
Abstract
It concerns three siblings (two 28 year old twin boys and a 25 year old woman) who presented a previous history of rupture of eyeball in one eye and very poor vision in the other. At the first ophthalmoscopic and instrumental evaluation, three patients presented with bluish sclera and keratoglobus in the intact eye. A genetic analysis with whole exome sequencing was then performed on the three siblings, identifying a biallelic variant of the PRDM5 gene that led to the diagnosis of Brittle Cornea Syndrome (BCS), a rare autosomal recessive disorder characterized by corneal thinning and blue sclera. To preserve the only intact eye from possible breakage, the three siblings were trained in using protective measures (polycarbonate goggles etc.) to carry out close monitoring of symptoms and were asked to continue with follow-up visits for ocular and systemic diseases associated with BCS. Given the poor best corrected visual acuity achievable with glasses and contact lenses, penetrating keratoplasty was performed, achieving good visual acuity maintained in the 2-year follow-up in two of the three patients. Knowledge of this pathology and its clinical manifestations is essential for early diagnosis and correct management of this rare but very debilitating pathology. To our knowledge, this is the first case series of BCS reported in an Albanian population.
Introduction
Brittle Cornea Syndrome (BCS) is a rare autosomal recessive connective tissue disorder with ocular manifestations often associated with extraocular involvement; corneal thinning, blue sclera, keratoconus, keratoglobus, high myopia and irregular corneal astigmatism are identified.1,2 It is precisely the ocular manifestations that have the greatest impact on the patient's life: all these manifestations seriously compromise vision and the progressive thinning of the corneal stroma predisposes to corneal ruptures even from minor trauma.1–6 Indeed when the cornea becomes particularly thin it is unable to withstand normal biomechanical stresses and spontaneous rupture can occur.2,3 Extra-ocular manifestations include deafness, joint hypermobility, skin hyperelasticity, arachnodactyly, developmental dysplasia of the hip and bone fragility.2,5,6 Cundy et al. identified the fact that parents with BCS have a bone fragility phenotype with a tendency to multiple recurrent fractures, osteopenia, lower z-scores and reduced cortical porosity on bone biopsy compared to parents with single allelic mutation in the ZNF469 gene. 6 We report the clinical findings of an Albanian family with BCS and the management of such conditions, by reviewing the available literature.
Findings
Case 1
25-year-old Albanian female patient was sent to our hospital for diagnostic tests. The patient presented a history of a previous rupture of the left eyeball as a consequence of a minor ocular trauma while living in Albania and orbital exenteration was the operation performed. The right eye (RE) at a first ophthalmoscopic evaluation presented a bluish sclera, thin cornea, and optically empty anterior chamber (AC) (Figure 1(a)). The RE best corrected visual acuity (BCVA) was 20/200. A topography (Figure 1(b)) and an optical coherence tomography (OCT) Visante of the anterior segment (Figure 1(c)) were then performed which revealed a generalized thinning of the cornea with Thinnest Point 157 µm, AC Depth of 3.84 mm, K-Max 73.0 D. From a systemic point of view, the ocular manifestations were associated with articular hyperlaxity and arachnodactyly. There was a concern for Osteogenesis Imperfecta (type I) because of the thin cornea and bluish sclera. The patient was sent for genetic analysis, a whole exome sequencing was performed and variant c.974delG (p. Cys325LeufsX2) was identified in PRDM5 gene, thus diagnosing Brittle Corneal Syndrome. Given the poor BCVA that can be reached in RE with glasses and contact lenses, penetrating keratoplasty (PK) was performed in RE (Figure 1(d)) with all the necessary precautions suggested in literature in suturing such a thin cornea. 4 The donor cornea was set with 10.0 nylon radial interrupted sutures; sutures were deeply taken in the donor tissue while long suture bites were set in the recipient cornea in order to optimize the sealing: -a secure graft-host interface was created, focal stress on the marginal tissue avoided and “cheese-wiring” of the sutures reduced. The following knots rotation was made with extreme caution to avoid intraoperative corneal rupture in such fragile tissue. The immediate post-operative period was free of complications. The patient was instructed to use protective polycarbonate glasses, and forced to adopt lifestyle changes to reduce any ocular trauma. The post-surgical follow-up included six-monthly checks with evaluation of BCVA, corneal topography (Figure 1(e)) anterior segment OCT Visante (Figure 1(f)) and pachymetry. The last two-year follow up confirms a stability of the topographic and pachymetric findings and the maintenance of a BCVA of 20/30 (Figure 1).

