
Abstract
Purpose:
To explore the association between elevated blood aldosterone levels and papillophlebitis and retinal artery occlusion in a young, healthy woman.
Case description:
A 19-year-old woman with an unremarkable medical history presented with sudden-onset visual loss in the right eye, which lasted for 10 hours. Fundus examination revealed retinal whitening, splinter hemorrhages, disc swelling, and tortuous vessels in the right eye. Optical coherence tomography revealed inner retinal thickening. Fluorescein angiography demonstrated a delayed arteriovenous transit time and delayed filling of the cilioretinal artery circulation. Further workup showed a high aldosterone level and aldosterone-to-renin ratio. The patient was treated with steroid pulse therapy and combined intravitreal injection of dexamethasone implant and aflibercept. Visual acuity was recovered from count finger at initial presentation to 6/15 on the fifth day. For over 2 months, the fundal manifestations gradually subsided. Three months after the episode, her visual acuity further improved to 6/6.7.
Conclusion:
This report emphasizes the potential role aldosterone plays in the complex disease mechanism of retinal vasculopathy. In addition, steroid pulse therapy is more effective when applied in conjunction with combined intravitreal injection therapy for rescuing impaired vision caused by retinal vascular occlusion.
Introduction
Papillophlebitis, a non-ischemic inflammatory variant of central retinal vein occlusion (RVO) (CRVO), is an uncommon clinical condition that is more prevalent in young healthy adults. 1 In some cases, CRVO may be associated with retinal artery occlusion (RAO). The pathogenesis of concurrent retinal vein and artery occlusion remains unknown. Several underlying risk factors may be associated with occlusive retinal disorders, including hypertension, hyperlipidemia, atherosclerosis, and diabetes mellitus. Other factors include autoimmune and inflammatory diseases, hyperhomocysteinemia, protein C and S deficiency, and vitamin B6 and folic acid deficiency. 2 However, little is known about the association between aldosterone and occlusive retinal vascular disease. Herein, we report an incidental finding of increased blood aldosterone levels in a young healthy woman who had papillophlebitis with concurrent RAO, and the treatment effect of combination therapy with intravitreal dexamethasone implant and aflibercept injection.
Case description
Written informed consent was obtained from the patient to disclose identifiable information presented in this case report. A 19-year-old woman presented to the emergency department with sudden-onset visual loss in the right eye for 10 hours. She reported a similar episode lasting 10 minutes about 3 weeks ago. Her anamnesis revealed neither ocular nor systemic diseases, except myopia under orthokeratology. She also denied pain, traumatic injury, contact history, or drug abuse. Her initial blood pressure reading was 132/67 mmHg.
On ophthalmologic examination, her best-corrected visual acuity (BCVA) was count finger in the right eye and 6/6 in the left eye. Intraocular pressure measured with pneumotonometry was 26 and 11 mmHg in the right and left eye, respectively. Anterior segment examination was normal, and no cells were noted on slit-lamp examination in both eyes. Funduscopic examination of the right eye showed retinal whitening confined to the posterior pole, retinal splinter hemorrhages, disc swelling, and tortuous vessels (Figure 1(a)), whereas the left eye appeared grossly normal. No vitreous cells were observed. Optical coherence tomography (OCT) revealed inner retinal thickening in the right eye (Figure 1(b)), and OCT angiography showed decreased macular vessel density. Fundus fluorescein angiography demonstrated a delayed arteriovenous transit time and delayed filling of the cilioretinal artery circulation (Figure 2(a) and (b)), but no marked vascular leakage was observed at all times. Due to the ischemic retinal condition, the patient immediately received hypotensive medication and anterior chamber paracentesis, and steroid pulse therapy (1 g/day) was administered for three consecutive days, followed by tapering with oral prednisolone. The patient also received combination therapy with an intravitreal dexamethasone implant and aflibercept injection on the second day.
