
Abstract
Objectives
This study aimed to compare three different fixation techniques for tibial tuberosity transposition (TTT) in cats in a non-cyclic load-to-failure model. The objective was to determine whether there was a significant difference between the maximum load at failure (MLF) and stiffness between a two-pin tension band wire construct (2PTBW), a two-pin construct with a maintained distal cortical attachment (2PDA) and a two-pin construct (2P), and to report the modes of failure of each group.
Methods
Tibiae from cat cadavers (n = 40) were allocated to one of four groups: 2PTBW, 2PDA, 2P and control (no surgery). The respective technique was performed on each tibia with a vertical alignment of the pins. Biomechanical testing was performed in a non-cyclic load-to-failure model; MLF, stiffness and mode of failure were recorded. Statistical analyses included one-way ANOVA and pairwise comparisons.
Results
The 2P group had a significantly lower MLF than the 2PTBW, 2PDA and control groups (P <0.05) and a significantly lower stiffness than the 2PDA and control groups (P <0.05). There was no significant difference between 2PTBW and 2PDA. The most common mode of failure in the 2PTBW group was vertical tearing of the tibial tuberosity, while in the 2PDA group, the distal cortical attachment fractured and the pins subsequently pulled out. The 2P group most commonly failed because of pin pull-out.
Conclusions and relevance
The 2PDA technique demonstrated similar strength to the 2PTBW technique in a load-to-failure model. The 2P technique was the weakest of the three. This study provides a foundation for further clinical research.
Plain language summary
In cats, when the kneecap moves out of place, it can be treated by moving the attachment of the ligament between the kneecap and the shin bone. This attachment can be fixed to the shin bone using different methods. We used shin bones from cat cadavers to test which method was the strongest and how each one broke when too much force was applied. We found that using two pins with a special wire or leaving part of the bone attached gave similar strong results. Using just two pins without extra support was weaker and broke more easily. This provides a foundation for further clinical research.
Keywords
Introduction
Patellar luxation (PL) is a common cause of lameness in small animals but occurs less frequently in cats than in dogs. 1 As in dogs, medial patellar luxation is more common than lateral patellar luxation.2 –4 The pathogenesis is not fully understood, but medialisation of the tibial tuberosity, resulting in a malalignment of the quadriceps mechanism and a shallow trochlear groove, have been identified as possible causes. 5 Compared with dogs, the feline patella is proportionally larger relative to the femoral trochlear groove and some laxity is considered physiological. 4
Surgical treatment in dogs is often empirical rather than evidence based. In cats, procedures are typically adapted from dogs despite potential differences in pathogenesis. Common surgical procedures include medial or lateral imbrication, medial or lateral release, anti-rotational sutures, wedge or block recession sulcoplasty and tibial tuberosity transposition (TTT).2,4,6 Partial parasagittal patellectomy has been suggested in cases where block recession sulcoplasty is performed to address the broad patella in relation to the trochlear groove and improve the patellofemoral contact.7,8 Corrective osteotomies of the femur are typically only performed in dogs where significant deformation is present. 9 This is rarely performed in cats, leaving TTT as the main commonly performed surgery for correcting malalignment of the quadriceps mechanism.2,4,6 A retrospective study reported that the complication rate associated with TTT is much higher in cats compared with dogs. 2 The authors suggested that this could be due to different handling properties of the bone, a smaller tibial tuberosity fragment, larger forces acting on the tibial tuberosity or relatively oversized implants. 2 Different methods for fixating the tibial tuberosity in TTT include fixation with one or two pins4,10 –14 with or without a tension band wire (TBW).4,10,14 –17 However, to the authors’ knowledge, no biomechanical study has been conducted in cats to determine the maximum load at failure (MLF) of different fixation constructs, which could provide a foundation for future clinical research.
The objectives of this study were as follows: (1) to determine the MLF, stiffness and mode of failure of three different TTT methods (complete osteotomy with two pins and a TBW [2PTBW], complete osteotomy with two pins [2P] and incomplete osteotomy with two pins [2PDA]); and (2) to compare these methods in a non-cyclic testing model.
