
Abstract
Oral and dental diseases are commonplace in cats, imposing a responsibility on primary care veterinarians to provide high quality oral healthcare for their feline patients. While patient assessment begins with an examination of the conscious cat, further assessment under anesthesia is necessary for the purposes of radiography and treatment, making anesthesia an essential component of feline dentistry. Because feline patients with oral and dental diseases, as well as those convalescing from surgery, generally experience pain, multimodal perioperative analgesia and anesthesia are standard features of oral and dental care. The ‘2025 FelineVMA feline oral health and dental care guidelines’ are coauthored by a Task Force of board-certified veterinary specialists and a veterinary technician specialist in dentistry convened by the Feline Veterinary Medical Association (FelineVMA). These experts have compiled evidence-guided recommendations for optimal oral health and dental care, including therapeutic interventions, in general feline practice. The focus is on the most commonly encountered oral and dental diseases in cats. These include periodontal disease, early-onset gingivitis, tooth resorption, endodontic disease and tooth trauma, feline chronic gingivostomatitis, developmental abnormalities such as malocclusion, and oral masses and growths, as well as various miscellaneous conditions. An extensive bibliography provides additional resources that extend beyond the topics reviewed in these Guidelines. Caregivers should be active participants in their cat’s oral and dental healthcare. Veterinary team members can empower their patients’ caregivers by educating them on signs of oral and dental disease in their cats and by providing home care guidance for maintaining oral and dental health. In any high-performing practice that cares for cats, the entire practice team are advocates for oral and dental care, and are knowledgeable about the principles of prevention and treatment of this important assortment of diseases.
Keywords
Introduction
Oral and dental diseases are common health problems in the domestic cat. Despite the relatively high prevalence of disease, prevention, recognition and diagnosis can be challenging both for cat caregivers and veterinary teams. With only a short period of domestica-tion 1 compared, for example, with dogs, cats have retained a strong survival instinct to conceal illness and pain. Their need for the safety of their home environment results in the protective emotion of fear–anxiety when they are removed.
Caregivers can be reluctant to bring their cat to the veterinary practice due to perceived stress in their cat before, during and after the veterinary visit. 2 Reluctance is further increased due to caregivers’ concerns related to mounting costs, the potential need for surgery and anesthesia, and the burden of care if treatment is needed at home. 3 Moreover, many caregivers may be unfamiliar with signs of oral and dental disease in their cats, further limiting the opportunity for diagnosis and treatment. For the veterinary team, the cat’s fear–anxiety response hampers oral examination and increases the challenge of identifying changes in the awake cat. These difficulties are further amplified if there is a need for team training in cat friendly interactions and/or a better understanding of feline oral and dental diseases. 4

The ‘2025 FelineVMA feline oral health and dental care guidelines’ provide a practical evidence-guided expert review of feline oral medicine, dentistry and oral surgery. The Guidelines are directed to all members of the veterinary team and include guidance on how to support caregivers as active participants in their cat’s dental healthcare. The Guidelines Task Force has provided information and recommendations based on an extensive literature review and, where published evidence is lacking, the authors’ cumulative experience.
Empowering the caregiver
Caregivers should be active participants in their cat’s oral and dental healthcare. As the veterinary team, we can empower caregivers by providing guidance, along with the tools necessary to succeed. Normal anatomy can be taught to caregivers by comparing oral models and anatomical drawings or pictures of the feline oral cavity and dentition with what we see in their cat’s mouth. For kittens, the veterinary team should describe the process of, and expected age for, the transition from deciduous to permanent teeth. Since cat friendly handling requires cooperation from the patient, 4 and time may be limited, the team should prepare the caregiver to observe the oral examination so that the opportunity is not missed. A return to the mouth later during the visit might provide a second opportunity to share our findings. Digital imaging of the cat’s mouth during the awake examination may be helpful. With the use of models, drawings and related caregiver resources (eg, information on dental care provided by Cats Protection 5 ), caregivers can be educated about common feline oral and dental diseases and how to recognize abnormalities.
Caregivers can observe for changes during the cat’s normal day-to-day activities, including eating, drinking, grooming, yawning or vocalizing. The veterinary team can proactively educate caregivers about the need to seek veterinary care should they detect unexpected oral odors, red or bleeding gums, chewing on one side of the mouth or with the head tilted to one side, dropping of food, pawing at the face, facial swelling, excess salivation, abnormal oral discharge of any kind and/or inappetence. Changes in appetite are an uncommon finding in cats with oral and dental diseases, so it should be emphasized to caregivers that a normal appetite does not always equate with a healthy mouth.
To successfully empower the caregiver in the prevention of periodontal disease (PD), the entire veterinary team needs to be aligned with respect to the information and recommendations they convey (see box ‘Veterinary team educational resources’). The veterinary team should be comfortable supporting and reinforcing recommendations made by the veterinarian.

Discussion and guidance for home preventive care starts with the first kitten visit and the recommendations should be reviewed at each appointment throughout the cat’s life. Caregiver resources can be found in the supplementary material accompanying these Guidelines. There is a confusing range of commercial products and procedures that make claims for the successful prevention or treatment of PD. The veterinary team will need to provide consistent messaging about what works, what is supported by science and what can be harmful. This should encompass:
✜ The need for, and importance of, regular oral evaluations of the awake cat by a veterinarian;
✜ Counseling on diets and treats that are appropriate for the prevention of PD;
✜ Recommendations for dental products for home care (eg, brushing, dentifrice, water additives and wipes – see Box 1);
✜ The importance of oral examination under anesthesia and problems associated with nonanesthetized (anesthesia-free) dental care;8,9
✜ The association between dental disease and pain.

Caregivers should be guided in the regular removal of plaque through brushing or wiping. Only safe and effective products should be recommended. Cooperative care training 4 can help to encourage the cat to participate willingly in the oral hygiene process; educational videos that the veterinary team can share to assist the training process, which can take time and effort, are available (see Videos 1 and 2 in the supplementary material). This training can also positively impact the cat’s acceptance of oral examinations at the veterinary practice.
Spectrum of care in dental health
The decision to pursue veterinary care for a feline pet is impacted by caregiver (client), veterinarian and patient factors (Figure 1). Spectrum of care includes and defines the factors that guide the veterinary team in providing individualized feline oral and dental disease management along a continuum. 4 This approach differs from a one-size-fits-all plan or the idea that there is only one ‘gold standard’ option for all patients.
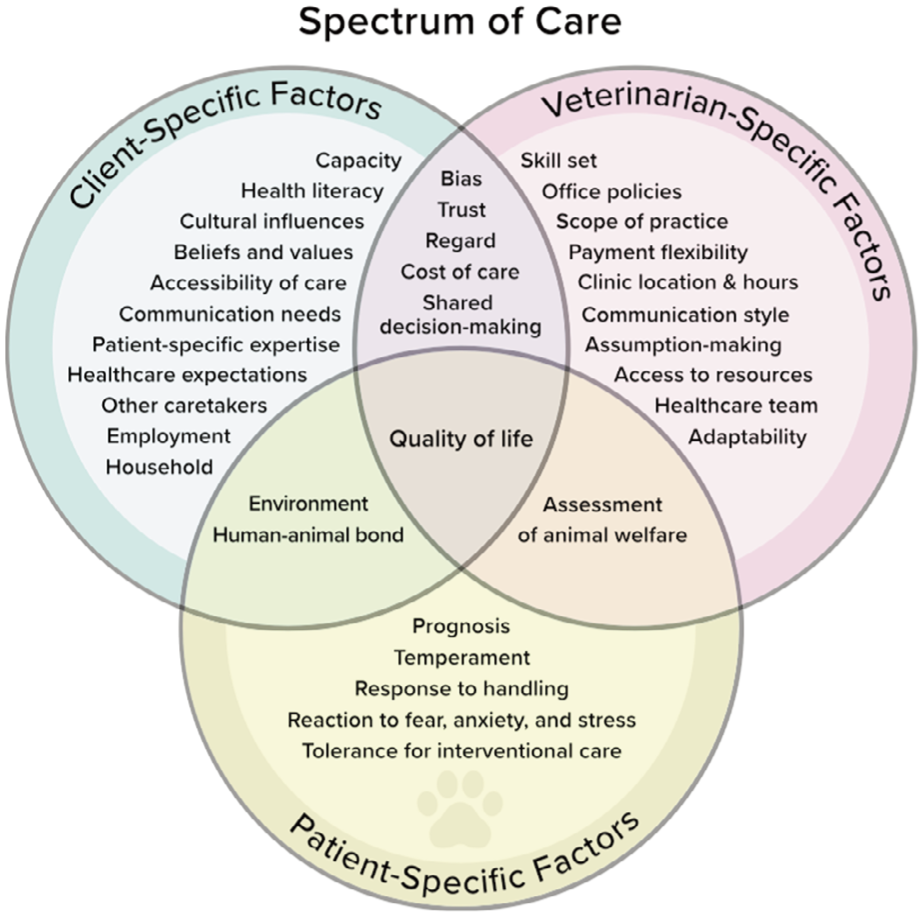
Client-, patient- and veterinarian-specific considerations that factor into the spectrum-of-care approach to the practice of veterinary medicine. Reproduced from Englar.3 Available at: https://journals.sagepub.com/doi/full/10.1177/1098612X231209855. Copyright The Author(s) 2023
Patient quality of life is a central consideration in determining a dental care treatment plan. As a result of spectrum-of-care factors, treatment expectations may not align between the veterinarian and caregiver. For example, the veterinary team may have a strong conviction of what constitutes ‘ideal’ care and consider that any other approach is deficient. This can be particularly difficult for caregivers to accept if they have different goals for treatment based on concerns about dental surgery or anesthesia, finances, cultural influences, difficulties with at-home care, or confusion over how the veterinary team’s recommendations compare with what they are exposed to through various media.
Open dialogue about expectations and goals will help the veterinary team create trust with the caregiver. Good veterinarian–caregiver communication avoids having clients feel that their concerns are not being heard or that the care being provided is inadequate. Communication with spectrum of care in mind allows the veterinary team to work with the caregiver in a shared decision-making process that results in a plan that is individualized and appropriate for all concerned, including the patient.
Feline oral and dental diseases
This section provides a narrative overview of the major feline oral and dental diseases, and consensus considerations for diagnosis and treatment. Table 1 lists relevant published literature and reported prevalence in relation to a number of these disease entities.
Prevalence of oral and dental diseases in cats by published source