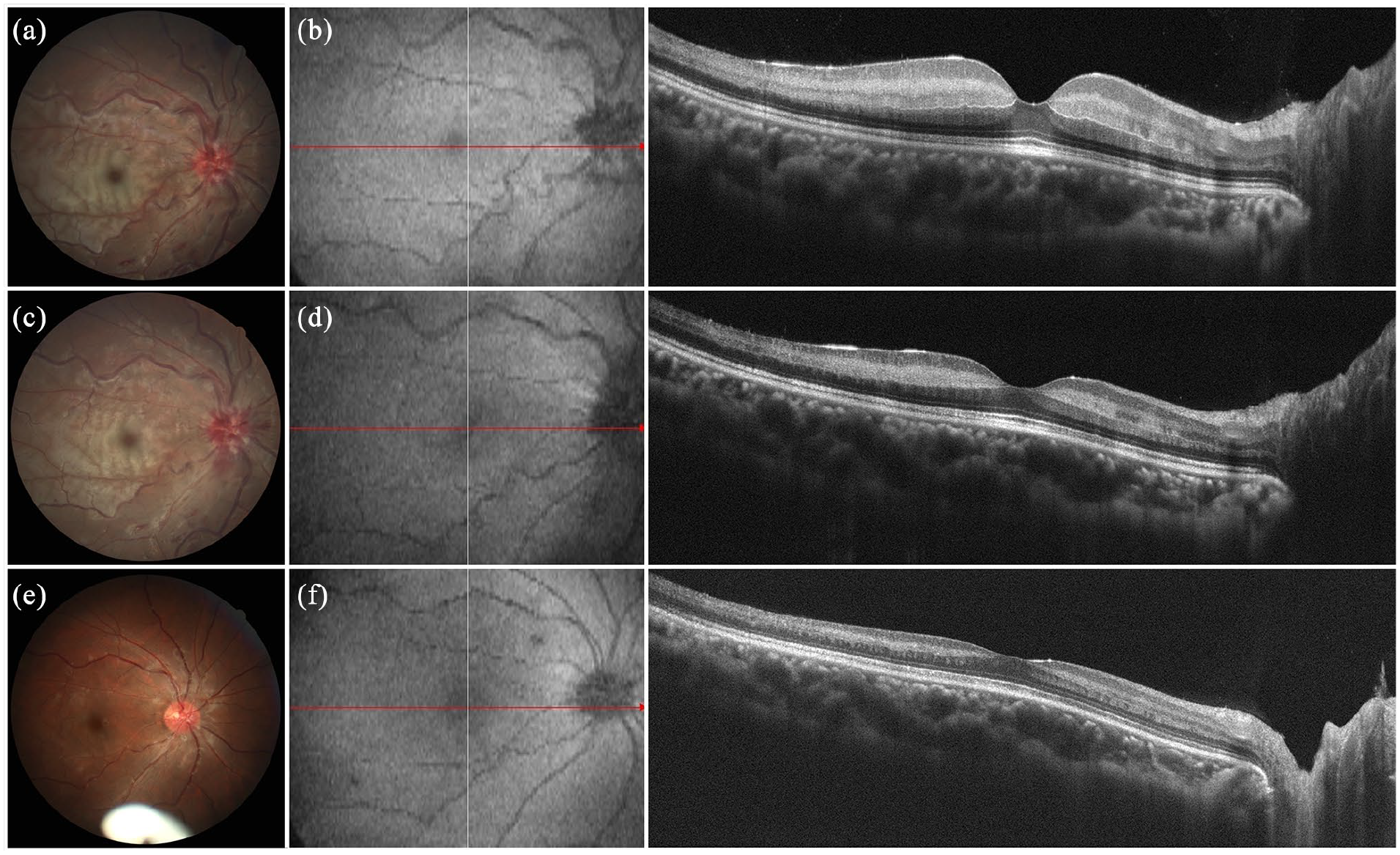
(a) Fundal findings at the first visit. Retinal whitening, hemorrhages, disc swelling, and tortuous vessels were noted. (b) The optical coherence tomography (OCT) revealed profound swelling of the inner retinal structure. (c and d) Colour photograph and OCT after 5 days. (e and f) After 2 months, the fundal examination showed a complete resolution of disc swelling, retinal whitening, and hemorrhage. The remnant of the intravitreal dexamethasone implant was observed.
