
Abstract
Objective
To assess the possible correlation between patients’ personality traits and subjective perception of quality of vision (QoV), after multifocal intraocular lens (mIOL) implantation.
Methods
patients who had bilateral implantation of a non-diffractive X-WAVE or a trifocal lens were assessed 6 months postoperatively. Patients answered the NEO-Five Factor Inventory (NEO-FFI-20) questionnaire (“Big Five five-factor personality model”) to examine their personality. Six months following surgery, patients were asked to fill a QoV questionnaire where they graded the frequency of 10 common visual symptoms. Primary outcomes were to evaluate the correlation between personality scores and the reported frequency of visual disturbances.
Results
The study comprised 20 patients submitted to bilateral cataract surgery, 10 with a non-diffractive X-WAVE lens (AcrySof® IQ Vivity) and 10 with a trifocal lens (AcrySof® IQ PanOptix). Mean age was 60.23 (7.06) years. Six months following surgery, patients with lower scores of conscientiousness and extroversion reported a higher frequency of visual disturbances (blurred vision, P = .015 and P = .009, seeing double images P = .018 and P = .006, and having difficulties focusing, P = .027 and P = .022, respectively). In addition, patients with high neuroticism scores had more difficulty focusing (P = .033).
Conclusions
In this study, personality traits such as low conscientiousness and extroversion and high neuroticism significantly influenced QoV perception 6 months after bilateral multifocal lens implantation. Patients’ personality questionnaires could be a useful preoperative assessment test to a mIOL.
Keywords
Introduction
Multifocal intraocular lenses (mIOL) are a viable solution for spectacle independence following cataract surgery. mIOLs currently available on the market have different optical designs, such as bifocal, trifocal, and extended depth of focus (EDoF). The advantages and disadvantages of each mIOL type in terms of visual performance at distance, intermediate and near distance have variable results. However, mIOLs are also frequently associated with visual disturbances including haloes, glare, and starbursts. More studies are focusing on the assessment, grading, and management of unwanted optical phenomena. 1 Quality of Vision (QoV) and patient satisfaction questionnaires are beginning to be a part of the criteria for success after mIOL, as patient reported outcomes are increasingly valued during mIOL postoperative evaluation.2,3
Surgeons have been trying to understand which objective and subjective factors play a role in patient satisfaction after mIOL implantation. One's individual cognitive and motivational characteristics are known to influence health perception,4,5 and a relationship between personality and visual perception has been studied.6,7 Woods et al. identified “low self-confidence” and “disorganization” to be correlated with a higher tolerance for blur, 6 although these authors tested the tolerance of blur of young college students in an experimental setting. Dell developed a preoperative questionnaire that included brief assessments of patients’ self-reported personality and found that personalities midway between “easygoing” and “perfectionist” tended to be the least happy after presbyopia-correcting IOLs. 8 Recently, two authors have proven that personality significantly influences patients’ satisfaction after mIOL.9,10 In addition, Mester et al. found a relationship between personality traits and the perception of visual disturbances. 11 Despite the increasing interest in the topic, there is still a paucity of research towards patients’ personality traits and whether they can influence subjective disturbances caused by photic phenomena and there is a lack of standardization in both methods for evaluating visual symptoms and in personality questionnaires’ scores. Ultimately, we lack information on whether a personality test can be used as an adjunctive preoperative tool to predict tolerance and satisfaction after cataract surgery with mIOL.2,7
The purpose of this study is to determine whether some personality traits could be associated with subjective visual complaints 6 months after bilateral implantation of a trifocal or a non-diffractive X-WAVE lens, using internationally validated personality and QoV questionnaires.
Methods
This was a single-site prospective, masked study conducted at the Ophthalmology Department at Centro Hospitalar e Universitário de Coimbra, Portugal. The study was approved by the local Ethics Committee and followed the tenets of the Declaration of Helsinki for biomedical research. All subjects signed an appropriate informed consent document. This study followed International Committee of Medical Journal Editors’ Recommendations for the conduct, reporting, editing, and publication of scholarly work in medical journals.