Aggregate range of prevalence
Periodontal disease
PD is one of the most common types of dental disease in cats and is only preventable or reversible before alveolar bone loss has occurred. To the general public, the term PD is synonymous with ‘gum disease’, though it involves other tissues and is caused by the host’s immune and inflammatory responses to bacterial infection of the periodontal tissues supporting the teeth (periodontium); that is, the tooth cementum, gingiva, alveolar bone and periodontal ligament (which acts as a sling between the tooth cementum and alveolar bone).
The term PD encompasses gingivitis, which is the early reversible stage of the disease process, and the progressive changes leading to periodontitis, where there is an irreversible loss of the supporting structures of the teeth. In gingivitis, the gum tissue may be erythematous, swollen or painful. Clinical signs of PD might also include halitosis, loose teeth, bleeding gums, gingival recession, inappetence and discomfort, as displayed by facial rubbing and being ‘mouth shy’, although in many cases clinical signs are absent.


Normal periodontal tissues (PD0). Neither gingival inflammation nor periodontitis is clinically evident (radiographs are required to confirm absence of bone loss). Image courtesy of Heidi Lobprise
Thickened gingiva but no pocket depth due to attachment loss (PD1) (radiographs are required to confirm absence of bone loss). Image courtesy of Heidi Lobprise

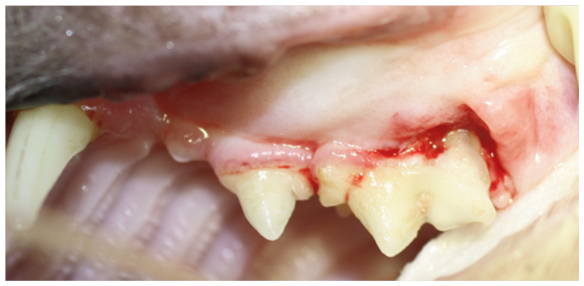
Early periodontitis (PD2). Left maxilla showing deposits of calculus and marginal gingivitis, with possible gingival recession at the maxillary canine tooth (204) (periodontal probing and radiographs are required to confirm <25% attachment loss). Image courtesy of Heidi Lobprise
Moderate periodontitis (PD3). Image courtesy of Heidi Lobprise
Advanced periodontitis (PD4). Image courtesy of Heidi Lobprise
Since a patient may have multiple teeth that have different stages of disease (see box ‘Stages of periodontal disease’), the severity of PD is determined on a tooth-by-tooth basis. 7 PD alternates between episodes of disease activity and quiescence. If untreated, PD progresses from mild inflammation to severe tissue destruction.
Pathogenesis
PD is a complex disorder resulting from an interplay between genetic predisposition, dysbiosis of the microbiome (involving bacteria, fungi and viruses) and the immune–inflammatory environment. Oral microbiota dysbiosis may cause disease through several molecular mechanisms. 24 Finely tuned ‘crosstalk’ between the oral microbiota, immune cells and epithelium is crucial for maintenance of the mucosal architecture and homeostasis. 25 There is also evidence to suggest that perturbations in the mucosal microbiota can modulate innate and adaptive immune responses, with inflammation arising due to changes in the balance of commensal or pathological microorganisms. 26
Diagnosis
Periodontitis may occur as a focal or localized disease, a semi-generalized disease or generalized disease (involving the entire dentition). Thus, a diagnosis of PD should consist of a tooth-by-tooth assessment. An anesthetized, comprehensive oral and periodontal examination with dental charting and full-mouth dental radiographs or advanced imaging is essential for this evaluation.
Complete periodontal assessment includes:
✜ Assignment of a plaque index, calculus index and gingival index (Table 2);
✜ Six separate points of measurement along the gingival sulcus/pocket (in mm);
✜ Measurement of gingival recession or gingival hyperplasia (in mm);
✜ Evaluation of furcation involvement of multirooted teeth (Table 2); and
✜ Mobility scoring (Table 2).
Periodontal disease indices

Based on American Veterinary Dental College (AVDC) nomenclature (avdc.org/avdc-nomenclature)
The veterinarian can then determine the level of periodontal attachment loss for each tooth. This guides the prognosis for tooth retention within the mouth.
Radiography
Full-mouth dental radiography will allow the amount of alveolar bone loss for each tooth to be ascertained, and whether attachment loss is horizontal or vertical (Figure 7). Additionally, the shape of furcation lesions is revealed, as well as the presence of concomitant pulp infection (ie, periodontal-endodontic lesions).

Radiograph of the left mandible of a cat with horizontal bone loss across several teeth. Image courtesy of Heidi Lobprise
Treatment
Plaque control with comprehensive supra- and subgingival plaque removal is at the heart of PD prevention and treatment. Tooth extraction may be necessary. Antibiotics are rarely indicated in the treatment of PD (see ‘Use of systemic anti-biotics’).26,28 Once the cat has recovered from periodontal care under anesthesia, caregivers can be advised to attempt oral home care, potentially including use of VOHC-approved products (see Box 1). For protective cats with fear–anxiety and pain, this may not be possible.
Early-onset gingivitis
Early-onset gingivitis, also referred to as feline juvenile gingivitis, is observed clinically as marked gingival erythema in cats around 6–8 months of age (Figure 8), and confirmed radiographically by bone loss representative of moderate-to-severe PD and histologically by neutrophilic lymphoplasmacytic inflamma-tion.29,30 The etiology is unknown. 29 Early intervention under general anesthesia is warranted to provide comprehensive periodontal treatment with extractions, as dictated by periodontal disease indices (Table 2). Follow-up evaluations are necessary as early-onset gingivitis can progress to aggressive periodontitis or feline chronic gingivostomatitis (FCGS). 30

Early-onset gingivitis, characterized by marked gingival erythema and even proliferation. Image courtesy of Heidi Lobprise
Chronic osteitis/alveolitis
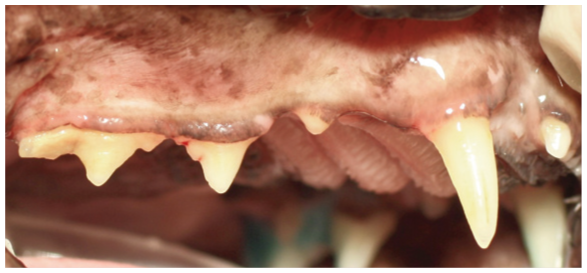
Chronic osteitis/alveolitis is a form of chronic periodontitis with buccal bone expansion that is seen most often in older cats (Figure 9). The inflammatory process will frequently involve crown or root resorption and extrusion (supereruption) of the tooth or multiple teeth. 31 The maxillary canine teeth are most commonly affected, with some mandibular canine involvement; often there is periodontal bone loss and even mobility. Extraction is frequently necessary.

Buccal bone expansion of the maxillary canines (104 and 204) in an older cat with super-eruption of all canines. Image courtesy of Heidi Lobprise


Normal occlusion. The mandibular canine teeth (304 and 404) are positioned between the maxillary third incisors (103 and 203) and canines (104 and 204).Image courtesy of Heidi Lobprise
Developmental abnormalities
While oral and dental diseases often occur in adult patients, there are a variety of developmental abnormalities that may be diagnosed in young cats. These can be related to maxillofacial development or to tooth development. In some cases, the abnormalities are observed as incidental findings, while for other feline patients they will cause significant clinical signs and pain. 29
Malocclusions
Malocclusions can either be developmental or acquired (eg, as a result of trauma or tumors). The focus of this discussion is developmental malocclusions, which should be treated when abnormal contact is causing trauma to soft tissue or to other teeth. See box ‘Normal occlusion’ for a description of the ideal dental alignment and Table 3 for a summary of how malocclusions can be divided into different classes based on whether they are primarily dental (only affecting teeth) or caused by skeletal abnormalities (involving abnormal relationships between the maxillae and mandibles).
Classification of feline malocclusions
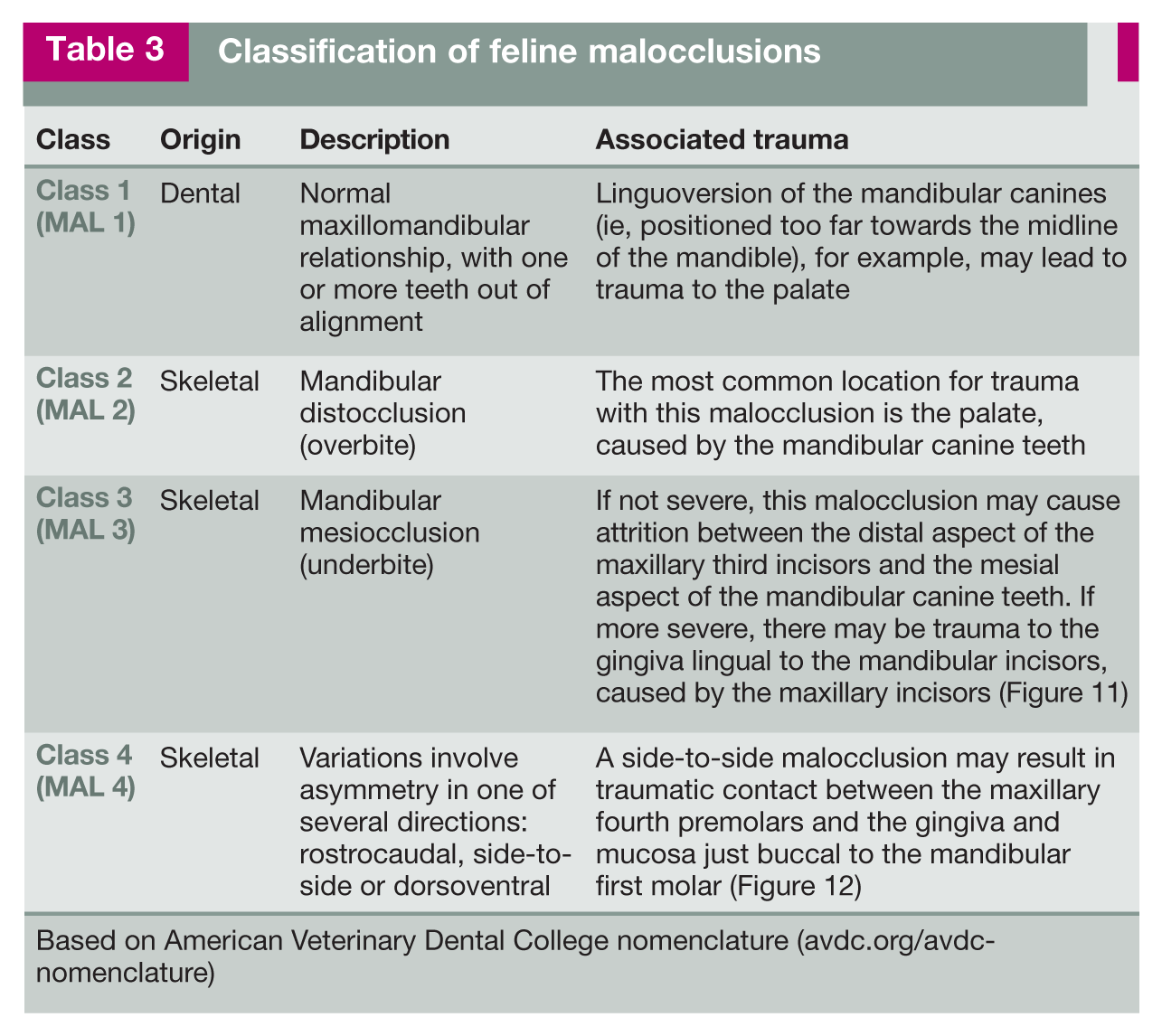
Based on American Veterinary Dental College nomenclature (avdc.org/avdc-nomenclature)

