
Abstract
Purpose
To report a case of branch retinal artery occlusion (BRAO) of the left eye combined with left congenital common carotid artery occlusion (CCAO) and internal carotid artery occlusion (ICAO).
Methods
Case report.
Results
A 36-year-old man presented with sudden vision loss of only the left eye without any signs or symptoms of brain diseases. Fluorescein fundus angiography (FFA) showed left BRAO, and computed tomography angiography (CTA) of the head and neck showed entire left CCAO and ICAO. The patient's left vertebral artery was anastomosed with the left occipital artery via the muscular branch, supplying blood retrogradely to the left external carotid artery. The right internal carotid artery compensated for blood supply to the left anterior cerebral artery and middle cerebral artery via anterior communication, and the left posterior communication artery compensated for blood supply to the left middle cerebral artery.
Conclusions
To our knowledge, this study was the first to report a case of BRAO combined with congenital CCAO and ICAO with vision loss as the first symptom and proposed the importance of head and neck examination in retinal artery occlusion at the first visit to a doctor.
Keywords
Introduction
Branch retinal artery occlusion (BRAO) is an ophthalmic emergency with poor visual outcome if the macula is involved. Emboli, including cholesterol emboli, thrombosis (often from the internal carotid artery or heart), and calcification emboli (often from heart valves), are the common causes of BRAO, among which emboli from the internal carotid artery (ICA) are the most common cause. Hence, BRAO is often associated with ICA stenosis or plaques. Distinct from the above common causes, in this study, we reported a rare case of unilateral BRAO with unilateral congenital common carotid artery occlusion (CCAO) and internal carotid artery occlusion (ICAO).
Case
A 36-year-old man came to our outpatient department with sudden onset of blurred vision in his left 2 eye for 16 h. Fundus radiography at another hospital showed paleness and oedema throughout the retina, cherry red spots in the macular area, and tapering of the retinal artery, which was diagnosed as central retinal artery occlusion (CRAO) of the left eye. The visual acuity of the left eye was no light perception, and the intraocular pressure was 18 mmHg. The patient had no history of hypertension, diabetes, heart diseases or craniocerebral diseases. Immediately, 0.5 mg nitroglycerin was administered sublingually, and retrobulbar injection was administered with anisodamine, lidocaine and dexamethasone. The craniocerebral CT showed no obvious positive signs, so computed tomography angiography (CTA) of the head and neck was further performed to prepare for ophthalmic artery thrombolysis. Surprisingly, the CTA results showed entire left CCAO and ICAO (Figure 1), in which ophthalmic artery thrombolysis could not be performed. Hence, the patient was immediately transferred to the neurology department for specialized treatment. Digital subtraction angiography (DSA) was further conducted and showed that the left vertebral artery was anastomosed with the left occipital artery via the muscular branch, supplying blood retrogradely to the left external carotid artery. The right internal carotid artery compensated for blood supply to the left anterior cerebral artery and middle cerebral artery via anterior communication, and the left posterior communication artery compensated for blood supply to the left middle cerebral artery, with sparse vessels in the left cerebral hemisphere compared with the contralateral side (Figure 2). After one week of treatment with low molecular weight heparin, batroxobin, trinosin, vitamin C and vitamin B6 in the neurology department, the visual acuity index of the left eye was /20 cm with temporal visual field, and fluorescein fundus angiography (FFA) showed macular branch of the inferior temporal artery occlusion (Figure 3). Therefore, the diagnosis was corrected as BRAO of the left eye.
