
Abstract
Purpose:
INVICOST, a medico-economic analysis, compared costs of managing treatment-naive patients with diabetic macular edema (DME) receiving intravitreal injections (IVIs) of aflibercept (AFL), dexamethasone implant (DXI) or ranibizumab (RAN) over 1 year.
Methods:
Healthcare resource use and associated costs were estimated using individual patient data from INVICTUS, a prospective, open-label, monocentric study. Healthcare costs comprised direct medical costs such as drug acquisition and administration, consultations and ophthalmological procedures. Costs were assessed from the French National Health Insurance perspective using published national tariffs expressed in 2019 euros.
Results:
Of the 60 treated eyes, 48 had no treatment switch; 14 received AFL, 19 received DXI and 15 received RAN. AFL-treated eyes received an average of 6.5 IVIs, DXI-treated patients received 2 IVIs and RAN-treated received 6.8 IVIs. All treated eyes received an initial prescription for adjunctive ocular medications and 349 follow-up procedures were performed including an average of 3.9 optical coherence tomography and 3.2 retinography procedures per eye. Average total direct cost of per-eye treatment was €4516 (€1128–€8257). Average cost was €5782 for eyes treated with AFL, €2779 with DXI and €5536 with RAN. Drug therapy was the cost driver: €4394 (76%) for AFL, €1915 for DXI (69%) and €4268 (77%) for RAN.
Conclusion:
The difference in total treatment cost is largely explained by the significantly lower frequency of IVI and annual cost of therapy with DXI, compared with AFL and RAN. INVICOST is the first study comparing treatment costs with AFL, DXI and RAN in France in current clinical practice.
Keywords
Introduction
In France, more than 5 million people are reported to have diabetes, of which types 1 and 2 account for 6% and 92% of cases, respectively. 1 Diabetic retinopathy (DR) is a serious complication of diabetes (estimated to occur in approximately 35% of individuals with diabetes worldwide); its prevalence is higher in type 1 diabetes than in type 2 (77% vs 25%). 2 As the severity of DR advances, vision-threatening diabetic macular edema (DME, 6.8% of DR) and proliferative retinopathy (7% of DR) can occur. 2 DME causes a decrease in visual acuity, which can progress to blindness when it affects the centre of the macula. In France, the estimated prevalence of DME is 3% of the diabetic population, which encompasses more than 100,000 individuals. 3
The treatment of DR and DME has changed considerably with the availability of intravitreal formulations of anti-vascular endothelial growth factor (anti-VEGF) agents and corticosteroids, relegating focal/grid macular laser to a treatment option in patients intolerant of or unresponsive to anti-VEGFs. In France, ranibizumab (RAN; Lucentis®, Novartis, Basel, Switzerland) became available in 2011. 4 A few years later, the therapeutic arsenal for treatment of DME expanded with the arrival of the anti-VEGF agent aflibercept (AFL; Eylea®, Bayer, Leverkusen, Germany), approved for this indication in March 2015, 5 and the sustained-release corticosteroid, dexamethasone implant (DXI; Ozurdex®, Allergan, an AbbVie company, North Chicago, IL, USA), available since 2014. 6 Intravitreal injection (IVI) methods, injection schedules and recommended follow-up visits vary amongst these agents. In 2017, the European Society of Retina Specialists published guidelines in which AFL, DXI and RAN were suggested as standard care in the treatment of DME. 7 These agents all require regular repeated injections which is burdensome for patients highlighting the advantages of long-lasting treatment options.
The efficacy and safety of RAN and AFL in the treatment of DME have been compared in at least one large, multicentre, randomized trial, 8 but there is a paucity of data comparing the differences between corticosteroids and these agents. The INVICTUS study was the first to compare the efficacy of these three treatments (RAN, AFL and DXI) with 6-month 9 and 12-month follow-up 10 in a real-life setting in France.
IVI therapies represent a considerable economic burden for the French National Health Insurance (NHI) system. In 2018, French NHI expenses for reimbursed IVI therapies amounted to €326.6 million for AFL, €47.0 million for DXI and €421.7 million for RAN, representing a 15.4% increase compared with 2017. 11
In addition to the cost of IVI therapies, the direct medical costs of treatment also include follow-up procedures, adjunctive ocular medications, medical transportation and the treatment of complications. No studies have been published thus far in France assessing and comparing the costs associated with the use of each agent from the perspective of the French NHI.
In this prospective, open-label monocentric INVICTUS study,9,10 consecutive patients with treatment-naïve DME were enrolled. No significant differences in baseline characteristics including visual acuity, central retinal thickness (CRT) and glycated hemoglobin were reported. Mean baseline best-corrected visual acuity (BCVA) in Early Treatment Diabetic Retinopathy Study letters was 57 ± 13.6, 59 ± 15.2 and 62.4 ± 14.1, in the AFL, DXI and RAN treatment groups (p = 0.36), respectively. Mean baseline CRT was 469.6 ± 104.2, 464.5 ± 152.6 and 450.1 ± 82.9, in the AFL, DXI and RAN groups (p = 0.86), respectively. Over 6 and 12 months, AFL, DXI and RAN were shown to have comparable clinical efficacy in improving BCVA and CRT in this real-life setting. Intraocular pressure was stable in the AFL and RAN groups and 19% (n = 4) of patients experienced an IOP ⩾25 mmHg or an increase ⩾10 mmHg controlled with local treatment.9,10 Using the data from INVICTUS, we performed a cost-minimization analysis to compare healthcare resource utilization (HCRU) and associated costs of managing DME with each of these agents.
