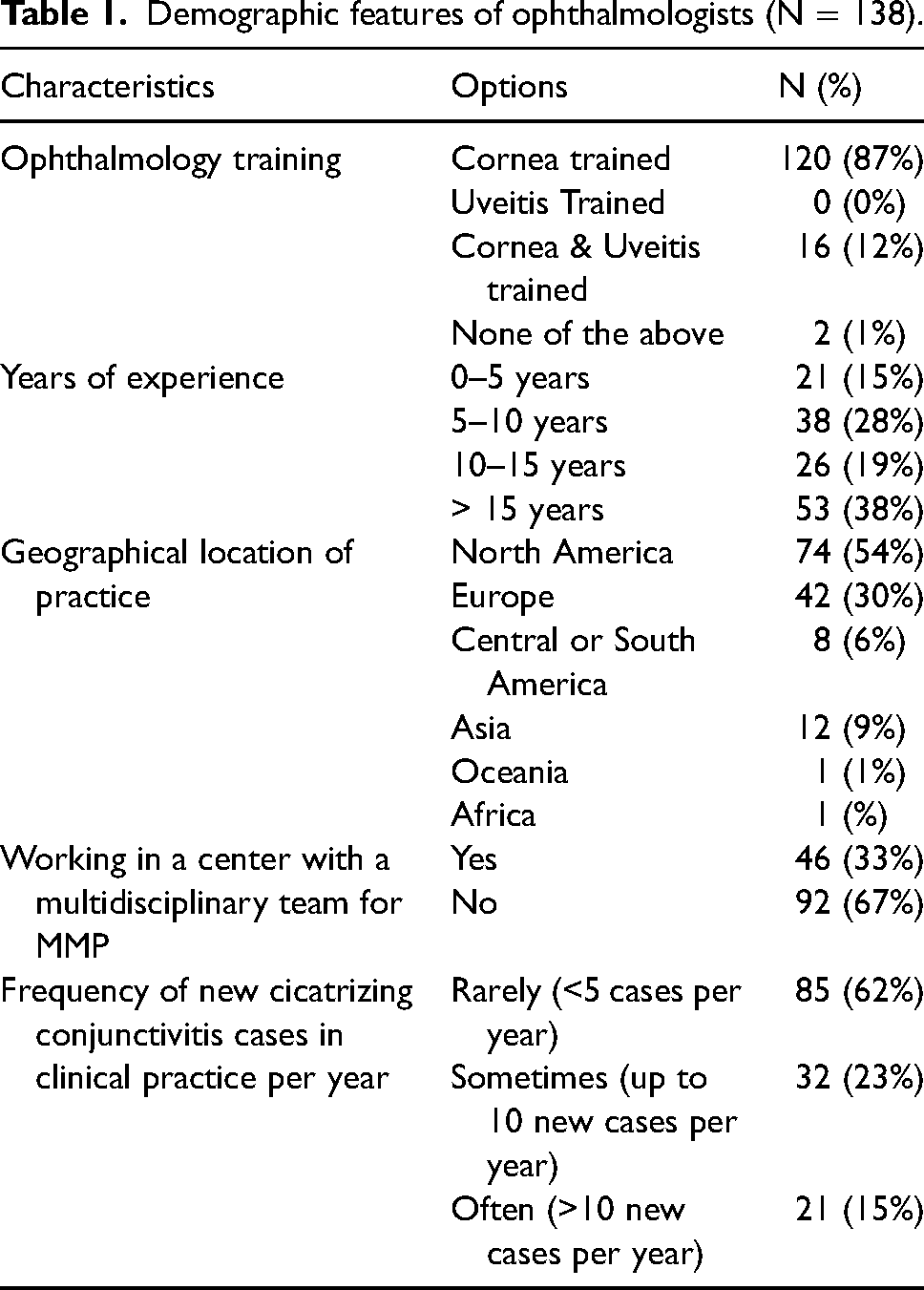
A total of 138 ophthalmologists responded to the survey. Table 1 highlights the demographic features of the respondents. The majority (n = 120; 87%) of respondents were cornea-trained specialists, and a minority (n = 16; 12%) are both cornea and uveitis trained. Most ophthalmologists had over 10 years of experience (n = 79; 57%) and practice in a non-multidisciplinary setting (n = 92; 67%). Those who did practice in multidisciplinary settings (n = 46) reported collaborating most with dermatology (n = 28), rheumatology (n = 13), oral medicine and dentistry (n = 8), oculoplastic (n = 7), and/or pathology (n = 6). Most ophthalmologists rarely encounter MMP in their practice with less than five new cases per year (n = 85; 62%).
