
Abstract
Objective
Oxytocin induction is a commonly used intervention during childbirth worldwide. This study aimed to compare the pain and stress levels of newborns born to mothers who administered synthetic oxytocin at birth with those who did not.
Methods
This quasi-experimental study included 164 participants and their newborns who were delivered vaginally in a public hospital. The data were collected using an Information Form, a Neonatal Follow-Up Form, and the Assessment of Neonatal Pain and Stress Scale (ALPS-Neo).
Results
In the study, there were no differences between the two groups in terms of the participants’ and newborns’ demographic characteristics (p > .05). During and after drying, before, during, and after the first injection, and before, during, and after blood glucose measurement, the mean ALPS-Neo scores were higher in the oxytocin induction group, with the difference being statistically significant (p < .001).
Conclusion
Although the data presented here are observational, the findings indicate that infants born to participants who underwent oxytocin induction exhibit more intense pain and stress responses. The pain-stress scores of newborns born to participants who underwent oxytocin induction were higher than those of newborns whose mothers did not receive oxytocin induction.
Introduction
Induction of labor refers to all interventions aimed at stimulating uterine contractions to initiate or accelerate the labor process (Sanchez-Ramos et al., 2024; Summers, 1997; Visscher, 1978). Induction of labor is one of the most commonly performed interventions during childbirth worldwide (NICE, 2021; Smith, 2006). According to data on maternal and perinatal health from the World Health Organization (WHO), which involves approximately 303,000 births across 24 countries, labor induction was performed in nearly 10% of the deliveries (WHO, 2018). Labor induction is performed either with or without rupture of the amniotic sac, based on the characteristics of the cervix, and involves mechanical or pharmacological stimulation of contractions before the onset of labor (Gupta et al., 2022; Shahabuddin & Murphy, 2022). Synthetic oxytocin is quite popular in this regard and is undoubtedly the most commonly used drug during the peripartum period. Between 1998 and 2007, the incidence of labor induction more than doubled, increasing from 9.8% to 23% (Giri et al., 2022; Monks & Palanisamy, 2021). Oxytocin improves maternal and neonatal health. Maternal benefits include reduced cesarean rates, postpartum bleeding, and maternal mortality, whereas neonatal benefits include reduced meconium aspiration syndrome, neonatal sepsis, and admission rates to neonatal intensive care units (Grobman et al., 2018; Middleton et al., 2020; Monks & Palanisamy, 2021). In cases of improper use, oxytocin can lead to adverse effects, such as uterine tachysystole, uterine contraction abnormalities, and fetal distress. Given these risks, it has been classified as a “high-risk drug” by the Institute for Safe Medication Practices (Clark et al., 2009; Rooks, 2009). Additionally, evidence suggests that the complication rates may be higher in women who undergo synthetic oxytocin induction than in those undergoing spontaneous vaginal labor. Oxytocin induction is associated with complications such as hyperstimulation, cesarean delivery, hypotension, antidiuretic effects, neonatal hyperbilirubinemia, uterine rupture, fetal distress, and others (Clark et al., 2009). In a review study by Monks et al. (2021) on the effects of oxytocin, it was emphasized that oxytocin may be associated with postpartum depression, breastfeeding difficulties, neonatal neurodevelopmental disorders, and chronic pain in newborns (Monks & Palanisamy, 2021). For the past 60 years, the use of oxytocin for labor induction has become increasingly common, with research primarily focusing on examining uterine contractions and maternal effects (Arrowsmith & Wray, 2014; Daly et al., 2020). However, despite evidence suggesting that oxytocin may reduce placental perfusion and enter fetal circulation (Nathan et al., 2021; Tyzio et al., 2006), it remains unclear whether it affects the fetus (Giri et al., 2022; Kenkel et al., 2019; Palanisamy et al., 2018). The aim of this study was to compare the early neonatal pain and stress levels of newborns born to participants who received synthetic oxytocin induction during labor with those who did not.
Hypotheses
Methods
Design and Setting
The study was designed as quasi-experimental research. The study population consisted of women who delivered vaginally at a training and research hospital in Turkey.
