
Abstract
Objectives
This study investigated the inter-rater reliability, agreement and responsiveness of the Feline Grimace Scale (FGS) in brachycephalic cats.
Methods
A total of 28 brachycephalic cats (mean age 6.6 ± 4.4 years, mean weight 4.2 ± 1.0 kg) undergoing ocular surgery were included in a prospective, randomised, blinded study. Cats presenting fear-anxiety behaviours were not enrolled. In total, 95 images of these cats were collected from video recordings pre- and postoperatively (before/after analgesia), scored by four raters using the FGS and compared with real-time scores. Limits of agreement (LoAs) and bias were evaluated using the Bland–Altman method (good or poor agreement if bias <0.1 or >0.1, respectively). Inter-rater reliability was assessed using the intraclass correlation coefficient (ICC; <0.50 = poor, 0.50–0.75 = moderate, 0.76–0.90 = good and >0.90 = excellent reliability). Generalised linear mixed models evaluated responsiveness (P <0.05).
Results
Inter-rater reliability (ICCsingle) was poor for muzzle tension (0.47, 95% confidence interval [CI] 0.36–0.58) and whiskers change (0.34, 95% CI 0.22–0.46), good for ear (0.81, 95% CI 0.74–0.86) and eye position (0.84, 95% CI 0.79–0.88), moderate for head position (0.71, 95% CI 0.59–0.79) and good for FGS total ratio scores (0.76, 95% CI 0.68–0.82). LoAs were in the range of –0.37 to 0.22 with a bias of –0.08, suggesting that some cats could have their scores affected in comparison with real-time scores. Mean FGS total scores decreased after analgesia pre- (0.56 ± 0.10 vs 0.38 ± 0.15; P = 0.005) and postoperatively (0.60 ± 0.18 vs 0.36 ± 0.15; P <0.001).
Conclusions and relevance
The FGS is a responsive pain-scoring instrument in brachycephalic cats with ocular pain, with good agreement and excellent inter-rater reliability for total ratio scores. Pain may be overestimated using image assessment in some brachycephalic cats.
Plain language summary
This study examined how consistent, accurate and sensitive the Feline Grimace Scale (FGS) is for evaluating pain in brachycephalic (flat-faced) cats undergoing ophthalmological (ie, eye) surgery. The FGS is a facial expression-based tool that helps veterinarians recognise pain in cats by observing subtle changes in the position of the eyes, ears, whiskers, muzzle and head. A total of 28 brachycephalic cats were included in a blinded, randomised study. Researchers collected 95 images from video recordings taken before and after surgery, both before and after pain relief. Four trained observers independently scored the images using the FGS, and these image-based scores were compared with real-time assessments performed during the procedure. The results showed that the FGS is highly reliable and responsive in detecting changes in pain levels in brachycephalic cats. Agreement among raters was excellent for the total FGS score, indicating that different observers tended to assign similar overall pain ratings. Some individual facial features, such as muzzle tension and whisker position, were less consistent between observers, while eye and ear position were rated more reliably. The FGS total scores decreased significantly after administration of analgesia, confirming that the scale is sensitive to pain relief. A difference was observed between image-based and real-time scores, suggesting that pain may be slightly overestimated in some brachycephalic cats when using images. This may be due to differences in anatomical facial features that affect facial expressions of pain. Overall, these findings support the FGS as a reliable and sensitive tool for assessing ocular pain in brachycephalic cats, while emphasising the need for careful interpretation when using image-based assessments.