Pre- and post-operative findings of case 1. (a) slit-lamp shows a clear but thin and ectatic cornea confirmed by topography (b) and AS-OCT (c). After performing a PKP, topographic maps (e) shows an irregular astigmatism due to the corneal suture (d, f).
Case 2 and 3
A few months after PK's intervention (Case 1), the woman's two brothers (28-year-old twins) arrived at our department for the clinical evaluation of BCS. Both twin brothers presented a history of a previous rupture of the left eyeball, not promptly treated, which had hesitated in phthisis bulbi. Case 2 on split-lamp examination presented a bluish sclera in the RE, thin cornea and optically empty anterior chamber, BCVA 20/200. A corneal topography and an anterior segment OCT Visante (Figure 2(b)) were then performed (Figure 2(a)) again showing a generalized thinning of the cornea with Thinnest Point 151 µm, AC Depth of 5.22 mm, K-Max 88.6 D. In Case 3 the anterior segment exam of the RE showed, in addition to the bluish sclera and thin cornea, peripheral anterior synechiae, irido-lenticular adhesions, BCVA light perception, IOP 31 mmHg, C/D ratio 0.9 and a generalized corneal thinning with anterior segment OCT Visante (Figure 3(a)). From a systemic point of view, both twin brothers presented joint hyperlaxity and arachnodactyly. They were then subjected to genetic analysis, Whole Exome Sequencing (WES) was performed and variant c.974delG (p.Cys325LeufsX2) was identified in PRDM5 gene, in both siblings, so BCS was confirmed. Both were then given the usual instructions in adopting changes in their lifestyle to minimize the opportunities for ocular trauma. Also in these cases, given the low BCVA, PK was performed in RE (in Case 3, after lowering the IOP up to 17 mmHg using oral carbonic anhydrase inhibitor, 250 mg three times daily for 3 days). At 2-year follow-up, in case 2, a stability of the topographic and pachymetric picture is confirmed, with IOP of 15 mmHg and the maintenance of a BCVA of 20/30; in case 3, BCVA was 20/200 with an IOP of 24 mmHg in topical therapy (fixed combination of brinzolamide and timolol eyedrops two times daily). All the 3 siblings were included in an integrated long-term follow-up process in such a way that they were encouraged to continue with follow-up visits and regular screenings for late-onset hearing loss (Figures 2 and 3).

Pre-operative topographic (a) and AS-OCT findings (b) of case 2 that shows an extremely curve and thin cornea that return to a normal topographic (c) and AS-OCT (d) aspect after PKP.

(a) Pre-operative AS-OCT findings of case 3, showing peripheral anterior synechiae with extensive irido-lenticular adhesions; (b) post-operative AS-OCT appearance of PKP with normally deep anterior chamber.
Discussion
Brittle cornea syndrome is a very rare disease, often underdiagnosed, with about 90 cases documented in literature,5,6 first described by Stein et al on twin children of consanguineous Tunisian family. 7 Now it has been identified in different parts of the world.5–11
Clincal features
BCS is a complex pathology and, especially in the first phase, it is not easily differentiable, phenotypically, from other collagen disorders with associated ocular manifestations, such as the kyphoscoliotic form of EDS, Stickler syndrome, osteogenesis imperfecta, or Marfan syndrome, especially when a corneal rupture has not yet occurred.2,5 However, although clinically very similar, differentiation is necessary for a managerial and prognostic point of view. The kyphoscoliotic form of Ehlers-Danlos Syndrome (EDS) is associated with a greater risk of visceral and aneurismatic ruptures, even mortal, while this risk has not been identified in patients with BCS. 2 BCS does not seem to have this problem but careful ocular management, closer follow-up and careful monitoring of visual symptoms are required. If it is true that in a first phase the central corneal thickness can be even normal, over the years, in all cases of Brittle Cornea Syndrome confirmed by genetic analysis, the central corneal thickness (CCT) becomes less than 400 μm, and in some patients, such as in our case series, the CCT may be less than 300 μm. The other connective tissue disorders within the EDS spectrum are known to have reduced CCT, but this is not pronounced as in BCS. 11 According to the data in literature, in BCS the corneal perforation event occurs very early at an average of 4.3 years old with more than half the cases resulting in blindness. 12 Ruptures occurred first at around age 2 years and gradually increased in frequency, seeming to reach a plateau at 10–12 years. 12 Burkitt et al in this case series reported a risk of corneal rupture greater than 70%. 2 In combination with hearing loss, which is reported in 41% of affected patients, this often results in severe sensory deprivation. 5 In this case series all the 3 patients had a history of a previous corneal rupture in one eye and keratoglobus in the other eye. The extraocular manifestations were, on the other hand, joint hyperlaxity and arachnodactyly.