We hypothesised the following: (1) that there is no significant difference in the stiffness and the MLF between the 2PTBW and the 2PDA construct; and (2) that the 2P construct has a significantly lower stiffness and MLF than the other two constructs.
Materials and methods
Tibiae (n = 40) were obtained from 22 skeletally mature domestic shorthair cats euthanased for reasons unrelated to this study. Written consent was obtained from owners to utilise the cadavers in this study. Inclusion criteria required skeletally mature cats free from tibia, stifle joint, patellar tendon or patella pathologies on dissection or preoperative radiographs. Exclusion criteria included open growth plates, fractures, severe soft tissue trauma near the knee or osteoarthritic stifle joints. The cadavers were cooled to 4°C after euthanasia and dissected within 48 h. The fibula and all soft tissues, except the patellar tendon, were removed and the quadriceps muscle was dissected proximal to the patella. The stifle joints were inspected for pathologies before the tibiae were wrapped in saline-soaked gauze and stored at –21°C. Before surgery and biomechanical testing, they were thawed at room temperature. Orthogonal radiographs (ControlX Medical) and photographs were acquired pre- and postoperatively.
Each tibia was randomly allocated to one of four groups: 2PTBW, 2P, 2PDA or control with no surgery performed.
Surgical procedure
For the 2PTBW group (n = 10), a line indicating the osteotomy was marked medially on the tibia using a permanent marker, extending from the impression near the intermeniscal ligament to the lesser tibial tuberosity. The osteotomy was performed with an oscillating saw (Akkulan 4; B Braun). The tibial tuberosity was shifted 3 mm laterally at its widest aspect and secured using two 1 mm Kirschner wires (Sanatmetall). One pin was placed at the centre of the most prominent aspect of the tibial tuberosity, while the second was positioned 3 mm distally using a three-dimensional-printed parallel guide. The pins were angled perpendicularly to the osteotomy and slightly medially to align with the medial cortex of the tibia. The pins were advanced until their tips fully penetrated the trans cortex at the caudal aspect. A mediolateral hole for the TBW was drilled using a 1 mm pin, positioned 3 mm distal to the osteotomy’s distal end and 3 mm caudal to the cranial cortex. A 0.8 mm cerclage wire (Sanatmetall) was threaded through the hole and wrapped around the proximal pin in a figure-of-eight configuration. A loop was formed on the opposite side of the free ends, which were also twisted once. The loop and ends were then twisted alternately until at least three twists were achieved on each side and the wire was well tensioned. Once sufficient tension was achieved, the twists were bent caudally using an additional twisting motion and trimmed, leaving three twists intact. The proximal pin was bent proximally, avoiding impingement on the patellar ligament. The distal pin was bent either proximomedially or proximolaterally to engage with the wire and both pins were cut 2 mm beyond the bend.
For the 2P group (n = 10), the osteotomy and placement of the pins were performed identically to the 2PTBW group, but no TBW was applied and both pins were bent proximally.
In the 2PDA group (n = 10), the osteotomy was made along the same line as described for the 2PTBW group. However, a distal cortical attachment was left intact, measuring 20% of the previously drawn line’s length on the medial cortex and 40% on the lateral cortex, as described in a study on dogs. 18 The tibial tuberosity was carefully bent 3 mm laterally and the pins were placed in the same manner as in the other groups. After lateralisation, the integrity of the distal cortical attachment was confirmed visually and on radiographs.
Regular flushing with saline solution was performed to keep the tibia and patellar ligament moist during the procedure and to ensure adequate cooling while sawing and advancing the pins. Postoperatively, the tibiae were wrapped in saline-soaked gauze and stored at 4°C until biomechanical testing, which was conducted within 24 h. The surgical procedures are illustrated in Figure 1.