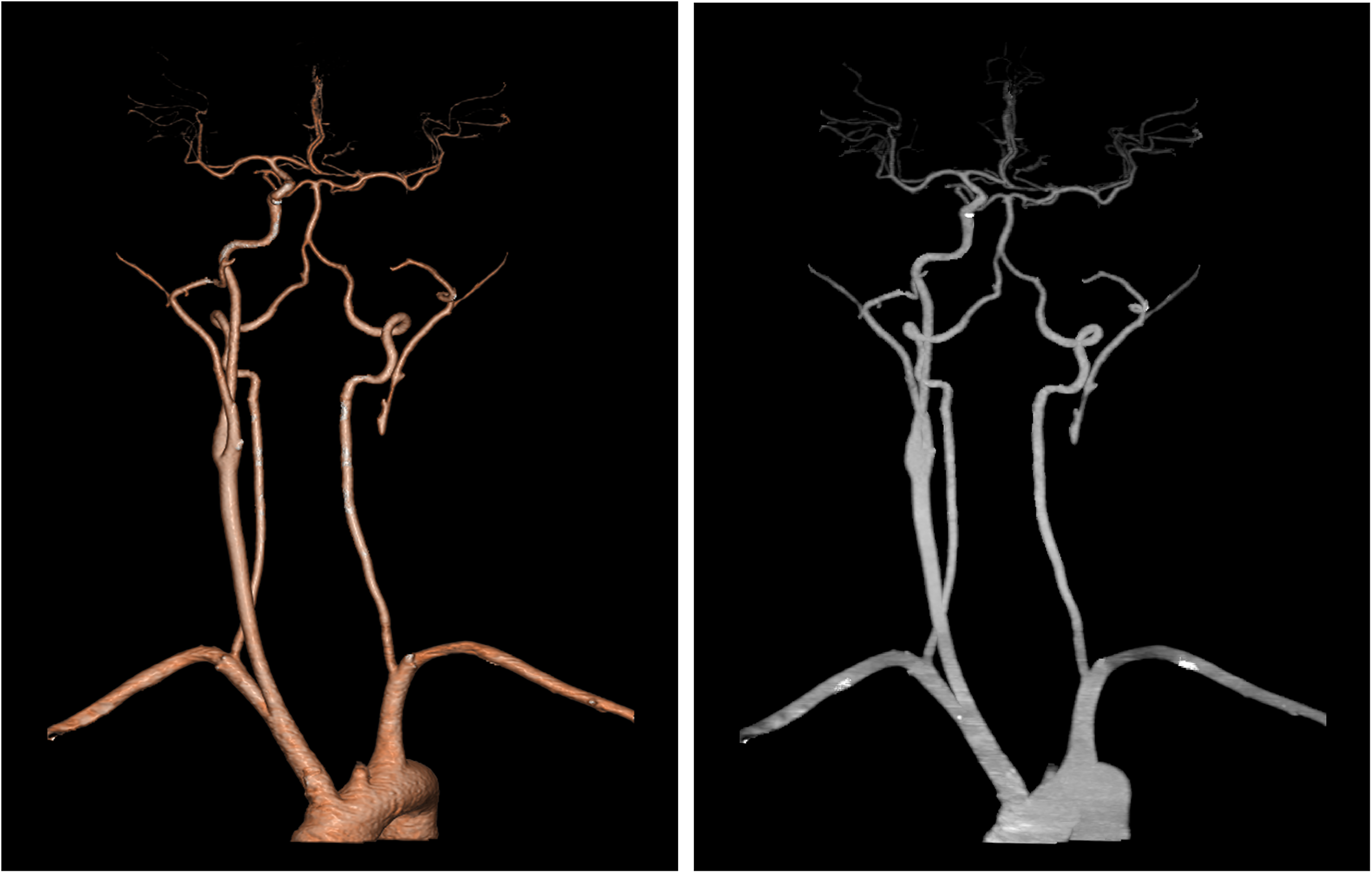
Computed tomography angiography of the head and neck showed occlusion of the left common carotid artery and internal carotid artery.
