
Abstract
Purpose
To analyse higher-order aberrations of an enhanced monofocal aspheric intraocular lens (IOL) in relation to the clinical outcome compared to a monofocal aspheric IOL.
Setting
Department of Ophthalmology, Charité – Universitätsmedizin Berlin, Germany
Design
Prospective, monocentric, controlled, non-randomized, two-armed study
Methods
After phacoemulsification, a total of 30 patients (60 eyes) were bilaterally implanted with either TECNIS Eyhance IOL model ICB00 (Johnson & Johnson Surgical Vision, Inc.) or TECNIS Monofocal 1-Piece IOL model ZCB00 (Johnson & Johnson Surgical Vision, Inc.) in 30 eyes each. Assessments were performed 1 and 3 months after surgery including refraction, uncorrected and best-corrected distance, intermediate and near visual acuity, defocus curves, contrast sensitivities under photopic, mesopic and mesopic conditions with glare, higher-order aberrations (HOAs) at pupil sizes of 5, 4, 3 and 2 mm and patient satisfaction.
Results
At 3-month follow-up, measurements of HOAs revealed significant higher negative internal and ocular primary spherical aberrations in the ICB00 group at pupil sizes of 5, 4, 3 and 2 mm. The ICB00 showed significant better results in intermediate and near visual acuity, but no difference in distance visual acuity. No significant difference was found in contrast sensitivities at any condition or spatial frequency. Spectacle independence was significant better without significant higher rates of dysphotopsia in the ICB00 group.
Conclusions
Higher negative spherical aberrations in the ICB00 group at all measured pupil sizes appear to lead to a superior clinical outcome in intermediate and near vision compared to the ZCB00 group without compromising contrast sensitivity or distance visual acuity.
Keywords
Introduction
Monofocal, multifocal, extended depth-of-focus (EDOF) and accommodative IOLs are, next to additional astigmatism correcting toric IOLs, principle options for lens replacement in modern cataract surgery.1–5 Monofocal IOLs with a single focal point are the most commonly implanted IOLs and are effective in restoring vision at one distance. They are relatively inexpensive and rarely cause photopic phenomena such as halos and glare. 1 Increased spectacle independence can be achieved with multifocal IOLs based on either diffractive designs, refractive designs or a combination of both. Diffractive designs split the light at diffraction grooves. Refractive designs work with different refractive power zones.6–10 On the other hand, multifocal IOLs can cause glare, halos, a lower contrast sensitivity or unsatisfactory intermediate vision.1,10–13 Due to the growing number of computer workstations, tablets and smartphones, the need for useful vision at an intermediate distance is increasing. The ESCRS Functional Vision Working Group 2020 came to the conclusion, that the maintenance of functionality at all distances should be the main goal and main indicator for cataract surgical intervention in the future. 14 EDOF IOLs contribute to this intentions with an extended depth-of-focus. 15 Nevertheless, EDOF IOLs also lead to dysphotopsia, to reduce them, neural adaptation and accurate patient selection is required.2,16 The enhanced monofocal TECNIS Eyhance IOL model ICB00 has been developed to overcome the issues of improving intermediate vision, minimizing the negative side effects of multifocality. 17 In this clinical study, we investigated the optical quality in relation to the clinical outcome of the enhanced monofocal ICB00 IOL in comparison to the monofocal TECNIS Monofocal 1-Piece IOL model ZCB00. To investigate if and how the ICB00 IOL can overcome the aforementioned issues was of particular interest.
Methods
Study design
In this prospective, monocentric, controlled, non-randomized, two-armed study, 60 eyes of 30 patients (15 patients in each group) were examined. The ICB00 IOL and the ZCB00 IOL were bilaterally implanted in 15 patients each. The surgeries were performed from July 2020 to August 2021 at the Department of Ophthalmology, Charité - Universitätsmedizin Berlin, Germany.
Ethics
Before patient enrollment, the study protocol (trial registration EA4/252/19) was approved by the ethics committee of the Charité - Universitätsmedizin Berlin, Germany. Written consent was obtained from all patients and the study was conducted according to the tenets of the Declaration of Helsinki.
Inclusion and exclusion criteria
Inclusion criteria were a minimum age of 18 years, a bilateral cataract requiring surgery, refraction target emmetropia and healthy eyes with an expected postoperative best-corrected distance visual acuity (BCVA) of Snellen 20/20 (0.0 LogMAR) in both eyes.
Exclusion criteria were an irregular or expected postoperative astigmatism of over 0.75 D, dilated pupil diameter of under 5 mm, any ocular trauma, surgery, or comorbidities reducing visual outcome.
IOL device description and lens choice
We compared the enhanced monofocal aspheric TECNIS Eyhance IOL model ICB00 (Johnson & Johnson Surgical Vision, Inc.) and the monofocal aspheric TECNIS Monofocal 1-Piece IOL model ZCB00 (Johnson & Johnson Surgical Vision, Inc.).
Both lenses are based on refractive technology, have the same overall geometry and are visually indistinguishable. The ICB00 IOL has a continuous, higher-order aspherical surface with an increase in refractive power from the lens periphery to the lens center to improve intermediate vision while maintaining distance vision. The ZCB00 IOL has a spherical aberration (SA) of −0.27 µm, the ICB00 IOL seems to have a similar amount of SA to compensate the corneal spherical aberrations. 18 The aspheric design of the anterior surface of the ZCB00 IOL reduces spherical aberrations to near zero. 19
The patients were informed of the advantages and disadvantages of the IOLs and were able to choose between both IOL types.
Surgical technique
Preoperative biometry was performed using IOLMaster 700 (Carl Zeiss Meditec AG) and IOL diopter power was calculated using the Barrett Universal II, Haigis and SRK/T formula to target emmetropia (± 0.5 D) for all eyes in this study.
Surgeries were performed by the same expert surgeon (E.B.) with 14 days between first and second eye surgery under peribulbar anesthesia using the standard surgical procedure with a 2.2 mm steep-axis clear corneal incision. Postoperatively, patients received eyedrops and ointment containing dexamethasone, neomycin sulfate and polymyxin-B-sulfate.