Participants
We included consecutive patients submitted to cataract surgery between january 2021 and march 2022. Inclusion criteria were as follows: patients under 70 years of age, eligible for cataract surgery, a corneal astigmatism of < 1.25 diopters (D) and regular topography measured with the Pentacam (Pentacam, OCULUS Optikgerate GmbH), pre-operative sphere in either eye inferior to ± 6 D. Exclusion criteria were amblyopia, previous ocular surgeries, ocular comorbidities such as glaucoma and retinal diseases and illiteracy. All IOLs were planned using the IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany); calculations were performed based on the Barret formula and the postoperative refraction target was set at emmetropia. Patients were randomly assigned to one of two multifocal intraocular lens (mIOL) implant: non-diffractive X-WAVE Alcon AcrySof IQ Vivity® and Trifocal Alcon AcrySof IQ PanOptix®. AcrySof Vivity is a non-diffractive lens with wavefront-shaping X-WAVE technology, with two smooth surface transition elements that simultaneously stretch and shift light without splitting it. 12 The AcrySof IQ PanOptix is a trifocal lens that has a central biconvex optic, with an inner diffractive and an outer refractive zone. It uses ENLIGHTEN® Optical Technology—a proprietary design that optimizes intermediate vision without compromising exceptional near and distance vision. 13 The surgery of the second eye had to have been completed within 1 month before the study visit. All surgeries were performed under topical anesthesia.
Visual outcomes
All patients underwent preoperative and postoperative complete ophthalmologic evaluation, including slit-lam biomicroscopy, fundoscopy and intraocular pressure measurement using Goldmann applanation tonometry. Subjective refraction was performed and monocular and binocular visual acuities (uncorrected and best distance-corrected) at distance (4 m) were recorded in Snellen notation and converted to LogMAR for statistical analyses. For intermediate (66 cm) and near (40 cm) vision assessment, we used the Radner-Coimbra Charts and recorded in logRAD. 14 Regarding mIOL power, the difference between both eyes was always inferior to 1.5 D, thus we used the power of the lens of the right eye as the independent variable for statistical analyses.
Personality and self-reported quality of vision