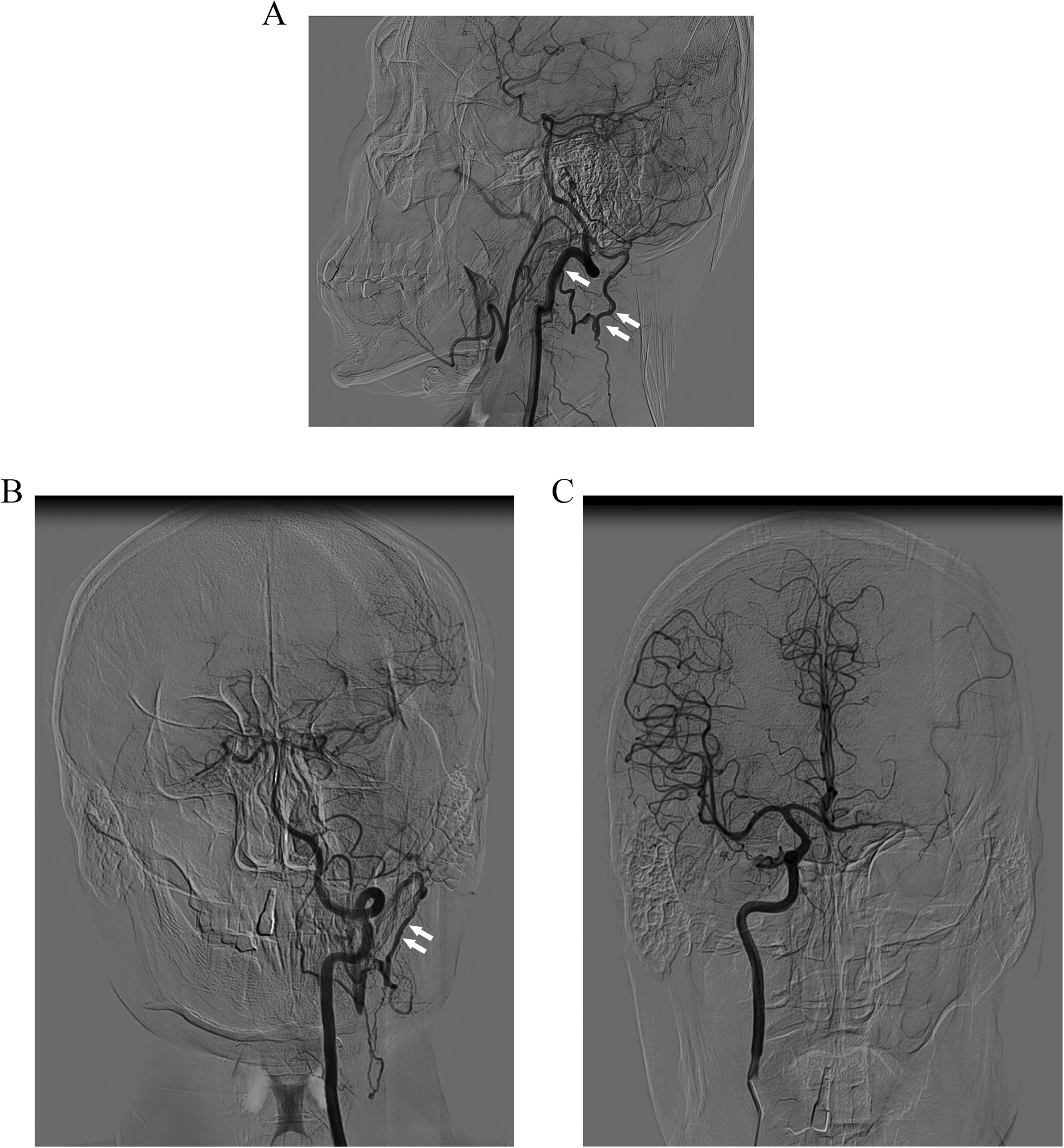
Digital subtraction angiography results. (A-B) The left vertebral artery was anastomosed with the left occipital artery via the muscular branch (one arrow), supplying blood retrogradely to the left external carotid artery, which was tortuous and meandering (double arrows). (C) The right internal carotid artery compensated for blood supply to the left anterior cerebral artery and middle cerebral artery via anterior communication, and the left posterior communication artery compensated for blood supply to the left middle cerebral artery, with sparse vessels in the left cerebral hemisphere compared with the contralateral side.