Material and methods
Study design
Based on the comparable efficacy of AFL, DXI and RAN on visual and anatomic outcomes in the INVICTUS study, INVICOST was designed as a cost-minimization analysis whose objective was to compare the management costs for treatment-naive patients with DME receiving AFL, DXI or RAN.
The analysis, was performed using primary data from the INVICTUS study, a prospective, nonrandomized, open-label, noninterventional, single-centre study conducted between January 2016 and January 2017 at the ophthalmology department of Hôpital Nord, Marseille. Patients presenting with treatment-naive DME and prescribed IVI AFL (2.0 mg), DXI (700 µg) or RAN (0.5 mg) were included consecutively (to limit selection bias) and were followed for 1 year. The choice of treatment was left to the discretion of the prescribing physician.
Data collection for the INVICOST analysis included patient-level demographic and clinical data (age, gender, place of residence, treatment laterality and treatment switch) and HCRU data (agents administered for treatment of DME, number of injections per agent, adjunctive ophthalmic therapies, ophthalmologic procedures, follow-up consultations, surgical treatment of complications and travel costs).
Cost estimation and data analysis
HCRU data were retrospectively collected from treatment initiation (i.e. first consultation or first IVI) through 12 months maximum. All resources captured across the data collection period were included in this economic analysis, regardless of duration of follow-up. HCRU data included all direct medical resources related to IVI (including drug acquisition and administration), ophthalmologic procedures, follow-up consultations, adjunctive eye treatments and surgeries and travel costs.
Costs were assessed from the French NHI perspective, using published national tariffs and were expressed in 2019 euros (Table 1). Due to the chronic medical condition of this diabetic patient population, all expenses were assumed to be fully supported by NHI. The mean cost per treated eye was calculated over the 1-year study period.
Unit costs for the valuation of healthcare resource use.
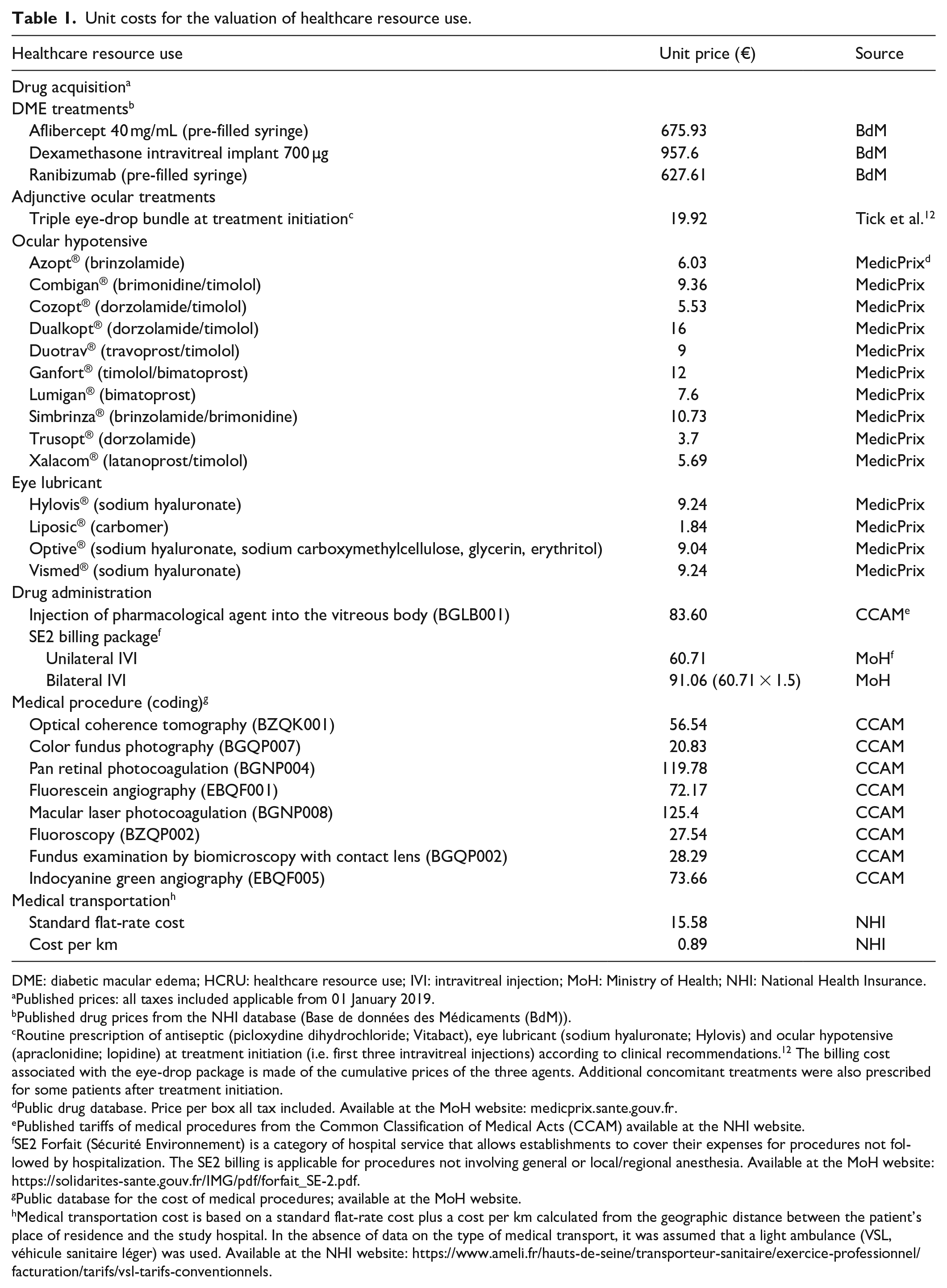
DME: diabetic macular edema; HCRU: healthcare resource use; IVI: intravitreal injection; MoH: Ministry of Health; NHI: National Health Insurance.
Published prices: all taxes included applicable from 01 January 2019.
Published drug prices from the NHI database (Base de données des Médicaments (BdM)).
Routine prescription of antiseptic (picloxydine dihydrochloride; Vitabact), eye lubricant (sodium hyaluronate; Hylovis) and ocular hypotensive (apraclonidine; Iopidine) at treatment initiation (i.e. first three intravitreal injections) according to clinical recommendations. 12 The billing cost associated with the eye-drop package is made of the cumulative prices of the three agents. Additional concomitant treatments were also prescribed for some patients after treatment initiation.