Six months after bilateral cataract surgery, all patients completed the QoV Questionnaire by McAlinden. 15 This is a 30-item instrument that evaluates 10 symptoms (glare, haloes, starbursts, hazy vision, blurred vision, distortion, double vision, fluctuation, focusing difficulties, and depth perception) rated in each of three scales (frequency, severity, and bothersome) (Figure 1, Supplemental Table 1). We reported only the frequency of symptoms, due to lack of data regarding severity and bothersome of symptoms (since patients who answered “never” to the question on the frequency of one symptom did not need to rate the severity and bothersome of that symptom). Also, patients filled the NEO Five-Factor Inventory (NEO-FFI-20), an abbreviated version of the NEO-FFI questionnaire which includes 20 sentences with responses rated on a 5-point scale (ranging from strongly disagree, 1, to strongly agree, 5) (Supplemental Table 2). 16 The scores are calculated for the “Big Five” Personality traits: Openness to experience (O), Conscientiousness (C), Extroversion (E), Agreeableness (A), and Neuroticism (N).17,14 It has been translated, adapted and validated into Portuguese language. 18
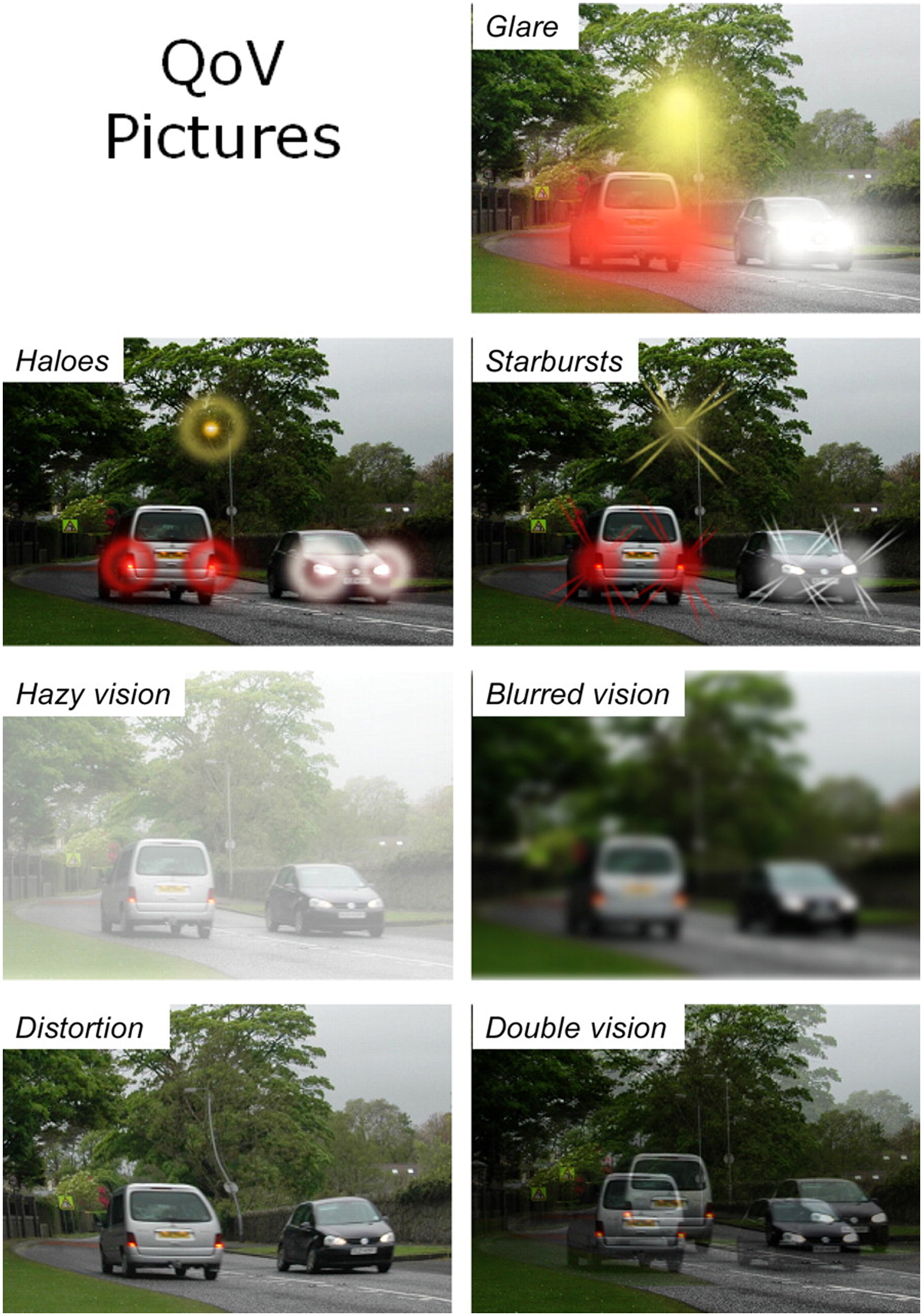
Quality of vision questionnaire.
Briefly, openness to experience is associated with a higher level of imagination and curiosity, focus on inner experience, aesthetic sensitivity, and a desire for knowledge. This personality trait is shared by intellectuals, freethinkers, and people with a strong imagination. Conscientiousness is a personality dimension that exhibits a tendency to plan and organize. It is related to academic and educational achievement and is characteristic of goal-oriented, trustworthy, and responsible individuals who are more likely to adhere to rules. Extroversion measures the level of an individual's sociability. Extraverts are friendly, cheerful, and active. They also tend to experience positive emotions. Concerning agreeableness, a person with high agreeableness score is altruistic, emphatic, and willing to help others. It is characteristic of trustful and humble individuals. Neuroticism shows that a person is more likely to experience negative emotions, such as anger, sadness, guilt, fear. It is the tendency to be irritable, bad-tempered, impulsive and to cope poorly.
Data analyses
Statistical analyses were performed using IBM SPSS Statistics, version 25. Demographics and visual and refractive postoperative outcomes were described using standard methods. Preoperative baseline characteristics and postoperative visual outcomes were compared between non-diffractive X-WAVE and Trifocal lenses using Mann-Whitney U-Tests. We also used the Kruskal-Wallis H test to see if there was an association in QoV scores between trifocal and non-diffractive X-WAVE groups. In order to determine which factors could be predictive of QoV answers, linear regression models were built. Each one of the 10 QoV questions was analyzed independently. P < .05 were considered statistically significant. Results are displayed as mean and (standard deviation). Whenever parametric test were used, 95% confidence intervals (CI) were provided.