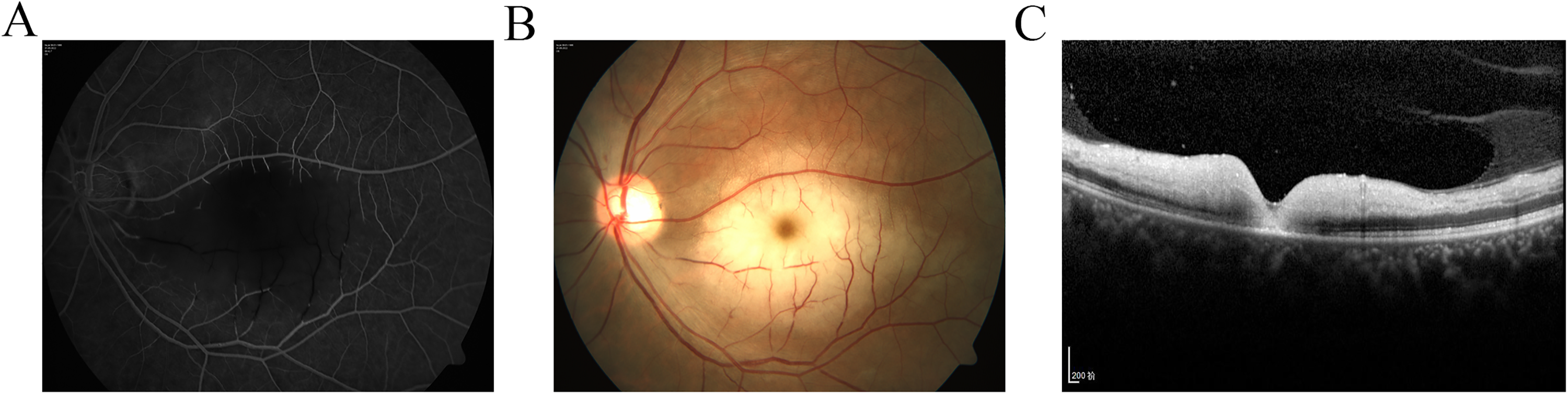
Ocular examination results after one week of treatment in the neurology department. (A) Fundus fluorescein angiography showed occlusion of the macular branch of the inferior temporal artery in the left eye. (B) Fundus photography showed the cherry red spot in the macula of the left eye and the pale oedema retina corresponding to the occluded artery. (C) Optical coherence tomography of the fundus revealed oedema of the inner retina, which is a typical characteristic of BRAO.
Discussion
Retinal artery occlusions (RAO), including CRAO and BRAO, are a common, visually disabling, ocular vascular occlusive disorder that is usually manifested as a sudden, dramatic onset of visual loss. 1 BRAO is estimated to account for approximately one-third of acute RAO, 2 manifested by thinning of blocked vessels and pale oedema of the retina in the area where the blocked vessels are distributed. In this BRAO case, the macular branch of the inferior temporal artery was involved (Figure 3), so the patient presented with cherry red spots in the macular area with poor vision.
Standard treatment modalities for RAO include ocular massage, anterior chamber paracentesis, intraocular pressure (IOP)-lowering agents (e.g., mannitol, acetazolamide, topical agents), hyperbaric oxygen and anticoagulants. However, these therapies are less effective.
Atherosclerosis-related thrombus, embolism, vasospasm, and giant cell arteritis are known causes of RAO. 3 Embolism is the most common cause of RAO. Plaques in the carotid artery are usually the source of embolism, and carotid Doppler/angiography showed the presence of plaques in 71% of CRAO cases and 66% of BRAO cases. 1 DSA-guided superselective ophthalmic artery thrombolysis or selective carotid intervention, which can induce rapid recanalization of the occluded arteries and reperfusion of the ischaemic retina when administered shortly after onset of visual loss, remains the preferred treatment method for RAO.2,4 Although no guidelines for acute RAO management are available, thrombolysis has been suggested to be a beneficial treatment. While the recommended time window for arterial thrombolysis is no more than 6−12 h, studies have found that better visual outcomes can still be observed even if the time window is extended to 24 h. 5 Therefore, we tried ophthalmic artery thrombolytic therapy for this case, although it was 16 h after the onset of vision loss. Before thrombolysis therapy, we completed the CTA examination of the head and neck and found complete left CCAO and ICAO, so the patient was transferred to the neurology department for specialized treatment instead of thrombolysis.