MAL 3 on the right side of a mandibular mesiocclusion. This case was asymmetrical (the left side was not as severe). Image courtesy of Heidi Lobprise
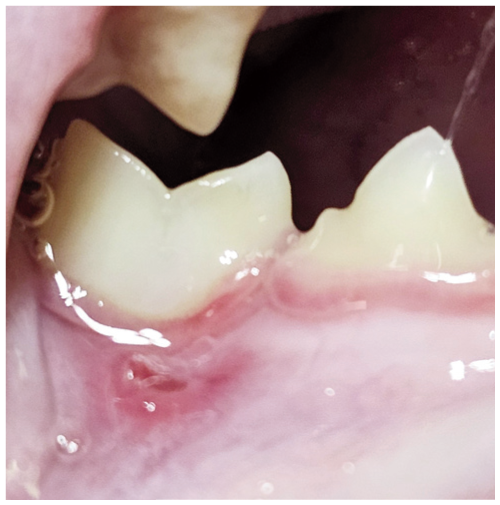
MAL 4 side-to-side malocclusion with damage to the mucosa buccal to the right mandibular first molar (409) caused by contact trauma from the right maxillary fourth premolar (108). Image courtesy of Heidi Lobprise
After careful evaluation of a malocclusion and consultation with the caregiver about their goals for the cat’s health, treatments should be offered that prioritize creation of a functional and pain-free occlusion. In contrast to human dentistry, treatments that involve purely cosmetic changes should not be offered as an option for feline dental patients. In addition, most skeletal malocclusions should be considered as potentially familial or genetic in origin, so breeding counseling may be needed. It is important to note that when malocclusions are identified in the deciduous dentition, treatment options may need to be considered in both the deciduous and permanent dentitions.
Abnormal dental anatomy
Variations in dental anatomy seen in cats include supernumerary teeth and roots, fused roots and hypodontia (absence of some teeth, leading to an incomplete permanent dentition). When evaluating abnormal dental anatomy, it is important to complete an anesthetized oral examination with radiographs to determine whether the abnormal teeth are vital and whether there are unerupted teeth. Supernumerary teeth that are not causing overcrowding can be maintained in the oral cavity.
Maxillofacial clefts
Maxillofacial clefts are recognized in cats, 32 and are abnormalities that involve failure of the two developmental halves of the maxillofacial structures to fuse during fetal development. Complete clefts that create a communication between the oral and nasal cavities typically require surgical correction in order for the cat to avoid future clinical problems, such as aspiration of food, chronic rhinitis and the risk of aspiration pneumonia.
Feline chronic gingivostomatitis
Stomatitis is classically defined as inflammation of the mucous membranes lining the mouth, a condition that causes pain and discomfort. FCGS is a more severe and persistent form of stomatitis. This painful oral disease is characterized by gingival inflammation extending into the mucosa, with erythema, ulceration and proliferation, and may involve the caudal oral cavity (Figure 13). (The terms fauces and faucitis were previously used but are less accurate.) Extension of inflammation into the esophagus has also been reported. 33 Cats with FCGS commonly have PD and tooth resorption, 34 although some cats will have no dental disease.

Feline chronic gingivostomatitis, with involvement of the caudal oral cavity. Image courtesy of Heidi Lobprise
Etiology and diagnostic criteria
The etiology of FCGS is likely multifactorial because the oral mucosa is constantly challenged by antigens derived from multiple sources, including food, grooming, and viral, bacterial and fungal microorganisms, as well as being impacted by the local and systemic immune system. Newer studies have evaluated the role of calicivirus, 35 the oral micro-biome,24,36 and immune and inflammatory genes and pathways. 37
Generally, diagnosis of FCGS is based on its clinical manifestations rather than histopathology or other clinicopathological findings. Hyperglobulinemia is common and may be pronounced. 34 Recent routine testing for feline immunodeficiency virus and feline leukemia virus is an important part of a cat’s evaluation prior to treatment because of the prognostic significance.
Treatment
Therapy is based on a thorough anesthetized oral examination and full-mouth dental radiographic evaluation. In most cases, it may be better to manage this disease rather than expect to treat and resolve it. 38 Traditionally, antimicrobials and immunosuppressive drugs (eg, corticosteroids) have been used as first-line treatments, yielding some positive response. However, chronic steroid usage and indiscriminate use of antimicrobials is not recommended since it does not resolve the disease nor treat related pain (and also raises issues regarding antimicrobial stewardship [see ‘Use of systemic antibiotics’]).
Until we learn more about its etiology, surgical intervention is the most effective method for management of FCGS. Two approaches are recommended. One is partial caudal mouth extractions, including extraction of the premolar and molar teeth. The other is full-mouth extraction of all of the dentition. Both options require extraction of retained roots and alveoloplasty. Appropriate analgesic therapy before, during and after extractions is essential. For some general practitioners, these procedures may require referral to a Board-Certified Veterinary Dentist® (see Box 2).

The consensus of the Guidelines Task Force is that early intervention is preferred. Whether full or partial mouth extractions are performed depends on the extent of inflammation around the incisors and/or canines. In cases where there is no inflammation around these teeth, partial mouth extractions can be performed provided caregivers are committed to regular follow-up.
In one study of 95 cases, 39% of patients showed substantial clinical improvement postextraction and 28% experienced complete resolution of stomatitis. 39 In spite of this, many patients will require continued medical management. Use of a scoring system such as the Stomatitis Disease Activity Index (SDAI) 40 – based on erythema and ulceration and/or proliferation of the oral mucosal tissues – may assist in determining the response to therapy and help to frame discussions with the caregiver regarding a patient’s prognosis (Table 4).
Stomatitis Disease Activity Index (SDAI) scoring criteria