Results
We included 20 patients (15 females), 10 subjects bilaterally implanted with a trifocal IOL (group 1) and 10 implanted with a non-diffractive X-WAVE IOL (group 2). There were no differences between the groups regarding demographic features (Table 1). There no significant differences found in most postoperative visual results between trifocal and non-diffractive X-WAVE groups, 6 months after surgery. Uncorrected (trifocal: −0.02 [0.04] logMAR; non-diffractive X-WAVE: 0.02 [0.06] logMAR) and corrected (trifocal: −0.07 [0.06] logMAR; non-diffractive X-WAVE −0.02 [0.06] logMAR) distance VAs were comparable (P > .05). DCIVA were also not statistically different among IOL groups (P > .05). However, patients in the trifocal group had significantly better DCNVA and UNVA visual results (0.08 [0.1] logRAD versus 0.24 [0.21] logRAD, P = .014 and 0.2 [0.13] logRAD versus 0.34 [0.11] logRAD, P = .023, respectively) (Table 1).
Demographic characteristics of patients and visual outcomes of PanOptix and Vivity intraocular lens groups.
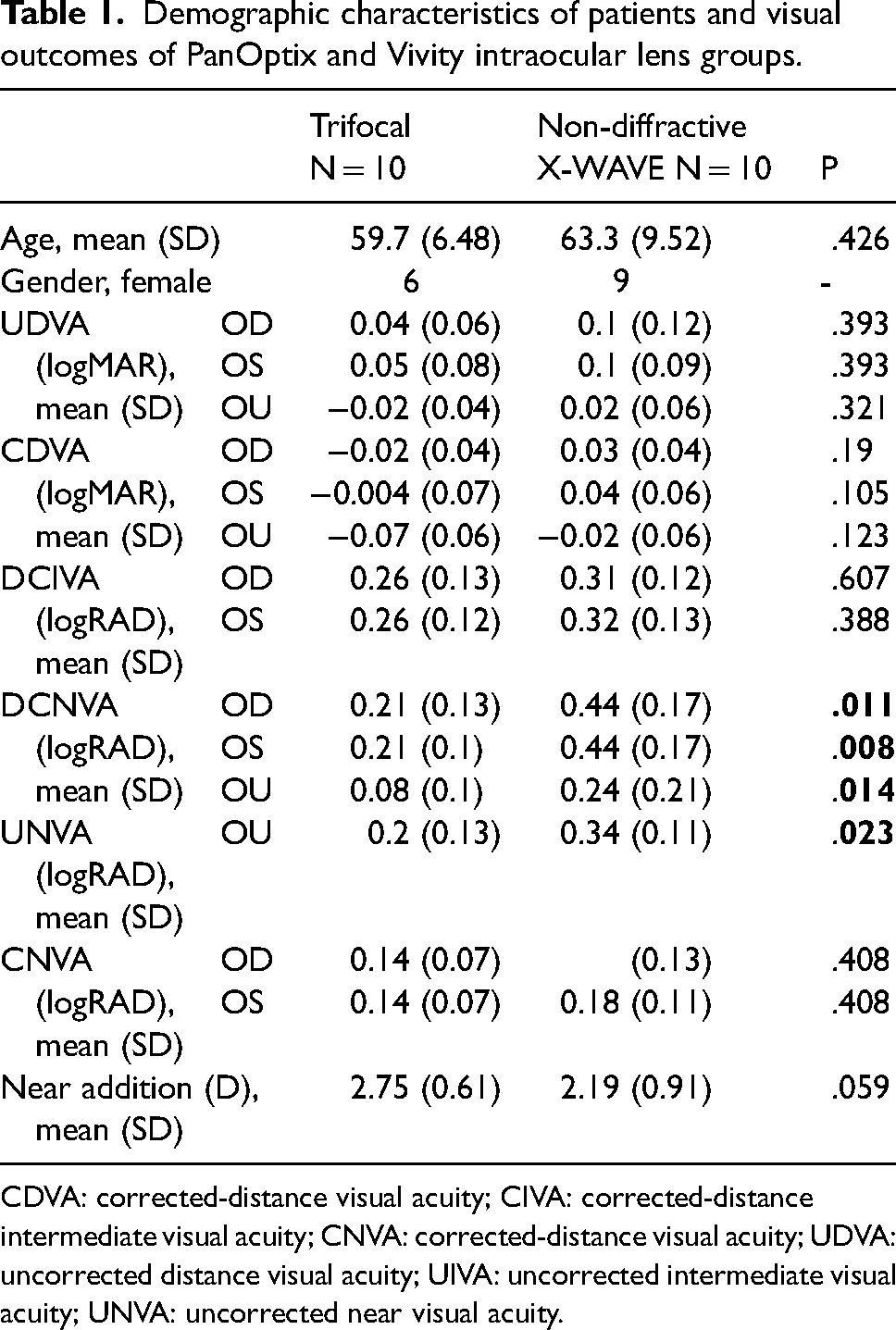