Demographic features of ophthalmologists (N = 138).
Diagnostic pattern
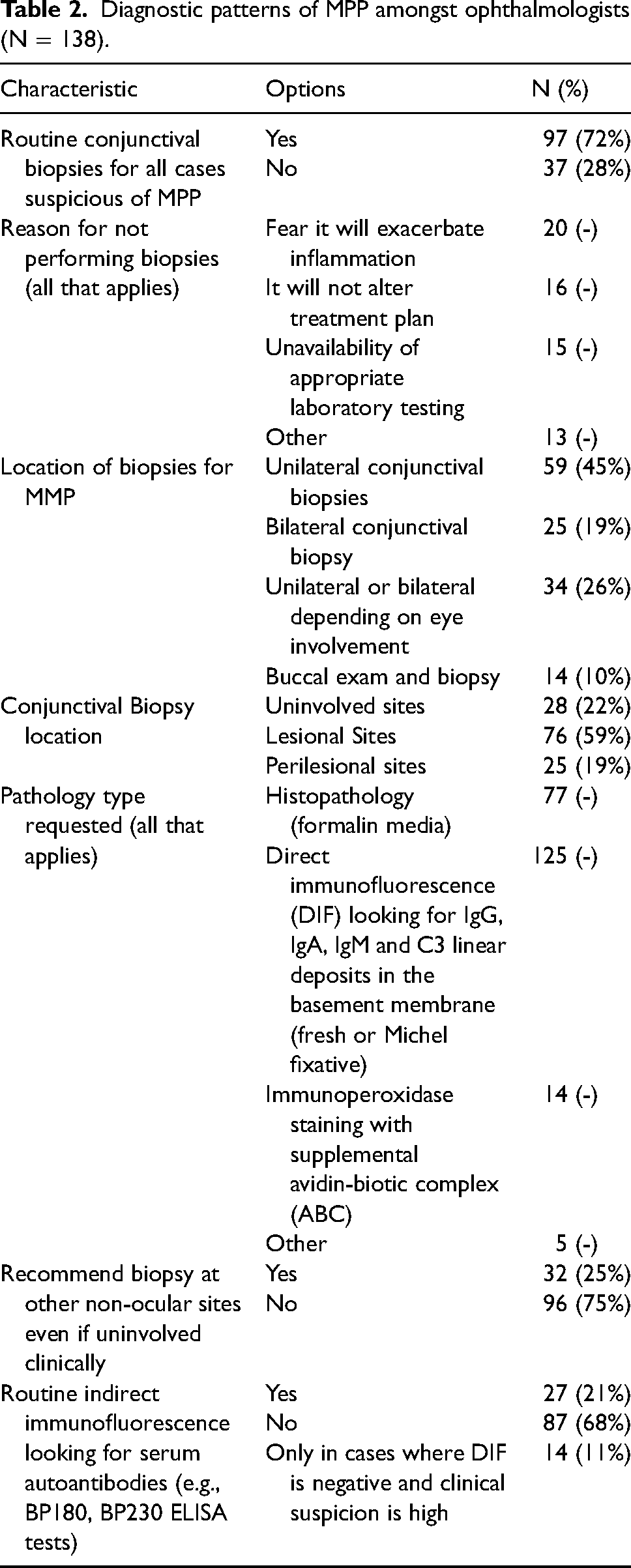
Table 2 highlights the diagnostic patterns of MMP amongst ophthalmologists. Most respondents report using biopsy to confirm the diagnosis of MMP (n = 97; 72%). Those who do not use biopsy (n = 37; 28%) attribute it to the fear of exacerbating the inflammation (n = 20), the belief that it may not alter the treatment plan (n = 16), and/or the unavailability of appropriate laboratory testing (n = 15). Some ophthalmologists (n = 8) do not perform biopsies and prefer to refer the cases suspect of MMP, either for extra-ocular biopsy or to a sub-specialist colleague. Ophthalmologists who perform ocular biopsies often perform unilateral conjunctival biopsies (n = 59; 45%) of perilesional sites (n = 76; 59%). Direct immunofluorescence (DIF) looking for IgG, IgA, IgM, and C3 linear deposits in the basement membrane (fresh or Michel fixative) is the pathology of choice for most ophthalmologists (n = 125). Additionally, over half of ophthalmologists also ask for histopathology using formalin media (n = 77). Only a minority perform immunoperoxidase staining with supplemental avidin-biotic complex (n = 14). Most respondents do not recommend or perform biopsies at non-ocular lesional sites (n = 96; 75%). Most ophthalmologists (n = 87; 68%) do not perform serology for indirect immunofluorescence (IIF) looking for autoantibodies (e.g., BP180 and BP230 salt split skin or ELISA tests). Figure 1 highlights the sub-group analysis based on experience level and geographical location of ophthalmologists. Overall, there are no statistically significant differences between respondents with less than 10 years of experience and those with more experience, except for increased routine indirect immunofluorescence looking for serum autoantibodies in more novice specialists (32% vs. 13%, p: 0.01). European ophthalmologists are performing more bilateral biopsies (40% vs 7%, p: < 0.01) and perilesional biopsies (78% vs. 55%, p: < 0.01) than their North American counterparts who opt for more of a unilateral and lesional approach. European specialists are also more likely to recommend biopsies at non-ocular sites (49% vs. 9%, p: < 0.01) than their North American colleagues.