Public drug database. Price per box all tax included. Available at the MoH website: medicprix.sante.gouv.fr.
Published tariffs of medical procedures from the Common Classification of Medical Acts (CCAM) available at the NHI website.
SE2 Forfait (Sécurité Environnement) is a category of hospital service that allows establishments to cover their expenses for procedures not followed by hospitalization. The SE2 billing is applicable for procedures not involving general or local/regional anesthesia. Available at the MoH website: https://solidarites-sante.gouv.fr/IMG/pdf/forfait_SE-2.pdf.
Public database for the cost of medical procedures; available at the MoH website.
Medical transportation cost is based on a standard flat-rate cost plus a cost per km calculated from the geographic distance between the patient’s place of residence and the study hospital. In the absence of data on the type of medical transport, it was assumed that a light ambulance (VSL, véhicule sanitaire léger) was used. Available at the NHI website: https://www.ameli.fr/hauts-de-seine/transporteur-sanitaire/exercice-professionnel/facturation/tarifs/vsl-tarifs-conventionnels.
HCRU and cost analyses were conducted in two study populations: the intent-to-treat (ITT) population of all treated eyes (with and without treatment switch during follow-up) and the subgroup of eyes that were not subject to treatment switch. The primary cost analysis included eyes without treatment switch to allow comparison of individual treatment costs. The secondary cost analysis included all treated eyes to provide an estimate of overall treatment cost per study eye. Analyzing a treatment-naive population (i.e. population of INVICTUS) permits economic analysis of a homogeneous population.
The mean duration of follow-up was estimated for all treated eyes and for each treatment group (AFL, DXI and RAN) without treatment switch. The duration of follow-up was estimated from the date of the first consultation or first IVI to the date of the last documented consultation or IVI. The analysis was performed at eye-level since patients could potentially have received bilateral treatment for DME.
Descriptive statistics were used to summarize the population characteristics (age, gender and eye laterality) at the patient level, and HCRU at the eye level. In view of the small sample size, nonparametric statistics (Wilcoxon signed rank test and Fisher’s exact test) were used for intergroup comparisons of baseline characteristics and treatment costs.
Results
Study population
In total, 47 treatment-naive patients with DME were included in the analysis and followed between January 2016 and January 2017. The mean age was 67 years (min–max: 48–86 years) and 53% were women. Most patients (72%, n = 34) had unilateral DME. There was no significant difference in baseline demographic or characteristics across treatment arms (Table 2).
Baseline characteristics of the study population.