Participants
The sample size of the study was calculated using the G*Power 3.1.9.2 program based on the mean and standard deviation values of neonatal pain scores reported by Cetinkaya et al. (2022; effect size: 0.666, α = 0.05, power: 0.95, oxytocin induction group: 60, non-induction group: 60). Considering possible data loss of 50%, groups of 90 participants were planned for each group. However, the study was completed with 85 participants in the oxytocin induction group and 79 participants in the non-induction group (a total of 164 participants and their newborns. The inclusion criteria were: Women with sufficient mental health to answer the questions, who naturally conceived, in the 38–42nd week of pregnancy, delivered a live, healthy, and single fetus vaginally, and whose newborn birth weight was greater than 2500 g
Women who had risk in the early postpartum period (e.g., postpartum hemorrhage) were excluded. Newborns who required oxygen, showed any risk condition or need for resuscitation, or requiring intensive care were excluded (Figure 1). CONSORT flow diagram outlining the execution and data collection process of the study.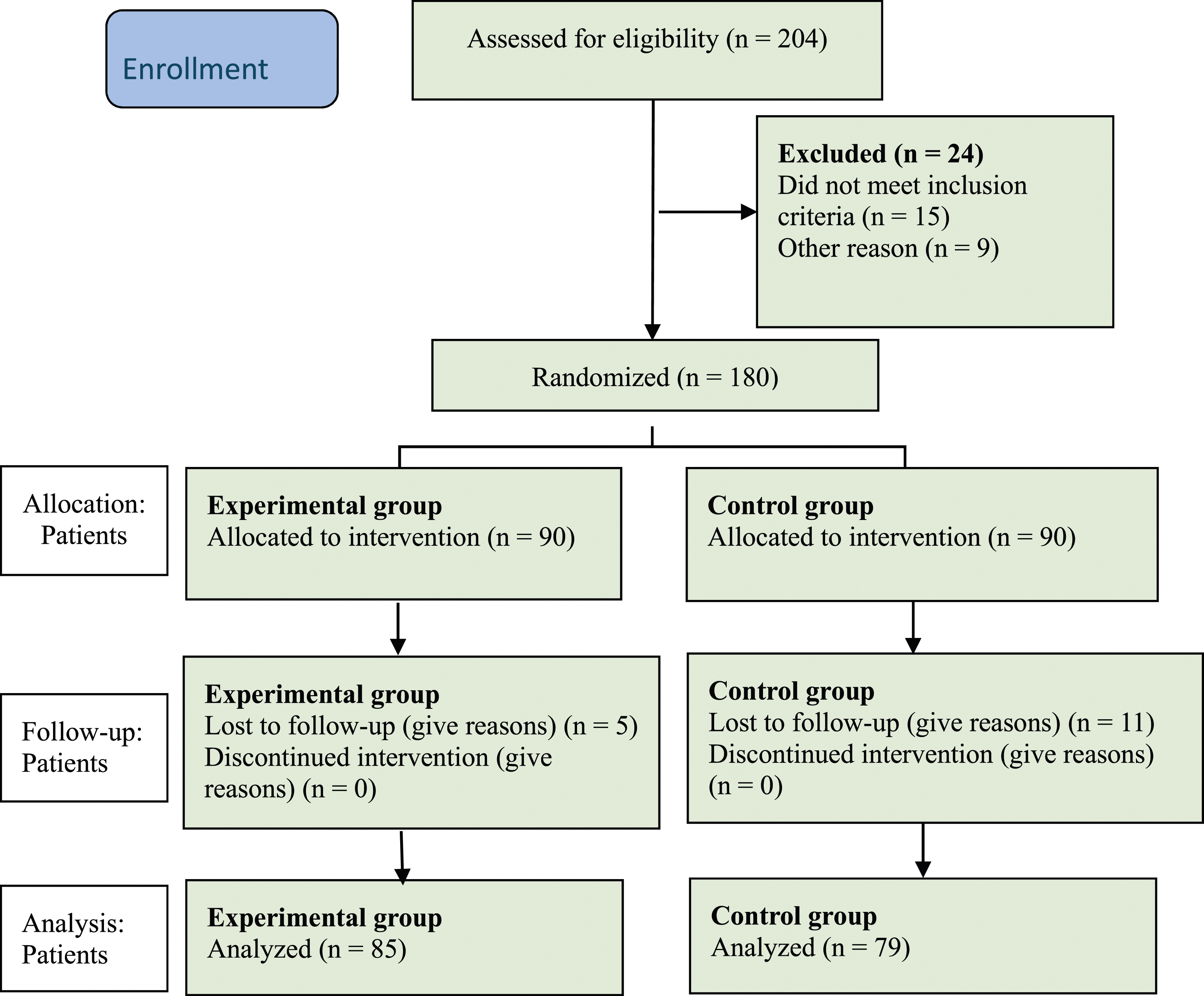
Data Collection Tools
Information form
This form consisted of 21 questions related to sociodemographic, obstetric, and neonatal characteristics to describe the demographic features of the participants (Barrett et al., 2015; Cetinkaya et al., 2022; Daly et al., 2020; Filippa et al., 2017, 2019, 2021; Souter et al., 2019).