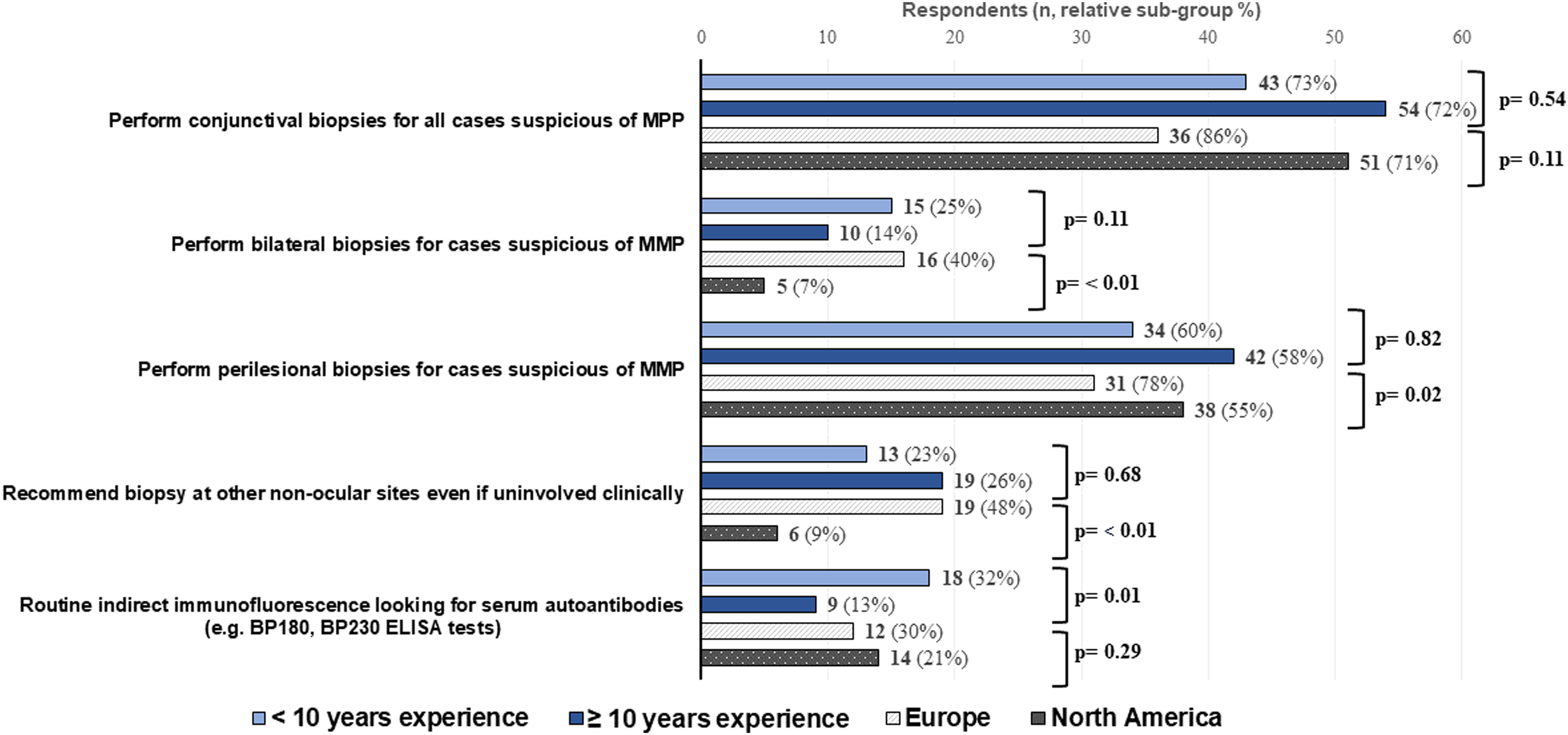
Sub-group analysis of practice patterns based on experience level and geographical location.