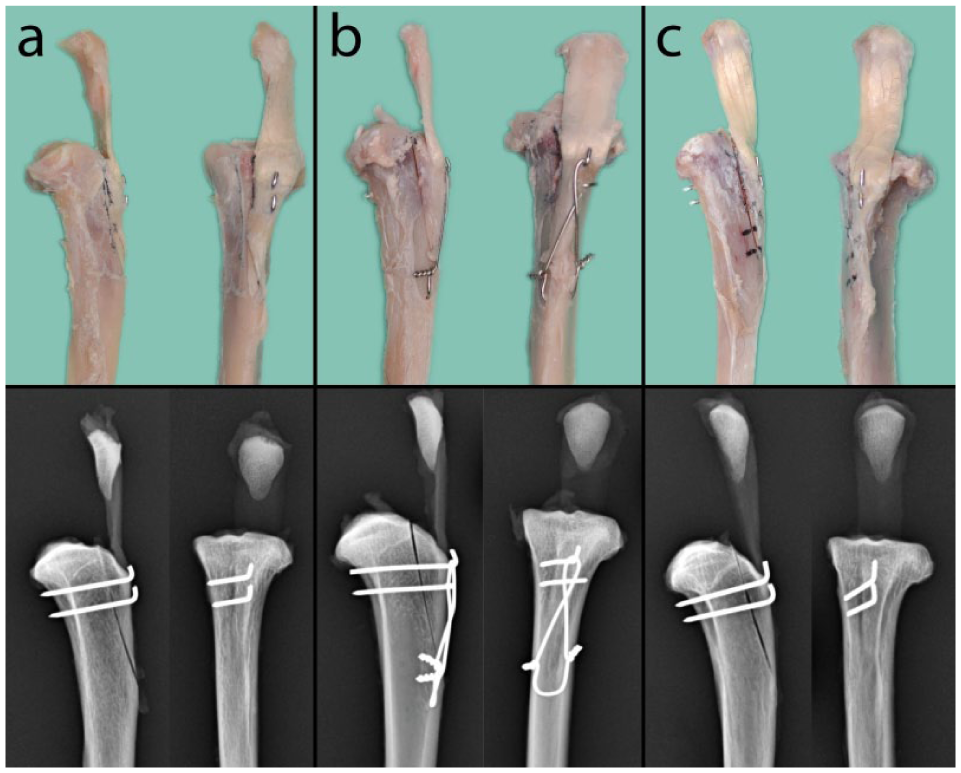
Photographs and radiographs of the three different techniques tested: (a) two-pin construct, (b) two pins with a tension band wire and (c) two pins with a preserved distal cortical attachment
Biomechanical testing
The tibiae were osteotomised distally to a length of 10 cm. Two 1.2 mm Kirschner wires were drilled orthogonally into the distal diaphysis to enhance anchorage in the potting material. The tibiae were then embedded in cylindrical plastic tubes (52 mm in diameter, 60 mm in height) using polymethyl methacrylate (PMMA), ensuring they were perpendicular to the base of the tube. The proximal aspect was wrapped in gauze soaked in sodium chloride solution throughout the process.
The tibiae were mounted in a servo-hydraulic biaxial machine (Instron) at a normal standing angle of 135°, as previously described for dogs 19 and cats 20 (Figure 2). The patella was secured in a clamp and the patellar ligament was pretensioned to 10 N. Tension was then increased at a rate of 10 N/s until the construct failed. A preliminary test was conducted using 12 specimens to assess the biomechanical setup and define a physiologically relevant loading condition. The pretension and loading rate variables were selected to mimic the testing protocols from previous studies but were adapted to the anatomical size of the cat’s patella and patellar tension from the current study.18,19,21 MLF (N), stiffness (N/mm) and mode of failure were recorded. Videos and photographs of each tibia were taken during and after testing to facilitate detailed failure mode analysis. If multiple failure modes occurred in a single specimen, the initial mode of failure was considered the primary mode of failure.

A tibia potted in polymethyl methacrylate and mounted at a 135° angle in a servo-hydraulic biaxial biomechanical testing machine. The patella was secured in a clamp
Statistical analysis
The number of specimens was determined by conducting a sample size calculation based on maximum load data published from previous biomechanical studies with similar set-ups.18,19,21 With the parameters of the effective size of 0.787, an alpha of 0.05 with a power of 0.8, the required number of samples was 10 per group.
