
Abstract
Objectives
The purpose of this retrospective, descriptive study was to assess CT findings and short-term outcome of cats with pyothorax presented to a referral hospital.
Methods
Thoracic CT studies of 41 cats with pyothorax comprising pre-contrast lung and soft tissue reconstructions and post-contrast soft tissue reconstructions were blindly reviewed by two European College of Veterinary Diagnostic Imaging (ECVDI) board-certified radiologists and a third-year ECVDI resident, referencing a predetermined list of imaging features. Clinical outcomes, including treatment options, survival to discharge and length of hospitalisation, were recorded.
Results
All cats (100%) had pleural effusion. Common imaging findings included intrathoracic lymphadenomegaly (85%), pleural thickening (85%), presence of pannus (81%) and evidence of pneumonia (49%). Pulmonary abscessation was suspected in 22% of cats and foreign bodies in 12%. Of the 41 cats, 20 were managed medically, 20 underwent surgery and one had unsuccessful medical treatment followed by surgical intervention. The median duration of hospitalisation was 7 days, and 36 cats survived to discharge.
Conclusions and relevance
This study demonstrates that cats with pyothorax commonly have marked changes on CT that involve multiple thoracic compartments. Our study population highlights that feline pyothorax can have a good short-term outcome when managed either medically or surgically.
Introduction
Feline pyothorax is a complex and potentially life-threatening condition characterised by the accumulation of purulent fluid within the pleural cavity.1 –3 Despite advancements in veterinary medicine, pyothorax remains a therapeutic challenge that may require a multidisciplinary approach for successful management.
Pyothorax most commonly affects young to middle-aged cats (mean age 4–6 years); no breed or sex predisposition has been identified.2,4 Presenting clinical signs include lethargy, inappetence, dyspnoea and pyrexia.1,2
The aetiology in cats is often unknown.1,2 Direct inoculation from penetrating wounds, such as bites, haematogenous or lymphatic spread from a systemic infection and extension from infection of adjacent structures, such as the lungs, have all been suggested as possible causes.2,5 –7 Foreign bodies are not commonly found in cats, contrary to dogs, although occasional cases have been reported.2,8,9
The diagnosis of pyothorax is achieved by analysing pleural fluid, which is generally proteinaceous with a high percentage of neutrophils.5,8 Various types of bacteria may be found. Compared with dogs, cats tend to have higher fluid cell counts and intracellular bacteria are more commonly found. 8
The choice of optimal treatment protocol for this condition remains controversial.4,6,7 Medical treatment is often utilised in the first instance. Surgical management may be recommended in the presence of focal mediastinal or pulmonary lesions detected on diagnostic imaging or when medical therapy fails. 7 In humans, CT is used to characterise pleural effusion, 10 and a CT scoring system has been created to guide management and prognosis in cases of pyothorax.10,11 Compared with radiography, CT can provide more detailed and accurate information regarding the extent and nature of the thoracic pathology. 12 A recent paper describes the CT findings of pyothorax in dogs. 13 However, to the authors’ knowledge, there are no publications describing the features of feline pyothorax on CT.
The aim of this study was to describe the CT findings in a population of cats presented with pyothorax. A secondary aim was to evaluate the short-term outcome of these cats.
Materials and methods
This was a retrospective, descriptive study. Ethical approval was granted by the institution’s ethical review committee (Animal Welfare and Ethical Review Body, reference VIN 22-054).
Our electronic medical records database (RxWorks; Covetrus) was searched for feline patients with a confirmed diagnosis of pyothorax between January 2012 and July 2023. Patients were included if they were treated at our institution and had a thoracic CT at their initial presentation. The diagnosis of pyothorax was considered confirmed by the presence of intracellular bacteria on cytology or a positive bacterial culture from the pleural effusion.
All imaging studies were acquired using the same CT scanner (Somatom Emotion 16; Siemens Healthineers) with the following helical acquisition parameters: kV 130, reference mAs 50, slice thickness 1.5 mm, pitch 0.8 and rotation time 0.6 s. Non-ionic iodinated contrast medium iohexol (Omnipaque; HE HealthCare) was administered intravenously at a standard dose of 600 mg I/kg at a rate in the range of 1.5-3 ml/s. Pre-contrast studies were reconstructed in lung algorithms (WL −500, WW 1500, slice thickness 1.5 mm). Pre- and post-contrast studies were reconstructed in soft tissue algorithms (WL 40, WW 400 and slice thickness 1.5 mm).