Diagnostic patterns of MPP amongst ophthalmologists (N = 138).
Treatment initiation
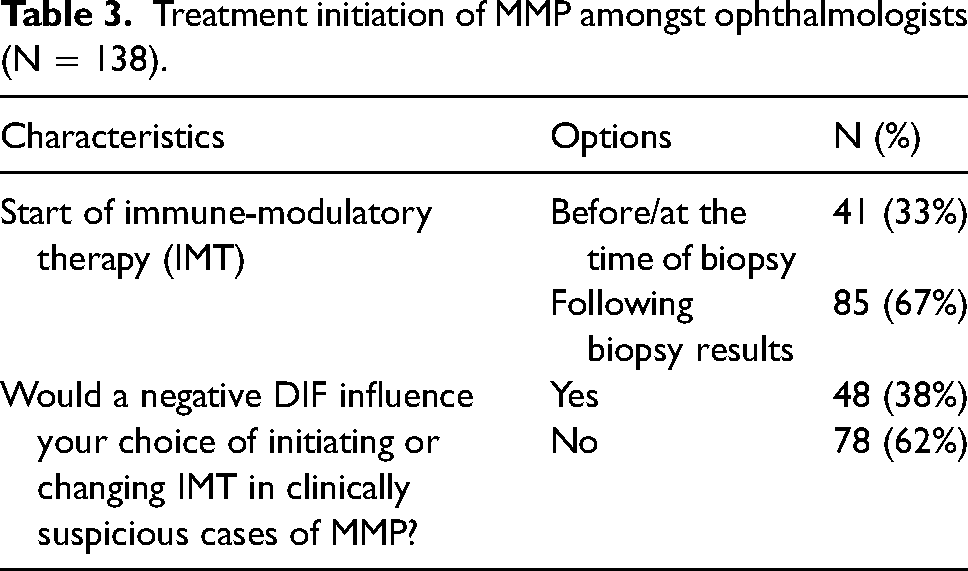
Table 3 highlights the treatment initiation pattern used by ophthalmologists. Most ophthalmologists reported waiting for biopsy results before the initiation of systemic immunomodulatory therapy (n = 85; 67%). However, a negative DIF would not influence the decision to start treatment in a clinically suspicious case of MMP in the majority of respondents (n = 78; 62%).
Treatment initiation of MMP amongst ophthalmologists (N = 138).
Discussion
This study highlights the preferred diagnostic tools and treatment decision-making factors in cases suspicious of MMP amongst ophthalmologists and cornea specialists. Four main concepts were explored in the context of MMP: biopsies, serology, initiation of treatment, and finally the multidisciplinary approach.
Current available guidelines for ocular MMP
The European guidelines (S3) on the diagnosis and management of MMP initiated by the European Academy of Dermatology and Venereology (EADV) published in 2021 in the journal of EADV are the only available guidelines for ocular MMP to date.3,5 The guideline committee includes two ophthalmologists, as well as dermatology, oral medicine, otorhinolaryngology and pathology colleagues.3
Biopsies in the diagnosis of ocular MMP
Responses to the survey suggest that there is heterogeneity in certain practice patterns for MMP, namely in biopsies. Over a quarter (n = 37; 28%) of ophthalmologists do not perform any biopsies for the diagnosis of MMP. The European guidelines (S3) are the first to propose an algorithm for the diagnosis and treatment of MMP.3,5 It is recommended in this guideline to complete DIF in parallel with serology analysis with indirect immunofluorescence and pemphigoid autoantibody tests (e.g., BP180 and BP230 ELISA) for all clinical cases suspicious of MMP in addition to routine histopathology to rule out other pathologies, such as neoplasia.5 According to the guidelines, a positive DIF confirms the diagnosis of MMP providing the appropriate clinical picture.5 The ophthalmologists that do not perform biopsies (n = 37; 28%) in this study attribute it to the fear that it may exacerbate inflammation, or that it may not alter the treatment plan and/or the unavailability of appropriate laboratory testing. A small subset of ophthalmologists (n = 8) chooses to refer their patients to a colleague for either ocular or extra-ocular biopsies. The findings of this study suggest that there is an opportunity for increased awareness and education worldwide in the field of ocular MMP. These heterogeneous findings also highlight the importance of universal guidelines in the diagnosis and management of ocular MMP.
