
Abstract
Aim
to assess the effectiveness of a new combination of topical solution with Hyaluronic Acid 0.2% and arnica extract 0.1% in reducing dry eye symptoms in a population of pediatric patients.
Methods
52 pediatric patients (aged 9 to 14 years) with signs and symptoms of dry eyes and allergic conjunctivitis were included in the study. Twenty-six patients were assigned to the Hyaluronic Acid 0.2%/ Arnica extract 0.1% group (Study Group) while 26 patients to the Hyaluronic Acid 0.2% group (Control Group). Clinical signs and symptoms were assessed at baseline and at week 4. The assessment plan included: slit-lamp examination, tear film break up time (TBUT), Schirmer's test and conjunctival hyperemia score. Ocular surface disease index (OSDI) score was used to evaluate subjective symptoms of dry eye disease.
Results
Both treatment groups showed improvements in the estimated clinical parameters after treatment. OSDI score was significantly lower in both treatment groups (Study group p = 0.02; Control group p = 0.04) at the end of the follow up period. Improvements in TBUT, Schirmer's test results and conjunctival hyperemia were statistically significant only in the Study group (p = 0.021; p = 0.03; p < 0.01 respectively).
Conclusions
Preliminary findings suggest that combined topical Hyaluronic Acid 0.2% and arnica extract 0.1% can be effective in reducing symptoms and signs of dry eye disease in children.
Introduction
Dry Eye Disease (DED) is a multifactorial disorder of the tear film and ocular surface resulting in eye discomfort. It is due to loss of the natural balance of the tear film and ocular surface. 1 The tear film has several important functions that are essential to the health of the eye. It provides trophic support to the epithelial cells in the cornea and conjunctiva, thus providing the anterior part of the eye a refractive and antimicrobial function. DED affects all age groups, it is generally considered rarer in children, although some new evidence suggests a higher prevalence of pediatric DED than considered before.2,3 The main etiologies causing pediatric DED were Meibomian gland dysfunction, Stevens-Johnson Syndrome and vitamin A deficiency. 4 Prolonged Video Display Terminal (VDT) use and learning activities (reading and writing) have been associated with decreased maximum blink interval, hence dry eye symptom onset.5,6
In 2017 the Tear Film and Ocular Surface Society (TFOS) published the Dry Eye Workshop (DEWS) II Diagnostic Methodology report, which established the most effective diagnostic management and provided a differential diagnosis for DED. 7 This report presented a strategy for the diagnosis of DED in the adults. Therefore, it didn't provide guidance on the treatment of pediatric DED, that was described as a rapidly growing problem. 8 Studies of children with DED have been generally conducted using TFOS DEWS criteria for adults and subjective symptoms were difficult to assess in pediatric patients.1,9
Allergies are one of the most common disorders in children, and ocular allergy is one of the most common ocular disorder encountered in clinical practice. The prevalence of allergic diseases in children aged 6–14 years varies significantly from 0.3% to 20.5% and is gradually increasing. 10 This increase may be due to genetic factors, air pollution in urban areas, pets and early childhood exposure. 10 Seasonal allergic conjunctivitis (AC) is the most common form of ocular allergy, accounting for 90% of cases. Grass, trees, weed pollen and outdoor molds are most common causes of AC.11,12 Although patients with AC have mild signs and symptoms, this may have an impact on academic performances and everyday tasks, resulting in poor overall quality of life. DED and AC are generally considered as different diseases. However, recent literature has shown that both conditions share similar characteristics, including several signs and symptoms. 13 Pflugfelder et al. 14 suggested that T cell activation and high levels of inflammatory of inflammatory cytokines such as epidermal growth factor, interleukin-1 (IL-1), IL-8, goblet cell damage and conjunctival epithelial damage can cause decreased mucin production and subsequent decreased tear film break-up time (TBUT). Many studies have shown instability of the mucins and decreased TBUT in patients with AC and suggested that upregulation of inflammation could affect chemical balance in the tears.15,16
Arnica montana (AM) has been widely used as a phytotherapeutic remedy for the treatment of several inflammatory conditions, pain and for postoperative care. It is more effective than placebo for the treatment of several conditions, including edema, ecchymosis and post-traumatic and postoperative pain. 8 Cumulative evidence suggests that AM can be an effective alternative to non-steroidal anti-inflammatory drugs for the treatment of some specific conditions. AM is a commercially available phytotherapeutic agent. It is used as analgesic and anti-inflammatory agent in patients with acute trauma. 17
The purpose of this study was to present preliminary data on the potential effectiveness of a new combined topical Hyaluronic Acid 0.2%/Arnica extract 0.1% in reducing dry eye symptoms and signs in a selected pediatric population.