Based on Anderson 40
Areas scored include the maxillary gingiva, maxillary buccal mucosa, mandibular gingiva, mandibular buccal mucosa, palatoglossal arch, sublingual tissue and molar flap More information on the SDAI scoring system is available in the supplementary material
Cases are considered refractory when there is a lack of response to tooth extraction therapy at least 6 months after surgery. 38 Numerous therapeutic regimens have been suggested for cats who are refractory to partial or fullmouth extractions (Table 5).
Treatment regimens evaluated in cases of refractory feline chronic gingivostomatitis
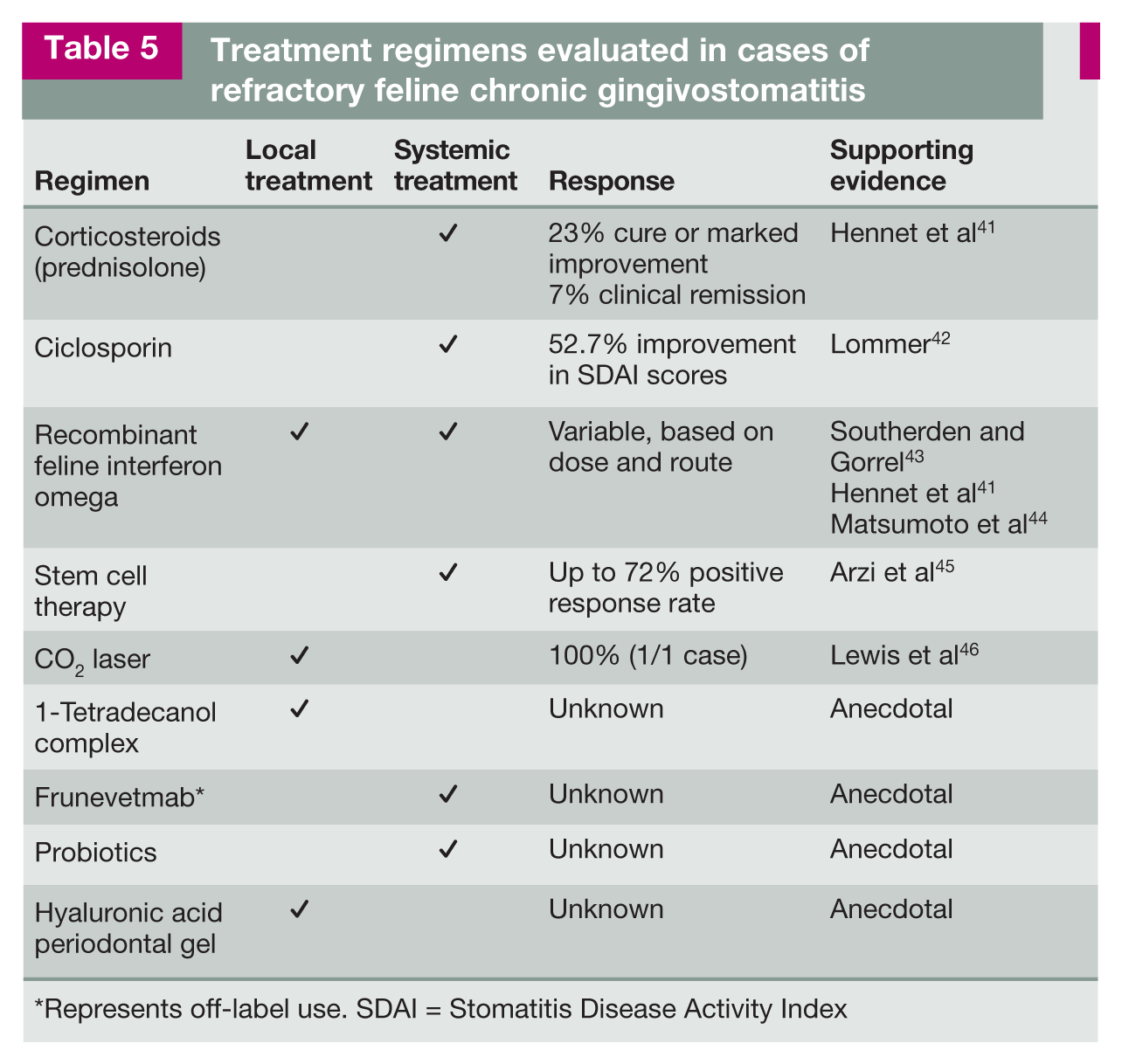
Represents off-label use. SDAI = Stomatitis Disease Activity Index


Type 1 tooth resorption affecting the left mandibular fourth premolar (308) and first molar (309). Image courtesy of Cornell University

Type 2 tooth resorption affecting the left and right mandibular canines (304 and 404). Image courtesy of Cornell University

Type 3 tooth resorption affecting the left mandibular first molar (309). Image courtesy of Cornell University
An open and honest discussion early on with the caregiver about the prognosis for cats with FCGS is essential. It is also important to emphasize the need for regular visits with the veterinarian following full or partial mouth extractions.
Tooth resorption
Tooth resorption is a common, progressive and often painful condition, with a reported prevalence in cats ranging from 28.5% to 67%.12,16–18 Abnormal activation of multinucleated odontoclasts results in resorption of mineralized tissues on the root surface that eventually extends coronally.47,48 The three types of tooth resorption recognized are described in the box ‘Classification of tooth resorption’.
Despite various hypotheses, the etiology of TR remains unclear.24,51–53 Studies have shown an increase in prevalence with increasing age,47,54 while findings regarding a specific breed predisposition have not been consistent.18,55 Although any tooth may develop resorptive lesions, the mandibular premolar teeth are most commonly affected, making them useful teeth to focus on during routine examination. 47
Diagnosis
✜
✜

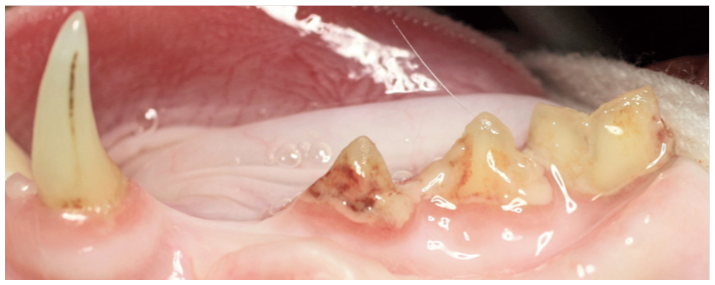
While not appearing inflamed, gingival tissue is encroaching into the resorptive lesions of the crowns of the third premolar (407) and first mandibular molar (409). Image courtesy of Heidi Lobprise
✜

Late-stage tooth resorption. Note the complete gingival coverage of the left mandibular third premolar (307). Image courtesy of Cornell University