The ophthalmologists in this study who do perform biopsies (n = 97; 72%) for cases suspicious of MMP mainly perform one unilateral ocular lesional biopsy (45%; 59%) for histopathology (formalin media) and/or for DIF looking for IgG, IgA, IgM and C3 linear deposits in the basement membrane (Fresh or Michel fixative) (n = 77; n = 125). European specialists follow the S3 guidelines more than their North American colleagues, recommending more bilateral and perilesional biopsies (40% vs 7%, p: < 0.01; and 78% vs. 55%, p: < 0.01 respectively). A large proportion of respondents do not perform routine histopathology (n = 58; 43%). Only a minority perform immunoperoxidase staining with supplemental avidin-biotic complex (n = 14; 10%). Immunoperoxidase techniques allow for an increase in sensitivity of biopsies up to 83% when used in conjunction with standard DIF.11 Most respondents reported not recommending extra-ocular biopsies to their patients (n = 96, 75%). European ophthalmologists were however more inclined to recommend biopsies at non-ocular sites as recommended by the S3 guidelines compared to their North American counterparts (48% vs. 9%, p = < 0.01). European ophthalmologists may be more inclined to follow the S3 guidelines due to close geographical location and thus better awareness of these guidelines. The European Academy of Dermatology and Venereology recommends performing bilateral perilesional biopsies of the least inflamed bulbar conjunctiva along with an extra-ocular site, such as the buccal mucosa or skin, for DIF.5 It is also recommended that a fourth ocular lesional biopsy be taken for routine histopathology to exclude possible sarcoid or ocular surface neoplasia.5 If a first DIF is negative, then a repeat biopsy is warranted.5 Multiple biopsies improve the detection of a positive test; however, the optimal number of biopsies is unknown.5 As such, this study highlights that there is a discrepancy between actual clinical practice and the currently available guidelines in terms of the biopsy location (bilateral vs. unilateral, lesional vs. perilesional), biopsy type (DIF vs. histopathology), and the number of biopsies (one vs. four) in the diagnosis of ocular MMP. This discrepancy may be influenced by the availability of local resources and expertise in certain health care settings. Previous literature has highlighted the poor prognosis in undetected MMP. As such, it is important for future research to explore the optimal number and types of biopsies, for both low and high resource settings.