Introduction
In recent years, the global popularity of brachycephalic breeds has risen significantly, with selective breeding further accentuating their anatomical abnormalities.1,2 The round-shaped brachycephalic skull is attributed to a reduction in the length of the face,1,2 a disproportionate increase in the height and width of the braincase, and an increase in the convexity of the calvaria.1,2 Clinical disorders predisposed by these traits are associated with hereditary and ocular diseases, obstructive airway conditions, and dermatological and gastrointestinal problems, among others.1 –4
Ocular-related disorders, such as entropion, chronic epiphora, conjunctivitis and corneal sequestrum, are frequently observed in brachycephalic cats.5,6 These issues could be inherently due to lagophthalmos and compromised tear film quality.5,7 Brachycephalic cats exhibit lower corneal nerve fibre density compared with mesocephalic breeds, resulting in significantly reduced corneal sensitivity.8,9
Successful pain management relies on accurate pain recognition. 10 Pain assessment in cats has evolved with the publication of specific guidelines,10,11 validated multidimensional composite pain scales12 –15 and the Feline Grimace Scale (FGS). 16 However, studies on the measurement properties of feline pain-scoring instruments have mostly been performed in adult domestic shorthair cats and not involved brachycephalic cats. The FGS consists of scoring five action units (AUs), namely ear position, orbital tightening, muzzle tension, whiskers change and head position. 16 Considering the extreme anatomical landmark changes observed in brachycephalic cats when compared with mesocephalic and dolichocephalic cats, it is not known if the FGS can be used reliably in these cats or if disagreements would be observed between real-time and image scoring. It is possible that some AUs are already ‘present’ (ie, scores of 1 or 2) in the healthy, pain-free brachycephalic cat because of the aforementioned anatomical changes, which could present a source of bias during FGS scoring. In this case, it could be possible that FGS scores would not be reduced after the administration of analgesia (ie, responsiveness); agreement between real-time and image FGS scoring would be poor. In addition, the presence of ocular pain and/or other types of pain as a result of brachycephalic anatomical abnormalities in cats that present for other types of surgery could result in higher FGS scores that are not attributable to the surgical pain. Scores may be even more affected in brachycephalic cats with ocular pain, as clinicians often apply adjustable Elizabethan collars (e-collars) before and after surgery to avoid self-trauma, which makes evaluation of certain AUs more difficult or even impossible.
The objective of this study was to investigate the inter-rater reliability, agreement and responsiveness (as part of construct validity) of the FGS in brachycephalic cats. The study did not have a set hypothesis considering its exploratory nature and the lack of a control group involving mesocephalic and dolichocephalic cats for comparison.
Materials and methods
Ethical approval
The study involving live cats was approved by the Animal Care Committee of the Université de Montréal (23-Rech-2250) and City University of Hong Kong (Project No. #9380145/AN-STA-00000522). Written consent from each cat caregiver was obtained before enrolment. The study involving human subjects received approval from the Ethics Review of Human Research (Protocol HU- STA-00001083) and was conducted according to the Tri-Council Policy Statement ‘Ethical Conduct for Research Involving Humans’. Data collection involving cats was conducted at the Centre Hospitalier Universitaire Vétérinaire, Faculté de médecine vétérinaire, Université de Montréal between October 2022 and January 2023, and at the Veterinary Specialty Hospital in Hong Kong between March and May 2024. This study followed the guidelines of the Canadian Council on Animal Care and is reported according to the ARRIVE guidelines. 17
Animals
Inclusion criteria were cats aged 1 year or older, with ocular manifestations involving pathologies that could induce acute pain (eg, ulcerative keratitis, corneal sequestration, glaucoma, eosinophilic keratitis). Exclusion criteria included patients with excessive fear-anxiety-related behaviours that may affect pain assessment or patients that had received anti-inflammatory/analgesic agents up to 12 h before admission. Cats requiring immediate care (respiratory distress, severe hypovolaemia, shock) were not enrolled. Cats were admitted approximately 4 h preoperatively. Food was withheld for up to 8 h before general anaesthesia.
Pain assessment and video recording
Physical and ophthalmic examinations were performed by a specialist at the American College of Veterinary Ophthalmology and the Asian College of Veterinary Ophthalmologists (DC, Hong Kong) or by a specialist at the European College of Veterinary Ophthalmologists (MV, Montreal). Cats were then housed individually for approximately 3 h in cages equipped with a water bowl, cardboard box, litter box and blankets. A high-definition wide-angle camera set at 60 frames/s (GoPro; Hero9) was attached to the cage bars at the level of the cats’ eyes and adjusted if needed during video recording. After a 10-min acclimation period to the attached camera, cats were undisturbed and filmed for 10 mins. Pain scoring was performed after video recording using the UNESP-Botucatu Feline Pain Scale-Short Form (UFEPS-SF) 15 and the FGS. Video recordings and pain assessment were conducted at the following time points: (1) before surgery and the administration of premedication/analgesia (baseline); (2) 40–60 mins after premedication/analgesia; (3) 2 h after the end of surgery; and (4) approximately 30 mins after the administration of postoperative analgesia. Video recordings and pain scoring were performed by one trained female observer (SM) with over 10 years of experience in feline medicine and surgery.