The CT studies were anonymised and reviewed by a third year (European College of Veterinary Diagnostic Imaging) ECVDI resident (IR) and two ECVDI board-certified radiologists (AM and EP) using an open-source dedicated DICOM viewing software (Horos, horosproject.org). The reviewers were aware of the diagnosis of pyothorax but blinded to all other clinical information. The CT images were evaluated for the following criteria previously agreed by the reviewers: (1) focal, multifocal or diffuse lesion distribution; (2) uni- or bilateral pleural effusion; (3) pleural effusion attenuation in Hounsfield units (HU); (4) presence and severity of pannus; (5) presence and distribution of pleural thickening (without distinction between parietal and visceral layers); (6) presence of CT findings consistent with pneumonia and the lobes affected; (7) presence of CT findings consistent with pulmonary abscessation and the lobes affected; (8) presence of mediastinal effusion, abscessation and/or gas; (9) sternal, cranial mediastinal and tracheobronchial lymphadenomegaly; (10) suspicion of foreign body and its location; (11) presence of pneumothorax; and (12) presence of thoracic drains. For the assessment of the pleural effusion attenuation, three circular regions of interest (ROIs) were placed over a collection of pleural effusions on the pre-contrast soft tissue reconstructed images, avoiding regions of pannus (Figure 1). The values for minimum, maximum and mean HU were collected for each ROI, and a mean of the three measurements was calculated. Pannus was defined as irregular soft tissue-attenuating bands that demonstrated contrast enhancement within the pleural cavity but had minimal contact with the pleural surface, helping to differentiate it from pleural thickening (Figure 2a,c). Increased parenchymal attenuation, with or without air bronchograms and in the absence of lung volume reduction, was required to support a diagnosis of pneumonia (Figure 2b). Fluid-attenuating lesions, with or without intralesional gas and surrounded by a soft tissue-attenuating, contrast-enhancing capsule, were considered suggestive of abscessation (Figure 2d).

(a) Pre-contrast soft tissue CT image demonstrating the technique used to measure the CT attenuation of pleural effusion with three regions of interest (green circles) in the pre-contrast soft tissue window. (b) The comparable post-contrast image confirms the absence of pannus or other soft tissue structures in the selected regions