Endpoints and assessments
All assessments were performed one and three months after second eye surgery, except for the defocus curve, measurements of higher-order aberrations, and the patient satisfaction measurements, which were taken only at three-month follow-up. All patients were examined by the same examiner (L.S.).
In addition to objective refraction (Auto Kerato-Refractometer KR-8900, Topcon), the subjective refraction was recorded with the maximum-plus-technique, as strongly recommended in the instructions for use of the ICB00 IOL. This is because autorefractometers may not measure postoperative refraction optimally in patients with the ICB00 IOL.18,20
Postoperative visual acuities were measured under photopic conditions with 100% contrast using Early Treatment Diabetic Retinopathy Study (ETDRS) Charts designed for the following distances: 4 m (far), 66 cm (intermediate) and 40 cm (near) with an illuminated ETDRS Standardized Viewer Model No. ESV1500 (GOOD-LITE).
Primary endpoints were monocular and binocular uncorrected distance (UDVA), intermediate (UIVA) and near visual acuity (UNVA), as well as best-corrected distance (BCVA), intermediate (BCIVA) and near visual acuity (BCNVA).
The following endpoints were secondary: Monocular and binocular Functional Acuity Contrast Test (F.A.C.T.) contrast sensitivities (Functional Vision Analyser, Stereo Optical) were measured best-corrected under photopic (85 cd/m2), mesopic (3 cd/m2) and mesopic conditions (3 cd/ m²) with glare (1 Lux) at the spatial frequencies of 1.5, 3, 6, 12 and 18 cycles per degree (cpd). Higher-order aberrations were measured using wavefront aberrometry (iTrace, Tracey Technologies) under mydriasis of 5 mm pupil size induced by phenylephrine tropicamide eye drops. Values for pupils measuring 4, 3 and 2 mm pupil size was obtained through post-examinational adjustment of the pupil size.
Monocular and binocular corrected distance defocus curves were conducted in 0.5 D steps from + 1.5 D to −4.0 D defocus under the visual acuity measurement condition at 4 m. Patient satisfaction was assessed with the National Eye Institute Refractive Error Quality of Life-42 (NEI-RQL-42) questionnaire.
Statistical analysis
Data analysis was carried out using the software SPSS Statistics version 25 for Windows (IBM).
All dependent variables were visually inspected for normal distribution in each group using histograms. As the histograms were not skewed and were free of outliers, parametric tests are appropriate. Because the mean age was different in the study groups, the linear generalized estimating equation (GEE) models, that were used for analysing binocular data (analysis at patient level), and the general linear models, used for analysing monocular data (analysis at eye level), were adjusted with respect to age. The robust variance estimator of the GEE models accounts for possible correlations between the left and right eye in the analysis of binocular data.
A post-hoc power analysis demonstrates that the t-test for independent samples has a power greater than 80% if the mean difference of monocular UIVA between the ZCB00 IOL and ICB00 IOL is 0.134 LogMAR or more and the sample size is n1 = 13 and n2 = 14 patients (pairs of eyes) with the ZCB00 IOL and ICB00 IOL respectively. We assume a common standard deviation of σ = 0.139 for both lens types and a Pearson correlation of r = 0.334 between left and right eye for monocular UIVA. The two-sided level of significance is α = 0.05. The power analysis was performed using the procedure MTT0U-1 of nQuery version 8.7.2.0.
Results
A total of 60 eyes of 30 patients was assigned to this study, each group comprised 15 patients with the same bilaterally implanted IOL (ICB00 or ZCB00). Three patients dropped out after the one-month-follow-up examination because of refusal (one ZCB00 patient) or due to surgery independent acute health problems (one ZCB00 and one ICB00 patient), so that a data set was available for 13 ZCB00 patients and 14 ICB00 patients. All IOLs were implanted in the capsular bag and all surgical procedures were uneventful. One adverse event (cystoid macular edema) occurred in each group at the one-month-follow-up, both were treated directly and healed without complications or any subsequent visual impairment. No clinically significant posterior capsular opacification was detected in any patient at one and three months postoperatively.
Patient characteristics
Patient Characteristics are displayed in Table 1. Except for the preoperative monocular BCVA and SE, no significant difference was observed. The mean implanted IOL power was 23.55 ± 2.41 D in the ZCB00 group and 21.10 ± 4.69 D in the ICB00 group, without statistically significant difference (p = 0.091).
Preoperative patient characteristics.