Analgesia, anaesthesia and surgery
After baseline assessment, cats (n = 28) received an intramuscular (IM) injection of methadone (0.3 mg/kg, Methone; Ceva) approximately 1 h before the procedure (ie, premedication/analgesia). A 22 G intravenous catheter was placed in one of the cephalic veins and general anaesthesia was induced with midazolam (0.15 mg/kg, Midazolam; Hameln Pharma) and a dose of propofol (6 mg/kg, ProproFlo; Zoetis) titrated to effect to allow endotracheal intubation. The arytenoids were desensitised using 2 mg of lidocaine 2% and cats were intubated with a cuffed endotracheal tube. Anaesthetic maintenance was performed with isoflurane in oxygen using a non-rebreathing system. Electrocardiography, non-invasive blood pressure, capnography, pulse oximetry and rectal temperature were monitored using a multiparametric monitor. Intravenous fluid therapy was administered using an isotonic crystalloid solution at 5 ml/kg/h throughout surgery. Adjustable e-collars (ie, soft/flexible or hard plastic according to the patient’s needs) were placed immediately after surgery or, when deemed necessary, at the time of premedication to avoid self-inflicted injuries. E-collars were then removed during preoperative, but not postoperative, pain assessment and video recording. Analgesia was administered 2 h after the end of surgery or earlier if UFEPS-SF scores were 4/12 or higher. Methadone (0.2 mg/kg IV) was administered to 23 cats, whereas two cats received buprenorphine (0.02 mg/kg IV). Meloxicam (0.1 mg/kg, Metacam; Boehringer Ingelheim) was administered by the subcutaneous route of administration at the end of the surgery, unless contraindicated (n = 1). Three cats that did not require surgery but received medical treatment were also included. Pain assessment and video recordings were performed at baseline and 40 mins to 1 h after the administration of methadone (0.3 mg/kg IM) for these three individuals. Each cat received individualised treatment with antibiotics and/or ophthalmic tear drops and/or ophthalmic autologous serum as per the clinician’s discretion.
Image capture, selection and cropping
Images were captured from video frames using a conversion software (Free Video to JPG Converter; DVDVideoSoft) at two frames/s. From each video recording (ie, time point), three images were selected, one from each third of the recording. The optimal image was chosen based on adequate resolution, lighting, frontal facial orientation with visible AUs and overall representativeness of the video content for that time point. Image selection was performed by a single observer (SM) who was blinded to the UFEPS-SF and FGS pain scores at the time of image selection. Images were cropped to include the entire face of the cat using Photo Editor (Windows 11; Microsoft) between July and August 2024.
Image scoring
Four veterinarians (KSD, MG, TB and PVS) were invited to score images. They included a feline specialist board-certified by the American Board of Veterinary Practitioners, two residency-trained individuals with extensive experience in clinical veterinary anaesthesiology and feline pain research, and a diplomate of the American College of Veterinary Anesthesia and Analgesia who was part of the development and validation of the FGS. The observers participated in a training session led by the principal investigator (PVS) before image scoring, using the FGS training manual. 16 Raters scored images from ‘Practice your skills’ in the FGS app (available from www.felinegrimacescale.com) followed by a discussion of their scores. In the study population, facial features and the use of adjustable e-collars were identified as potential sources of variability in facial landmark identification and pain scoring, notably muzzle conformation, whisker misalignment and head position due to the presence of the e-collar.
An online survey (QuestionPro) was then created for image scoring after randomisation using a sequence generator (www.random.org). Raters were not aware of treatment or time points. According to the FGS, ear position, orbital tightening, muzzle tension, whiskers change and head position were scored for each image and by each rater as follows: 0 = not present/absent; 1 = moderate presence/uncertainty about presence; or 2 = obviously present. If the AU was not visible, raters could opt to choose ‘not possible to score’. Considering the ocular pathologies, observers were instructed to assess the contralateral (ie, unaffected) eye when scoring orbital tightening. The FGS total ratio score was calculated by summing the scores from each AU and dividing by the maximum possible score, excluding the AUs marked as ‘not possible to score’. Image scoring was carried out in September 2024 over two sessions, separated by a 1-week interval to reduce observer fatigue. Images were excluded when at least two AUs could not be scored by a single observer.