Neonatal pain and stress assessment scale (ALPS-Neo)
Developed by Lundqvist et al. (2014) was used to assess pain and stress in premature and term neonates. This scale is a 3-point Likert-type instrument consisting of 5 items: facial expression, breathing pattern, limb tone, hand and foot activity, and activity level. Measurements were conducted through observation. The scores increased as the levels of pain and stress increased. A score between 3 and 5 indicates mild pain and stress, whereas a score above 5 indicates severe pain and stress. The scale was developed by Lundqvist et al., who reported a Cronbach’s alpha coefficient of 0.95 (Lundqvist et al., 2014). The validity and reliability of the scale was examined by Ceylan and Bolışık, who found a Cronbach’s alpha coefficient of 0.81 (Ceylan & Bolışık, 2017). In this study, we determined the Cronbach’s alpha coefficient to be 0.86.
Study procedure
In the study, participants were divided into two groups based on the physician’s recommendation: those who received synthetic oxytocin induction and those who did not. Data were collected through self-reporting and observation. Neonatal pain stimuli were assessed under three headings: drying, first injection, and blood glucose measurement. Data were verified and collected before, during, and after these procedures by one researcher and two independent blind observers. The two independent blinded observers were not informed about whether the participant had received synthetic oxytocin.
Ethical Dimensions of the Study
Consent was obtained from the institution where the research was conducted and participants. Approval was obtained from the Clinical Research Ethics Committee of Kocaeli University (approval number: GOKAEK-2022/10.23). The study was registered at ClinicalTrials.gov (registration number: NCT06474000). Permission to use the measurement device (ALPS-Neo) was obtained from the author via email. Additional informed consent was obtained from all participants who provided identifying information in this article. The tenets of the Declaration of Helsinki were adhered to throughout the study.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics 29.0 (IBM Corp, Armonk, NY, USA). Descriptive statistical methods (frequency, percentage, mean, standard deviation) were used to evaluate the sociodemographic data. Chi-square and t-tests were used for comparative analysis of the data. A p-value of p < .05 was considered statistically significant.
Results
Comparison of Demographic Characteristics Between Oxytocin Induction and Control Groups (n = 164).
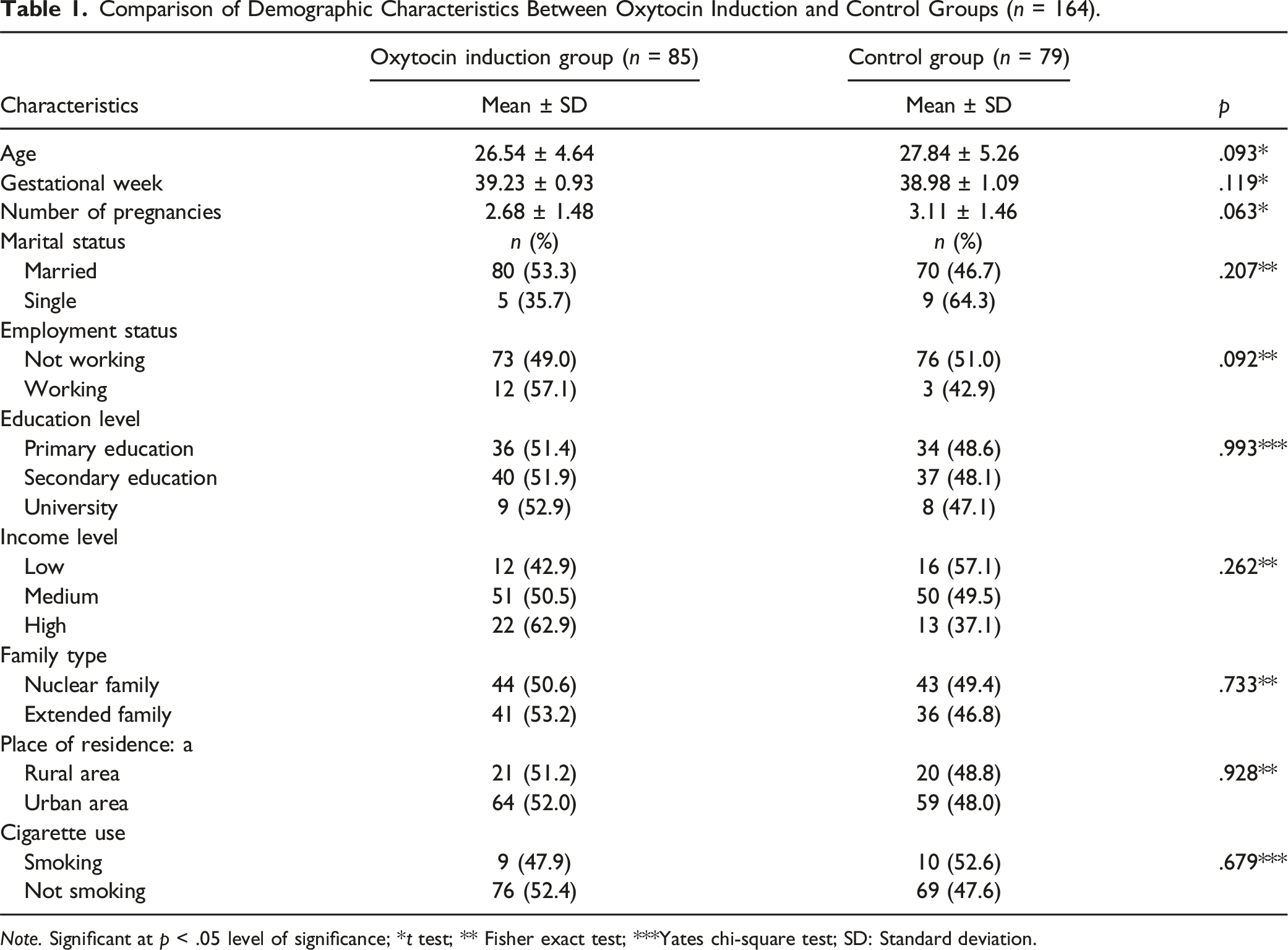
Note. Significant at p < .05 level of significance; *t test; ** Fisher exact test; ***Yates chi-square test; SD: Standard deviation.
Comparison of Newborn Characteristics Between Synthetic Oxytocin Induction and Control Groups (n = 164).
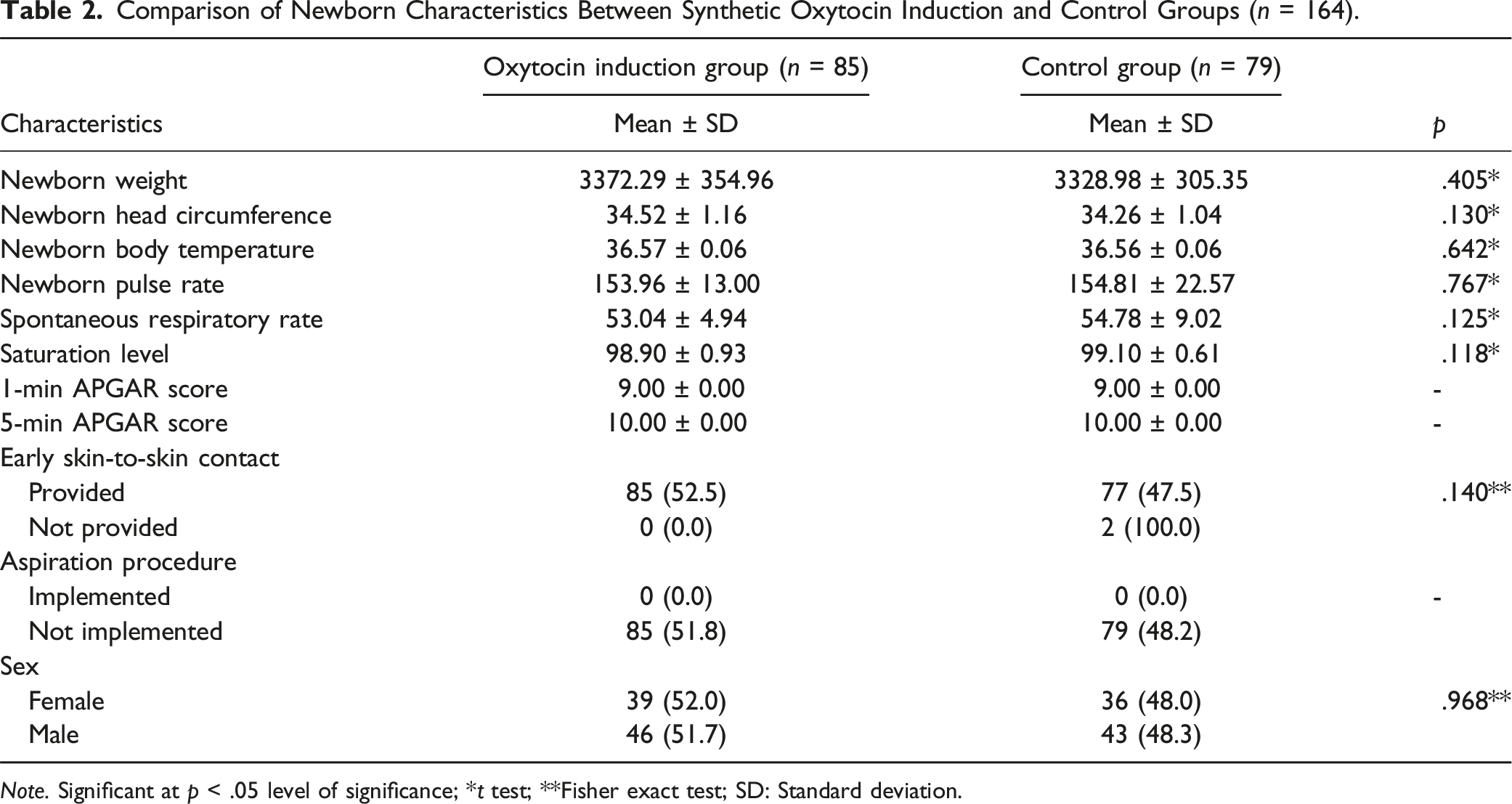