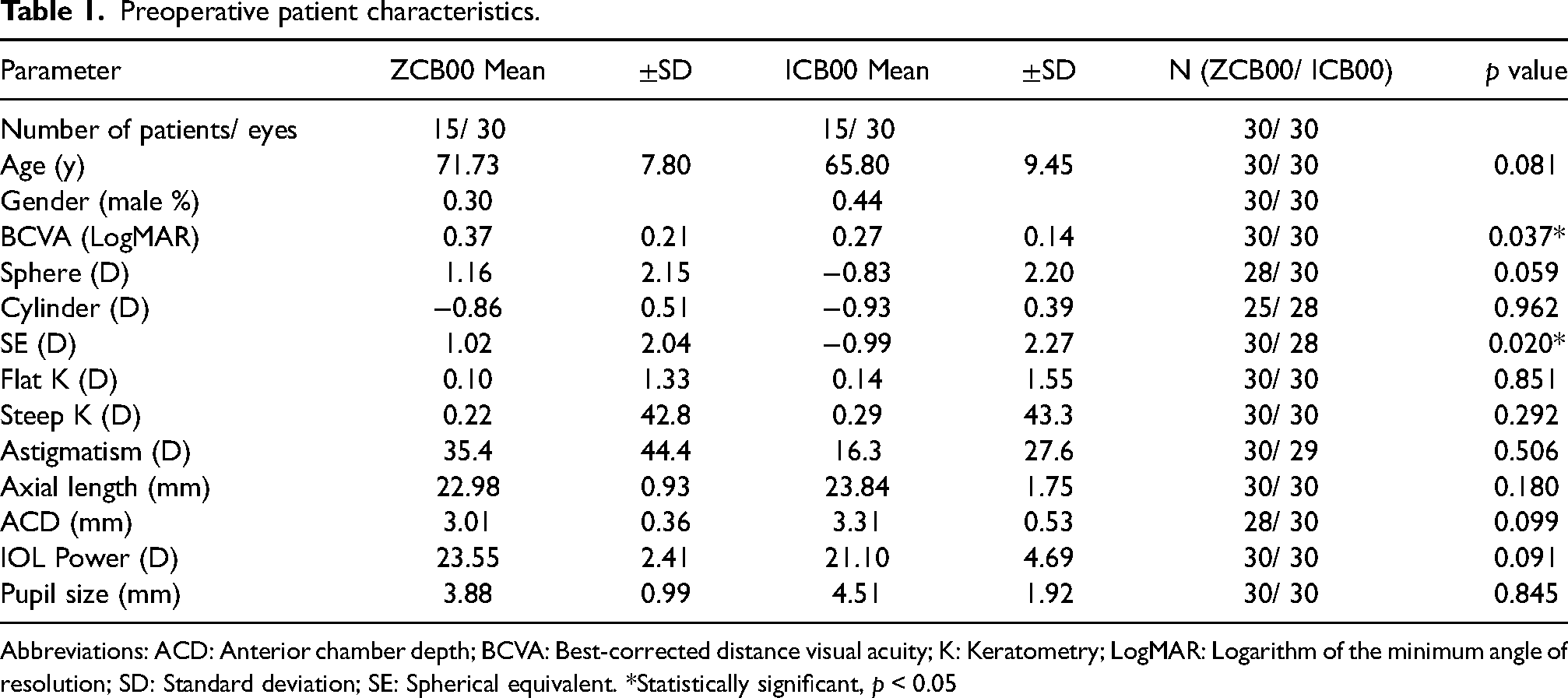
Abbreviations: ACD: Anterior chamber depth; BCVA: Best-corrected distance visual acuity; K: Keratometry; LogMAR: Logarithm of the minimum angle of resolution; SD: Standard deviation; SE: Spherical equivalent. *Statistically significant, p < 0.05
The preoperative corneal HOAs measured at a pupil diameter of 5, 4, 3 and 2 mm are shown in Table 2 and reveal no statistically significant difference.
Preoperative corneal HOAs.
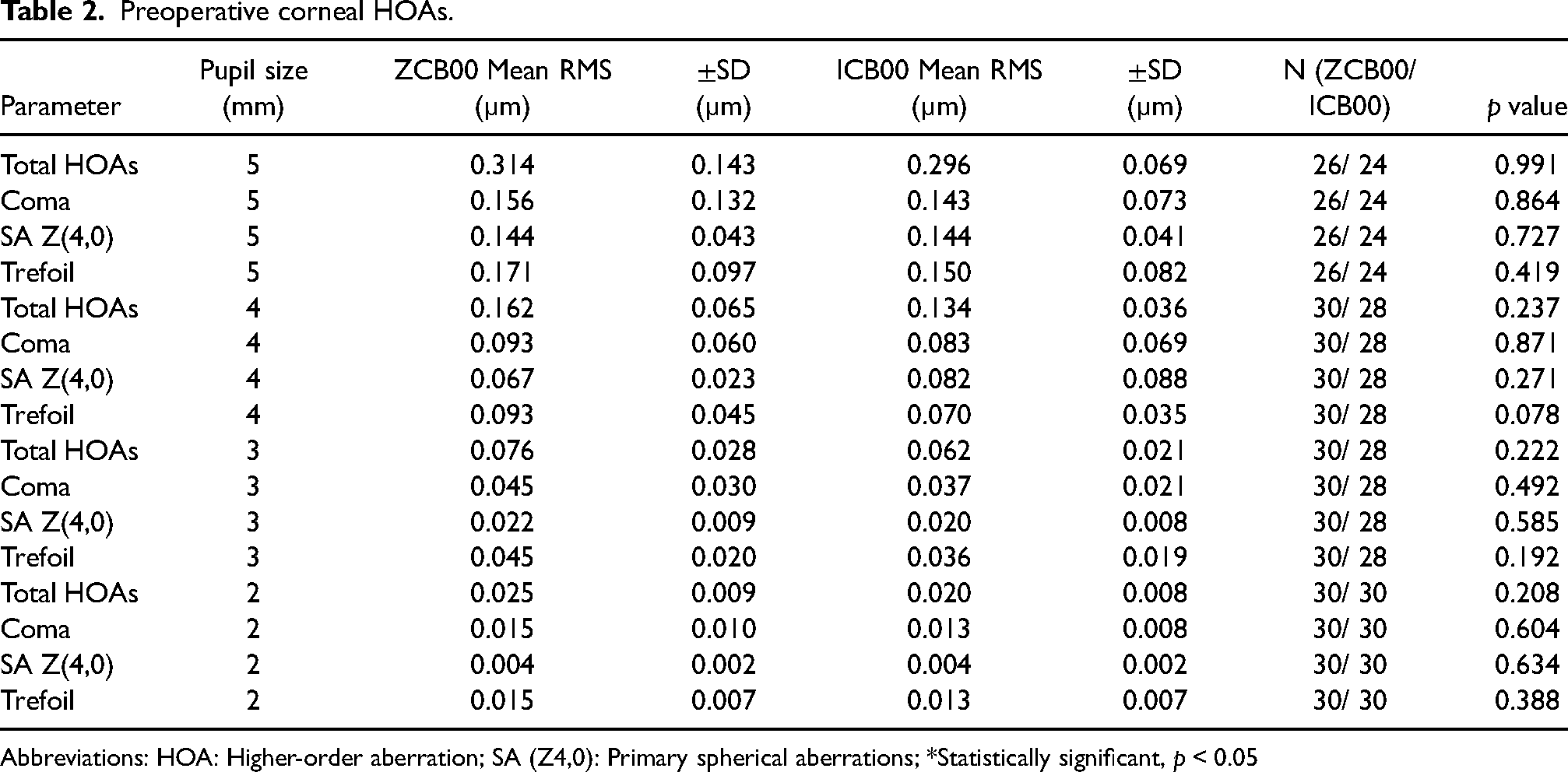
Abbreviations: HOA: Higher-order aberration; SA (Z4,0): Primary spherical aberrations; *Statistically significant, p < 0.05
Refraction and visual acuity
Table 3 presents the subjective refraction and visual acuities at three months. The mean postoperative spherical equivalent (SE) of −0.29 ± 0.48 D in the ZCB00 group and −0.24 ± 0.35 D in the ICB00 group did not differ statistically significantly (p = 0.55). Monocular and binocular UDVA and BCVA did not differ significantly. At monocular and binocular intermediate (UIVA and BCIVA) and near distances (UNVA and BCNVA), the ICB00 group showed significantly better results.