Statistical analysis
Statistical analyses were performed using RStudio version 2022.07.1-554 (https://www.rstudio.com). The intraclass correlation coefficient (ICC) was used to assess the inter-rater reliability of each AU and total FGS ratio scores. The two-way mixed effects model was used to compute ICCs with the absolute agreement for a single (ICCsingle) and average (ICCaverage) rater separately. The following interpretation of inter-rater reliability was used: ICC <0.50 = poor reliability; 0.50–0.75 = moderate reliability; 0.76–0.90 = good reliability; and >0.90 = excellent reliability. 18 The number and percentage of cats receiving rescue analgesia on the basis of FGS total ratio scores assigned by the four raters (ie, image-based assessment) were calculated and compared using Pearson’s χ2 test. Agreement between scores by raters and the veterinarian who performed pain assessment in real time (ie, gold standard) was assessed using the Bland–Altman method. A bias less than 0.1 was acceptable, indicating very good agreement. A bias greater than 0.1 (>1 unit in the FGS score) was considered unacceptable, indicating poor agreement. According to this method, a bias with a negative value may suggest an overestimation of the FGS scores by raters compared with the gold standard, whereas a positive bias can suggest an underestimation of the FGS scores.18,19 The limits of agreement (LoAs) were interpreted in relation to the analgesic threshold of the FGS (0.39). 16 Two repeated measure generalised linear mixed effect models were used to compare FGS total ratio scores assigned by raters before and after the administration of analgesia in the preoperative (ie, premedication) and postoperative (ie, rescue analgesia; time point 4) periods, separately. The FGS total ratio score was the response variable, administration of analgesia was an independent variable and individual subjects were taken as random effects. Three repeated measure linear mixed effect models were developed with respect to FGS total ratio scores (gold-standard observer/image-based and real-time assessment) and UFEPS-SF scores (real-time assessment) to evaluate the effect of the e-collar on pain assessment, before and after rescue analgesia, postoperatively. The presence or absence of the adjustable e-collar was added as a co-factor.
Results
A total of 28 brachycephalic cats (13 spayed females and 15 neutered males; mean age 6.6 ± 4.4 years, mean weight 4.2 ± 1.0 kg) undergoing ocular surgery were included in a prospective, randomised, blinded study. Breeds included Exotic Shorthair (n = 13), Persian (n = 5), British Shorthair (n = 5), British Longhair (n = 3), Scottish Fold (n = 1) and Devon Rex (n = 1). Ocular surgery included lamellar keratectomy (with or without grafting for corneal ulcers or corneal sequestrum) (n = 17) and enucleation (n = 8). Non-surgical cases included ulcerative keratitis (n = 3).
A total of 95 images were collected. Eight images were excluded from the statistical analyses (ie, two AUs or more were not possible to score). Inter-rater reliability (ICCsingle) was poor for muzzle tension (0.47, 95% confidence interval [CI] 0.36–0.58) and whiskers change (0.34, 95% CI 0.22–0.46), good for ear position (0.81, 95% CI 0.74–0.86) and orbital tightening (0.84, 95% CI 0.79–0.88), moderate for head position (0.71, 95% CI 0.59–0.79) and good for FGS total ratio scores (0.76, 95% CI 0.68–0.82) (Table 1).
Inter-rater reliability of the Feline Grimace Scale in brachycephalic cats

Data are single and average intraclass correlation coefficient (ICCsingle and ICCaverage, respectively) and 95% confidence intervals (CIs). The ICCsingle and ICCaverage were interpreted as follows: <0.5 = poor reliability; 0.5–0.75 = moderate reliability; 0.76–0.9 = good reliability; and >0.9 = excellent reliability
On the basis of FGS total ratio scores assigned by raters 1, 2, 3 and 4, 66 (77.64%), 65 (76.47%), 64 (75.29%) and 60 (70.59%) of the images would have surpassed the threshold for rescue analgesia (Figure 1), respectively. The number of images that would have surpassed the threshold for rescue analgesia did not differ between observers (P = 0.73).

The number of cats that would have received (YES) or not received (NO) rescue analgesia according to Feline Grimace Scale total ratio scores assigned by observers 1, 2, 3 and 4
The bias of –0.08 suggested acceptable, very good agreement. However, LoAs were in the range of –0.37 to 0.22, suggesting that some cats could have their scores affected in comparison with real-time scores; some data points were outside the upper LoAs (Figure 2).

Bland–Altman plots showing agreement of Feline Grimace Scale scores between raters (RAs) and the gold standard (GS). Bias (central yellow continuous line) and the limits of agreement (orange dotted lines) are indicated on the plot. The x-axis displays the mean values between the GS and the RAs, while the y-axis represents the differences between the GS and the RAs
The mean FGS total ratio scores decreased after analgesia pre- (0.56 ± 0.10 vs 0.38 ± 0.15; P = 0.005) and postoperatively (0.60 ± 0.18 vs 0.36 ± 0.15; P <0.001) (Figures 3–5, Table 2).