Methods
This cross-sectional case control study was conducted at the Ophthalmology Department, Bambino Gesù IRCCS Pediatric Hospital in Rome, Italy and included healthy children between the age of 6 and 14. Exclusion criteria were patients who had received therapies for dry eye disease and allergic conjunctivitis one month before enrollment, lagophthalmos, eyelid disorders (eg, blepharitis, keratosis, history of trauma, hordeolum), autoimmune disease, thyroid disease, history of ocular trauma, isotretinoin therapy, antihistamines, antidepressants, steroids, medications for attention deficit and hyperactive disorders and other drugs, underweight, malnutrition and contact lens wear.
Fifty-two children were screened for eligibility; all patients had a clinical diagnosis of DED and AC. This study was conducted in accordance with the Declaration of Helsinki and General Data Protection Regulation. Informed consent was obtained from all participants and their parents. (ClinicalTrials.gov Identifier: NCT04872829).
Patients were divided into two groups: the Study Group consisted of 26 patients with DED and AC assigned to receive Hyaluronic Acid 0.2% / arnica extract 0.1% fixed combination (one drop three times daily) while the Control Group consisted of 26 patients with DED and AC assigned to receive Hyaluronic Acid 0.2% (one drop three times daily). Both groups received treatment for 4 weeks.
Ophthalmic examinations
A single ophthalmologist performed all ocular assessments, which included slit-lamp examination of the anterior segment, Tear Break-Up Time (TBUT), Schirmer's test and conjunctival hyperemia score.
TBUT was measured using fluorescein strip moistened with one drop of balanced salt solution. After the fluorescein strip was applied to the inferior conjunctival fornix, all patients resumed normal blinking pattern for several seconds. After fluorescein solution was spread over the corneal surface, the patients kept their eyes open up to the occurrence the first defect of tear film. TBUT was defined as interval between the last complete blink and the appearance of the first dry spot on the precorneal tear film. Each eye was tested three times and the average value of measurements was reported. Schirmer's test was performed using paper strips inserted into patients’ eyes for five minutes (Whatman filer paper strips, Clement Clarke), without using topical anesthetic. The strips were inserted into the lower fornix near the lateral canthus, away from the cornea. The papers were left in place for 5 min, during which the patients were asked to keep their eyes closed. Then the strip was removed, and the wet portion of the strip was measured against the millimeter scale. Both eyes were tested simultaneously. A value of less than 5 mm was used to indicate severe dry eyes and a value of less than 10 mm marginal dry eyes.7,18,19 Conjunctival hyperemia score was graded on a scale ranging from 0 (none) to 3 (severe). 19 Each patient was assessed by the same ophthalmologist at day 0 (enrollment, baseline) and after four weeks.
Questionnaire
Ocular surface disease index (OSDI) score was used to evaluate subjective ocular symptoms. This is an objective parameter for the diagnosis of DED. Modified OSDI score ranged from 0 to 100 points. Higher scores were correlated with increased discomfort due to DED. OSDI was calculated at baseline and at the end of the follow-up period.