Detection of a tooth resorptive lesion using a dental explorer. Image courtesy of Heidi Lobprise
✜
Treatment
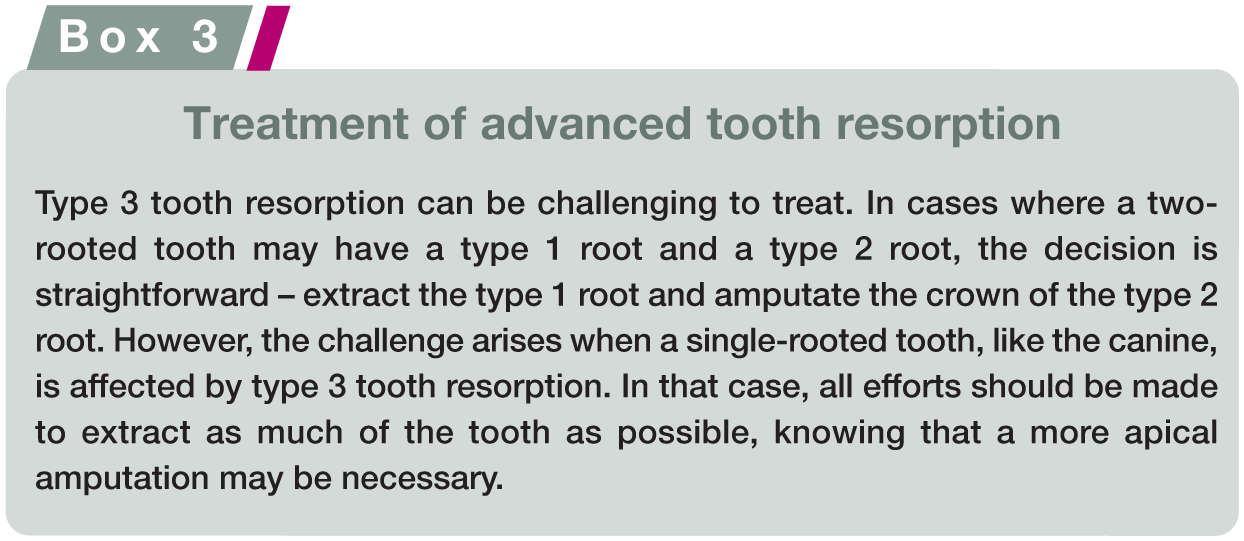
The principal aim of treatment is the alleviation of pain. Unfortunately, no prevention for tooth resorption has been found and there is no method of stopping the progression of an already existing lesion. Intervention options are outlined below, and the treatment of advanced tooth resorption is described in Box 3.
✜
✜
✜
Follow-up
Given the progressive nature of this condition, once a cat has been diagnosed with tooth resorption, it is likely that more lesions will develop in currently unaffected teeth. Caregivers should be informed that radiographic re-checks are necessary, ideally on an annual basis.
Oral and dental trauma
Tooth trauma
Tooth trauma leading to pulp exposure is the most common cause of endodontic disease in cats (Figure 20a). Endodontic disease is defined as inflammation and infection of the pulp complex within a tooth, resulting in pulp necrosis. Tooth fractures can be classified based on whether or not pulp exposure has occurred (Table 6), 56 and evaluation of the involvement of pulp is important when determining what treatment should be given.
Types of tooth trauma and recommended treatment
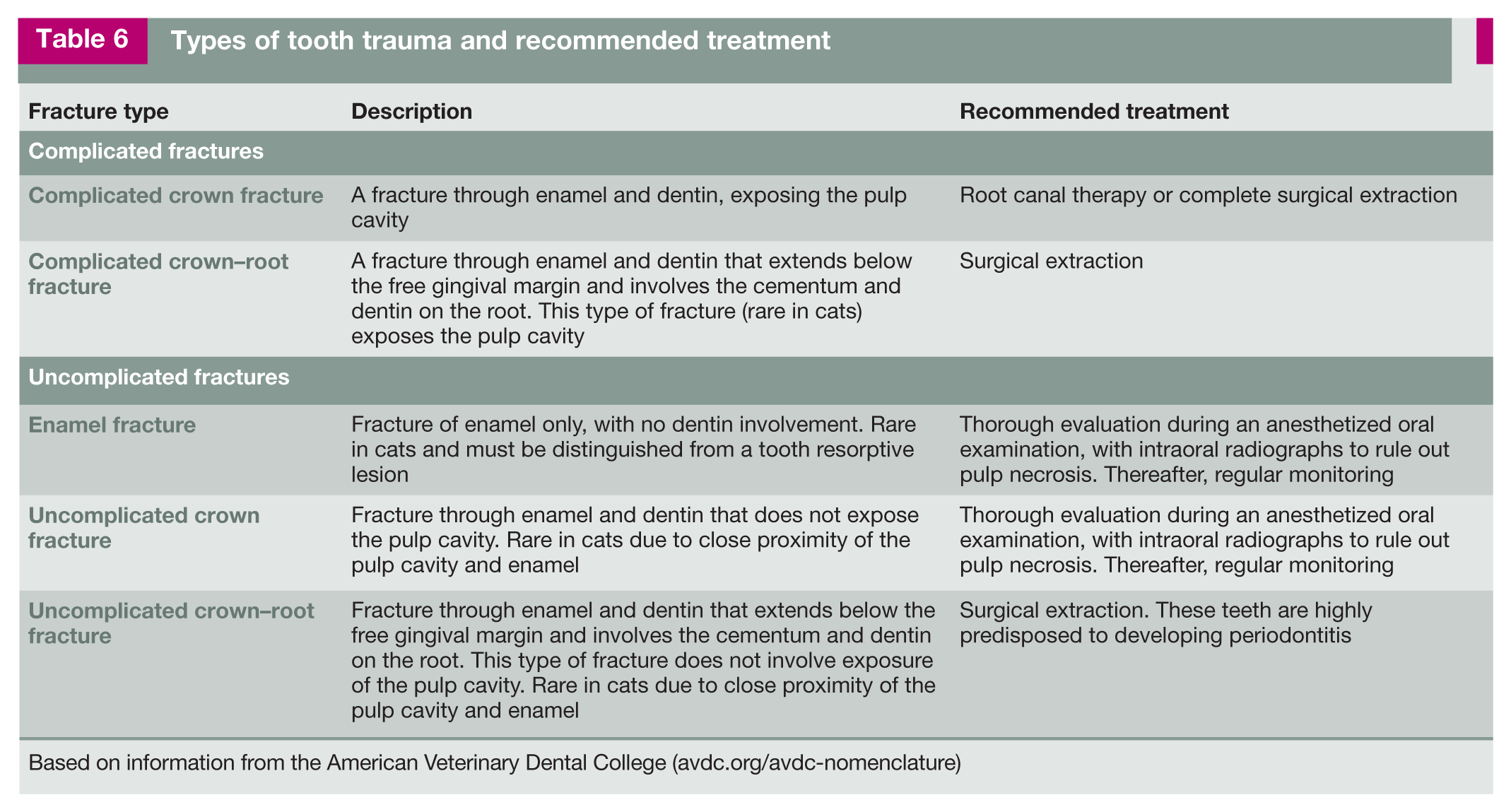
Based on information from the American Veterinary Dental College (avdc.org/avdc-nomenclature)
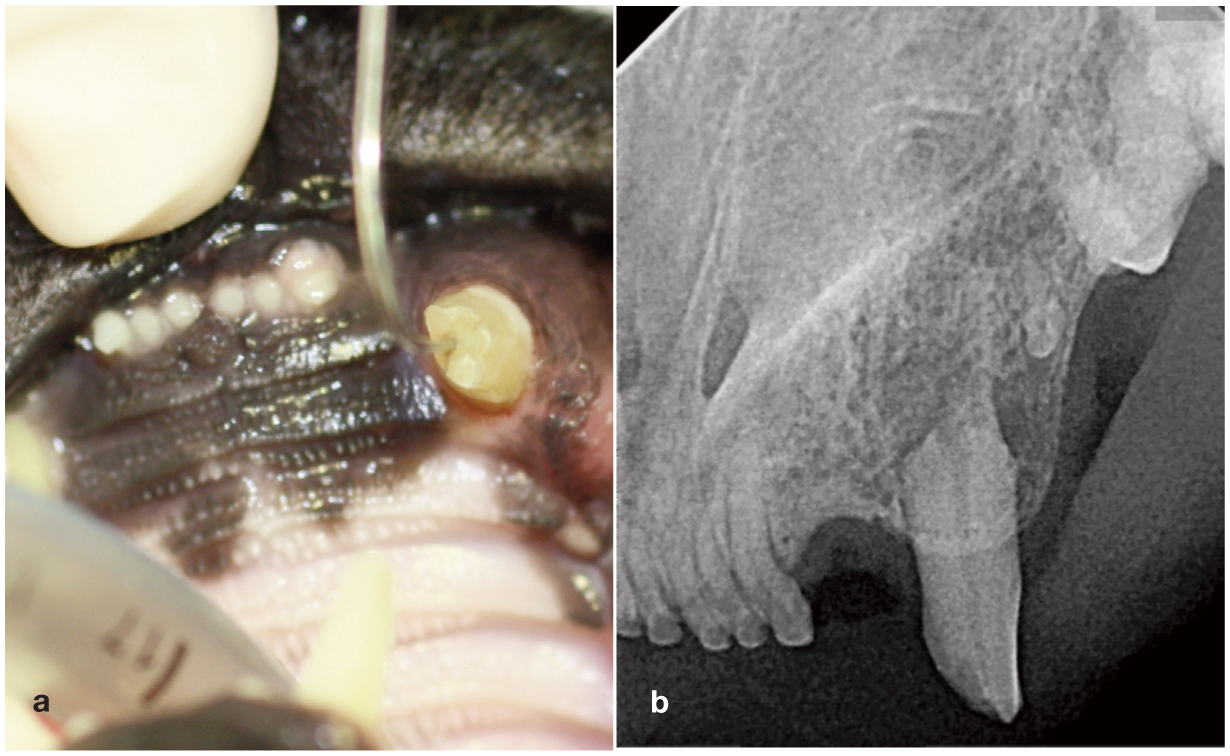
(a) Complicated crown fracture with dental explorer inserted into exposed pulp in the left maxillary canine (204). (b) Radiographic examination revealed signs of root resorption in the affected tooth. Extraction is indicated in such cases. Images courtesy of Heidi Lobprise
Diagnosis is based on examination of tooth structures combined with radiographic findings consistent with endodontic disease, including periapical lucency, inflammatory root resorption (Figure 20b), failure of the pulp cavity to narrow with age and condensing osteitis adjacent to the apex. 57
Treatments for endodontic disease include surgical extraction or root canal therapy if there is no resorption present. Complicated fractures involving the pulp cavity require treatment even if the cat is not showing overt signs of pain. Uncomplicated fractures may still result in pulp necrosis and must be evaluated prior to recommending a monitoring approach to the tooth in the oral cavity.
Tooth luxation/avulsion
Tooth luxation is the displacement of a tooth from its alveolus, while avulsion is the complete removal of a tooth from its alveolus; in both cases there is damage to the structures of the periodontium. While sometimes due to external trauma, luxation or avulsion can also be a sequela of advanced PD or neoplasia. In rare cases of luxation, tooth repositioning can be considered. More commonly, diagnostic radiography is needed to evaluate the cause and extent of the injury, followed by extraction with closure of the site.
Maxillofacial trauma
Maxillofacial trauma can result in soft tissue injuries, fractures, symphyseal separation or temporomandibular joint luxation.58,59 Cats have a fibrocartilaginous joint at their mandibular symphysis, which may have a degree of laxity normally. If there is no soft tissue involvement with mild symphyseal laxity, no treatment is necessary.
Due to the complexity of feline maxillofacial anatomy, intraoral radiography can only provide good imaging of the dentate portion of the jaw. Skull radiographs are limited in their diagnostic relevance because of superimposition of osseous structures. Depending on the nature of the traumatic injury, multiple fractures may be missed. In the absence of referral to a specialist, a combination of intraoral and skull radiography may allow for conservative management of maxillofacial trauma. Three-dimensional imaging such as CT or cone beam CT is much more ideal for evaluating complex maxillofacial trauma involving the caudal maxilla, mandible and temporomandibular joint (Figure 21). In such cases, a referral specialist may facilitate advanced maxillofacial repair.

Conventional CT image of a cat with extensive trauma to the craniofacial region, including the maxillary, palatine, pterygoid and nasal bones. Image courtesy of the Department of Dentistry and Oral Surgery, Colorado State University
Oral masses and growths
Caregivers should be encouraged to report any observations suggestive of a growth in their cat’s mouth, which should trigger prompt assessment by a veterinarian. Assessment may start with a conscious oral examination, but will likely involve diagnostic imaging and biopsy to better define and diagnose the lesion. Thorough oral examination at every visit may reveal preclinical lesions. Clinical signs will vary depending on the type of mass and its location. Most overt clinical signs are associated with advanced disease and can include changes in chewing behavior, decreased appetite, reduced grooming, halitosis, oral bleeding, ptyalism, facial deformity and muscle wasting.
It is important that veterinarians initially consider the differential diagnoses for oral masses broadly (neoplastic vs non-neoplastic), and narrow their list based on signalment, history, clinical signs, lesion location and appearance. 60 Table 7 outlines a systematic approach to evaluating oral masses in the cat according to neoplastic status. Detailed discussion of each differential diagnosis is beyond the scope of these Guidelines, but is accessible in the literature cited.
Types of oral masses in the cat


Gingival squamous cell carcinoma. Image courtesy of Cornell University

Feline inductive odontogenic tumor in the right maxilla. Image courtesy of Cornell University

Eosinophilic granuloma. Image courtesy of Cornell University

Pyogenic granuloma at the site of an extracted mandibular first molar (409) due to contact trauma from the right maxillary fourth premolar (108). Image courtesy of Heidi Lobprise
Diagnostics
✜
✜
✜
Although fine-needle aspiration and cytology of oral masses has been reported as being an appropriate diagnostic method, 79 it is not always definitive and histopathology will often still be necessary.
Miscellaneous conditions
Medication-related osteonecrosis of the jaw
Cats treated with a bisphosphonate or anti-resorptive drug for idiopathic hypercalcemia can be at risk for medication-related osteonecrosis of the jaw. 71 If possible, any dental surgery should be performed prior to the use of bisphosphonates. Oral discomfort and swelling, with a draining tract or abscess at a focal, non-healing extraction site, is the most common presentation. 71 Aggressive debridement and appropriate antibiotic use are indicated, and revision surgeries are often required.
Patellar fracture and dental anomaly syndrome
Patellar fracture and dental anomaly syndrome is characterized by atraumatic (patellar) bone fractures, persistent deciduous teeth and impacted permanent teeth in young cats. 80 Jaw swelling, osteomyelitis and necrotic bone may also be present. 81 Given the severity of osteomyelitis, early and aggressive surgical intervention is warranted. Extraction of persistent deciduous teeth and impacted permanent teeth, along with debridement of affected bone, is typically necessary for optimal results. 82
Autoimmune oral diseases
Autoimmune blistering skin diseases can have oral manifestations (Figure 26). 83 In cases of mucous membrane pemphigoid, the oral cavity (gingiva, soft and hard palate) is the most common site for lesions. 83 Fragile vesicles and bullae that progress to ulceration and deep erosion can also be seen in pemphigus foliaceus and, rarely, pemphigus vulgaris. 84 The vesicles and ulceration should be differentiated from calicivirus lesions. While there have been historical reports of drug-induced pemphigus foliaceus, underlying triggers in pemphigus foliaceus and autoantibody targets in pemphigus vulgaris have not been identified. 84 Vasculitis from reactions to drugs, vaccines, trauma or infections may cause deep erosions and ulcers with scarring.