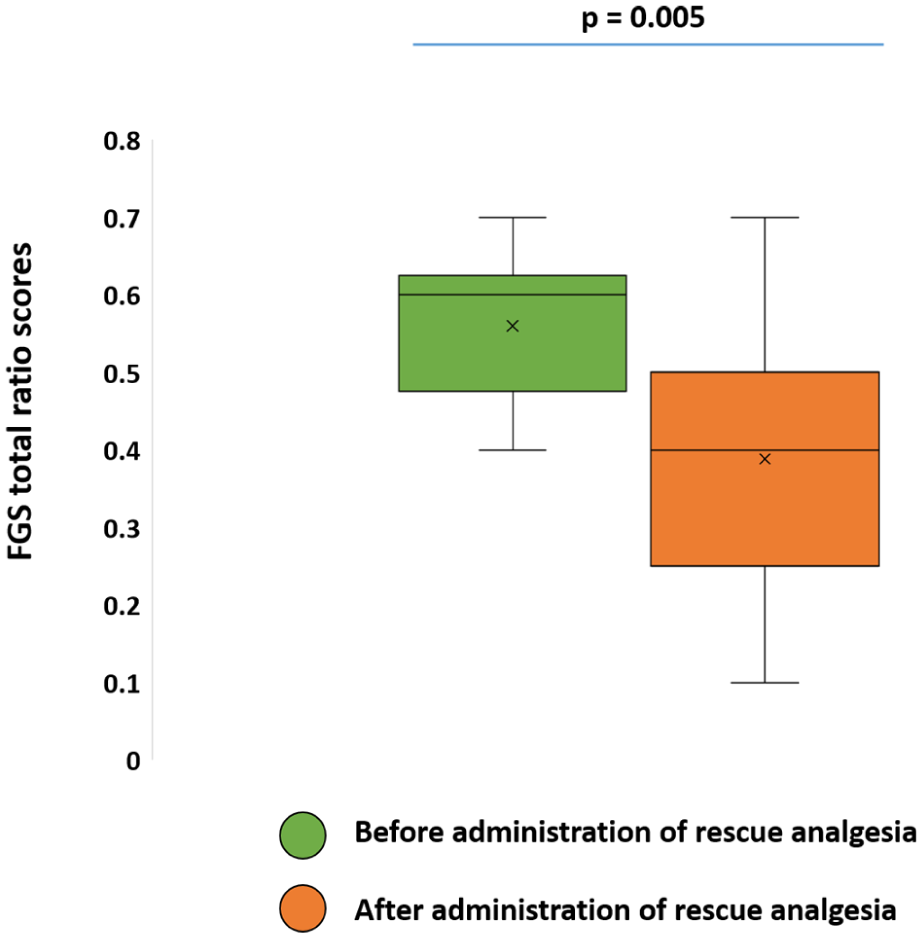
Box and whisker plots showing minimum, maximum, median and interquartile range values for Feline Grimace Scale (FGS) total ratio scores before and after administration of analgesia in the preoperative period
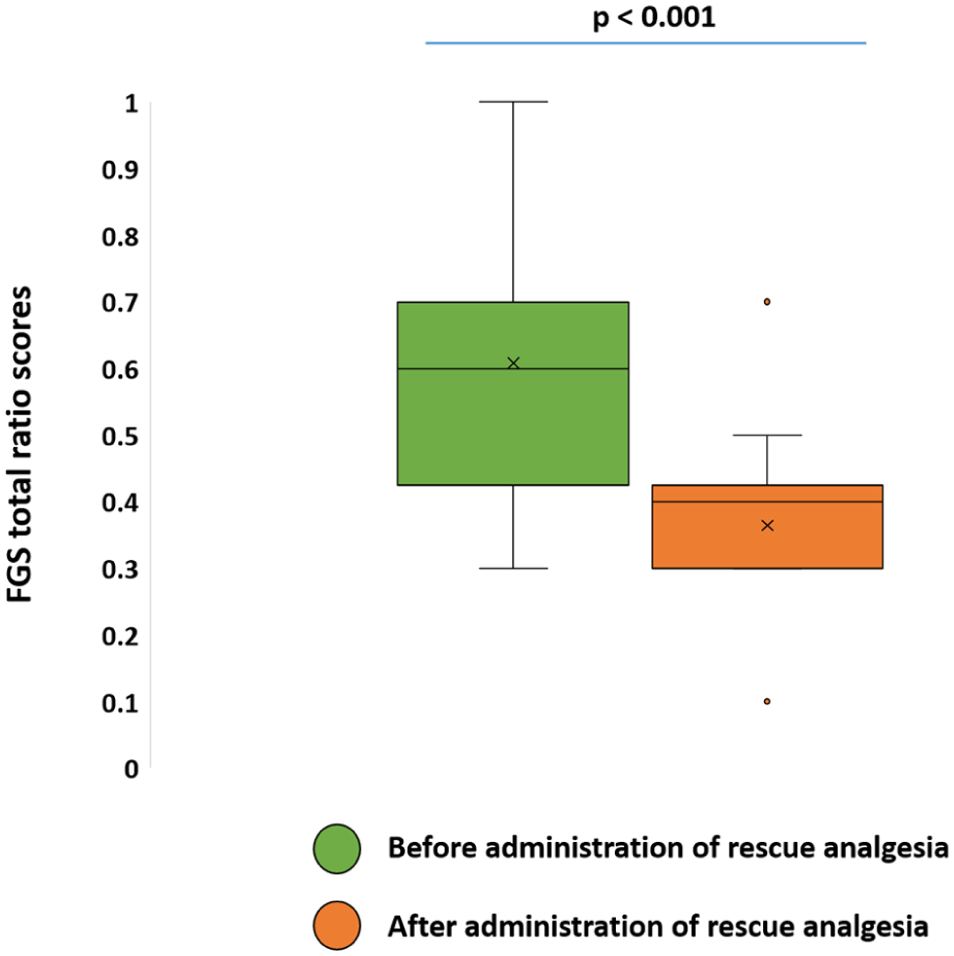
Box and whisker plots showing minimum, maximum, median and interquartile range values for Feline Grimace Scale (FGS) total ratio scores before and after administration of analgesia in the postoperative period

Representative images of the same brachycephalic cat with ocular pain at four time points for image-based pain scoring: (a) preoperative baseline (before analgesia); (b) preoperative (after analgesia); (c) 2 h postoperatively (before analgesia); (d) postoperative, after analgesia
Results of the repeated measure linear mixed effect models with respect to Feline Grimace Scale total ratio scores before and after administration of analgesia in the perioperative and postoperative period*

The category ‘after analgesia’ was a reference category in the model
SE = standard error
Mean FGS total ratio (0.56 ± 0.21 vs 0.46 ± 0.22; P = 0.05) and UFEPS-SF (4.91 ± 1.3 vs 3.26 ± 2.25; P = 0.001) real-time scores were significantly higher in cats without an e-collar than in cats with an e-collar, respectively. However, image-based FGS scores had a similar trend but were not significantly affected by the presence or absence of an e-collar (P = 0.06) (Table 3).
Results of the repeated measure linear mixed model with respect to Feline Grimace Scale total ratio scores using image scoring before and after administration of analgesia in the postoperative period*