Carotid artery diseases are the most common causes of RAO. The mechanisms of RAO caused by carotid artery diseases are commonly embolism, artery stenosis and arterial spasm, 1 while congenital anomalies are rare. The anatomy of the Circle of Willis is shown in Figure 4 (Created with BioRender.com). The absence of the ICA is a rare anomaly that occurs in only 0.01% of the population 6 and may present with developmental delay, subarachnoid haemorrhage, transient neurologic events, or other developmental abnormalities. 7 Andrea et al. reported a case of bilateral segmental agenesis of the ICA that presented with occasional mild headaches with no brain abnormalities. 8 Dragoş et al. described one case of left ICA agenesis accompanied by the absence of the precommunicant part of the left anterior cerebral artery and of the right posterior communicating artery with benign symptoms, including dizziness and headache. 9 However, most congenital anomalies of the ICA are asymptomatic because of the sufficiently developed collateral vessels and are usually discovered by chance.6,10 CCAO accounts for 1%–5% of all cerebrovascular events.
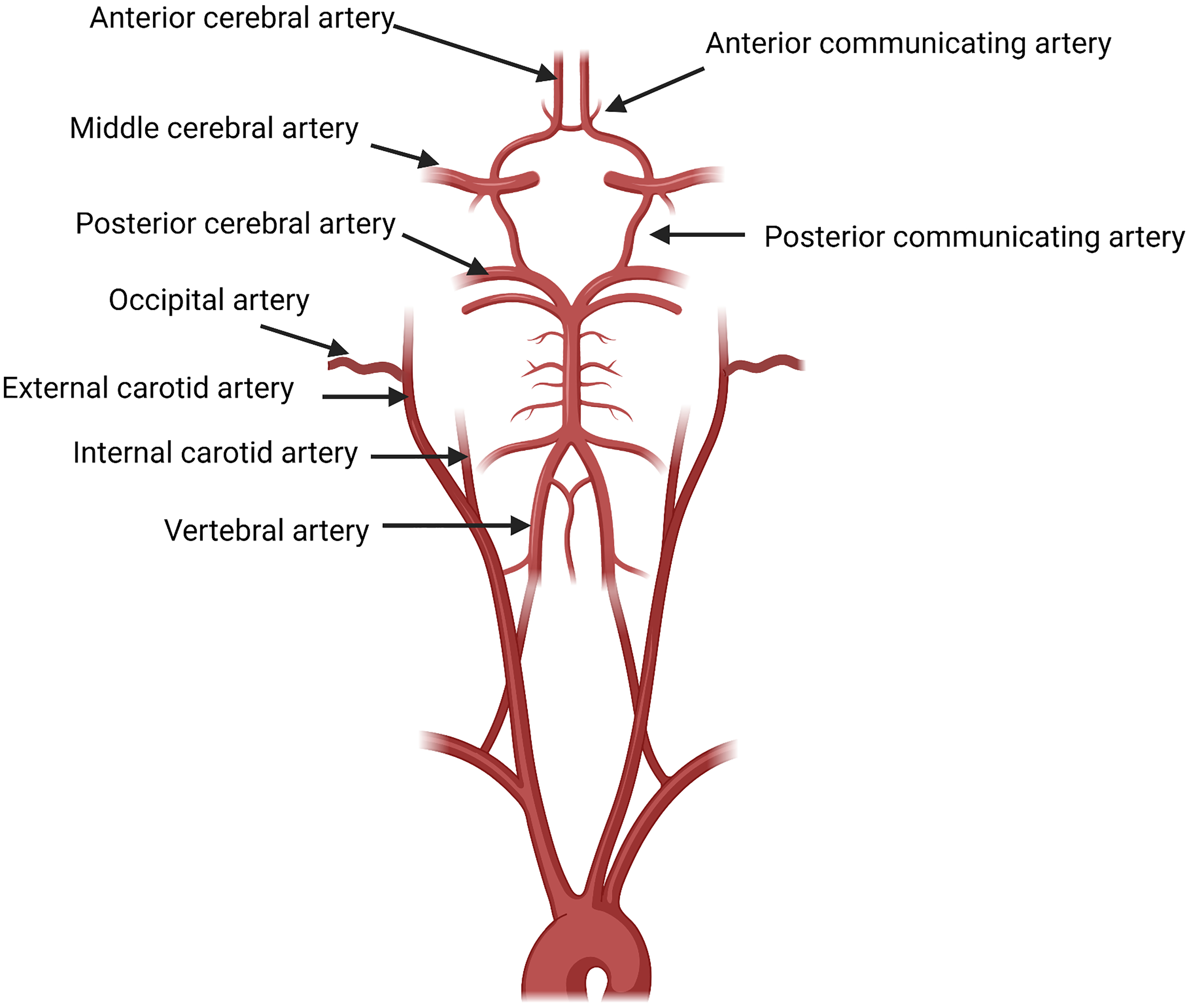
The anatomy of the circle of willis.