Genetics of BCS
Although some characteristics may lean more towards a BCS than the EDS spectrum (such as the particularly low CCT value and the history of spontaneous corneal perforation), there is no pathognomonic sign of BCS, as well as there are no clear diagnostic criteria for BCS, especially in an early stage of the disease. From a genetic point of view, however, the BCS appears well framed. Biallelic variants in two genes, ZNF46913–15 and PRDM512,16 have been identified as being responsible for BCS.13–15 Two forms of BCS will thus be genotypically distinguishable: type I in which the biallelic mutation is found in the ZNF469 gene and type II where the biallelic mutation involves the PRDM 5 gene. The ZNF469 gene (encoding zinc finger protein 469) is a transcription regulator that participates in pathways regulating extracellular matrix and collagen synthesis. 13 The PRDM 5 gene, identified later by Burkitt Wright et al in 2011 as the second locus for BCS, would also appear to be a transcription factor that regulates extracellular matrix (ECM) development and maintenance in corneal and bone cells.14,15 In our case series WES was performed to confirm clinical diagnosis and variant c.974delG (p.Cys325LeufsX2) was identified in PRDM5 gene, in all the 3 Brothers. Whole exome sequencing was performed on genomic DNA using the Ion AmpliSeq Exome platform (ThermoFisher), sequencing data were analyzed with platform-specific pipeline softwere, Torrent Suite v5.6 and Ion Reporter v5.1. It is therefore necessary to include these two genes in the genetic analysis for the diagnostic setting of those forms of collagen disorders with associated ocular manifestations so as to allow early identification and treatment of BCS.
Clinical management
Given the high frequency of corneal ruptures and its subsequent low visual outcome, it is clear that the main objective of the doctor will be, through an early diagnosis of BCS, to implement a whole series of measures to prevent these complications. We will then proceed to the recognition of risk factors and to instruct patients, or their parents if children, on a series of behaviours to minimize the risk of corneal trauma, even of minimal entity. 11 It will in fact be recommended to use protective polycarbonate glasses, avoid contact sports and rough play etc.2,10,16 It is clear, however, how it can be particularly difficult, especially when dealing with small children, to make them wear protective glasses all day, as too many restrictions in everyday life can strongly impact on their quality of life and affect their social sphere. We suggest to lead the patient and his parents create a routine easy to follow and that does not make the patient feel “different”, but that, at the same time, minimizes the chances of being exposed to ocular trauma. 