Cat with bullous pemphigoid lesions on the (a) tongue and (b) ear. Images courtesy of the Department of Dentistry and Oral Surgery, Colorado State University
Perilesional biopsy (lesion bordered with normal tissue) should be performed for any suspicious lesion, unless a full vesicle can be obtained. Treatment usually follows the general principles of immunosuppressive therapy.
Sialocele
Sialocele, the submucosal or subcutaneous collection of saliva, is uncommon in cats. 85 When present, clinical signs include dysphagia, ptyalism and swelling of the neck. 86 The sublingual (Figure 27) and cervical regions are most commonly affected (ie, involving the mandibular and sublingual glands and their ducts). Typically, the cause is unknown. Surgical removal of the affected gland(s) is recommended, as marsupialization or drainage alone often leads to recurrence.

Sublingual sialocele. Image courtesy of Heidi Lobprise
Feline orofacial pain syndrome
Feline orofacial pain syndrome (FOPS), likely a neuropathic disorder impacting the trigeminal nerve, presents with signs of oral and facial discomfort (licking, chewing, tongue mutilation, pawing at the face). 87 Disease episodes, which are usually unilateral, seem to be triggered by stimuli such as erupting teeth, PD, tooth resorption and stress, and these need to be addressed. Typical pain management regimens are insufficient to provide relief, although anticonvulsant medication can be helpful. Most commonly seen in Burmese cats, FOPS is considered to be a heritable disease.
Patient assessment, evaluation and documentation
History and physical examination
Whenever possible, it can be helpful to have caregivers fill out a patient history form in advance of the visit. This may include information on lifestyle, nutrition, dental history, current home care and medications, and behaviors observed at home. Receiving this information in advance of an appointment can help alert the practitioner to areas of concern.
Any comprehensive oral evaluation must start with a non-anesthetized patient and include a preoperative medical history and complete physical examination. 88 This will allow the veterinarian to identify conditions that might impact the ability to safely anesthetize a patient, and can help determine whether the patient is experiencing pain and might benefit from analgesia before the anesthetized procedure. It can also give clues to oral and dental diseases that may be affecting the cat’s overall health. For example, unilateral nasal discharge can be a sign of endodontic disease. A poor haircoat might be associated with decreased grooming, which can point to oral pain. Other information collected in the medical history that might indicate oral disease include facial rubbing, ptyalism, decreased appetite, food avoidance or changes in food texture preferences. Subtle behavioral changes can also be significant in cats. Use of open-ended questions about the cat’s behavior will help to identify nonspecific signs of pain including decreased activity or decreased sociability with caregivers or other animals in the home.
Careful auscultation of the heart and lungs, palpation of the abdomen, and evaluation of trends in the patient’s body weight, body condition score and lean muscle mass are all important screening tools for a patient who will be considered for an anesthetized procedure. Certain cases may require additional preanesthetic screening. Blood pressure testing should be included for patients over 9 years of age and those with evidence of target organ damage (hypertensive retinopathy, cardiac changes, behavioral changes related to cognitive and neurological function, evidence of kidney disease).89,90 Completion of blood pressure assessment early in the evaluation process is consistent with cat friendly principles. 2


Directional terminology of the maxilla and mandible. Image courtesy of Heidi Lobprise
Awake oral and dental examination
A thorough, non-anesthetized oral examination in cats who will allow it, or sedated examination in cats who will not, is a critical part of preparing the patient and caregiver for a future dental procedure. It will also allow the veterinarian to schedule the procedure appropriately, factoring in enough perioperative time for complicated cases. Additionally, this is an excellent time to evaluate the patient’s emotions and related behaviors and to make determinations about treatment and management of transportation, hospitalization-related stress and the need for any previsit medication. In some cats, procedural sedation and analgesia can be very effective for allowing an oral examination (see ‘Anesthesia and analgesia’). 94 The preliminary awake-patient examination should incorporate cat friendly techniques to minimize fear–anxiety and pain associated with interactions and handling, and in order for the examination to be completed efficiently. 4
Findings of the examination help guide communication with caregivers about what to expect during an anesthetized dental proce-dure. 95 Many caregivers have concerns about the possibility of tooth extraction and the risks associated with anesthesia. Good veterinarian– caregiver communication can make this a less stressful experience for them. The awake-patient examination also allows the veterinary professional to provide the caregiver with a more accurate fee estimate so that surprises on the day of the procedure are kept to a minimum.
The non-anesthetized oral examination can be broken down into four steps – extraoral examination, examination of occlusion, examination of oral soft tissues and examination of tooth structures. Each of these steps can take just a few moments and can deliver a wealth of information (see Video 3 in the supplementary material).
✜
✜
✜
any deviation from normal anatomical shape, color and size, as well as any asymmetry, should be noted.
✜
Oral and dental examination under anesthesia
Preparation for anesthesia includes a comprehensive physical examination and interpretation of appropriate clinicopathological tests, followed by assignment of an American Society of Anesthesiologists (ASA) physical status classification (Table 8). 96 Assessment of preanesthetic health can be challenging in cats because they often hide disease. Clinicopathological tests that should be considered in assignment of ASA status include, as a minimum, blood urea nitrogen,
ASA physical status classification system modified for cats
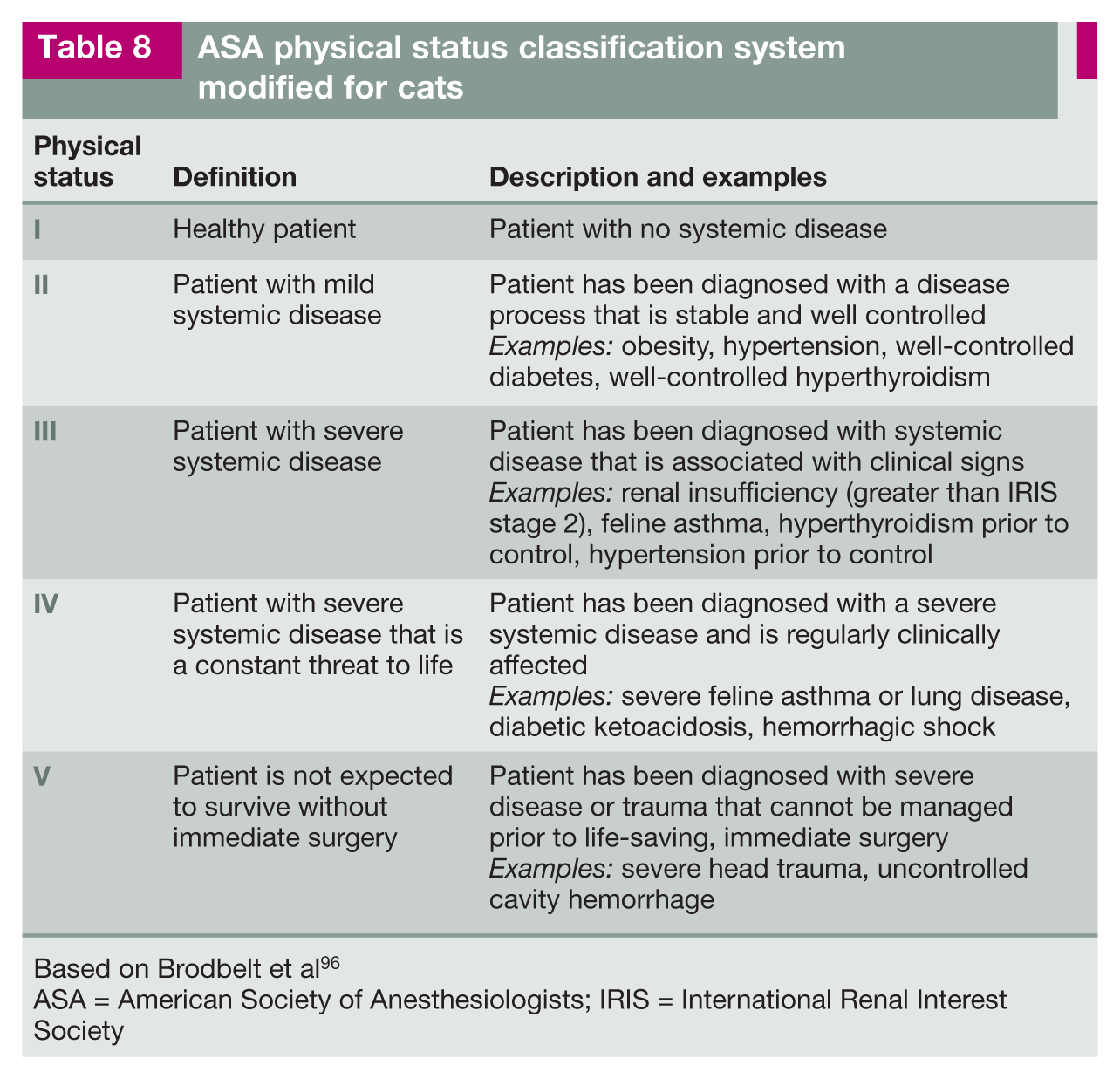
Based on Brodbelt et al 96
ASA = American Society of Anesthesiologists; IRIS = International Renal Interest Society
creatinine, hematocrit, total protein, alanine transferase and alkaline phosphatase values. In most cats, a more complete pre-surgical screening is appropriate, with test selection being patient dependent. Testing may include N-terminal pro B-type natriuretic peptide, thyroid panel, urinalysis, complete blood count and additional blood chemistry tests (eg, blood glucose, symmetric dimethylarginine and electrolytes). Additional screening tests may be deemed necessary based on increasing ASA status, including thoracic radiographs, electrocardiography and preoperative blood pressure measurement.
The majority of dentistry patients will be in the I, II and III ASA classifications. A cat’s age is a risk factor independent of ASA status, especially for cats over 12 years of age. 97 However, in one study looking at 138 cats undergoing more than 30 mins of general anesthesia, veterinary ASA status (as derived from the human literature), but not age, was considered a risk factor for the development of perianesthetic complications. 98 In a recent large prospective study, the rate of anesthesia-related deaths was only 0.63% in cats; however, nearly 75% of mortalities occurred in the postoperative period, highlighting the need for careful postoperative monitoring. 99
After a cat has been determined to be an appropriate candidate for anesthesia and the caregiver has been prepared for the procedure, with an understanding of the cost, the team can proceed. When implementing a plan for anesthetic procedures, it is important to develop a system that can be performed in a similar way by everyone in the practice. This approach avoids missed steps in the anesthesia and examination protocol. The findings of the awake and anesthetized oral examination must be evaluated in relation to the patient’s radiographic findings. In other words, both the awake and anesthetized physical examination findings and the radiographic results should be considered together to develop an appropriate treatment plan for the patient.
A comprehensive anesthetized oral examination allows the veterinarian to evaluate structures that would not be visible in an awake patient. These include the tonsils, soft palate and sublingual region. All findings should be recorded on a dental chart (see supplementary material for an example). This oral examination is important for numerous reasons, including as a screening tool for oral cancer. Any abnormalities identified should be photographed and a determination made about whether an oral biopsy should be obtained. Before-and-after photographs of the oral cavity are recommended for documentation/tracking of disease progression and response to therapy, and for caregiver education.
Following examination of the oral cavity, the teeth should be evaluated one at a time, with findings recorded on the dental chart. Parameters that should be recorded for each tooth include the level of gingivitis, gingival recession, probing depth, mobility, furcation exposure and the presence of pathology, using the indices described in Table 2. This charting is performed with the aid of a probe and dental explorer, which may be stand-alone instruments or combined as a dual-ended explorer-probe (see box ‘Equipment considerations for feline patients’).