The presence or absence of an Elizabethan collar (e-collar) was added as co-factor. The categories ‘after analgesia’ and ‘e-collar absent’ were reference categories in the model
SE = standard error
Discussion
In the current study, the investigation of the applicability of the FGS in brachycephalic cats with ocular pain is reported by evaluating its agreement, reliability and responsiveness using image-based pain scoring. Overall, the results demonstrate that inter-rater reliability was good using ICCsingle and excellent using ICCaverage for FGS total ratio scores. A similar percentage of images with scores surpassing the threshold for the administration of analgesia was observed among the four experienced raters. Similarly to what has been reported in shorthaired adult cats and kittens,18,20 the FGS total ratio scores decreased after analgesia in the pre- and postoperative period, demonstrating responsiveness as part of construct validity. Agreement between real-time and image scoring was acceptable using Bland–Altman analysis. Brachycephalic craniofacial conformation in purebred cats (eg, Persian, Exotic Shorthair, British Shorthair) has been linked to a range of disorders (ie, ophthalmic, facial, dental, respiratory and neurological), many of which may induce acute pain and/or maladaptive pain19,21,22 that are often underdiagnosed. Therefore, these findings are significant for feline welfare, as the FGS is now an acute pain assessment instrument with reported applicability and validity in brachycephalic cats, a population underrepresented in clinical research due to its intrinsic limitations related to anatomical variability. However, there were some differences in the results in comparison with previous literature that require attention, as discussed below.