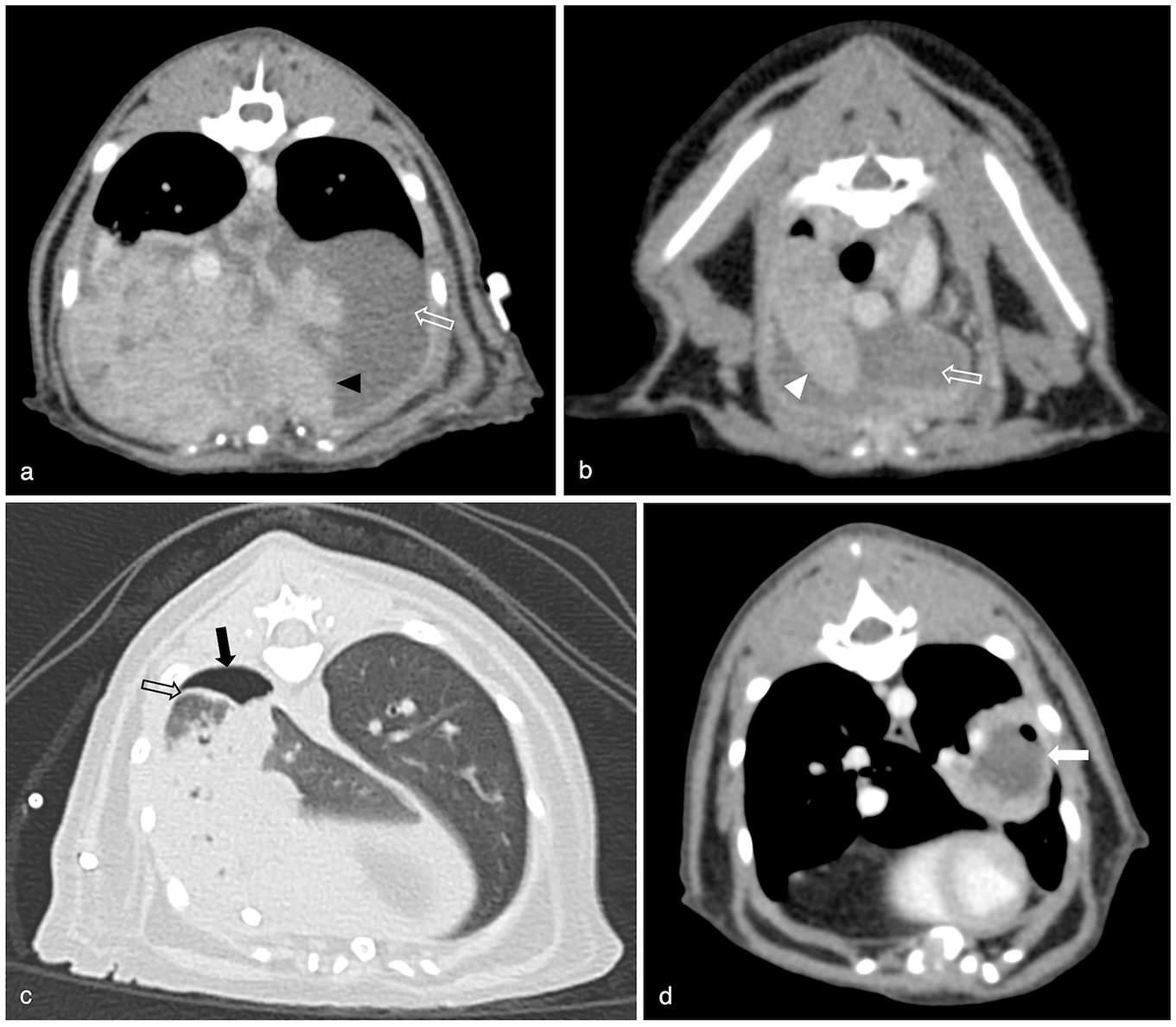
Examples of CT findings in our population: (a) irregular soft tissue-attenuating, contrast-enhancing bands within the pleural space consistent with marked pannus formation (black arrowhead); (b) pneumonia characterised by increased pulmonary parenchymal attenuation and maintained lung volume (white arrowhead); (c) thickening of the visceral pleura (black hollow arrow), best visualised in the lung window and in this instance highlighted by adjacent pneumothorax; (d) abscess formation with intralesional gas (white arrow) in the left caudal lung lobe. Pneumothorax (black arrow) and pleural effusion (white hollow arrow) can be seen in multiple images
Patient signalment, including breed, age, sex and neuter status, was recorded. Details of treatment records (medical or surgical), surgical findings (if applicable) and short-term outcome were collected by the first author (IR) and reviewed in collaboration with a European College of Veterinary Emergency and Critical Care board-certified specialist in emergency and critical care (HW) and a European College of Veterinary Surgeons board-certified surgeon (MP). Medical treatment consisted of administration of antibiotic medication with or without concurrent placement of thoracic drains for aspiration of the pleural space and/or lavage. Surgical treatment consisted of median sternotomy for lavage and/or lung lobectomy and/or mediastinectomy and/or pericardiectomy, in addition to the aforementioned medical therapies.
Recorded short-term outcomes were survival to discharge and length of hospitalisation in days. There was no consistent follow-up after discharge from hospital; therefore, long-term outcomes, such as incidence of recurrence, could not be assessed.
Results
Signalment
A total of 41 cats met the inclusion criteria. Breeds included domestic shorthair (n = 24, 58.6%), Maine Coon (n = 8, 19.5%), Ragdoll (n = 2, 4.9%) and one each (2.4%) of Oriental, Burmese, Siamese, Havana Brown, Ocicat, Burmilla and crossbreed. There were 14 female cats (one entire and 13 neutered) and 27 male cats (two entire and 25 neutered). The median age was 4 years (range 7 months to 14 years).