The acquired data were tested for normal distribution using the Shapiro–Wilk test and Levene’s F test. Pearson’s correlation coefficient (r) was calculated to assess the correlation between weight and stiffness or MLF across groups. Since all data followed a normal distribution, a one-way ANOVA was conducted to evaluate differences in MLF and stiffness across the four groups. A two-sample t-test was subsequently used for pairwise comparisons of stiffness and MLF between groups. When applicable, P values were adjusted for multiple comparisons using the Bonferroni correction. A P value <0.05 was considered statistically significant in all analyses.
Statistical analysis was conducted using commercially available software (IBM SPSS Statistics and GraphPad Prism 10).
Results
All cats included in the study were skeletally mature, with a median weight of 3.85 kg (range 2.4–5.5, mean 3.73). No statistically significant correlation was found between weight and stiffness or weight and MLF in any of the four groups. Stiffness, MLF and the mode of failure are recorded in Table 1.
Stiffness, maximum load at failure (MLF) and modes of failure in each group

Data are mean ± SD (range)
In one specimen, the tibial tuberosity tore before the tibia fractured at the level of the polymethyl methacrylate
Fractures at stress risers were at the level of a pin, the transverse cerclage hole or the distal aspect of the osteotomy
Significantly different from the control group (P < 0.001) and 2PDA group (P <0.001)
Significantly different from the 2PTBW group (P =0.025), 2PDA group (P = 0.01) and control group (P <0.001). No other significant differences between groups were found
2P = complete osteotomy with two pins; 2PDA = incomplete osteotomy with two pins; 2PTBW = two pins and tension band wire
Stiffness
The stiffness of the control group (P <0.001) and the 2PDA group (P <0.001) was significantly higher than that of the 2P group. No significant differences were observed between the other groups. Stiffness results are shown in Figure 3.
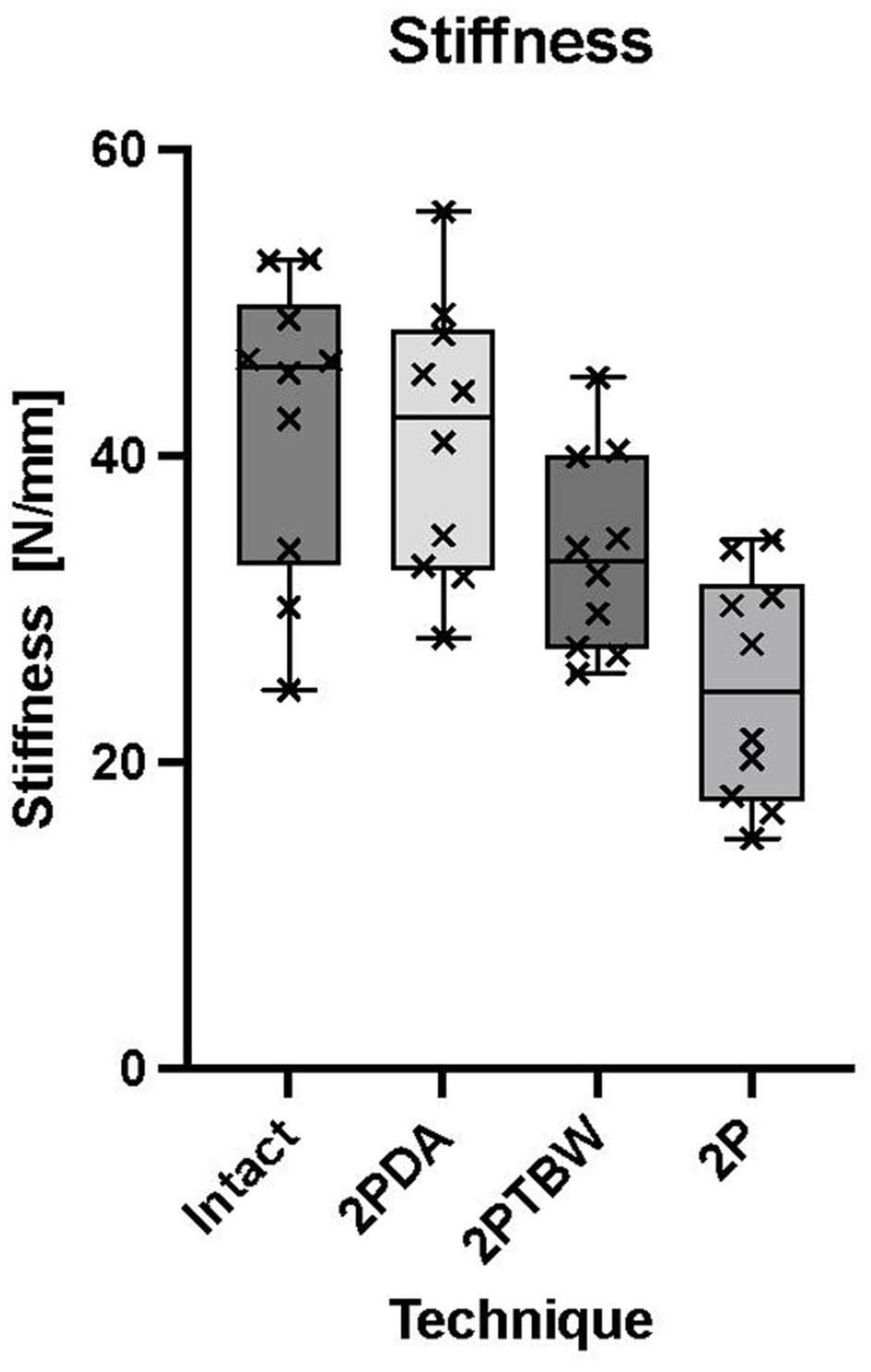
Box and whisker plots comparing the stiffness (N/mm) of intact tibiae, incomplete osteotomy with two pins (2PDA), two pins and tension band wire (2PTBW) and complete osteotomy with two pins (2P). The stiffness of the 2P group was significantly different from the 2PDA (P = 0.0005) and intact groups (P = 0.0002)
Maximum load at failure