CDVA: corrected-distance visual acuity; CIVA: corrected-distance intermediate visual acuity; CNVA: corrected-distance visual acuity; UDVA: uncorrected distance visual acuity; UIVA: uncorrected intermediate visual acuity; UNVA: uncorrected near visual acuity.
The QoV questionnaires showed that at the 6-month follow-up the most frequent visual symptoms reported by patients were seeing haloes (very often = 30%, quite often = 30%) (Figure 2). When comparing the reported frequency of symptoms between the trifocal and the non-diffractive X-WAVE group, the Kruskal-Wallis H test showed a statistically significant difference in seeing haloes, χ2(1) = 5.909, P = .015, with a mean rank haloes score of 7.40 for non-diffractive X-WAVE and 13.60 for trifocal IOL. In response to the question “How often do you experience halos?” 80% trifocal patients answered “Quite often” and “Very often” compared to 40% of non-diffractive X-WAVE patients. The non-diffractive X-WAVE IOL was also predictive of a lower frequency of seeing haloes (B = -1.3, 95% CI, −2.24–0.35; P = .01). There were no differences regarding the frequency of other symptoms between trifocal and non-diffractive X-WAVE groups (P > .05). Also, no relationships were found between mIOL power and the frequency of visual symptoms (P > .05), except for “glare”, as higher mIOL powers were significantly correlated with a higher frequency of “glare” (B = .135, 95% CI, .027-.243; P = .018).
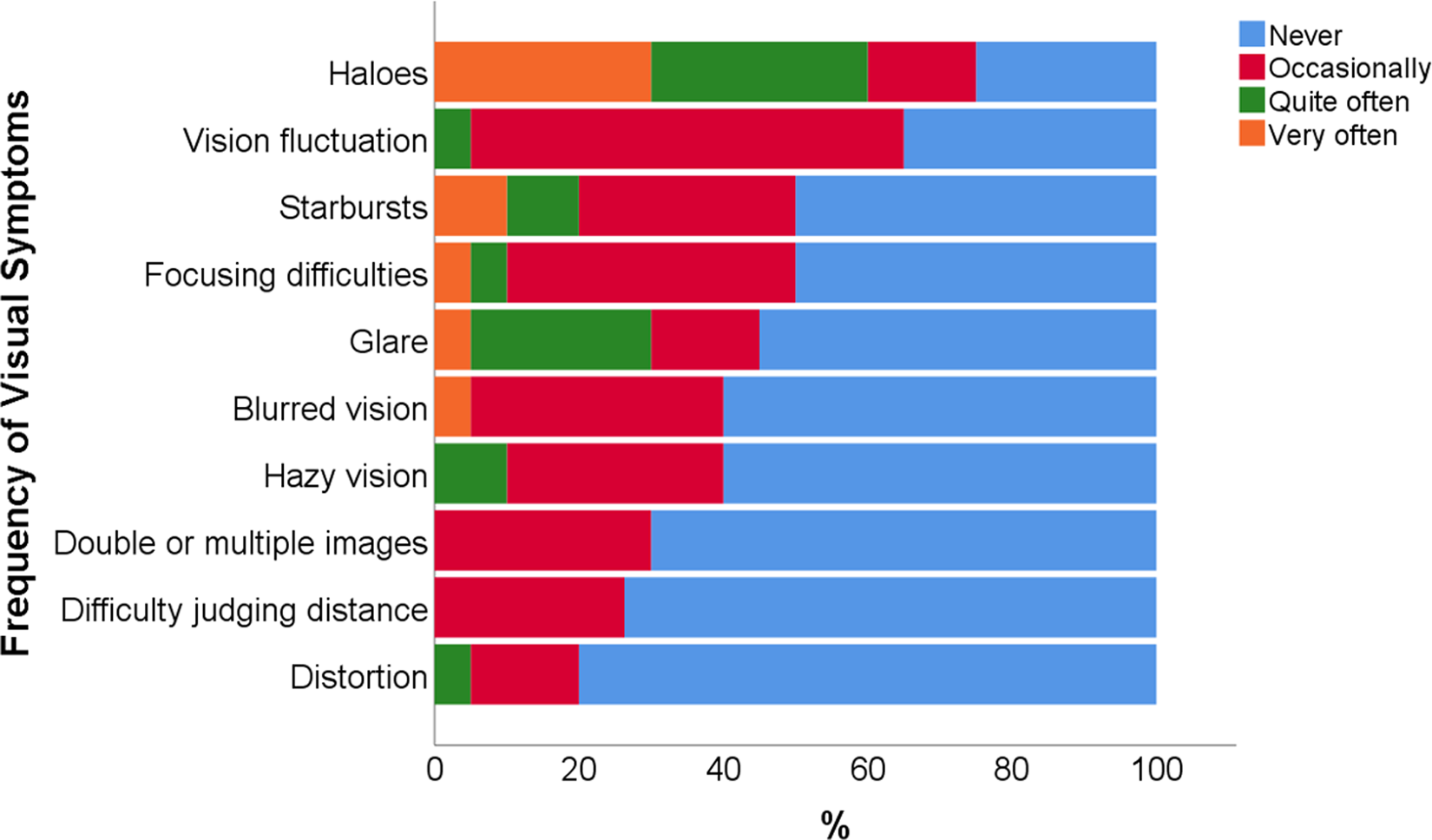
Visual symptoms reported by patients in both groups, 6 months after bilateral cataract surgery with multifocal intraocular lens implantation.
The results of the NEO-FFI-20 distribution scores of openness to experience, extroversion, agreeableness, and neuroticism showed no differences between mIOL groups, but patients in the trifocal group had significantly higher mean scores of conscientiousness (18 [1.94] versus 14.78 [2.48], P = .013) (Table 2). Besides, we found an inverse relationship between age and conscientiousness scores (B = -.16, 95% CI, -.32–.007; P = .004). There were no other correlations between patient's age and personality scores, nor with the frequency of reported symptoms (P > .05).
Scores of the “Big Five” personality traits for each mIOL group.
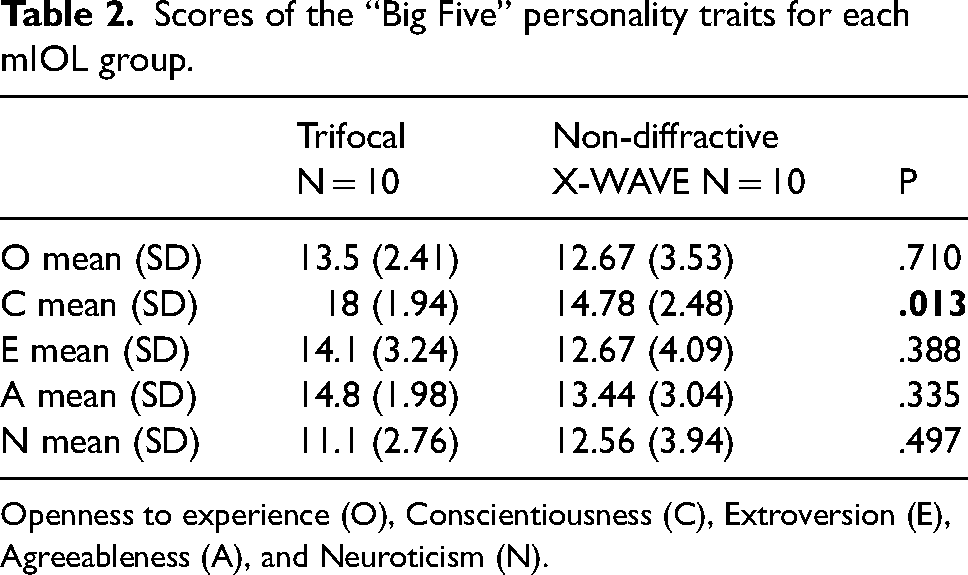
Openness to experience (O), Conscientiousness (C), Extroversion (E), Agreeableness (A), and Neuroticism (N).