Subjective refraction and visual acuity at 3-month-follow-up.
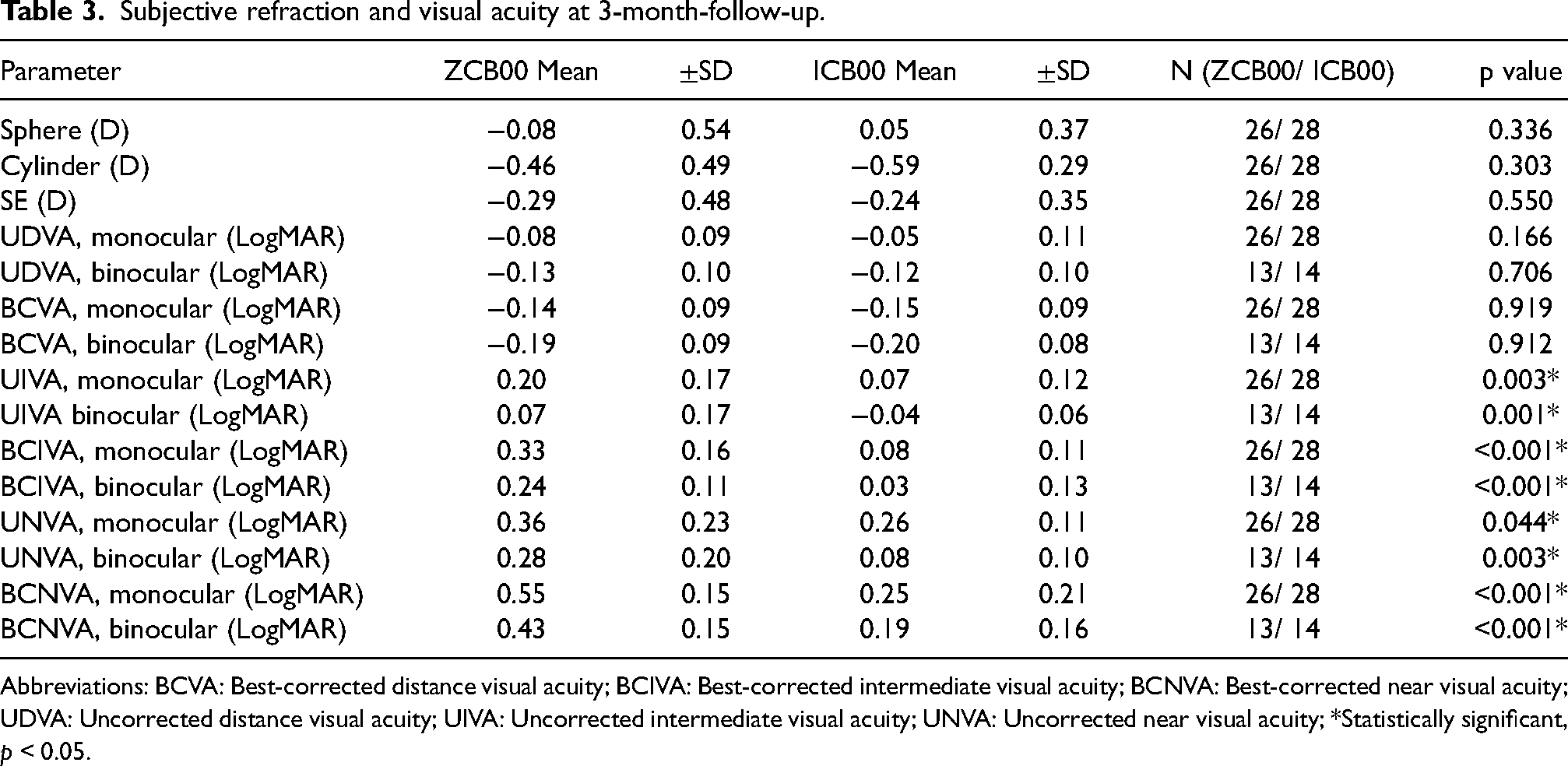
Abbreviations: BCVA: Best-corrected distance visual acuity; BCIVA: Best-corrected intermediate visual acuity; BCNVA: Best-corrected near visual acuity; UDVA: Uncorrected distance visual acuity; UIVA: Uncorrected intermediate visual acuity; UNVA: Uncorrected near visual acuity; *Statistically significant, p < 0.05.
Defocus curves
Both defocus curves (Supplemental Figure 1) reached their visual acuity peaks at 0.0 D defocus and did not differ at far distance. With the beginning of negative defocus, there was a plateau with better visual acuity results in the ICB00 group.
The monocular defocus curve showed between −1.0 D to −2.0 D and −3.0 D to −3.5 D significantly better vision results in the ICB00 group.
The binocular defocus curve displayed statistically significant better visual acuity results in the ICB00 group between −1.0 D to −3.5 D.
Contrast sensitivities
Concerning the monocular and binocular best-corrected measured contrast sensitivities both groups showed comparable results under photopic (Supplemental Figure 2), mesopic (Supplemental Figure 3) and mesopic conditions with glare (Supplemental Figure 4) over all spatial frequencies without any statistically significant difference.