The MLF was significantly lower in the 2P group than in the 2PTBW group (P = 0.025), the 2PDA group (P = 0.01) and the control group (P <0.001). No significant difference was found between the 2PTBW group and the 2PDA group (P = 1), between the 2PTBW group and the control group (P = 0.112) or between the 2PDA group and the control group (P = 0.233). MLF results are shown in Figure 4.

Box and whisker plots comparing the maximum load at failure (MLF) (N) of intact tibiae, incomplete osteotomy with two pins (2PDA), two pins and tension band wire (2PTBW) and complete osteotomy with two pins (2P). The MLF of the 2P group was significantly lower than that of the other three groups (P <0.05). No significant difference was found between the intact, 2PDA and 2PTBW groups (P > 0.05)
Mode of failure
The most common mode of failure in the 2PTBW group was the vertical tearing of the tibial tuberosity, while the pins remained in place (n = 4) (Figure 5). In one specimen, the tibial tuberosity tore before the tibia fractured. The tibia fractured at the level of the PMMA in two specimens, at the level of the distal pin in one specimen and at the level of the PMMA in two specimens. In one specimen, the cerclage wire untwisted and the pins were pulled out.

A vertical tear of the tibial tuberosity was a common mode of failure in the two pins and tension band wire group, with the pins and the cerclage wire remaining intact (n = 4)
In the 2PDA group, the most common mode of failure was a fracture of the distal cortical attachment with subsequent pin pull-out (n = 5). The tibia fractured at the level of the PMMA in two specimens and at the level of the distal aspect of the osteotomy in three specimens; the tuberosity fractured proximally at the level of the distal pin, while the cortical attachment remained intact, in one of these three.
In the 2P group, the most common mode of failure was a pin pull-out (n = 8), followed by tibial fracture at the level of the distal pin (n = 1) and tuberosity displacement over the pins, with the pins remaining in the tibia (n = 1).
In the control group, the most common modes of failure were fractures at the level of the PMMA (n = 4) and ruptures of the patellar ligament (n = 4). One specimen fractured just distal to the insertion of the patellar ligament and one fractured in the diaphysis, proximal to the PMMA.
The modes of failure are shown in Figure 6.