Reliability refers to the consistency of measurements, whether across different observers (inter-rater reliability) or repeated assessments by the same observer (intra-rater reliability). The ICCsingle measures the reliability of one rater, while the ICCaverage measures reliability across raters. The ICCsingle is most relevant clinically, as FGS scoring is typically performed by a single rater. In this study population involving brachycephalic cats with ocular pain and with or without an e-collar, the FGS total ratio scores showed good inter-rater reliability (ICCsingle = 0.76). Previous studies reported good and moderate inter-rater reliability using the FGS total ratio scores in adult shorthaired cats and kittens (ICCsingle = 0.89 and ICCsingle = 0.68), respectively.18,20 In the present study, inter-rater reliability of whiskers change and muzzle tension was comparatively lower than other AUs and consistent with previous findings.16,18,20 This may be attributed to the anatomical variability among brachycephalic breeds,2,3,5,21 particularly in muzzle length and whisker orientation, which deviate from domestic shorthair cats. It may be challenging to define a round or elliptical shape of the muzzle in brachycephalic cats, given its awkward orientation, making it difficult to score it reliably. Head position demonstrated lower inter-rater reliability in comparison with other AUs, in contrast to earlier findings.18,20 Head position scoring was likely affected by the presence of an e-collar postoperatively, when cats were predominantly in sternal recumbency. The presence of the e-collar represents a limitation during image-based pain scoring, as it often involves visualisation of an imaginary line crossing the shoulder line, which may not be possible when cats are wearing an e-collar. Nevertheless, ear position and orbital tightening scoring present good and excellent reliability according to ICCsingle and ICCaverage, respectively, similar to previous studies.16,18,20 Some brachycephalic cats have short ears and may present several types of ocular pathologies that could have affected the scoring of these two AUs. However, inter-rater reliability was not affected and this hypothesis was not corroborated.
A Bland–Altman analysis was conducted to assess agreement and bias of FGS scores between real-time and image-based pain scoring. Bias was acceptable with indication of very good agreement between image and real-time scoring. The negative bias value of –0.08 suggests a slight overestimation of image-based scores by raters when compared with real-time assessment. These findings contrast with a previous study in adult domestic shorthair cats undergoing ovariohysterectomy, where real-time scores were slightly higher than image-based scores. 20 However, in both cases, over- or underestimation of scores was likely not clinically relevant and simply a reflection of the individual variability related to participants of the study and their experience. In addition, comparisons between real-time and image-based scores will always be subject to bias as the real-time observer is aware of time point (pre- or postoperatively), body posture/activity and the cat’s medical condition, whereas image-based scoring is conducted by raters who are unaware of these conditions. 20 Despite acceptable agreement, the LoAs should be interpreted in relation to the analgesic threshold of the FGS. LoAs were in the range of –0.37 to 0.22, suggesting that, overall, both upper and lower LoAs did not surpass 0.39 when considering the bias of –0.08. However, Figure 2 demonstrates that some data points are above the upper limits of agreement; for these individual cats, there could be a chance that pain scores would have been underestimated. In these cases, painful cats would not have received analgesia, with consequences for their health and welfare. Acute pain assessment is challenging in brachycephalic cats with ocular pathologies that may be wearing an e-collar. 10 Nevertheless, when images of the same individual are compared before and after analgesia (Figure 5), pain assessment may be easier, as changes in facial expressions are clearer than using isolated images. Becoming familiar with these brachycephalic patients before an elective surgery, for example, allows the observation of ‘normal’ facial expressions and their changes when pain is present.23,24
The FGS total ratio scores decreased after analgesia in both the pre- and postoperative periods. This confirmed the responsiveness of the FGS in brachycephalic cats with ocular pain after the administration of analgesia. Similar findings were observed in adult cats and kittens, as well as those undergoing multiple dental extractions.16,18,20,25 However, scores after the administration of analgesics were still close to the threshold suggested for interventional analgesia, which differs from previous studies. 16 Possible explanations include the influence of brachycephalic anatomical features, suboptimal analgesia or the inherently difficult nature of treating ocular pain, a challenge also reported in human medicine.26–28 In humans, ocular pain is a key clinical feature in ophthalmology and is commonly reported as photophobia, blepharospasm, tearing, itching, burning and a foreign body sensation. 29 In veterinary patients, photophobia, blepharospasm, ocular discharge/tearing and itching can often be observed.30 –32 A recent audit reported that 57% of hospitalised canine ophthalmology patients had no recorded pain assessment. 33 This likely stems from both the complex neural mechanisms underlying ocular pain and the unavailability of validated tools for this purpose. Ocular pathologies are highly prevalent in horses. Recently, an ocular pain scale was published 34 and refined, 35 and includes the assessment of facial expressions, blepharospasm, overall behaviour and lacrimation, among others. The scale identifies ocular pain with good inter-rater agreement and responsiveness after analgesic therapy. However, training on pain assessment is still required. 35 Correlations between intraocular pressure, orbital inflammation and postoperative ocular pain have been documented in humans, 36 and evidence from a preliminary study in dogs with glaucoma suggests increased mechanical sensitivity after enucleation. 37 In cats, ocular conditions such as corneal sequestration and keratitis differ substantially in their clinical presentation and severity.6,7,38 Therefore, it remains unclear how these different pathologies and demographics (eg, sex, breed) influence pain assessment and treatment, highlighting the need for further investigation of ocular pain in cats.