Higher-order aberrations
The HOAs of 5, 4, 3 and 2 mm displayed no statistically significant differences of corneal HOAs between both groups (Figure 1). However, significantly greater negative primary internal spherical HOAs (SA Z(4,0)) were found in the ICB00 group (Figure 2) leading to significantly higher and negative ocular SA Z(4,0) (Figure 3). The internal and ocular SA Z(4,0) were decreasing from larger to smaller pupil sizes. The ocular SA Z(4,0) of the ZCB00 group were near zero µm at all pupil sizes.
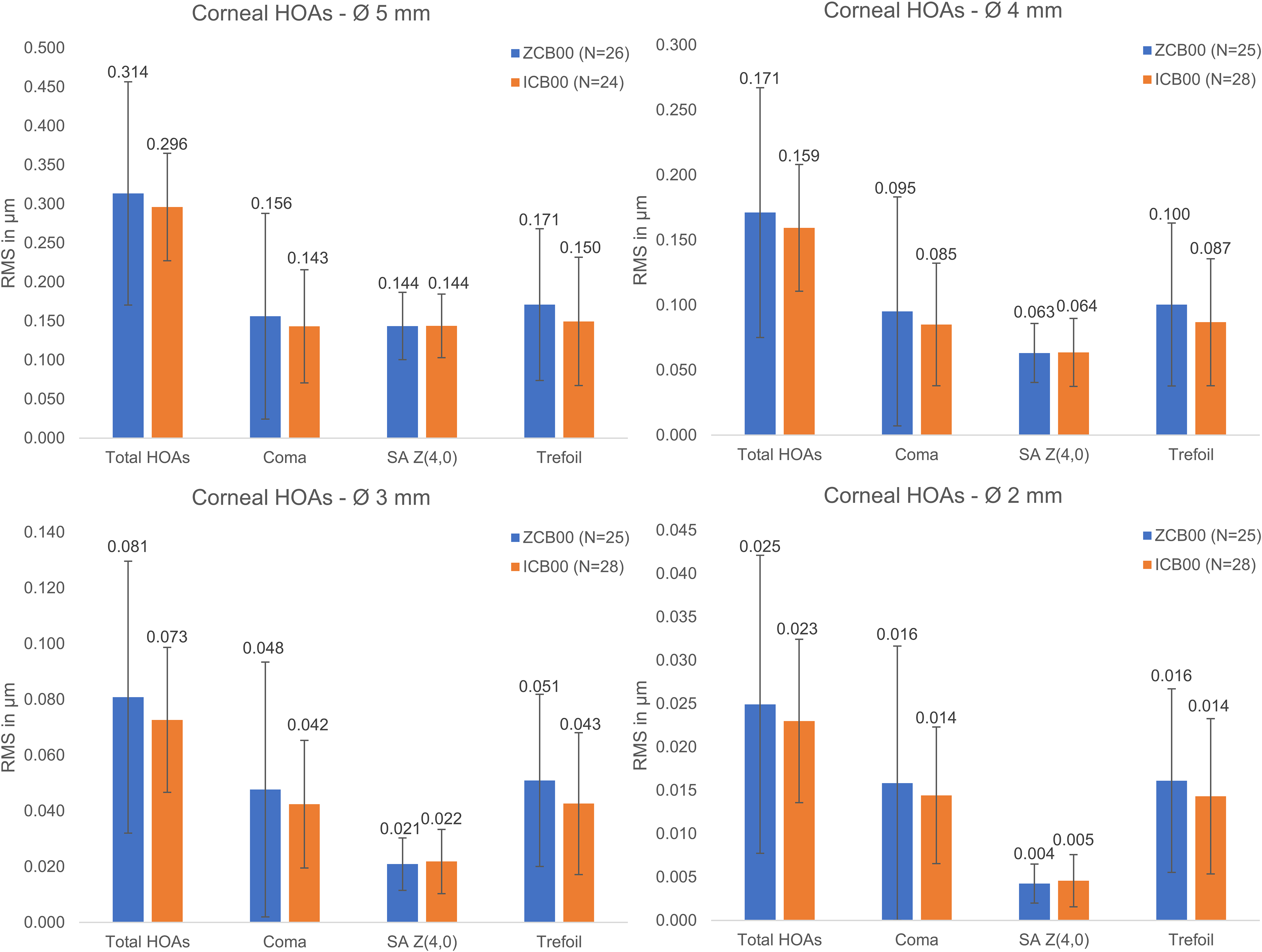
Mean corneal HOAs at different pupil diameters ± sd at 3-month-follow-up. Abbreviations: HOA: Higher-order aberration; RMS: Root mean square; SA Z(4,0): Primary spherical aberration; *Statistically significant, p < 0.05.