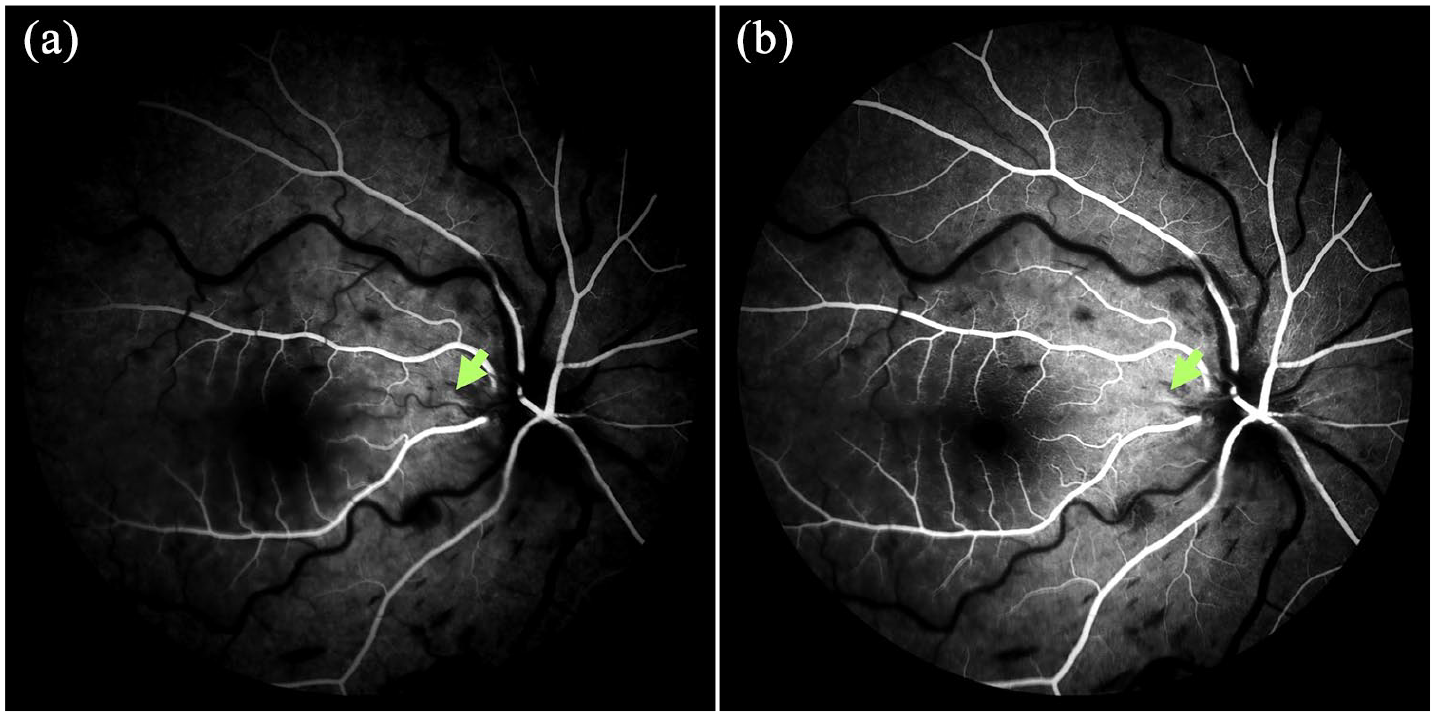
(a and b) Fluorescein angiography showed delayed presence of the cilioretinal artery (green arrow).
Extensive laboratory workup, including blood count, erythrocyte sedimentation rate (ESR), protein C, protein S, lipid profile, coagulation profile, D-dimer, prothrombin time, antithrombin, plasma viscosity, immunoglobulins, antinuclear antibody, ds-DNA, anticardiolipin antibody, antineutrophil cytoplasmic antibodies, anti-cyclic citrullinated peptide antibody, rapid plasma regain, aldosterone, renin, and homocysteine levels, were ordered to identify the underlying cause. The laboratory findings only showed a mild elevation in ESR. Surprisingly, the level of aldosterone, which was tested after lying down for 30 minutes, was 335 pg/ml (normal:10–160 pg/ml), and the aldosterone-to-renin ratio was 32.3. Abdominal ultrasound and magnetic resonance imaging, chest computed tomography, and carotid Doppler ultrasonography all yielded negative results.
After the initiation of steroid pulse therapy, the patient’s BCVA gradually improved and reached 6/15 in the right eye on the fifth day. After 1 month, her blood aldosterone returned to 33.4 pg/ml, and the aldosterone-to-renin ratio was 5.79. During the 2-month follow-up period, the disc swelling, retinal whitening, and pre-retinal hemorrhage had resolved (Figure 1(c–f)). The patient’s BCVA further improved to 6/6.7 in the right eye 3 months after the acute episode.
