
Abstract
Lesson
We report a case of retinal artery occlusion in a young adult in early pregnancy found to have a patent foramen ovale as the source of the embolism. This report suggests the importance of early cardiac investigation in such individuals.
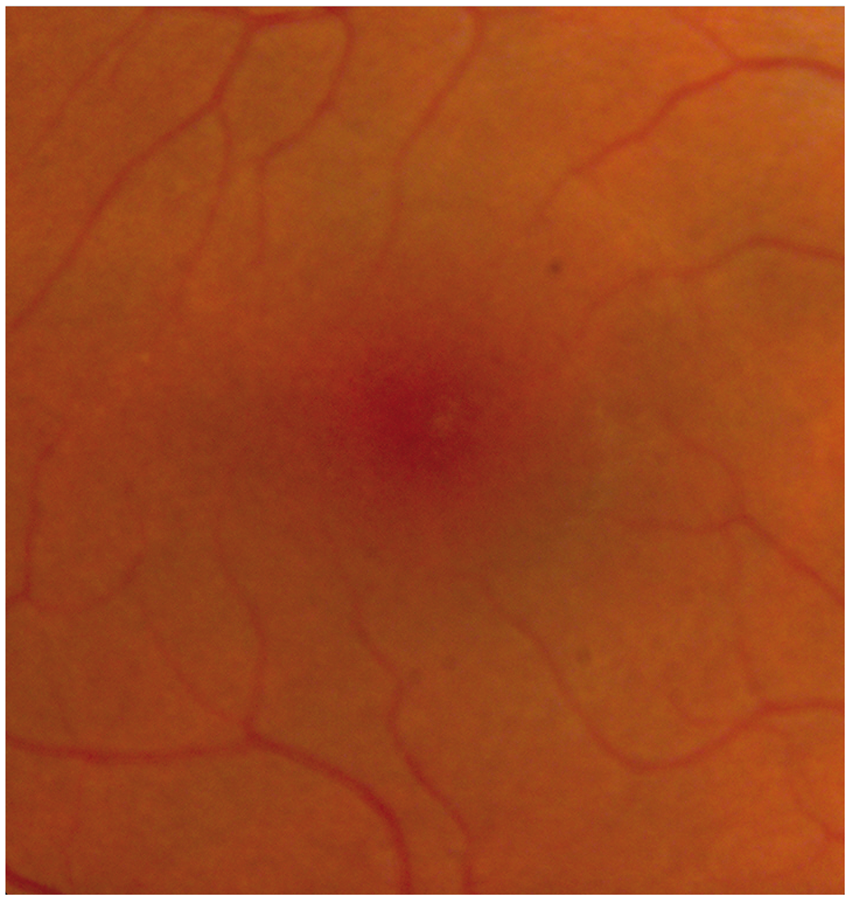
A 32-year-old female Caucasian presented with a sudden onset decrease in vision in the left eye. She complained of a small left paracentral scotoma with associated left-sided headache. Presenting Snellen acuities were 6/6 right eye and 6/9 left eye. Colour vision was full in both eyes, however, slightly slower on the left side compared to the right. There was an early left relative afferent pupil defect. Anterior segment examination was unremarkable. Fundus examination showed marked pallor in the left nasal macula at presentation, consistent with a branch retinal artery occlusion. A very subtle change remains on the post-partum colour images when comparing the left nasal macula to the right at high magnification (Figures 1 and 2).
High magnification of left macula with subtle pallor in the nasal border (shown by arrow). High magnification of normal right macula.
The patient was 10 weeks pregnant at the time. She had a history of endometriosis and mild hypotension. She had one previous normal pregnancy. There was a strong family history of vascular events from myocardial infarction, deep vein thrombosis and a presumed cerebrovascular accident. The patient was an ex-smoker for two years.
Investigations for causes of arterial occlusion were performed including a thrombophilia screen, B scan ultrasound of the eye, chest X-ray and an echocardiogram. Thrombophilia screen, clotting factors and cardiolipin antibodies were negative. Fluorescein angiogram could not be carried out during the pregnancy due to the unknown risks to the foetus.
A previously undiagnosed 4 mm patent foramen ovale was found and closed with an 18 mm Amplatzer transcatheter device. She was kept on a 75 mg daily dose of aspirin.
Discussion
‘In 1564, Leonardi Botali, an Italian surgeon, was the first to describe the presence of foramen ovale at birth.’2 Patent foramen ovale is a source of paradoxical embolism, and it was described by Cohneim in 1877. 2 The RECO study group later found that 45% of central retinal artery occlusion patients under 45 years had cardiac abnormalities, of whom 27% needed anticoagulation or cardiac surgery. 3
‘Patent foramen ovale is a flap-like opening between the atrial septa primum and secundum at the location of the fossa ovalis that persists after age of 1 year.’2 In utero, the foramen ovale serves as a physiologic conduit for right-to-left shunting. Once the pulmonary circulation is established after birth, left atrial pressure increases, allowing functional closure of the foramen ovale. This is followed by anatomical closure of the septum primum and septum secundum by the age of 1 year.
With increasing evidence that patent foramen ovale is the culprit in paradoxical embolic events. James Lock postulated that the patent foramen ovale anatomy results in a cul-de-sac between the thin septa primum and thick septum secundum, 4 predisposing individuals to haemostasis and clot formation.2 Any conditions that increase right atrial pressure more than left atrial pressure can induce paradoxical flow and may result in an embolic event. 4
Our patient was 10 weeks pregnant, at the time of presentation. Retinal artery occlusion can occur in pregnancy due to an induced hypercoagulable state. During pregnancy, clotting is altered by a 50% increase in fibrinogen, increases in coagulation factors II, VII, VIII, IX and X, decreases in prothrombin and partial thromboplastin time, decreased fibrinolytic activity and stasis of blood in the lower half of the body. Because the retinal artery obstruction occurred so early in pregnancy, another mechanism can be proposed. This occlusion may represent a paradoxical embolism in the form of amniotic fluid from the uterine vessels passing through the patent foramen ovale to the retinal artery with activation of complement and granulocyte aggregation.
Patients with patent foramen ovale and paradoxical embolism are at increased risk of recurrent systemic thromboembolic events, ranging from 3.2% to 3.8% per year. The optimal management of these patients remains controversial. Long-term anticoagulation, surgical patent foramen ovale closure and percutaneous transcatheter closure of the patent foramen ovale have been proposed as therapeutic options. 1 Transcatheter techniques to close patent foramen ovale have been used with increasing frequency during the last few years.
It is important to consider a diagnosis of a patent foramen ovale, when there is a young patient presenting with a retinal artery occlusion.5 A multisystem examination is required and prophylactic measures need to be taken against systemic thromboembolic disease.