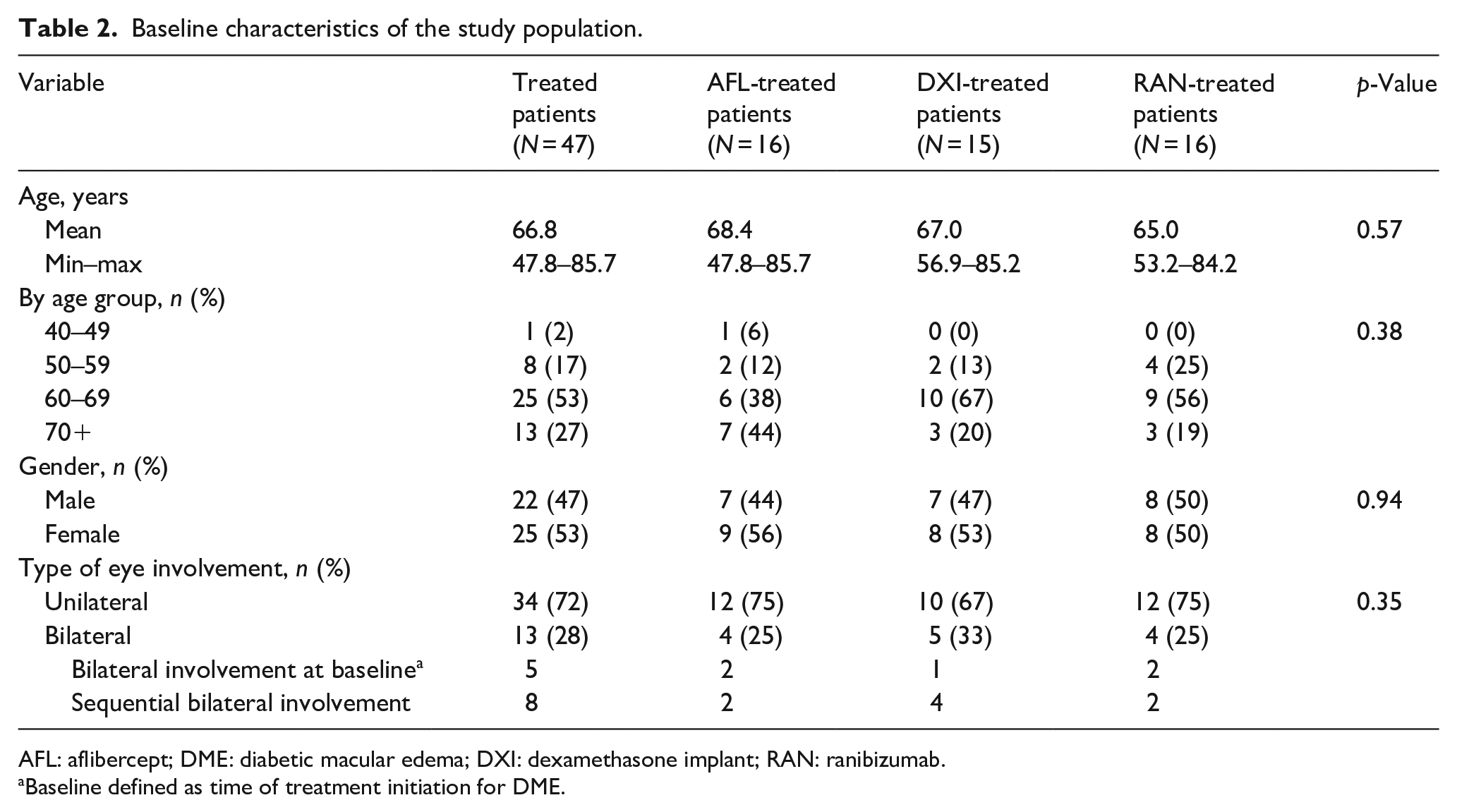
AFL: aflibercept; DME: diabetic macular edema; DXI: dexamethasone implant; RAN: ranibizumab.
Baseline defined as time of treatment initiation for DME.
In total, 60 treated eyes were included in the analysis, of which 20 initiated treatment with AFL, 21 initiated treatment with DXI and 19 initiated treatment with RAN. Amongst these, 48 eyes were not subjected to treatment switch (Figure 1).