Two periodontal probes with lines marked for measuring in millimeters. Probes differ in terms of their measurement markings, so it is important to know what the specific instrument measures. Image courtesy of Heidi Lobprise


Examples of standard and sharp periosteal elevators surgical length carbide dental burs. Image courtesy of Cornell University

(a) Root tip pick and (b) root tip forceps. Images courtesy of Cornell University
To make the anesthetized oral examination as efficient as possible, it is ideal to perform ‘fourhanded dentistry’. One person (two hands) performs the oral examination utilizing the probe and explorer, while a second individual (two additional hands) records the information on the dental chart. 100 Both individuals must be appropriately trained to avoid missing pathology or confusing tooth names and numbers. If a veterinary technician or nurse is performing the oral examination (Box 5), then a veterinarian must confirm the findings and interpret the dental radiographs prior to planning treatment.
Radiography has been discussed throughout the Guidelines, as it pertains to the evaluation of oral and dental disease, as well as therapy assessment. Appropriate care for a patient requires, at a minimum, complete intraoral radiography.

All abnormal findings from the anesthetized oral examination must be recorded, particularly if an extraction is considered necessary. The completed dental chart is an important communication tool between veterinary professionals and should document all procedures performed (see box ‘Dental terminology and anatomy’). 101
Anesthesia and analgesia
Acknowledgement that oral and dental diseases, including assessment and treatment, can be painful is a strong rationale for analgesia. While good perioperative analgesia is critical, it is also important to provide the patient with pain management once disease is identified during the awake oral and dental examination, and until the procedure can be performed. The FelineVMA and the Guidelines Task Force oppose anesthesia-free dentistry and endorse previously published position statements concerning anesthesia-free dental treatments.7,102
This section covers some of the key principles of anesthesia and analgesia in the context of feline dentistry and oral care. For further guidance, the reader is referred to the following resources:
✜ AAFP feline anesthesia guidelines. 103
✜ 2020 AAHA anesthesia and monitoring guidelines for dogs and cats. 104
✜ 2022 AAFP/ISFM cat friendly veterinary interaction guidelines: approach and handling techniques. 4
✜ 2022 AAHA pain management guidelines for dogs and cats. 105
✜ The American College of Veterinary Anesthesia and Analgesia small animal anesthesia and sedation monitoring guidelines. 106
Presurgical considerations
During the awake examination, a comprehensive physical assessment is just as important as a detailed oral examination in determining a full list of concerns and for recommending clinical pathology testing.
Prior to the procedure itself, guidelines for recognition and management of protective emotions should be followed, 4 as a cat’s fear–anxiety can increase their perception of pain (see ‘Awake oral and dental examination’). An ASA classification should be assigned (see Table 8) and any comorbidities identified, such as endocrine, renal or cardiac conditions. Some patients may require additional stabilization of their condition prior to anesthesia.
All medications and supplements administered to the patient should be reviewed. Drugs that impact blood pressure, heart rate and cardiac or respiratory function should be evaluated for administration (or cessation) prior to the procedure and anesthetic event (Box 6). If it has been determined that previsit pharmaceuticals are warranted, such as anxiolytics (eg, gabapentin, pregabalin), antinausea agents or antacids, they should be given according to the manufacturer’s instructions and the findings of any related peer-reviewed studies. Antinausea drugs may be more effective if administered the night before the procedure. Food should be withheld for 4–6 h in healthy patients, 2–4 h in diabetic patients and 6–12 h in those patients at risk for regurgita-tion. 108 Water should not be withheld.

While one study has shown that gabapentin may decrease systolic blood pressure in healthy cats as well as those with chronic kidney disease, this is likely more important in the context of monitoring or treating feline hypertension, and less relevant to blood pressure under anes-thesia. 108 Given the benefits of decreasing stress levels and potential hypertensive responses to procedural stimuli, gabapentin should still be considered for use in order to alleviate fear–anxiety and increase compliance. 4
Anesthetic considerations
Preoperative medication should include analgesia and sedation appropriate to the patient’s ASA status, pain levels and comor-bidities. 103 Induction followed by inhalant anesthesia or total intravenous anesthesia with oxygen support requires intubation and protection of the airway. Airway-related complications include tracheal tears 109 and an increased risk of high airway pressure damage due to the small lung capacity of cats. 97 Use of anesthetic checklists can help coordinate the team’s efforts.
Placement of an intravenous catheter and administration of intravenous fluids is critical in general anesthesia. Given their relatively low blood volume (50–60 ml/kg), most cats require a fluid rate of 3 ml/kg/h. 110 For patients with renal compromise (International Renal Interest Society stage 3 or higher), at least 4 h of preoperative fluid therapy, at a rate of 3–5 ml/kg/h while monitoring for evidence of fluid overload, is recommended.111,112
Dental procedure times can vary dramatically in length and may be unpredictable due to the severity and extent of disease.
Preoperative and intraoperative analgesia
In addition to any analgesia provided during the preanesthetic period, other techniques such as local and regional blocks, and constant rate infusions (CRIs) can be employed for the dental surgery patient.
Local and regional blocks
Local and regional blocks are critical multimodal pain management techniques that are used to enhance perioperative patient comfort, help improve anesthesia stability and safety, and ease the transition to postoperative pain management. 7 Local anesthetic choice is dependent upon availability and surgeon preference.
There are several different approaches to block various regions of the mouth. Some commonly used regional blocks include inferior alveolar nerve blocks (eg, mandibular block; Figure 32), infraorbital nerve block (Figure 33), caudal maxillary nerve block (Figure 34) and mental nerve block. When regional blocks are not possible, another option may be to infiltrate local anesthetic in the mucosa at the surgical site to help block regional soft tissues.