Regarding “Big Five” scores and QoV answers, each personality trait was introduced as predictor of the frequency of each visual symptom. Patients with lower conscientiousness scores reported having more frequently blurred vision (B = -.113, P = .015), seeing double or multiple images (B = -.075, P = .018) and vision fluctuation (B = -.095, P = .027). Patients with lower extroversion scores reported more frequent blurred vision (B = -.086, P = .009), seeing double or multiple images (B = -.59, P = .006), having vision fluctuation (B = -.075, P = .012), having difficulties focusing (B = -.099, P = .022) and having difficulty judging distance or depth perception (B = -.048, P = .032). Finally, higher neuroticism scores were predictive of having difficulties focusing (B = .095, P = .033). Furthermore, analyses adjusting for covariates such as age, mIOL type and mIOL power showed similar findings, except for the relationship between having “difficulty judging distance or depth perception” and extroversion scores, that lost statistical significance after adjusting for mIOL type (B = -.046, P = .052).
Discussion
The current study aimed at understanding whether different personality traits could influence answers to the subjective QoV questionnaire, 6 months after bilateral trifocal or non-diffractive X-WAVE lens implantation. We compared both groups in terms of refractive outcomes, QoV scores and personality scores, to ensure there no significant differences among them. Groups differed only in DCNVA and UNVA and conscientiousness scores. We then looked for a correlation between subjective QoV and “Big Five” scores, including the whole study-population, given that we were interested in the global influence of personality on perceived quality of vision, independently of the chosen mIOL.
We found a significant correlation between some personality characteristics and visual complaints of patients with two different mIOL designs but whose refractive outcomes, postoperative satisfaction and personality scores were overall comparable.
Therefore, given the similarity between groups, results were most likely not influenced by mIOL performance.
Both mIOLs provided good uncorrected and corrected distant and intermediate distance VA, however, patients in the trifocal group had significantly better DCNVA and UNVA results, in line with previous studies.1,19 The QoV questionnaires were analyzed at the 6-month follow-up, and the most frequent visual symptoms reported by patients were haloes, followed by vision fluctuation. The non-diffractive X-WAVE was also associated with seeing haloes less often, compared with the trifocal lens. These results tie well with previous studies.20,21 Halos are one of the most reported visual disturbances22,23 among diffractive mIOL patients, hence this particular non-diffractive X-WAVE IOL, having no diffractive rings, is considered a good option for patients who are very averse to unwanted visual phenomena or those who frequently engage in night driving.22,23 In our study, there were no differences regarding the frequency of other symptoms between trifocal and non-diffractive X-WAVE groups (P > .05). However, two other authors found the TECNIS Symfony® IOL (an EDoF lens) to have worse QoV scores compared to other trifocal lenses.19,24 Differences among answers could be explained to some extent by subjective perception and individual tolerance. Our results showed that patients with higher mIOL power reported more frequent glare, which could be explained by the fact that as lens power increases, so does the amounts of optical aberrations, besides other factors influence glare, such as lens decentration and pupil diameter, which were not approached in this study.
Patients with lower extroversion scores reported more blurred vision, seeing double or multiple images, vision fluctuation and difficulties focusing. Extroverted people are friendly and talkative; people with lower extroversion scores, on the other hand, show reserve in social contacts and lack of optimism, which can lead to more attentiveness towards oneself experiences and a more negative insight of visual perception. Patients with lower conscientiousness scores reported more blurred vision, seeing double or multiple images and vision fluctuation. Conscientiousness characterizes an individual's degree of organization, persistence, and motivation in goal-oriented activities.