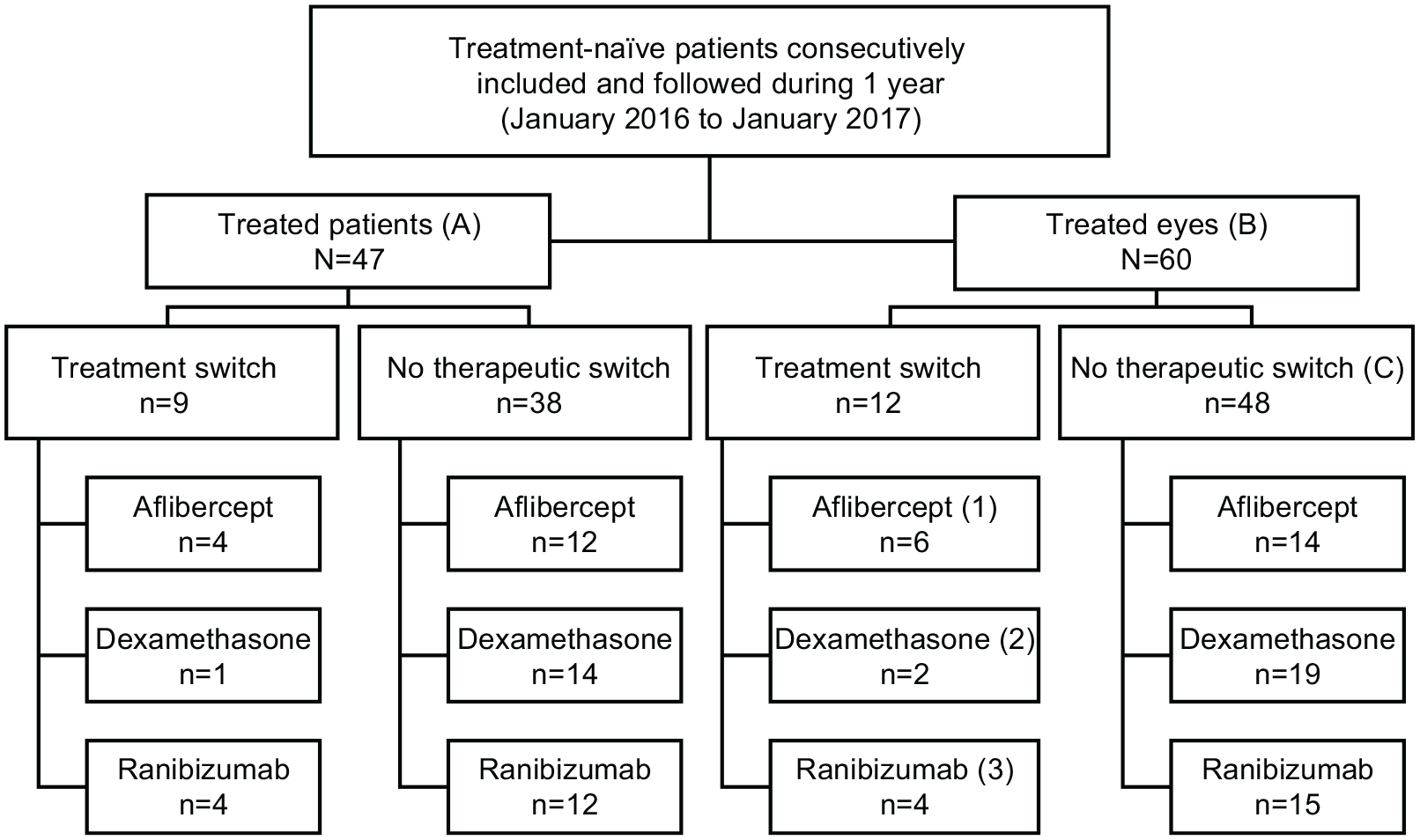
Flow chart of the analysis populations.
The mean (±SD) duration of follow-up was estimated at 292 ± 69 days (range: 72–368) (9.7 months) for all treated eyes (N = 60). For eyes without treatment switch (N = 48), the mean (±SD) duration of follow-up was estimated at 312 ± 52 days (range: 188–360) for AFL-treated eyes (10.4 months), 266 ± 81 days (range: 72–350) (8.9 months) for DXI-treated eyes and 298 ± 71 days (range: 94–358) (9.9 months) for RAN-treated eyes.
Healthcare resource use costs
For all treated eyes (N = 60), 292 IVIs were performed (118, 120 and 54, respectively, for AFL-, RAN- and DXI-treated eyes) over the follow-up period. All patients received routine adjunctive picloydine/hyaluronate/apraclonidine eye drops on initiation of study treatment and 44.7% (21/60) received vouchers for medical transportation (145 vouchers), representing a mean of 3.6 vouchers per patient. The mean distance between the patient’s place of residence and the study hospital was 19 km.
For treated eyes that did not require a switch in therapy (N = 48), 231 IVIs were performed, corresponding to an average of 6.5 IVIs for AFL-treated eyes, 2.0 IVIs for DXI-treated eyes and 6.8 IVIs for RAN-treated eyes. During follow-up, 28% of eyes in this subgroup required lubricant eye-drops, with use being slightly higher in eyes treated with AFL and RAN than in DXI-treated eyes (respectively, 36%, 33% and 16%). In total, 275 follow-up medical consultations were performed in the 48 eyes that did not require a therapy switch (mean 4.6 consultations per treated eye). RAN-treated eyes had slightly fewer consultations than AFL- and DXI-treated eyes (respectively, 3.8, 4.6 and 5.1). Regarding ophthalmic procedures, 3.9 optical coherence tomography and 3.2 retinography examinations were performed on average per treated eye. Only three eyes underwent surgical interventions during follow-up (1-day cataract surgery: two in DXI-treated eyes and one in AFL-treated eyes) (Table 3).
Healthcare resources use (eye-level) during follow-up.