Adjustable e-collars are routinely used in veterinary practice to prevent self-trauma and protect surgical sites, despite documented welfare concerns. 39 In this study, the postoperative use of an e-collar did not significantly affect image-based pain scores. However, there was a trend for real-time FGS total ratio and UFEPS-SF scores to be lower in cats with an e-collar compared with cats without one. This trend should not be ignored, since previous research found increased behavioural distress (eg, attempt to remove the collar, head shaking) in cats wearing e-collars after ovariohysterectomy compared with those using wound-protection corsets. 40 It is possible that the use of an e-collar inhibits pain-induced behaviours and/or alters AU scoring. Individual variability, personality traits and prior exposure to e-collars, particularly in cats with recurrent ocular pathologies (ie, non-healing ulcerative keratitis), may increase tolerance to these objects. Our group is currently investigating the effects of e-collars during acute pain assessment using the FGS. It remains unclear how pain scores might differ within the same individual with and without the e-collar, and such a comparison was beyond the scope of this study because of ocular safety concerns; itching and attempts to scratch the eyes were observed during the study. When possible, the use of a comfortable, cat-friendly e-collar should be prioritised. 23
This study has limitations, including the challenges posed by the unique anatomical features of brachycephalic cats, particularly in the assessment of facial expressions. To the authors’ knowledge, this was the first study investigating pain assessment and ocular pain in this population. The findings highlight the need for improved awareness of ocular pain, a condition often underdiagnosed in feline practice. We are currently conducting an extensive evaluation of the duration and frequency of normal and pain-induced behaviours using validated ethograms and a specific software in cats with ocular pain. Beyond facial expressions, comprehensive pain assessment should include response to palpation (ie, light touch or pressure near the surgical site using gauze and standard best practices), as outlined in item 4 of the UFEPS-SF. Although frequently overlooked in ophthalmology, this measure proved valuable when cautiously applied during our data collection. It is also difficult to extrapolate how our findings would have been different in a population of adult domestic shorthair cats with or without ocular pain/an e-collar. Deep learning models have been described for the FGS, 41 and we are now investigating if landmark prediction and automated pain scoring using the FGS could be applied to brachycephalic cats after refinement. Ideally, e-collars should be removed during pain assessment so they do not bias evaluations in these cats. However, this should be done with caution as some cats can scratch or rub their eyes, with potential damage to the cornea and surrounding tissues, especially after surgery. In brachycephalic cats, the observation of facial expressions and pain behaviours before and after surgery or the administration of analgesics is fundamental; the authors recommend taking pictures of these patients for comparison. Changes in action units may be more obvious for an individual brachycephalic cat with this latter approach, as demonstrated in Figure 5.
Conclusions
The FGS demonstrated responsiveness to the administration of analgesics in brachycephalic cats before and after surgery. Good inter-rater reliability was observed for total FGS ratio scores in this population of cats. Acceptable agreement was demonstrated using the Bland–Altman analysis. However, image-based assessments may lead to slight pain overestimation in this population, likely due to anatomical features that limit accurate evaluation of facial expressions. These findings underscore both the clinical applicability and limitations of the FGS in brachycephalic cats, emphasising the importance of comprehensive real-time pain assessment and continuous monitoring for effective pain management.
Footnotes
Acknowledgements
The authors are grateful to the personnel, veterinary nurses and technicians at the Veterinary Specialty Hospital, City University of Hong Kong, and the Centre Hospitalier Universitaire Vétérinaire (Université de Montréal) for their valuable assistance during data collection.
Author note
The results of this investigation were presented at the 2025 World Feline Congress, Edinburgh, Scotland on 27–29 June 2025. This manuscript represents a portion of the first author’s PhD degree thesis to the Université de Montréal.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.