Diagnostic criteria for dry eye disease and allergic disease
DED was diagnosed based on a combination of survey data and ophthalmic examinations, according to the Dry Eye Workshop (2017). 7 Data on signs and symptoms were collected. Objective signs included a TBUT < 10 s or positive corneal and conjunctival fluorescein staining. A modified OSDI score greater than 20 points was used to indicate subjective symptoms. Diagnosis of AC was based on past history, clinical symptoms such as ocular itching, redness, tearing or ocular pain and slit-lamp examination showing chemosis, hyperemia or palpebral conjunctival papillae.
Statistical analysis
Children were divided into two groups. OSDI score, TBUT, Schrimer's test and conjunctival hyperemia data were compared at baseline and four weeks after treatment. Statistical analyses were performed using SPSS software for Windows (version 21; SPSS, Inc., Chicago, IL). Continuous variables were compared between the two groups using the Student's t-test. A p value < 0.05 was considered statistically significant.
Results
Patients were divided in two groups: the Study group (26 patients) and the Control group (26 patients). Patients’ age ranged from 6 to 14 years. Baseline demographic characteristics were homogenous between the two groups: mean value was 9 years old in the Study group and 9,08 years old in the Control group. In the Study group, mean OSDI score was 46.57 ± 10.01 at baseline and 17.17 ± 9.32 after treatment (p = 0.02); in the Control group, mean OSDI score was 46.08 ± 12.13 at baseline and 32.23 ± 12.95 after treatment (p = 0.04) (Figure 1). Both results were statistically significative.
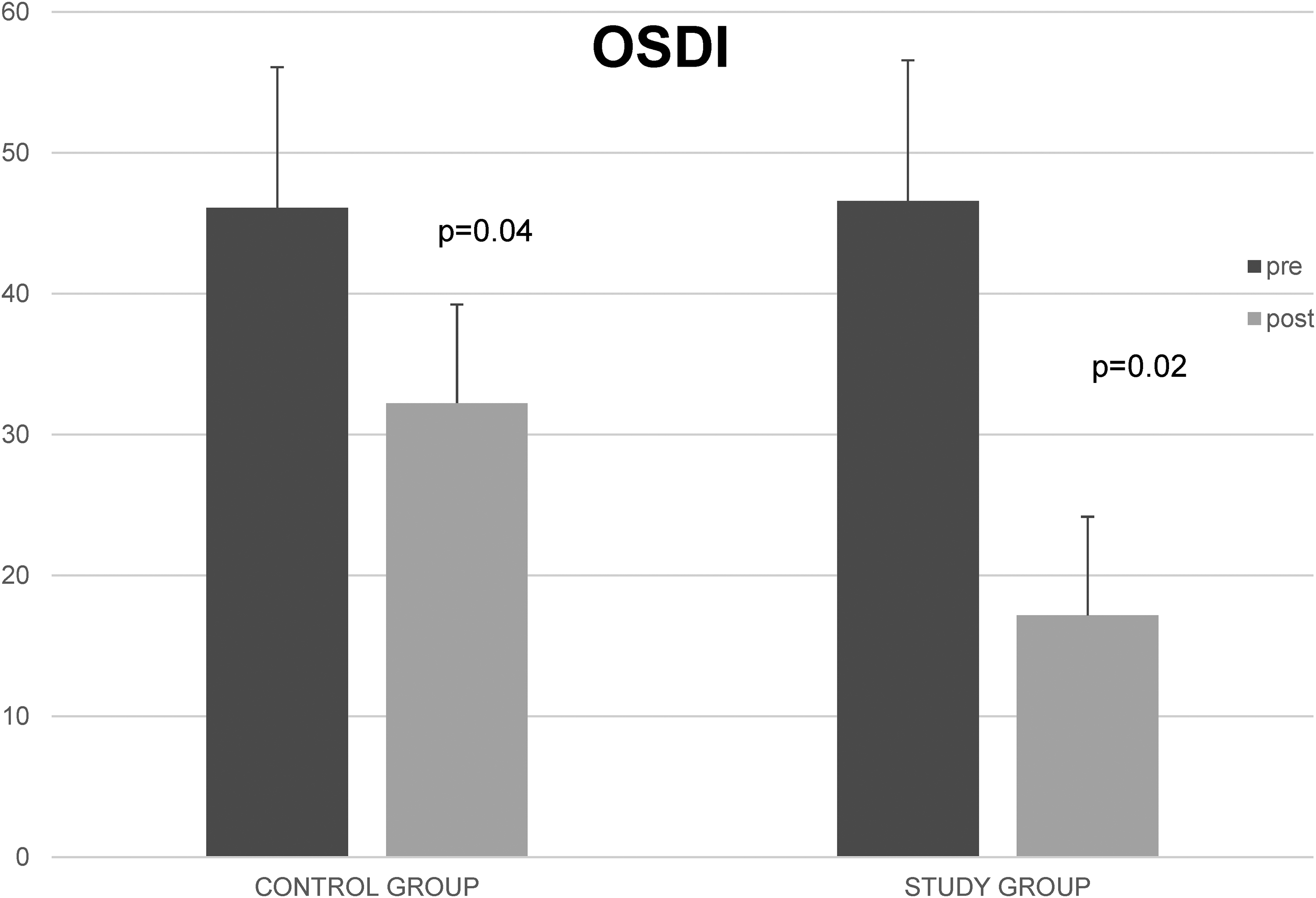
Ocular surface disease index (OSDI) score pre and post treatment.
In the Study group, TBUT was 4.22 ± 1.05 s at baseline and 8.92 ± 1.16 s after the treatment (p = 0.021); in the Control group TBUT was 4.38 ± 1.07 s at baseline and 6.68 ± 1.3 s after four weeks (p > 0.05) (Figure 2).
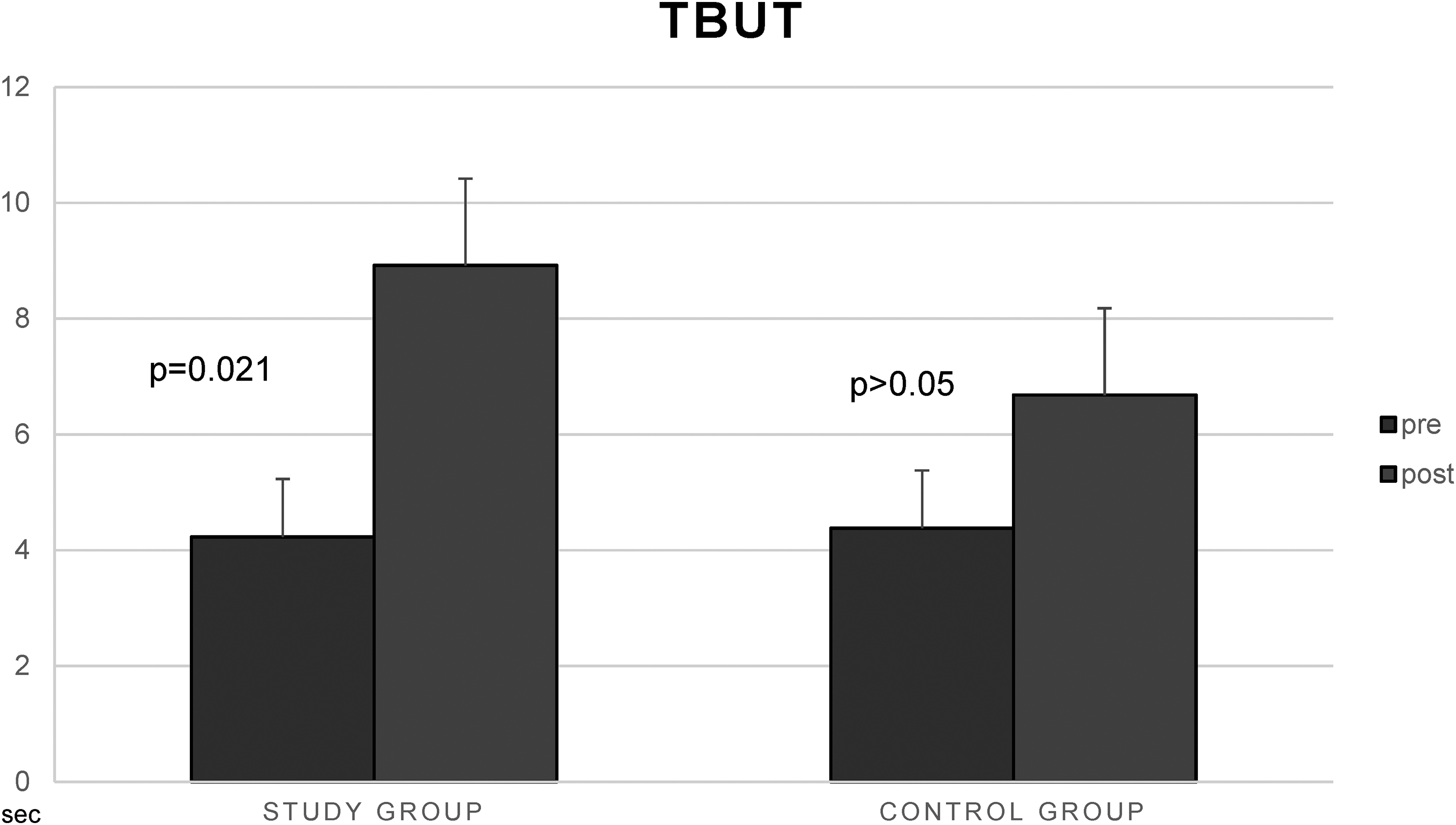
Tear film break up time (TBUT) pre and post treatment.
In the Study group, Schirmer's test score was 7.89 ± 0.93 mm/5 min at baseline and 9.18 ± 0.8 mm/5 min after treatment (p = 0.03); in the Control group, baseline Schirmer's test score was 8.11 ± 1.04 mm/5 min and 8.85 ± 1.23 mm/5 min after treatment (p > 0.05) (Figure 3).

Shirmer's test pre and post treatment.
In the Study group, conjunctival hyperemia score was 2.52 ± 0.64 at baseline and 0.26 ± 0.53 after four weeks (p <0.01); in the Control group, baseline conjunctival hyperemia score was 2.39 ± 0.54 and 1.65 ± 0.56 at the end of treatment (p > 0.05) (Figure 4). The combination Hyaluronic Acid 0.2%/ Arnica extract 0.1% ophthalmic solution was well tolerated in the study population and no local adverse events were recorded. All clinical parameters evaluated showed improvement after treatment; OSDI score was significantly lower at the end of the follow up period in both groups, but only the study group had statistically significant improvements in TBUT, Schirmer's test scores and conjunctival hyperemia.