Note. Significant at p < .05 level of significance; *t test; **Fisher exact test; SD: Standard deviation.
Comparison of ALPS-NEO (Pain-Stress) Mean Scores for Newborns in the Oxytocin Induction and Control Groups During Drying, Injection, and Blood Glucose Measurement (n = 164).
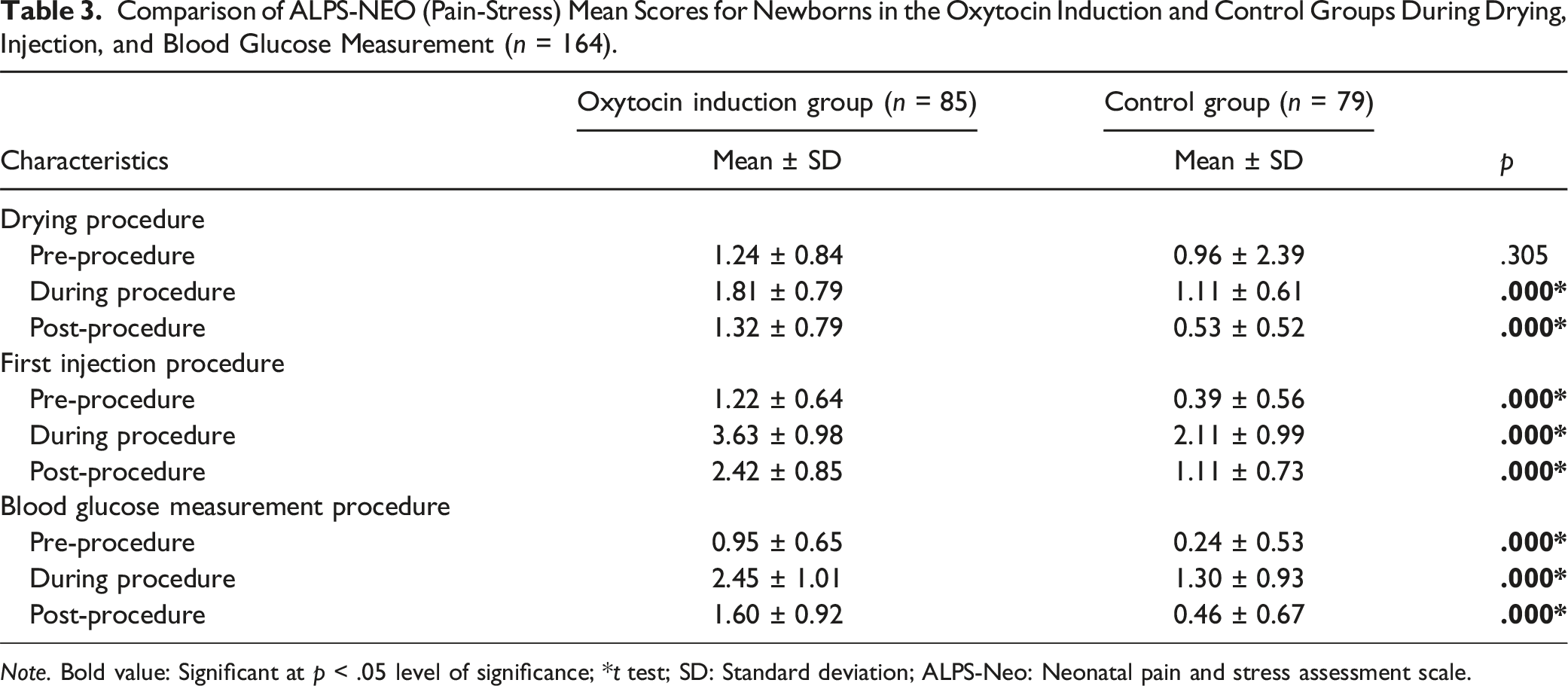
Note. Bold value: Significant at p < .05 level of significance; *t test; SD: Standard deviation; ALPS-Neo: Neonatal pain and stress assessment scale.
Discussion
To date, no comprehensive study has examined the relationship between intrapartum synthetic oxytocin and the separation of newborns from mothers and exposure to painful interventions. This study compared early neonatal pain-stress levels between newborns whose mothers received oxytocin induction and those whose mothers did not. In this study, only the pain-stress mean scores of the newborns before drying were similar. Newborns of participants who received synthetic oxytocin induction had higher pain-stress scores during and after the drying procedure, before, during, and after the first injection procedure, and before, during, and after the blood glucose measurement than those in the control group.
The review of the literature revealed that there are limited studies on the fetal effects of synthetic oxytocin administration during the intrapartum period. A meta-analysis examining the effects of synthetic oxytocin on newborns reported that maternal intrapartum synthetic oxytocin did not