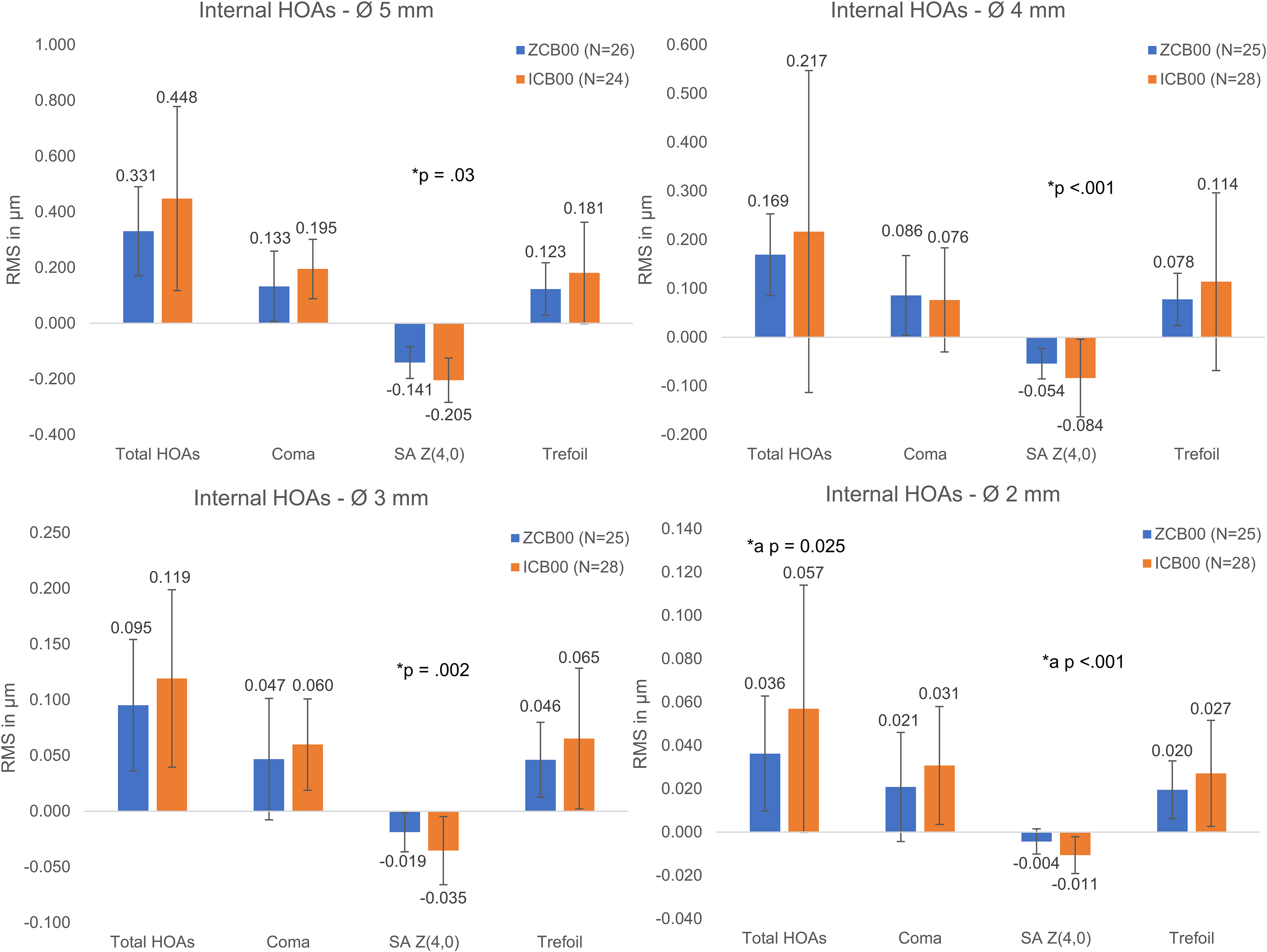
Mean internal HOAs at different pupil diameters ± sd at 3-month-follow-up. Abbreviations: HOA: Higher-order aberration; RMS: Root mean square; SA Z(4,0): Primary spherical aberration; *Statistically significant, p < 0.05; *a: Statistically significant influence of the IOL-type and the age.
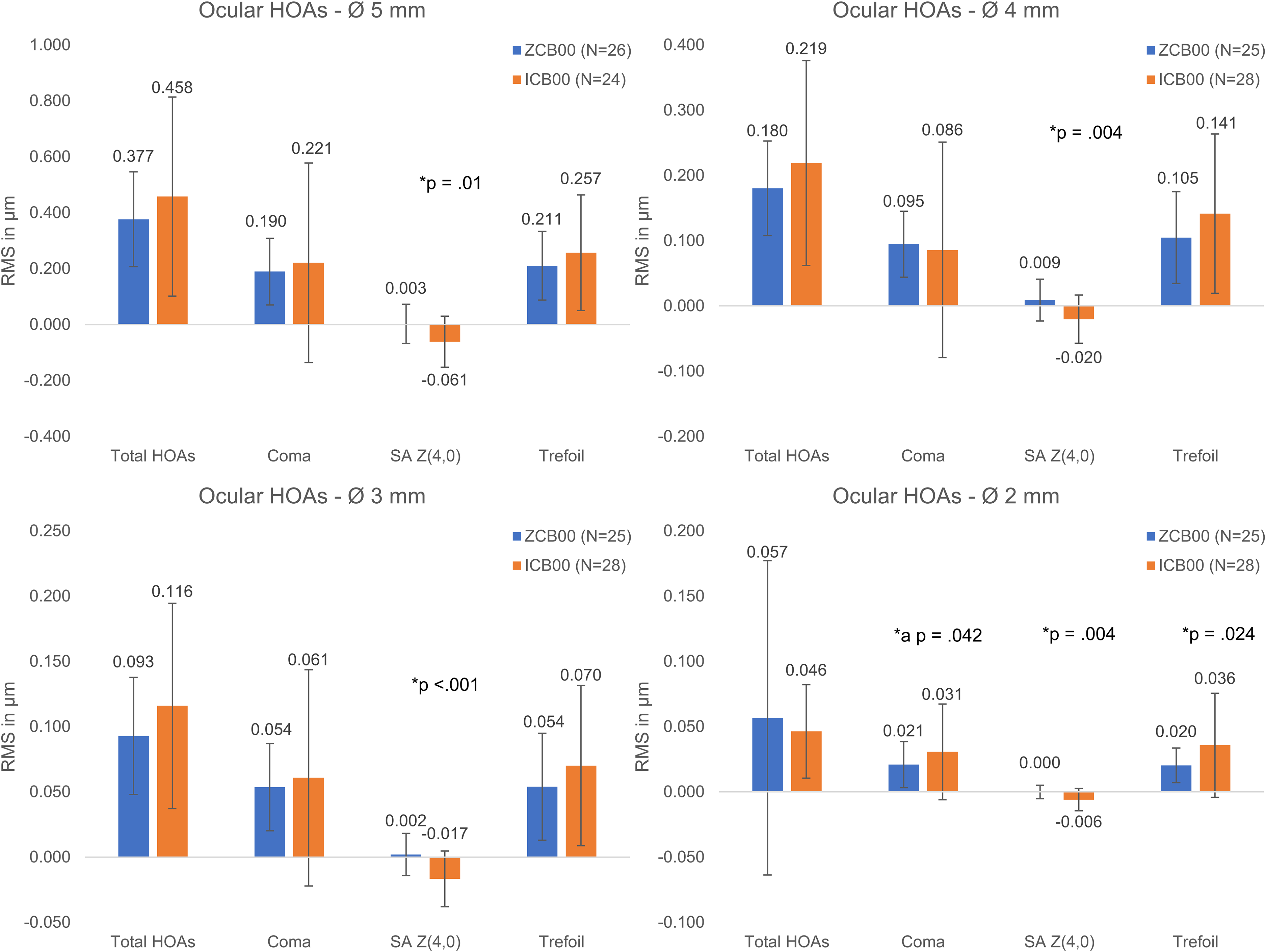
Mean ocular HOAs at different pupil diameters ± sd at 3-month-follow-up. Abbreviations: HOA: Higher-order aberration; RMS: Root mean square; SA Z(4,0): Primary spherical aberration; *Statistically significant, p < 0.05; *a: Statistically significant influence of the IOL-type and the age.