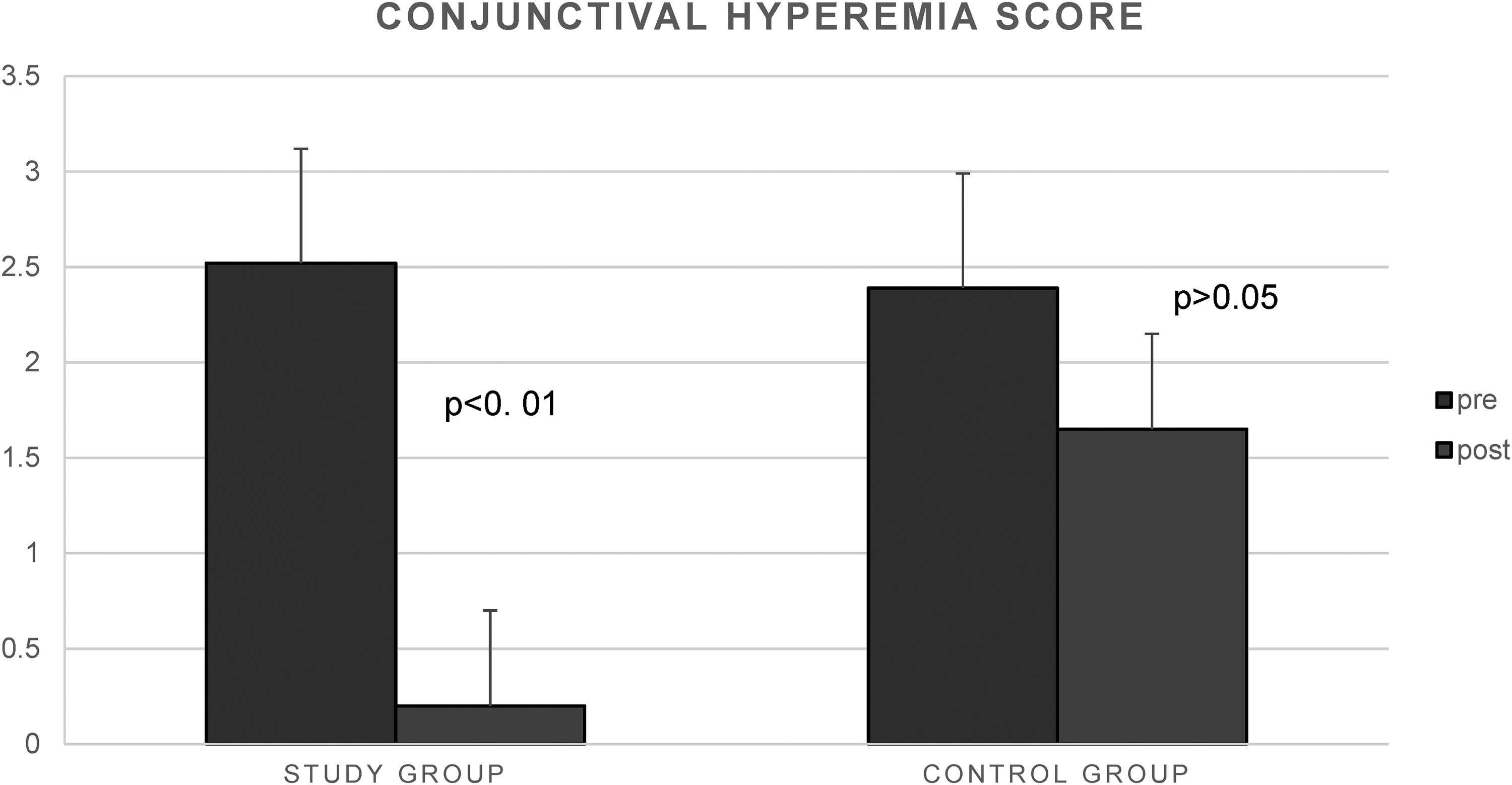
Conjunctival hyperemia score pre and post treatment.