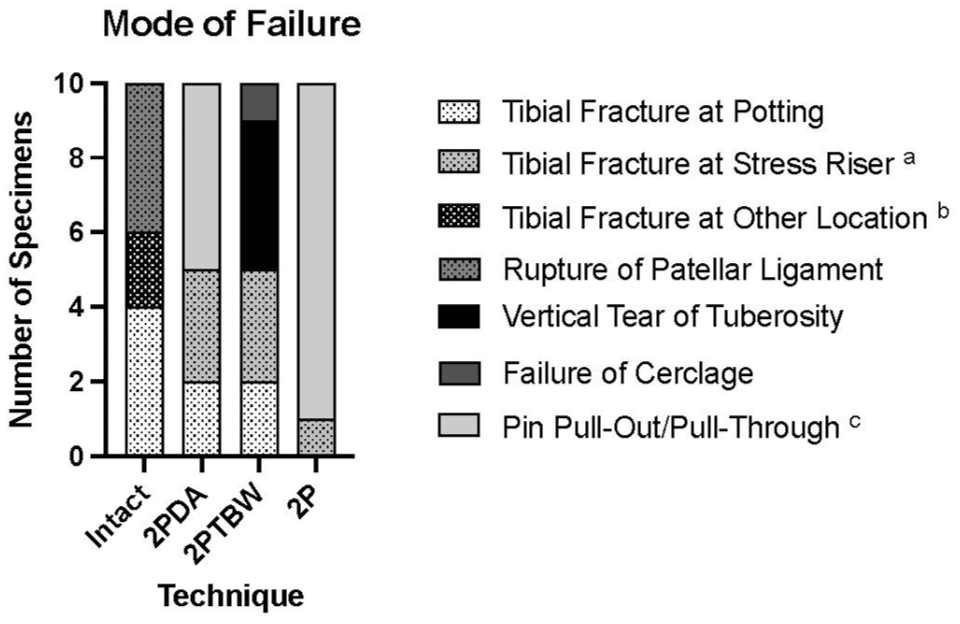
Bar chart showing the different modes of failure in the intact, complete osteotomy with two pins (2P), incomplete osteotomy with two pins (2PDA) and two pins and tension band wire (2PTBW) groups. In the 2PDA group, one specimen failed because of a tibial tuberosity fracture at the distal pin (fracture at stress riser) and tibial fracture. aStress risers included either pin holes, the transverse hole for the cerclage wire or the distal aspect of the osteotomy. bOther locations were mostly diaphyseal, except for one intact tibia, which fractured distal to the insertion of the patellar ligament. cOne specimen in the 2P group failed by pin pull-through, with the pins remaining in the tibia. All other failures classified as pin pull-out/pull-through involved pin pull-out with the pins remaining in the tibial tuberosity. In the 2PDA group, all failures classified as pin pull-out were preceded by a fracture of the distal cortical attachment, followed by pin pull-out
Discussion
This study investigated three methods for the fixation of the tibial tuberosity in TTT in cats using a non-cyclic load-to-failure model. To our knowledge, this is the first biomechanical study to evaluate different fixation methods for TTT in cats.
We were able to accept the first hypothesis, which stated that there is no significant difference in MLF and stiffness between fixation with 2PTBW and fixation with 2PDA. We also accepted the second hypothesis, which stated that fixation with 2P has the lowest MLF and stiffness among the three constructs.
Even though the 2P technique exhibited the lowest MLF, its stability in a clinical setting remains unclear. Since cats load their hindlimbs with four to five times their body weight during high jumps, 22 it is likely that significant forces are acting on the quadriceps muscle, making a more stable construct beneficial. The data suggest that the 2P technique is more likely to clinically fail as it is the weakest construct and might be least capable of counteracting the forces from the quadriceps muscle. Clinical data in dogs suggest a higher rate of tibial tuberosity avulsion if a single K-wire was used compared with 2PTBW. 14 Further research, such as clinical trials in cats, is needed to confirm this hypothesis.
Although no significant difference in MLF was observed between the 2PTBW and 2PDA groups, the 2PTBW group showed some unique characteristics in failure mode.