Discussion
To the best of our knowledge, this is the first report to demonstrate the association between aldosterone, papillophlebitis, and RAO. Previously, Demirok et al. reported a case of unilateral papillophlebitis and CRAO in a 23-year-old young female. 3 The patient presented with a very poor visual acuity (BCVA of 20/200), which recovered to 20/20, 20 days after the initial presentation without any medical or surgical intervention except on oral acetylsalicylic acid 100 mg/day. Similar to our case, the laboratory survey yielded positive results for slightly elevated white blood cells, ESR, and C-reactive protein; the radiologic imaging studies were all negative. Unexpectedly, they found a mutation in the gene encoding methylenetetrahydrofolate reductase. However, in our case, the homocysteine level was within the normal range, excluding the possibility of hyperhomocysteinemia-related thromboembolic events. However, the laboratory data were remarkable for an elevated blood level of aldosterone and a high aldosterone-renin ratio only.
Several hypotheses may explain the increased level of blood aldosterone in patients with retinal vasculopathy. Aldosterone plays a role in regulating the immune response in retinal vascular disease via different mechanisms. First, aldosterone may potentiate its oxidative capacity by increasing the production of oxygen radicals through the upregulation of the nicotinamide adenine diphosphate oxidase complex in the endothelium. 4 This can lead to thrombosis and fibrosis in the retinal vasculature and increased inflammatory response.4 –6 In 2009, Berka-Wilkinson et al. 6 showed that the renin-angiotensin-aldosterone system had an in vivo effect on retinal microvascular cells by cultured endothelial cells (EC) and a model of oxygen-induced retinopathy (OIR). The authors found a positive correlation between the administration of aldosterone and an increase in EC tubulogenesis, and that the process of neovascularization could be enhanced by aldosterone and inhibited by mineralocorticoid receptor (MR) antagonists or aldosterone synthase in the OIR model. 6 This evidence may emphasize the role of aldosterone in retinal vascular disorders.
Second, aldosterone can mediate the inflammatory response through the recruitment of macrophages into the retinal vasculature. Several studies involving animal models of RVO were undertaken to prove this phenomenon. Allingham et al. 7 used immunohistochemistry to examine the retina tissues and found that mice with RVO exposed to aldosterone had higher numbers of infiltrating mononuclear phagocytes than the control. Similarly, Ebneter et al. 8 reported macrophage aggregation into the retina caused by the macrophage invasion from the systemic circulation, following hypoxia and the disruption of the blood-retinal barrier in experimental BRVO mice. Aldosterone could also upregulate the expression of monocyte chemoattractant protein-1 mRNA and the endothelial leukocyte adhesion protein, such as intracellular adhesion molecule 1 gene, leading to retinal inflammation.4,6
Third, aldosterone could also target Müller glial cells, as Müller cells are composed of a high-level MR expression. 7 Because Müller cells are critical for homeostatic and metabolic support of retina neurons, the disruption of Müller cells could lead to dysfunction of retina neurons.7,8 Previous studies have reported that aldosterone may affect the function of Müller cells by altering the distribution and localization of ion channels, such as aquaporin4 and Kir4.1, leading to pumping dysfunction and subsequent development of vascular leakage and tissue edema. 7
Based on the clinical appearance of a fern-like pattern, papillophlebitis associated with paracentral acute middle maculopathy should be considered. Currently, there are no consensus guidelines for the treatment of papillophlebitis concurrent with RAO. Several regimens, including systemic, periocular or intravitreal corticosteroid therapy, intravitreal injection of anti-vascular endothelial growth factor (anti-VEGF) agents, platelet inhibitors, as well as anticoagulants therapy have been reported for the treatment of papillophlebitis,.9,10 However, none reported the treatment combining dexamethasone implant and aflibercept injection. Our case showed a relatively rapid improvement in BCVA, BCVA recovery and a complete resolution of macular edema during the follow-up visits after the initiation of the pulse therapy followed by a combination therapy using anti-VEGF agents and dexamethasone intravitreal implant, suggesting a certain treatment effect in such cases.
In summary, our report highlights the role of aldosterone in the complex pathogenesis of retinal vascular diseases. Since the exact mechanism of aldosterone-related retinal vasculopathy remains poorly understood, further research is necessary to elucidate the underlying mechanisms and explore the therapeutic potential of aldosterone-targeted strategies to treat retinal vascular diseases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.