11 As regards the visual impairment of these patients, a correct and frequently updated correction of the refractive error will be required to avoid the onset of amblyopia.2,10,11 The correction of the refractive error can be done with glasses and, when these are no longer sufficient, especially in the presence of irregular astigmatism, contact lenses can be used. To achieve better visual acuity, in some cases it is recommended to use contact lenses and glasses at the same time. 2 However, some authors advocate caution in wearing contact lens especially when cornea is extremely thin. 17 The limited chances of correction of the irregular astigmatism caused by keratoglobus and keratoconus, together with the onset of high myopia, at the early period of BCS, still causes a visual acuity often impaired. 10
Surgical management
The surgical management of a patient with BCS has always been considered very problematic and the choice of one of the different approaches available will be evaluated by the surgeon in accordance with its possible complications and the specificity of the case. In the presence of a corneal perforation, a very frequent complication in BCS, surgical management presents several critical issues. Being in the presence of a very thin and fragile cornea, when trying to suture the wound, the “Cheese wiring” of sutures and tissue breakdown are frequent, while when you opt to perform a penetrating keratoplasty, there is a greater risk of intraoperative corneal perforation during rotation stitches. 4 Therefore, over the decades, various authors have proposed a variety of approaches for the management of these ruptures providing some practical advice in the application of sutures to minimize any loss of tissue during surgery and any post-operative leakage: Table 1 resumes the characteristics and management of corneal ruptures in patients with BCS.4,18–23 The surgical plan must foresee that from a simple repair of laceration one can be forced to turn to a corneal transplantation or that a primary PK can be a viable option to restore ocular integrity in fragile corneas following trauma when tissue loss precludes simple repair.18–20,24 For these authors PK can be used as an integrity restoring procedure with the hope of repeating the procedure later in order to visually rehabilitate the patient. 18 In this regard Izquierdo et al suggested, in the execution of the PK, to use 11.0 nylon sutures with long suture bites in order to reduce the risk of post operative leak. 4 With Lazaridis et al we saw the use of Epikeratoplasty, always used as a refractive procedure, as a temporary measure for tectonic restoration of perforated corneas following corneal melts. 21 In their 2021 case report, Safae et al instead used a multilayered amniotic membrane graft to manage a corneal rupture in a 6-year-old girl diagnosed with BCS while maintaining a 1/10 BCVA in the 4-month follow-up. 22 Recently Matalia et al, since suturing ruptures or lacerations in Brittle corneas are technically difficult with no clear-cut guidelines or protocol on how to go about, has tried to provide, by exposing its case report, tips for handling Brittle corneal perforations. He also addressed the problems encountered during surgery, highlighted the suturing techniques that can be customized and gave an insight into postoperative care. 23