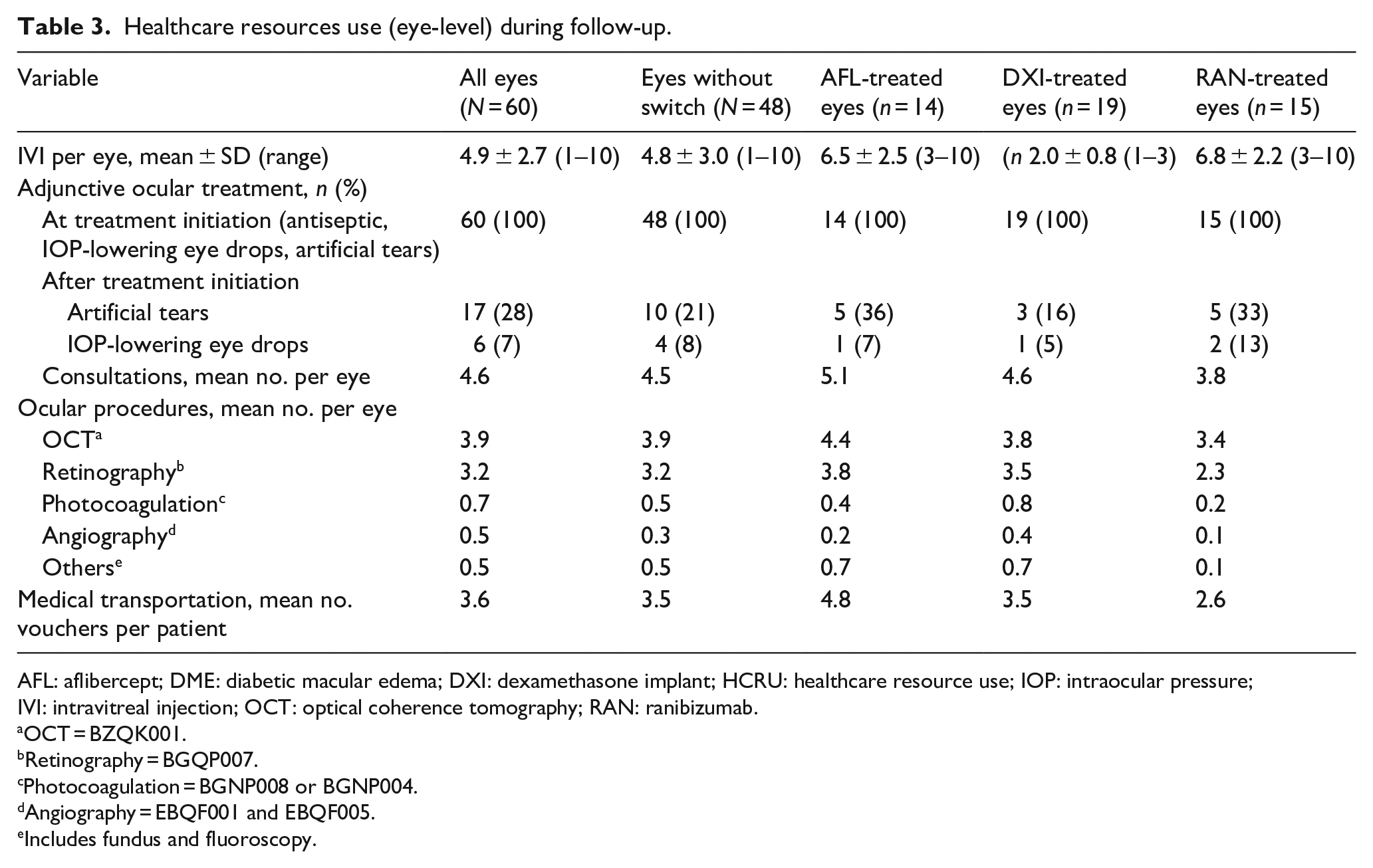
AFL: aflibercept; DME: diabetic macular edema; DXI: dexamethasone implant; HCRU: healthcare resource use; IOP: intraocular pressure; IVI: intravitreal injection; OCT: optical coherence tomography; RAN: ranibizumab.
OCT = BZQK001.
Retinography = BGQP007.
Photocoagulation = BGNP008 or BGNP004.
Angiography = EBQF001 and EBQF005.
Includes fundus and fluoroscopy.
In all treated eyes (N = 60), the mean total direct medical cost per treated eye was €4626 (range: €1128–8256), with an average of 4.9 IVI per eye during the approximate 9.7 months of follow-up. Drug acquisition cost was the major component, representing €3436 on average (74% of total cost), followed by the IVI administration costs (mean €649, 14%) and ophthamological procedures (mean €311, 7%).
For the population of all treated eyes, mean treatment cost increased with the number of IVIs performed per eye: €5719 for 6.2 IVI on average for AFL-treated eyes, €2834 for 2.1 IVI on average with DXI-treated eyes and €5458 for 6.6 IVI on average with RAN-treated eyes (Figure 2(a)).