Discussion
Ocular allergy and DED are ocular disorders often encountered in daily clinical practice. They are a therapeutic challenge which can reduce significantly quality of life and efficiency.20,21 Epidemiological studies showed that, in the general population, the prevalence of ocular allergy and DED ranged from 10% to 30% and from 5% to 50% respectively.7,20–22 However, even if ocular allergy seems to occur more frequently in younger patients,20,23 DED prevalence increases with age. 21 DED and ocular allergy are two different pathological conditions affecting the ocular surface. However certain clinical signs and symptoms are stackable. 24 Large cross-sectional studies showed that the coexistence of these two conditions was a common feature.24,25 Several studies tried to evaluate the link between DED and ocular allergy, suggesting that ocular allergy can predispose patients to DED. TFOS DEWS II in recent times included allergic conjunctivitis among possible risk factors for DED. 21 Ocular itching, swelling, and tearing are the most common symptoms reported by patients with the various forms of ocular allergy, whereas photophobia and pain are typical symptoms in patients with the most severe forms. These patients usually have corneal involvement (up to 70% of cases), with a range from superficial punctate keratitis to ulcers and plaques.22,26
Although the use of artificial tears has demonstrated success in reducing symptoms of irritation or decreasing ocular surface dye staining in DED, there have been no clinical trials to evaluate the efficacy of single components of the ocular lubricants in a pediatric population. 27
This study included a group of pediatric patients with clinical diagnosis of allergic conjunctivitis and dry eye disease. We analyzed specific parameters such as TBUT, Schirmer's test score, conjunctival hyperemia and OSDI score at baseline and after four weeks of treatment. The study group received Hyaluronic Acid 0.2%/arnica extract 0.1% while the control group Hyaluronic Acid 0.2%. The study group showed improvements in all the estimated clinical parameters after treatment. This study explored the pathophysiological hypothesis stating a relationship between inflammation and DED and AC. Inflammation, including innate immune response and adaptive response, is a key element of the vicious circle of DED. Mitogen-activated protein kinases and NF-kB signaling pathways, generation of inflammatory cytokines such as IL-1 and TNF-a and the upregulation of matrix metalloproteinases (MMP) production by epithelial cells are involved in acute response. Adaptive response is triggered by the activation and migration of resident antigen-presenting cells to the regional draining lymph nodes, in which they stimulate naive T cells (Th0), leading to the expansion of IL-17-g and IFN-g-secreting Th17 (Th17/1) cells.28–31
Allergen-induced conjunctival inflammatory response is associated with IgE-mediated mast cell activation, leading to the release of preformed mediators, including histamine and proteases (acute phase). The subsequent de novo formation of chemokines and cytokines triggers a cascade of cellular and molecular events, with the enrollment and activation of eosinophils and of Th2 and Th1 lymphocytes (late stage).30,32
Proteolytic enzymes, in particular MMP-9, play a key role in DED pathogenesis by disrupting intercellular epithelial tight junctions, leading to a breakdown of the ocular surface epithelial barrier. 28 MMP-9 has recently been proposed as one of the best biomarkers of DED severity 33 and as a diagnostic biomarker that can be assessed by a point-of-care immunoassay. 34
Elevated concentration of MMP-1, MMP-2, and MMP-9 in tears and elevated ratio of MMPs/tissue inhibitor have been well demonstrated in patients with vernal keratoconjuctivitis and in a minority of patients with allergic conjunctivitis.35,36 In patients with ocular allergy as well as in patients with DED, MMP-9 is significantly associated with corneal epithelial damage.
AM is a commercially available phytoterapeutic agent used as analgesic and anti-inflammatory agent in patients with acute trauma. 17 There is biologic plausibility supporting the potential effectiveness of Arnica as a modulator of the healing process in the postoperative period. Arnica has been showed to inhibit histamine release by mast cells, 37 neutrophil elastase, and NF-κB,38,39 which are involved in the inflammatory cascade.
This is the first study to document the effectiveness of combined topical Hyaluronic Acid 0.2%/Arnica extract 0.1% in reducing signs and symptoms of DED and AC in children. Preliminary findings suggest that AM can be effective in reducing dry eye symptoms in a selected pediatric population. Patients did not experience any adverse event. Further studies with larger sample sizes and extended follow-up periods are needed to validate our results.
Footnotes
Abbreviations
Authors’ contributions
LB, SP and MF conceived and designed the study, SP conducted the literature search. LB, SP and MF were involved in the analysis and interpretation of data. SP drafted the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article.
Consensus for publication
The study is being conducted in accordance with the declaration of Helsinki. Informed consent was obtained from all participants and their parents.
Competing interests
The authors declare that they have no competing interests.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The included studies have been approved by local ethics committees.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.