At a pupil diameter of 2 mm the ICB00 group showed also significantly higher total internal HOAs as well as higher ocular coma and trefoil.
Furthermore, secondary (sixth-order) internal spherical HOAs (SA Z(6,0)) were significantly higher at 4, 3 and 2 mm pupil diameter (Supplemental Table 1) in the ICB00 group. At 5 mm, there was no statistically significant difference between the groups in SA Z(6,0).
Patient satisfaction
The analysis of NEI-RQL-42 (Supplemental Figure 5) displayed significant better scores for dependence on correction, expectations, diurnal fluctuation, and glare in the ICB00 group and no significant differences in the scores for clarity of vision, near vision, far vision, activity limitations, worry, suboptimal correction, appearance and satisfaction with correction.
Six ZCB00 patients (46.2%) and ten ICB00 patients (71.4%) never or sometimes needed glasses when reading something short. Two ZCB00 patients (15.4%) and 9 ICB00 patients (64.3%) never or sometimes needed glasses when reading something long.
The glare-score in the NEI-RQL-42-Figure consists of two items (17 and 38b).
Two ZCB00 patients (15.38%) and two ICB00 patients (14.29%) reported halos. The mean score of the perception of halos or starbursts (item 17) differed not significantly (ZCB00 = 88.46 ± 24.19; ICB00 patients = 91.07 ± 27.04; p = 0.329).
Eight ZCB00 patients (61.54%) and two ICB00 patients (14.29%) reported glare and the average score of the appearance of glare (item 38b) showed significantly better scores in the ICB00 group (ZCB00 = 44.23 ± 41.19; ICB00 = 89.29 ± 27.24; p = 0.002).
Discussion
The enhanced monofocal and refractive ICB00 IOL provides a continuous power increase from the periphery to the center of the higher-order aspheric anterior surface. It consists of the same material and has same overall dimensions and geometry as the monofocal aspheric and refractive ZCB00 IOL. 18 To the best of our knowledge, no information about the modified SA was published by the manufacturer. The pupil diameter can have an influence on the SA of the IOL, as Greve et al. showed in their study with a refractive EDOF IOL based on SA using iTrace. 21 In this study we investigated the HOAs at different pupil diameters in relation to the clinical outcome of an enhanced monofocal IOL compared to a monofocal IOL.
Contact profilometry measurements of Tognetto et al. demonstrated a minimal central deviation for the ICB00 IOL when comparing it to the monofocal AAB00 and ZCB00 IOL. 22 In vitro measurements of Vega et al. could show an additional power of 0.5 D in the central 2 mm zone of the 20.0 D ICB00 IOL. This is being associated with higher negative SA Z(4,0) for pupil diameters less than 3.5 mm and similar SA Z(4,0) for larger pupil diameters in comparison to the ZCB00 IOL. 23 In our study, we did not only found significant higher SA Z(4,0) for 3 and 2 mm but also for 5 and 4 mm pupil size. Corresponding to our results Schmid et al. found a significant increase in negative SA Z(4,0) in the ICB00 IOL (22.0 D) and slightly increased SA Z(10,0) using a Shack-Hartmann-Sensor in an in situ model eye with an aperture of 5.8 mm. The increase of negative phase values were measured in the central 1 mm of the lens while the periphery of the lens had positive phase values. A transition zone was measured between these areas. 24 It is difficult to compare in vivo and in vitro studies because in vitro studies do not take into account the influence of different human corneas or other parts of the eye. In our setting, we used a ray-tracing aberrometer. The in vitro studies mentioned before used a Hartmann-Shack aberrometer. Pilger et al. found comparable ZCB00 IOL HOAs to our results also measured in vivo by using the iTrace. 25 Alio et al. found significant differences in HOAs between the ICB00 IOL and the monofocal spherical AcrySof SA60AT and other non-monofocal IOLs at pupil diameters of 4 and 3 mm measured in vivo using the pyramidal wavefront sensor (PWS)-based aberrometer. They also displayed a significant difference in the HOAs between 4 mm and 3 mm pupil diameter in the ICB00 group. 26 Nanavaty et al. showed statistically significant differences in total and internal spherical aberrations between the ICB00 IOL and the aspheric monofocal RayOne IOL measured in vivo using the iTrace. 27
Regarding other studies, the ICB00 IOL achieved significant superior monocular and binocular UIVA and BCIVA without significant differences in UDVA and BCVA in comparison to the ZCB00 IOL.17,18,28–30 Contrary to our study, Mencucci et al. did not find any significant differences in monocular and binocular UNVA and BCNVA. 17 Corresponding to our study, Corbelli et al., Kang et al., Yangzes et al. and Huh et al. showed significant differences in UNVA, Corbelli et al. also found significant differences in BCNVA.29–32
While Mencucci et al., Corbelli et al. and Unsal et al. displayed significant differences at −1.0 D and −1.5 D in binocular defocus curves of the ICB00 IOL in comparison the ZCB00 IOL, Huh et al. (−1.0 D to −3.0 D) and our study found a wider range of significant differences.17,28–30 Consistent with our results the binocular ICB00 IOL defocus curves of Eguileor et al., Corbelli et al., Auffarth et al., Mencucci et al. and Lee et al. dropped below 0.2 LogMAR between −1.5 D and −2.0 D of defocus.17,18,30,33,34
In accordance with our results, other controlled studies did not find any significant differences in postoperative contrast sensitivities under photopic, mesopic and glare condition between the two IOLs.17,18,28,30 Vega et al. displayed slightly worse modulation transfer function (MTF) scores at distance vision for pupils from 2 to 3 mm in in vitro measurements for the ICB00 IOL in comparison to the ZCB00 IOL. 23 Schmid et al. concluded from their in vitro study that in large pupils the periphery of the lens aims to preserve contrast sensitivity. 24
The superior UNVA results of the ICB00 group resulted in a slightly higher mean patient satisfaction score regarding near vision, however, this difference did not reach statistical significance. In order to achieve a better subjectively perceived near vision, the lens seems to need even more central power. 23 Nevertheless, our results in better ICB00 IOL visual acuities in near and intermediate distances were reflected in a significant better result in subjective perception of the dependance on correction as described in other studies.17,30
Several studies did not report any significant differences between the ICB00 IOL and the ZCB00 IOL regarding the occurrence of halos or starburst consistent to our results.17,18,23,28–30,35
Surprisingly, we found in our study a significant lower occurrence of glare in the ICB00 group, while other studies displayed no significant differences.17,18,28–30 However, our contrast sensitivity measurements under mesopic conditions with glare showed no differences between the groups.