CT findings
All CT findings are shown in Table 1.
Summary of the CT findings

Data are n (%)
Pleural effusion was present in all the cats included in the study, unilaterally in five and bilaterally in the remaining 36. Pleural thickening was identified in 35/41 (85.4%) cats. Pannus formation was detected in 33/41 (80.5%) patients.
Thoracic lymphadenomegaly was identified in 35/41 (85.4%) cats, with involvement of multiple lymph node centres in 24/35 (68.6%). The sternal lymph node group was the most commonly affected, being enlarged in 33/41 (80.5%) cats. Tracheobronchial and cranial mediastinal lymphadenomegaly was present in 20 (48.8%) and 17 (41.5%) cats, respectively.
Pneumonia was suspected in 20/41 (48.8%) cats, involving multiple lung lobes in the same patient in 11/20 (55.0%). The most commonly affected lung lobe was the left cranial (9/20), while the accessory lobe was the least affected (1/20). In total, 10 pulmonary abscesses were identified in nine of the cats, with the caudal lung lobes more commonly affected (7/10).
A foreign body was suspected in 5/41 (12.2%) cats, four within the lung parenchyma (involving left or right caudal lung lobes) and one within the pleural space. Of these five cats, two had unilateral pleural effusion.
Pneumothorax was present in 30/41 (73.1%) patients and the volume ranged from very small to moderate. Information pertaining to previous drain placement or thoracocentesis had not consistently been recorded. However, all cats with chest drains in place at the time of CT (24/42, 58.5%) also had pneumothorax.
The pleural effusion HU was assessed in all patients, and the mean of the measurements was 12.52 (range −12.45 to 37.16).
Clinical information and short-term outcome
A total of 20 cats had medical treatment only and 20 underwent surgical intervention only. One cat initially had medical management for 5 days; however, because of recurrent thoracic drain occlusion and lack of improvement, it underwent surgical treatment. This cat is included in the surgical treatment group for the purposes of outcome assessment.
Of the five cats with suspected foreign bodies on CT review, three had undergone surgical treatment. Histopathology confirmed a foreign body within a bronchus of the resected right caudal lung lobe of one of these cases, as initially suspected during image review (Figure 3). No foreign body was detected in the remaining two. In addition, one foreign body located in the pleural space was identified during surgery in a cat where retrospective CT review had not revealed it. Plant material was confirmed as a foreign body in 2/41 (4.9%) cats in the study and in 2/21 (9.5%) of those surgically treated. Both affected cats had unilateral effusion on CT.

(a) Dorsal and (b) transverse CT images in soft tissue reconstruction pre-contrast. Small linear mineral attenuating foreign body (white hollow arrow) detected in the right caudal lung lobe during the CT review. The patient underwent surgery for right caudal lung lobectomy. On histopathology, a foreign body (confirmed to be plant material) was found within a bronchus of the excised lung lobe
The overall survival to discharge was 87.8% (n = 36/41), and the proportion of survivors was not significantly different between cats treated surgically (19/21, 90.5%) and cats treated medically (17/20, 85%). Of the cats that did not survive to discharge, one had a cardiac arrest due to septic shock and the other four were euthanased because of clinical deterioration (n = 2), persistent hypotension (n = 1) and development of congestive heart failure (n = 1).
The median length of hospitalisation for the whole population was 7 days (range 4–16). There was a comparable median but with slight variation in range between the surgically and the medically treated cats: 7 days (range 5–12) and 7 days (range 4–16 days), respectively.
Discussion
Some studies report unilateral effusion in feline pyothorax cases14,15; however, bilateral effusion is more common.8,14,16 One recent study found no statistical difference in the presence of unilateral vs bilateral distribution of inflammatory vs neoplastic effusion. 17 In our study, pleural effusion was present in all cats, with a minority (n = 5/41) having a unilateral distribution. We suggest the more common bilateral effusion in our population could result from a high prevalence of systemic or parapneumonic spread of disease. Conversely, unilateral effusion may be more likely to occur secondarily to a localised infection source, such as a foreign body or focal pneumonia. Another possible explanation is that, in a referral patient population, enough time could pass between onset of infection and presentation of the cats to the referral hospital to allow the pleural infection to spread into both hemithoraxes in the majority of the patients.