increase fetal oxytocin levels at birth. According to the researchers, synthetic oxytocin administered at clinical doses does not transfer from the mother to the fetus (Buckley et al., 2023). According to the literature, synthetic oxytocin must pass through both the placenta and the fetal blood-brain barrier (Uvnäs-Moberg, 2024). However, it should be noted that the fetal blood-brain barrier is not sufficiently mature and permeable, and that the fetal neurohypophysis, where oxytocin is secreted, largely lacks a blood-brain barrier (Monks & Palanisamy, 2021). Although evidence regarding whether peripherally administered oxytocin crosses the mature blood-brain barrier is conflicting, animal studies have shown that oxytocin can cross the immature blood-brain barrier in the developing fetal brain (Kenkel et al., 2019; Meziane et al., 2015). Therefore, synthetic oxytocin administered during birth may affect the fetal neurodevelopmental process. Although there are gaps in dose-response data, the association between synthetic oxytocin during birth and autism spectrum disorders has gained importance in recent years (Oberg et al., 2016; Soltys et al., 2020; Stokholm et al., 2021). There is limited evidence regarding the neurodevelopmental effects of synthetic oxytocin passing from the mother during birth (Kenkel et al., 2014; Omaru et al., 2024). Therefore, conducting studies on this topic is challenging when considering the dose of the oxytocin used.