In line with our results, a study by Rudalevicius et al. 9 showed that patients with conscientiousness and agreeableness as dominant personality traits demonstrated the highest satisfaction with the postoperative outcomes. Another study evaluating pseudophakic presbyopic corrections found openness to experience, conscientiousness and extraversion to be major contributors to satisfaction rates. 10 In contrast with our findings, Mester et al. found compulsive checking, orderliness, competence, and dutifulness to be correlated to the perception of halos and glare after mIOL implantation. 11 However, investigators did not attribute a score to each one of the Big Five personality traits, instead, identified four psychometric characteristics to have a significant impact on patient satisfaction. We also found higher neuroticism scores to be associated with difficulties focusing. A similar study concluded that the neurotic personalities reported a higher incidence of glare and difficulties with depth perception. 9 Neuroticism is the tendency to experience negative emotions and to cope poorly. Other studies have shown a correlation between neuroticism and a negative perception of self-health.4,5
In our study, patients in the trifocal group had significantly higher mean scores of conscientiousness and better UNVA and DCVA. However, we believe this did not influence our results as there were no differences in subjective QoV scores between both groups. Firstly, the subjective complaints that were associated with conscientiousness were some of the same associated with neuroticism and extroversion. Secondly, DCIVA and CNVA were similar between groups, and complaints of blurred vision, seeing double or multiple images and vision fluctuation among patients with lower conscientiousness scores (and therefore in the non-diffractive X-WAVE group) were most likely independent of a worse performance of the non-diffractive X-WAVE lens in DCNVA and UNVA.
There are many other factors that influence QoV and postoperative satisfaction, such as motivation and preoperative expectations, besides neuroadaptation, as we previously published.2,25 If a patient is dissatisfied postoperatively, the underlying causes (IOL tilt or decentration, opacification of the posterior capsule, refractive error, etc.) should be addressed before trying to justify complaints with the patient's personality. Nevertheless, this study shows that some personality traits are associated with a higher frequency of some visual complaints after mIOL surgery. Patient selection for mIOL should consider not only biometry, ophthalmologic findings, and daily activities, but also personality traits.11,26
This study has some limitations. Our sample is small and data have been collected only 6 months after surgery. We chose this time period to allow for neuroadaptation to visual symptoms to occur.2,25,27 There are also intrinsic limitations to the NEO-FFI-20 model, as stated by McAdams, there is an oversimplification of the constricts of personality, no consideration of human experience and disregard of human behavior and context. It can thus be considered a model to provide information about persons when one knows nothing else about them. 28 However, it is a simple instrument to use, easy for the patients to understand and applicable even in very busy Ophthalmology clinics.
Conclusion
To summarize, patients with lower scores of conscientiousness, extroversion and higher scores of neuroticism had a higher frequency of visual complaints after mIOL surgery. Lower conscientiousness, lower extroversion and higher neuroticism had a negative impact on the subjective frequency photic phenomena and thus are important factors to consider for patient selection for mIOL.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231176313 - Supplemental material for The influence of personality on the quality of vision after multifocal intraocular lens implantation
Supplemental material, sj-docx-1-ejo-10.1177_11206721231176313 for The influence of personality on the quality of vision after multifocal intraocular lens implantation by Rosa L. Pinheiro, Miguel Raimundo, João Q. Gil, Jorge Henriques, Andreia M. Rosa, Maria João Quadrado, Conceição Lobo and Joaquim N. Murta in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721231176313 - Supplemental material for The influence of personality on the quality of vision after multifocal intraocular lens implantation
Supplemental material, sj-docx-2-ejo-10.1177_11206721231176313 for The influence of personality on the quality of vision after multifocal intraocular lens implantation by Rosa L. Pinheiro, Miguel Raimundo, João Q. Gil, Jorge Henriques, Andreia M. Rosa, Maria João Quadrado, Conceição Lobo and Joaquim N. Murta in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors did not receive any financial support from any public or private sources
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.