Serology testing for the diagnosis of ocular MMP
In this study, most ophthalmologists reported not performing routine immunofluorescence looking for serum autoantibodies (e.g., BP180, BP230) (n = 87; 68%). Serology techniques are more used by specialists with less than 10 years of experience (18% vs. 9%, p: 0.01). This could be explained by the novel nature of serologies, hence why more recent practitioners might feel more comfortable using them in their clinical practice. The S3 guidelines recommend performing routine serological testing in parallel to the ocular and extra-ocular biopsies outlined above.3,5 This discrepancy in clinical practice may be due to the availability of laboratory testing in certain settings or the lack of awareness of its usage in the diagnosis of MMP. Conjunctival biopsies with DIF are helpful tools for diagnosis, however, biopsies may be inconclusive considering the low sensitivity of the diagnostic procedure.6–8 Serology testing in this setting allows for increased yield, but in ocular MMP, both DIF and serology may still be negative in up to 50% of cases.5
Initiation of treatment of MMP
In this study, most ophthalmologists choose to start immune-modulatory therapy (IMT) only following biopsy results (n = 85; 67%). Most ophthalmologists indicated that a negative DIF would not influence their choice in initiating therapy in clinically suspicious cases of MMP (n = 78; 62%). These findings are in accordance with the S3 European guidelines, which recommend starting treatment only once the final diagnosis is obtained.3,5 The S3 guidelines indicate that up to 50% of cases of ocular MMP may be immunopathology unconfirmed, but that an ocular MMP diagnosis may be made once more than 25 other causes of cicatrizing conjunctivitis have been excluded.3,5 Previous literature has shown that patients with progressive cicatrizing conjunctivitis with negative DIF likely have MMP until proven otherwise.12 Previous ophthalmology literature recommends treating and diagnosing DIF-negative and IIF serology negative MMP, and to reassess should the disease trajectory or response to treatment not match expectations.13,14
Multidisciplinary approach in MMP
Ophthalmologists in this study rarely encounter cicatrizing conjunctivitis in their clinical practice (n = 85; 62%). Most respondents reported treating MMP in a non-multidisciplinary setting (n = 92; 67%). Those who did practice in multidisciplinary (n = 46; 33%) settings reported collaborating most with dermatology (n = 28), rheumatology (n = 13), oral medicine and dentistry (n = 8), oculoplastic (n = 7), and/or pathology (n = 6). The S3 guidelines recommend managing MMP as part of a multidisciplinary team, including oral medicine, dermatology, and otorhinolaryngology.3,5 This discrepancy between clinical practice and the guidelines may be in part caused by the health care systems in which the ophthalmologist's practice which may limit interdisciplinary collaboration, such as community or private practice.
MMP in our academic centers
In our centers, a definitive diagnosis of MMP is confirmed once there is an appropriate clinical picture with either (1) a positive DIF from oral or conjunctival mucous membranes, or (2) a negative DIF with a positive IIF, or (3) a negative DIF and IIF with signs of disease progression with other causes of symblepharon ruled out.14 Ophthalmologists perform biopsies when the eye is least inflamed in all cases suspicious of MMP.15 Clinicians first perform bilateral perilesional ocular biopsies when the eye is least inflamed, preferably in the upper conjunctiva for improved healing, one buccal biopsy, and finally, bilateral lesional biopsy for formalin histopathology to rule out other causes of cicatrizing conjunctivitis, such as neoplasia. Repeat biopsies are considered if only inflamed lesional sites are available initially. Serology studies are recommended for multi-site MMP if local resources allow for it and especially if a first DIF is negative or if the eyes are severely inflamed and not ready for biopsy. Of note, serum autoantibody testing has been reported to be ineffective for ocular-only MMP.14 If clinical suspicion is very high for MMP, a course of oral steroids is started if there are no contraindications with a possible later bridging to IMT in collaboration with dermatology and/or rheumatology colleagues. Interdisciplinary care is encouraged given the morbidity and the rarity of the disease.
One of the limitations of this survey is that most ophthalmologists rarely see cicatrizing conjunctivitis in their practice, therefore there might be recall bias in addition to self-selection bias. Additionally, most respondents are cornea specialists, thus these results may not be representative of comprehensive ophthalmologists who may encounter cicatrizing conjunctivitis in their practice or other ophthalmology sub-specialties. Another limitation is that the survey was only active for a period of 8-weeks, thus only providing a snapshot in time of the ophthalmologist's practice patterns.
To our knowledge, this is the first survey study evaluating preferred practice patterns in the diagnosis of mucous membrane pemphigoid amongst ophthalmologists. This study highlights a heterogeneity in the diagnosis pattern between ophthalmologists and contrasts these practice patterns with the current literature. With the existing situation, literature has highlighted that most patients with ocular MMP are diagnosed and treated late, and thus present with advanced cicatrizing disease and complications.3 A universal standardized multidisciplinary approach with evidenced-based input from all relevant subspecialties may aid with the early detection of MMP, thus helping to decrease the time to diagnosis and treatment and help prevent blinding complications. Additional awareness and continuing education on ocular MMP may also contribute to a more unified approach and thus help detect early disease.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231178110 - Supplemental material for Survey: Preferred practice patterns in the diagnosis of mucous membrane pemphigoid amongst cornea specialists
Supplemental material, sj-docx-1-ejo-10.1177_11206721231178110 for Survey: Preferred practice patterns in the diagnosis of mucous membrane pemphigoid amongst cornea specialists by Sarah Moussa, Maya Tong, Marie-Claude Robert, Mona Harissi-Dagher, Sajjad Ahmad and Samir Jabbour in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.