Intraoral approach to the inferior alveolar nerve block. Image courtesy of the Department of Dentistry and Oral Surgery, Colorado State University

A 27 gauge needle is inserted into the infraorbital foramen, dorsal to the maxillary third premolar (107). This foramen is located at the most rostral aspect of the zygomatic arch. Image courtesy of the Department of Dentistry and Oral Surgery, Colorado State University

Subzygomatic approach to the caudal maxillary nerve block. Image courtesy of Heidi Lobprise
When planning a caudal maxillary nerve block on a cat, for example, it is important to be aware that the infraorbital canal is on average 3 mm long, regardless of skull shape. With any technique, extreme care must be taken with needle placement, including when confirming negative aspiration prior to injection. 113 In one study involving injection of dye and radiocontrast material, there was no significant difference in the distribution of injected material between an infraorbital technique (ie, needle not advanced into the infraorbital canal) and a caudal maxillary approach (percutaneous). 114
Analgesia in the oral cavity should be the goal during postoperative recovery (see ‘Postoperative recovery and discharge’). This can be achieved by repeating regional blocks at the end of the procedure or utilizing longer-acting agents. The duration of effect of a local anesthetic agent such as bupivacaine can be prolonged with the addition of opioids or vasoconstricting agents (eg, alpha-2 agonists, epinephrine). 115 Addition of epinephrine to oral local anesthesia may result in complications. 116 Longer-acting bupivacaine products are not labeled for use in the oral cavity, but may be considered.
Postoperative recovery and discharge
Monitoring and appropriate management of surgical patients is critical in the postoperative period, with over 60% of all anesthetic-related deaths in cats occurring within the first 3 h of the recovery period. 117 While some cats may be susceptible to hypothermia when under anesthesia, others may experience rebound hyperthermia, potentially associated with hydromorphone as well as other medications. 118
Use of multimodal analgesia extends into the postoperative and discharge periods. Nonsteroidal anti-inflammatory drugs, opioids (some with longer duration), gabapentinoids, N-methyl-D-aspartate (NMDA) receptor agonists and adjunct modalities (eg, cool compresses, targeted pulsed electromagnetic fields, cold laser, acupuncture) can optimize patient comfort. Patients identified as having neuropathic pain (eg, FOPS) may require a comprehensive management plan before, during and perhaps long-term after the procedure.87,119
Oral and dental surgical care under anesthesia
Anesthetic care, 103 dental radiography 120 and dental surgical care 121 for the feline patient have been covered in detail elsewhere. The focus in these Guidelines is specific practical considerations in reference to cats undergoing oral and dental surgery.
When should the first dental procedure be considered?
In the absence of any developmental abnormalities or juvenile manifestations of oral disease, clinicians may consider dental and oral assessment under anesthesia for patients beginning at 2 years of age. This would encompass careful assessment of the oral soft tissues as well as collection of baseline intraoral radiographs to help evaluate the teeth for PD/periodontitis and/or tooth resorption.
General considerations for feline dental procedures under anesthesia
✜
✜
hypothermia. Active warming of the patient (eg, using devices with conductive fabric or forced-air warming) is necessary, along with regular monitoring of body temperature during and immediately after the procedure.
✜
✜
✜

Methods of holding the mouth open for oral and dental surgery: (a) a portion of syringe used as a mouth prop and (b) the surgeon’s/technician’s fingers wedged gently in the mouth. In both cases, prolonged opening of the oral cavity should be avoided. Images courtesy of Cornell University
✜

Dental radiology safety chart. Adapted with permission from Cornell University
✜
✜
Typical workflow and staging of procedures
Box 7 describes the typical workflow for a feline patient undergoing a dental procedure as a series of steps. In some cases, there may be a necessity to consider staging of the procedure, particularly if more extensive oral surgery needs are found or if the procedure is prolonged. The initial assessment with radiographs, scaling and polishing, and simple extractions may be performed immediately, with either the advanced oral surgical procedures scheduled for a later date or the patient recommended for referral to a dental specialist (see Box 2).

Retained mesial root tip following incomplete extraction of the right mandibular first molar (409). Image courtesy of Heidi Lobprise

Displacement of the mesial root tip (and incomplete extraction of the distal root) of a left mandibular molar (309). Image courtesy of the Department of Dentistry and Oral Surgery, Colorado State University
Specific considerations in relation to tooth extraction
Extraction kit
Extraction technique and appropriate armamentarium for feline patients have been thoroughly described elsewhere.131–133 Some practical pointers regarding the extraction kit are given in the box ‘Equipment considerations for feline patients’.
Postsurgical complications
Potential complications during and following extractions have been described in the litera-ture134–138 and are listed in Box 8. Most complications can be avoided with appropriate instrumentation, good surgical technique and familiarity with regional anatomy.


Postoperative considerations
The following actions should be part of a postoperative checklist:
✜ Remove pharyngeal gauze pack.
✜ Suction any remaining fluid.
✜ Check oral cavity and pharynx for debris (a laryngoscope is helpful).
✜ Dry the patient’s head.
✜ Reapply eye lubrication.

Dehiscence and persistent oronasal fistula formation at the extraction site of a maxillary canine tooth (204). Image courtesy of the Department of Dentistry and Oral Surgery, Colorado State University

Lip entrapment trauma and oronasal fistula formation. Image courtesy of the Department of Dentistry and Oral Surgery, Colorado State University

Lip entrapment in an awake cat. Image courtesy of Naomi Hoyer
Analgesia indications
Analgesia is always indicated following any surgical procedure, including tooth extraction. Consideration should be given to readministering regional blocks if the procedure was more than 2–3 h in duration. Administration of analgesics (injectable or, for example, an opioid or ketamine CRI) can be initiated or continued in the immediate postoperative period, especially for patients undergoing extensive surgery. Use of long-acting opioids may be considered as part of a multimodal analgesia protocol, where available.
Oral analgesia choices will depend on the patient’s age and general health. Generally, a multimodal approach with 3–7 days’ post-surgical analgesia is adequate for most procedures. Postoperatively, the response to analgesia should be monitored using a validated pain-scoring system such as the Feline Grimace Scale.139,140 This particular scale has been validated for use both in the veterinary practice setting and at home by feline caregivers.141,142
Nutritional support
Postoperatively, some cats may be inappetent, particularly those who have undergone extensive procedures such as full-mouth extractions. Ensuring adequate intra- and postoperative analgesia will minimize oral pain that would otherwise discourage cats from eating. Patients may also need appetite stimulants and, in certain situations, preemptive placement of an esophageal tube. 143
Use of systemic antibiotics
Systemic antimicrobials are usually not indicated for routine dental prophylaxis or after tooth extractions. In cases of periodontitis, systemic antimicrobials are not a substitute for surgical treatment. In most cases of periapical tooth root abscesses, debridement of infected tissue is sufficient to control infection. 144
The Guidelines Task Force supports the pursuit of good antimicrobial stewardship. The use of systemic antimicrobials is generally not indicated before, during or after comprehensive oral examination and treatment under anesthesia. Antimicrobials have been routinely overused and misused, in some cases for unnecessarily prolonged periods associated with dental surgery. 145 The Task Force endorses the ‘2022 AAFP/AAHA antimicrobial stewardship guidelines’. 144
Antibiotic use in dentistry should be based on several patient factors. The patient’s immune status and the potential for immunosuppression are important considerations when deciding if antibiotics are indicated. Antimicrobials should not be used ‘just in case’.
The following recommendations are made for the use of systemic antibiotics when treating PD and performing dental extractions:
✜
✜
✜
These recommendations for systemic antimicrobial use in PD are generally applicable to other feline oral and dental diseases.
Conclusions
The ‘2025 FelineVMA feline oral health and dental care guidelines’ present evidence-guided recommendations for optimal oral and dental care, including therapeutic interventions, in general feline practice. An up-to-date review of common feline oral and dental diseases is provided, focusing on the role of prevention and early diagnosis and treatment. Moreover, a detailed discussion of assessment of the feline oral cavity encompasses both the awake and anesthetized examinations. As such, these Guidelines offer valuable reading and reference material for the entire veterinary team.
Veterinary team members provide ideal care when knowledge is shared and there is uniformity in the recommendations given to caregivers. Therefore, the goal is to foster collaborative relationships with caregivers that provide consistent messaging and an understanding of their cat’s oral and dental needs, and how to safely address them.
Daniel Dominguez of the FelineVMA; and Britta Siegenthaler, currently enrolled at the College of Veterinary Medicine and Biomedical Sciences, Colorado State University, in the preparation of the Guidelines manuscript.
Summary Points
✜ Oral and dental diseases are commonplace in cats.
✜ Veterinarians and veterinary teams have a responsibility to provide high-quality oral healthcare for their feline patients.
✜ The ‘2025 FelineVMA feline oral health and dental care guidelines’ provide up-to-date information about feline oral and dental diseases, including best practices for prevention, diagnosis and management.
✜ The entire practice team need to be advocates for oral and dental care, and knowledgeable about the principles of prevention and treatment of this important assortment of diseases.
✜ Preventive care strategies assist in maintaining feline oral health and achieving early diagnoses.
✜ Working closely with the caregiver is integral to fostering a good relationship that will increase caregiver receptiveness to guidance in home preventive care and in the pursuit of targeted treatment.

Supplemental Material
Supplementary Material
Feline dental chart.
Supplemental Material
Supplementary Material
Links to videos
Supplemental Material
FelineVMA client brochure
‘Feline dental care’.
Supplemental Material
Supplementary Material
Feline Stomatitis Disease Activity Index (SDAI) scoring chart.
Footnotes
Acknowledgements
These Guidelines were supported by an educational grant to the FelineVMA from Dechra. The Task Force gratefully acknowledges the contribution of Edward W Kanara, DVM, DABVP, of the Kanara Consulting Group; Mark Dana of Scientific Communications Services; Heather O’Steen, CAE of the FelineVMA; Liz Novak of the FelineVMA;
Supplementary material
The following supplementary material files are either available via the links below or at go.jfms.com/ 2025FelineVMAGLs_supplementarymaterial and at catvets.com/dental:
✜ Feline dental chart.
✜ Video 1: How to clean your cat’s teeth/feline dental care. catvets.com/how_to_clean_teeth. Courtesy of Cats Protection.
✜ Video 2: Helping your cat accept having its mouth checked. catvets.com/mouth_check. Courtesy of International Cat Care.
✜ Video 3: Non-anesthetized oral examination. catvets.com/feline_oral_exam. Courtesy of CSU VetCE at Colorado State University.
✜ FelineVMA client brochure: ‘Feline dental care’.
✜ Periodontal disease: catfriendly.com/periodontal.
✜ Caring for your cat’s teeth: catfriendly.com/ dentalcare.
✜ How to brush your cat’s teeth: catfriendly.com/ howtobrush.
✜ Feline Stomatitis Disease Activity Index (SDAI) scoring chart.
✜ 2022 ISFM consensus guidelines on the management of acute pain in cats. go.jfms.com/Acute_Pain_GLs.
Conflict of interest
Members of the Task Force have received financial remuneration for providing educational material, speaking at conferences and/or consultancy work; however, none of these activities cause any direct conflict of interest in relation to these Guidelines.
Funding
The members of the Task Force received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.