Compared to EDOF IOLs in other studies, the ICB00 IOL seems to achieve inferior spectacle independence.21,25,30,34 Lee et al., Corbelli et al. and Jeon et al. showed comparable UDVA, BCVA, UIVA and superior UNVA in the EDOF cohorts.30,34,36 The EDOF IOLs led to increased occurrence of halos and glare at similar contrast sensitivities.21,25,30,34
Our study limitations include the small sample size and the different mean age. A longer follow-up would be preferable because of neuro-adaption. 37 The age difference was tested not statistically significant and additionally age adjusted tests were used to show the resilience of the group data. A randomization would have led to better comparability, but our study thus reflects the situation in real life regarding the patients IOL choice.
In conclusion the enhanced monofocal ICB00 IOL achieved superior outcomes at intermediate and near distances providing higher spectacle independence without compromising far vision. Ray-tracing aberrometry in patients with the ICB00 IOL showed significantly higher negative spherical aberrations in pupil sizes of 5, 4, 3 and 2 mm without causing any significant differences in total ocular HOAs in comparison to the aspheric monofocal ZCB00 IOL. In this study we could demonstrate this optical feature of the ICB00 IOL, previously known form in vitro optical bench studies, to the best of our knowledge for the first time in a clinical setting. Although the ICB00 IOL does not compensate the spherical aberrations of the cornea to the same extent as the ZCB00 IOL, this does not compromise the visual function and does not provoke other detectable optical side effects. The enhanced monofocal ICB00 IOL seems to be a good alternative to monofocal IOLs, especially in patients who desire a little higher spectacle independence. To finally assess the clinical value of monofocal IOLs with enhanced optics, such as the ICB00 and other IOL models with comparable optics from other manufacturers, further larger clinical studies are necessary, especially to be able to differentiate the indications for ICB00 and EDOF IOLs more precisely in the future.
Supplemental Material
sj-tif-1-ejo-10.1177_11206721221134171 - Supplemental material for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL
Supplemental material, sj-tif-1-ejo-10.1177_11206721221134171 for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL by Lucas Nicola Steinmüller, Daria Greve, David Rua Amaro, Eckart Bertelmann and Christoph von Sonnleithner in European Journal of Ophthalmology
Supplemental Material
sj-tif-2-ejo-10.1177_11206721221134171 - Supplemental material for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL
Supplemental material, sj-tif-2-ejo-10.1177_11206721221134171 for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL by Lucas Nicola Steinmüller, Daria Greve, David Rua Amaro, Eckart Bertelmann and Christoph von Sonnleithner in European Journal of Ophthalmology
Supplemental Material
sj-tif-3-ejo-10.1177_11206721221134171 - Supplemental material for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL
Supplemental material, sj-tif-3-ejo-10.1177_11206721221134171 for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL by Lucas Nicola Steinmüller, Daria Greve, David Rua Amaro, Eckart Bertelmann and Christoph von Sonnleithner in European Journal of Ophthalmology
Supplemental Material
sj-tif-4-ejo-10.1177_11206721221134171 - Supplemental material for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL
Supplemental material, sj-tif-4-ejo-10.1177_11206721221134171 for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL by Lucas Nicola Steinmüller, Daria Greve, David Rua Amaro, Eckart Bertelmann and Christoph von Sonnleithner in European Journal of Ophthalmology
Supplemental Material
sj-tif-5-ejo-10.1177_11206721221134171 - Supplemental material for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL
Supplemental material, sj-tif-5-ejo-10.1177_11206721221134171 for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL by Lucas Nicola Steinmüller, Daria Greve, David Rua Amaro, Eckart Bertelmann and Christoph von Sonnleithner in European Journal of Ophthalmology
Supplemental Material
sj-docx-6-ejo-10.1177_11206721221134171 - Supplemental material for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL
Supplemental material, sj-docx-6-ejo-10.1177_11206721221134171 for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL by Lucas Nicola Steinmüller, Daria Greve, David Rua Amaro, Eckart Bertelmann and Christoph von Sonnleithner in European Journal of Ophthalmology
Supplemental Material
sj-docx-7-ejo-10.1177_11206721221134171 - Supplemental material for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL
Supplemental material, sj-docx-7-ejo-10.1177_11206721221134171 for Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL by Lucas Nicola Steinmüller, Daria Greve, David Rua Amaro, Eckart Bertelmann and Christoph von Sonnleithner in European Journal of Ophthalmology
Footnotes
Acknowledgements
E.B. and C.v.S. contributed equally to this work and should therefore be regarded as equivalent authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.