Only one cerclage wire untwisted in the 2PTBW group, which is consistent with other biomechanical studies on dogs.18,21 However, this contrasts with the study by Natsios et al, 19 where most of the TBWs failed because of wire breakage, likely due to the use of a 0.6 mm wire, compared with the 0.8 mm wire used in our study. Four specimens failed because of vertical tearing of the tuberosity while the pins and TBW remained intact, which has not been previously described in biomechanical studies in dogs.15,18,19,21 A possible explanation could be the relatively smaller tibial tuberosity and different bone properties in cats as well as the vertical alignment of the pins. Although Zide et al 21 reported no difference between vertical or horizontal alignment of the pins in dogs, horizontally aligned pins could potentially provide more resistance against a vertical tear but might also increase the likelihood of a tibial tuberosity fracture, which we observed in only one specimen in the 2PDA group, in combination with a tibial fracture. Further investigation is warranted to understand the implications of construct design and pin orientation on failure modes in feline TTT.
In a retrospective study of dogs, the only factor associated with a decreased risk of complications was maintaining a distal cortical attachment. 16 One reason for this could be that healing may be improved by preserving some blood supply to the tibial tuberosity through the intact periosteum and cortical bridge. A study of tibial tuberosity advancement (TTA) in dogs using the modified Maquet technique reported faster healing of the osteotomy 23 compared with the traditional TTA technique with a complete osteotomy. 24 However, clinical studies are necessary to investigate this factor in TTT cases. Nevertheless, it should be noted that a distal cortical and periosteal bridge is typically maintained in clinical cases regardless of whether a TBW is applied. However, in our study a complete osteotomy in the 2PTBW group was performed to ensure consistency with previous biomechanical studies in dogs18,21 and to allow for a clear assessment of the stabilising effect provided by the TBW. Further studies are warranted to evaluate whether a combination of a maintained distal attachment and a TBW is biomechanically superior to one technique or the other.
The 2PDA technique carries a risk of intraoperative fracture of the distal cortical attachment, ultimately resulting in a biomechanically inferior 2P construct. Therefore, a TBW should be considered if a fracture of the distal attachment is detected during surgery or on radiographs. The risk may be reduced by using a dedicated device, as described by Sullivan et al, 18 which allows for slower, more consistent and precise bending. However, this device was not used in our study because it is not readily available in most institutions and is therefore rarely used.
In contrast to similar studies on dogs,18,19,21 more tibial fractures were observed in all groups except for the 2P group. In a study of small dogs, 19 the mean body weight and the MLF were higher than those of the cats in our study when comparing similar techniques. This suggests that the higher incidence of fractures is likely attributable to the smaller size of the tibiae while having a construct of similar strength. Differences in the mechanical properties and anatomy of the feline tibia could play an additional role. Fractures near stress risers, such as pin or cerclage holes, may also result from relatively oversized implants. A retrospective study in cats suggested this as a possible reason for the higher complication rate of TTT in cats compared with dogs. 2 Among all groups, 9/17 fractures occurred at the level where the potting engaged the tibia, which likely resulted from the lever arm of the tibia and the high stress concentration in that area. The dissection of the fibula likely reduced the overall load stability and increased the chance of a fracture before the construct could fail.
This study has several limitations and the results should be interpreted with caution. An ex vivo cadaver study does not accurately reflect physiological conditions, which means this study provides only limited insight into the behaviour of the different techniques in vivo. Similarly, a non-cyclic load-to-failure model does not simulate the physiological load over an extended period. As a result, factors such as material fatigue and healing were not considered, and potential complications may only arise after some time. The 135° standing angle was adopted from studies on dogs 19 and cats. 20 However, this angle may not accurately represent the physiological loading conditions when walking or jumping. The relatively small sample size may obscure significant differences between groups. Therefore, the clinical application of these results should be approached with caution.
Conclusions
This study demonstrated that the 2PDA technique in cats is as equally strong as the 2PTBW technique in a load-to-failure model. The 2P technique was found to be the weakest of the three techniques. Given the limited research on the pathophysiology and treatment of patellar luxation in cats, further studies are necessary to improve clinical outcomes. In particular, clinical trials are needed to evaluate these techniques under physiological conditions over longer periods to consider factors such as material fatigue, pin migration and healing. This study provides a potential foundation for such future clinical research.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.