In this study, we observed that the pain-stress scores of the oxytocin induction group were similar to those of the non-induction group in the initial measurements (pre-drying). However, when considering responses to subsequent painful stimuli, the pain-stress scores of the oxytocin induction group were found to be higher than those of the control group. Oxytocin receptors are found in the decidua and other tissues of the uterus. These receptors increase prostaglandin production during labor. Local prostaglandins cause myometrial contractions and indirectly lead to cervical changes. Additionally, the increased pressure on the baby’s head on the cervix due to uterine contractions further exacerbates this effect (Uvnäs-Moberg et al., 2019). Decreased blood flow and oxygenation to the fetus due to contractions can lead to the accumulation of lactic acid in the fetus (Felis, 2023). This can cause the fetus to experience less pain in the initial stages of the early neonatal period and more pain in later stages. This situation is more balanced with endogenous oxytocin because maternal compensation maintains this balance. However, as labor progresses, especially in births in which synthetic oxytocin is used, contractions become stronger and more frequent. There are relatively shorter relaxation periods between contractions, which further shortens the duration of uterine tissue recovery. This not only increases maternal pain and stress but can also reduce fetal blood flow (Daly et al., 2020; Khajehei, 2017; Uvnäs-Moberg et al., 2019). Thus, synthetic oxytocin administration can increase maternal metabolic and autonomic outcomes caused by physiological labor contractions and reduce fetal blood flow. As a result, it may have chronic negative effects on pain and stress perception in the fetus due to the accumulation of lactic acid (Buckley et al., 2023). Gabriel et al. (2015) reported that intrapartum oxytocin administration may inhibit the expression of several primitive neonatal reflexes associated with breastfeeding. Additionally, Bell et al. (2013) videotaped and examined the first hour of mother-infant interactions and found that infants exposed to higher levels of exogenous oxytocin had lower sucking success and poorer bonding. The researchers suggested that this might be due to chronic pain in the early neonatal period (Bell et al., 2013).
Finally, in contrast to the studies mentioned above, there are also animal studies showing that oxytocin plays a role in bonding and has analgesic properties (Filippa et al., 2019). In studies involving human neonates, the analgesic effect of exogenous oxytocin during painful procedures has been advocated. However, these studies have been conducted with neonates in the intensive care unit during the late neonatal period (Barrett et al., 2015; Filippa et al., 2019; Grobman et al., 2018; Monks & Palanisamy, 2021).
Limitations
This study has several strengths. One of the reasons for this is that it was one of the first studies on this topic. Another strength was the focus on the neonate’s response to painful procedures during the early neonatal period. However, there were also some limitations in the study. One of these concerns was the unequal amount of synthetic oxytocin administered and its inability to be measured. Additionally, data collected were limited to pre-drying, initial injection, and blood glucose measurements during the early neonatal period. Additionally, the study included two independent and blinded observers; however, the fact that the third person, the researcher, was not blinded could have introduced bias.
Implications for Policy and Practice
Synthetic oxytocin remains one of the most commonly used methods for labor induction worldwide. However, it is still classified as a “high-risk medication.” Research in this area is primarily limited to physician-led studies due to the necessity of physician orders. Therefore, studies that include midwives should be conducted. Oxytocin is widely used to initiate and support labor; therefore, it plays a critical role in labor management. Midwives are directly involved in the administration and monitoring of oxytocin during labor, which allows them to observe its effects on both mothers and newborns. Moreover, their experience in managing labor complications and interventions can contribute to improving clinical practices and patient outcomes. Lastly, longitudinal, comprehensive studies that can quantitatively measure oxytocin levels and explore this topic in greater depth are needed.
Conclusions
This study focused on the pain-stress responses of neonates to early neonatal stimuli in participants who received synthetic oxytocin during labor compared with those who did not. The average pain-stress scores were higher in the oxytocin induction group during and after the drying process, before, during, and after the initial injection, and before, during, and after the blood sugar measurement. The current findings provide justification for the need for more comprehensive studies on the effects of synthetic oxytocin on newborns at birth.
Footnotes
Acknowledgments
We sincerely thank all the women and their newborns who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Consent was obtained from the institution where the research was conducted and participants. Approval was obtained from the Clinical Research Ethics Committee of Kocaeli University (approval number: GOKAEK-2022/10.23). The study was registered at ClinicalTrials.gov (registration number: NCT06474000). Permission to use the measurement device (ALPS-Neo) was obtained from the author via email. Additional informed consent was obtained from all participants who provided identifying information in this article. The tenets of the Declaration of Helsinki were adhered to throughout the study.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author upon request.