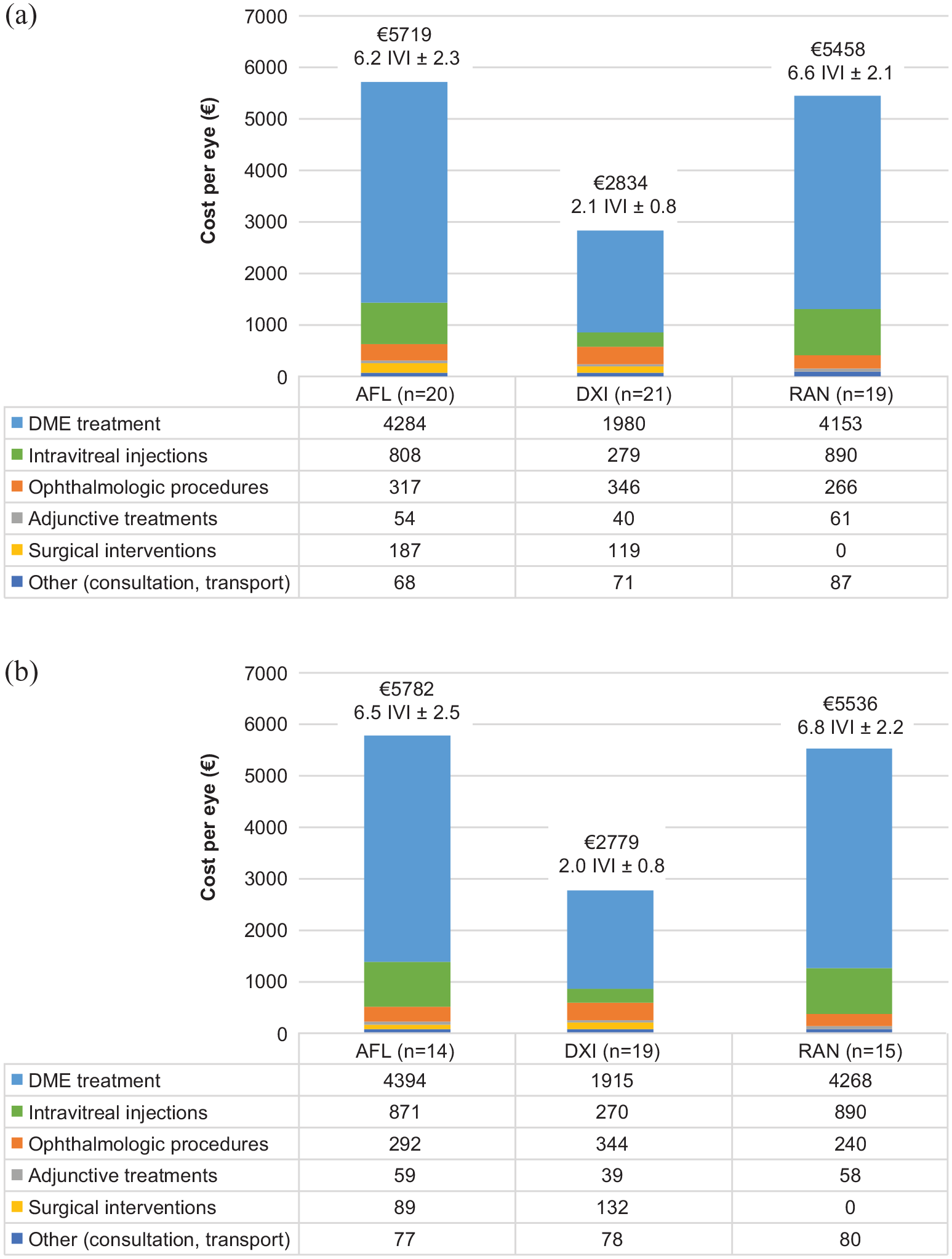
Breakdown of total treatment cost by drug for (a) all treated eyes and (b) eyes without treatment switch.
In the population of eyes that did not switch treatment (N = 48), the mean total treatment cost per eye was €4516 (range: €1128–8257). A breakdown of treatment costs by drug for this population is presented in Figure 2(b).