Unlike ICAO, which has been studied extensively, the literature on CCAO is sparse. 6 Doniel et al. reported a case of congenital absence of the common carotid artery (CCA) with a ruptured anterior communicating artery aneurysm, of which the right internal and external carotid artery originated from the ipsilateral inominate artery. 11 In our case, the left vertebral artery was anastomosed with the left occipital artery via the muscular branch, supplying blood retrogradely to the left external carotid artery, and DSA showed that the left external carotid artery was tortuous and meandering, which was different from the normal external carotid artery, suggesting dysplasia of the external carotid artery, Moreover, the patient's right internal carotid artery compensated for blood supply to the left anterior cerebral artery and middle cerebral artery via anterior communication, and the left posterior communication artery compensated for blood supply to the left middle cerebral artery, with sparse vessels in the left cerebral hemisphere compared with the contralateral side (Figure 2). Therefore, the patient has not shown obvious brain symptoms and signs thus far due to the strong compensatory blood supply system in the left cerebral hemisphere. We speculated that the CCAO and ICAO in this case were due to congenital dysplasia, which led to the establishment of the “compensatory blood supply system” because in the case of acute CCAO and ICAO, patients could not establish compensatory blood supply in a timely manner and would inevitably develop corresponding cerebral ischaemic manifestations, which was not seen in this case.
Normally, after originating from the CCA, the ICA passes through the dura mater and leaves the cavernous sinus to branch off the ophthalmic artery (OphA). The OphA follows the optic nerve through the optic canal and passes through the optic canal into the orbit, which is divided into the intracranial segment, intracanalicular segment and intraorbital segment. The branches of the OphA include the central retinal, posterior ciliary, lacrimal, ophthalmic muscle, anterior ethmoid, posterior ethmoid, supraorbital, medial palpebral, and dorsal nasal arteries, supplying nutrients to the eyeball tissues and their appendages. Because the blood supply to the eye derives from the ICA, CCAO or ICAO can present with ischaemic ocular symptoms (e.g., amaurosis fugax, RAO, ophthalmic artery occlusion, or ocular ischaemic syndrome). 12 Congenital absence of the ICA is often associated with carotid canal atresia and ICA-related structural abnormalities, such as variations in the origin of the OphA to provide blood flow to the eye for normal physiological function. 7 There are several types of OphA variants, such as an OphA that originated from the middle meningeal artery (MMA) or the cavernous segment of the ICA, 13 and the OphA variant haemodynamically may be more susceptible to retinal infarction. Because the ocular artery is very small in DSA images, the origin of OphA could not be clearly seen from DSA in this case. To our knowledge, this was the first report of a case of BRAO with congenital CCAO and ICAO.
In this study, we reported a rare case of BRAO combined with congenital CCAO and ICAO with vision loss as the first symptom and proposed the importance of carotid artery-related examinations in the primary diagnosis of BRAO in the outpatient department.
Footnotes
Acknowledgements
Not applicable.
Author contributions
Shoubi Wang and Weijie Ouyang collected the details of the case, and wrote the manuscript. Yidan Zhang helped analyze the DSA images. Han Chen reviewed and edited the manuscript. All authors approved the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability statement
The datasets generated during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent for publication
The study was waived by the Ethic Committee of the First Affiliated Hospital of Xiamen University. The written informed consent was obtained from the patient.
Funding
This study received no financial support.