Clinical findings and management of corneal ruptures in patients with brittle corneal syndrome.
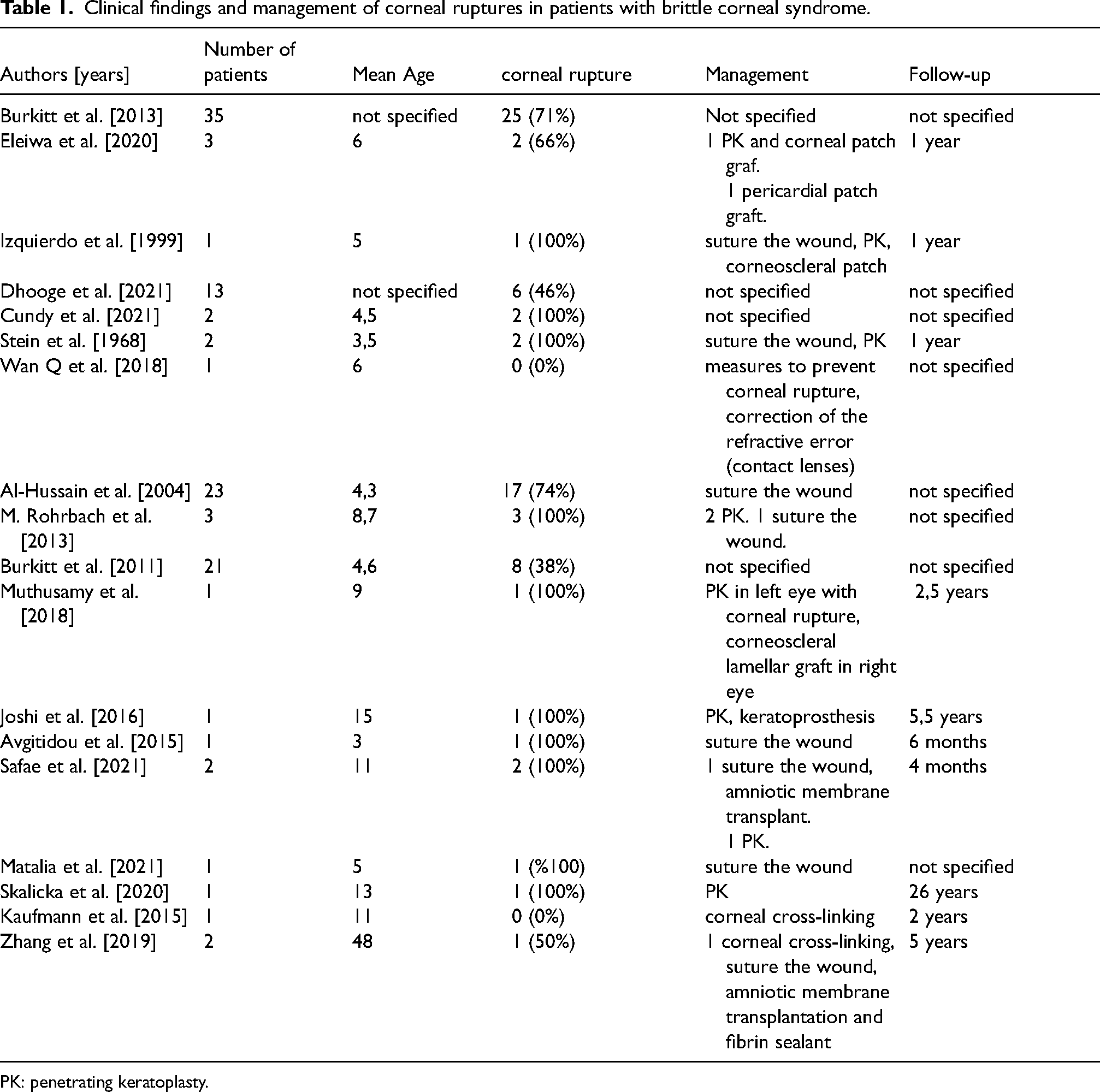
PK: penetrating keratoplasty.
The use of an onlay corneal lamellar graft to reduce high levels of myopia in non-perforated BCS eyes has been described in literature. The patient, who was blind in the other eye as a consequence of a penetrating corneal injury in childhood, complained poor vision in the intact eye with intolerance to glasses and contact lenses. Although at first there was an impressive reduction of myopia from −23 dioptres to −5 dioptres and an improvement in navigational ability, he later developed acute corneal hydrops and glaucoma requiring cycloablation.16,25 Also debated is the possibility of cross linking (CXL) in patients with BSC26,27: progressive corneal thinning may result in keratoglobus or keratoconus and CXL has been attempted to stop this progression. Given the low value of corneal thickness to reduce endothelial injury, the authors opted for an epithelium on procedure – whose results have been described to be as effective as the standard Dresden protocol in halting the progression of Keratoconus, 28 thus reducing UV penetration into the cornea, and the UV light exposure was also reduced in proportion to CCT, obtaining encouraging results. 26 More alarming is the recent case report of corneal perforations after corneal cross-linking for keratoconus in a woman harboring potentially pathogenic variants in the ZNF469 gene. 27 We present a case series of three siblings diagnosed with Brittle Cornea Syndrome, decided to perform a penetrating corneal transplant despite no corneal perforation being found achieving such satisfactory visual results. Other researchers and clinicians should consider that in their practice. Furthermore the contribution of the article is, to our knowledge, to have described the first case series of BCS reported in Albanian population and to have done a systematic revision of the existing literature (Table 1).
Conclusion
Brittle Cornea Syndrome is a rare, and difficult to manage, disease. Its infrequency, together with having systemic manifestations similar to other pathologies often lead to underdiagnosis of this disease with disastrous consequences. In the case series we carried out, it is clear that these three siblings did not receive a prompt diagnosis of Brittle Cornea Syndrome. The consequence has been the lack of appropriate prevention and management of the frequent corneal breaks that occur in this pathology. Patients in fact had a correct diagnosis only once they went to our medical facility and after having already suffered a corneal rupture in one eye, whose management was not immediate: without the precautions that in such thin corneas are mandatory, it has resulted in blindness and phthisis bulbi. It is therefore necessary to know the existence of this pathology in order to be able to carry out the right diagnostic investigations, and, once the diagnosis has been made, implement the right complication prevention and management procedures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.