Discussion
This cost-minimization analysis compared for the first time the cost of managing treatment-naive DME patients with AFL, DXI or RAN from the perspective of the French NHI in the French clinical practice setting. The results indicated that the total treatment cost of managing DME was lower with DXI than with RAN or AFL. This difference was mainly driven by the lower number of IVIs performed in the DXI treatment arm (mean 2.0) compared to the RAN and AFL treatment arms (mean 6.8 and 6.5, respectively) over the follow-up period (mean ~10 months). The need for three initial monthly loading doses with anti-VEGFs, but not with DXI, helps to explain this cost difference. This finding corroborates the results of a previous Korean study conducted in a DME population comprising incident as well as prevalent cases, which showed a 33% lower treatment cost for DXI compared to RAN and AFL over a 12-month period. 13
The frequency of injection of anti-VEGF agents in this study is lower than the currently recommended frequency of injection as per the treat-and-extend (T&E) protocol,14,15 which aims to maintain patients’ visual acuity in the long term while reducing the number of follow-up visits, procedures and injections. This is explained by the fact that the INVICTUS study was conducted in 2016–2017, before the implementation of the T&E protocol. Thus, the current cost estimation probably underestimates the cost of managing DME for the three molecules but this does not bias the comparison between the three molecules. However, for DXI, in clinical practice, there is a consensus on early re-injections (i.e. usually 3–4 months after the first injection). Real-life clinical practice is reflected by the results of the INVICTUS study, in which the mean (±SD) number of IVIs at 6 months of follow-up is approximately 4.6 ± 1.1 for AFL-treated eyes, 1.4 ± 0.5 for DXI-treated eyes and 4.8 ± 0.8 for RAN-treated eyes. 9 However, our results are consistent with a literature review of observational studies on the treatment of the DME. 16
In the INVICOST analysis, it should be noted that the mean number of IVIs reported is lower than that reported in the INVICTUS study at 12 months. 10 This difference is explained by the fact that analyses in the INVICTUS study were confined to study eyes completing the 12-month treatment period, whereas in INVICOST the analyses were performed in eyes with varying treatment durations (to reflect the actual cost of managing patients in a real-life setting in accordance with the study objective).
Compared to RAN-treated eyes, DXI-treated eyes were subject to a slightly higher frequency of follow-up visits (mean 4.6 vs 3.8), which is consistent with the fact that corticosteroid use requires systematic control of intraocular pressure (IOP) and monitoring of efficacy to anticipate the recurrence period, whereas RAN requires a loading dose without intermediate control. However, in this study, the need for IOP control and monitoring appeared to contribute little to the overall cost. The difference might also be expected to diminish during the second year of follow-up, as the treating physician becomes more familiar with the individual patient’s DXI dosing requirements. In contrast, AFL-treated eyes experienced more follow-up visits than DXI-treated eyes (mean 5.1 vs 4.6); this may be related to the longer duration of follow-up (mean 10.4 months) and higher number of OCT/retinography procedures observed in the AFL treatment cohort, or it may possibly indicate selective use of AFL in patients with more advanced disease.
In terms of treatment switch, all treatment switches observed in this study are consistent with published data17,18 and are generally explained by lack of efficacy, safety (e.g. IOP increase) or the need for reducing the frequency of injection.
Regarding medical procedures, it should be noted that there is probably an over-representation of retinography procedures in this patient population; retinography is a technique that is, usually available in larger centres and allows for precise and rapid analysis, but which is less frequently performed in private practice. This would explain the under-reporting of fundus examinations performed in this study. This observation highlights one of the main limitations of this analysis, namely the small sample size. A multicentre study with a larger sample size would provide better representation of intercentre variation in the use of healthcare resources in real-life practice.
In addition to the variable duration of study follow-up for the three treatment arms that could be a potential confounder of HCRU, this analysis does not take into consideration the future occurrence (beyond year 1) of cataracts, whose frequency is expected to be higher with corticosteroids than with anti-VEGF treatments. Indeed, cataracts usually appear during the second year of treatment. 6 The need for surgical intervention was only captured during the 12 months of follow-up. A longer period of follow-up would likely have narrowed the treatment cost advantage associated with DXI use. Despite this limitation, it should be noted that there was no significant difference between the three treatment groups in proportion of phakic patients at baseline (59% in AFL group, and 57% in DXI group and 53% in RAN group). 9
Another study limitation is the shortage of information on the transport demands placed on patients in traveling to the study centre: travel distance was considered identical for all patients residing in the conurbation of Marseille. In the absence of the type of medical transportation used, the most expensive mode of transport (VSL) was assumed to avoid underestimation of travel costs.
Conclusion
The INVICTUS study demonstrated that, in the real-life setting, intravitreal corticosteroid and anti-VEGF treatments produced comparable visual and anatomic outcomes at 6 and 12 months of follow-up in patients with treatment-naive DME. Within this clinical practice setting, the use of corticosteroids appears to be the less expensive treatment option over the first 10 months of treatment. Practitioners may need to weigh the possible occurrence of cataract or IOP elevation typically reported with corticosteroid use against the cost advantage of corticosteroids and their less frequent injection scheme that can contribute to reducing the burden of injections for certain patients.
Footnotes
Acknowledgements
Editorial assistance was provided to the authors by Evidence Scientific Solutions, Inc, Philadelphia, PA, and funded by Allergan, an AbbVie company.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Pierre Gascon reports no conflicts of interest. Isabelle Borget reports consultancy fees from Allergan (an AbbVie company). Alban Comet reports consultancy fees from Allergan (an AbbVie company) and Bayer. Frédéric Matonti reports consultancy fees from Allergan (an AbbVie company), Alcon, Bayer, Bausch & Lomb, Horus, Novartis and Théa. Laurence Carton and Laure Dupont-Benjamin are employees of AbbVie. All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Allergan (prior to acquisition by AbbVie Inc.).