Assessment of pleural effusion attenuation has been suggested as a means of distinguishing between effusion types. In human medicine, studies have shown that although there is overlap among most effusion types, exudates should be considered when CT attenuation values exceed 15 HU. 18 This approach has also been studied in dogs, where CT attenuation was found to help differentiate exudates from transudates, 19 with a threshold of above 14 HU suggested for exudates, modified transudates and haemorrhage. 20 The mean HU value found in our study (12.52 HU) falls below this threshold. However, the use of pleural effusion attenuation to distinguish effusion types in feline patients has not been validated. In fact, when this was attempted, no significant variation in HU values was found between different effusion types. 20
Additional findings, such as pleural thickening, may be used to further assist in the distinction of exudates from other types of pleural effusions. Several studies have tried to assert this, both in human 18 and veterinary medicine. 21 Çullu et al 18 reported that human patients with pyothorax had significantly more pleural thickening than patients with other types of effusions. A study in dogs and cats 21 suggested that visceral pleural thickening is more common in pyothorax and chylothorax when compared with malignant pleural disease. The high percentage of cats with pleural thickening in our population supports its role as a characteristic feature of pyothorax. Before data collection, we had established that distinguishing between visceral and parietal pleural thickening was challenging, with low agreement between the three CT reviewers. As a result, this was not recorded as a specific data point. We also believe that, in practice, this distinction is unlikely to be a useful feature when differentiating effusion types.
Although Reetz et al 21 also found that sternal lymphadenomegaly was more common in non-transudative effusions, overall, descriptions of lymphadenomegaly in cats and dogs with pyothorax are lacking in the veterinary literature. The sternal lymph nodes play an important role in draining the thoracic wall 22 and pleura, 23 which likely explains why sternal lymphadenomegaly was commonly identified in our population. The cranial mediastinal and tracheobronchial lymph nodes are more actively involved in the lymphatic drainage of the mediastinal structures and lungs, respectively. 22 In some individuals, the cranial mediastinal lymph nodes also receive afferent lymphatic vessels from the sternal nodes. Given the multifocal and widespread thoracic abnormalities observed in our study population, it is therefore not unexpected that cranial mediastinal and tracheobronchial lymphadenomegaly were frequently found. In the absence of cytological or histopathological evaluation in most cases, the lymphadenomegaly was presumed to be reactive in nature, secondary to thoracic pathology.
Parapneumonic spread is thought to be a common cause of pyothorax in cats.3,4,8,14 The physiopathology of this is explained by the extension of the inflammatory process from the pulmonary parenchyma to the visceral pleura and consequent increase of the capillary microvascular permeability. That, in turn, facilitates the movement of fluid and inflammatory cells into, but not out of, the pleural space as intrapleural pressure is lower than interstitial pressure. 24 Previous studies have reported the presence of pneumonia on thoracic radiographs in 53% of cats with pyothorax. 14 Our population had a similar prevalence of CT features consistent with pneumonia, which supports the previous thesis. Interestingly, the prevalence of pneumonia in this study is significantly higher than the 6.9% reported in a recent study of canine patients, 13 suggesting there may be notable differences in the aetiology of this condition between the two species. As an additional consideration, rounded atelectasis has been described in patients (both dogs and cats) with nodular pulmonary lesions and pyothorax. 25 Although we did not assess for this as a specific criteria in our study population, and we cannot completely rule out that rounded atelectasis was misrepresented as pneumonia in any instance, our requirement for maintained or increased parenchymal volume to assign regions as affected by pneumonia leads us to believe that our results are unlikely to be significantly skewed by this.
Another apparent contrast between species is the prevalence of foreign bodies as the cause of pyothorax, which is currently believed to be more common in dogs than in cats. 8 A recent study of 101 dogs 13 identified a foreign body during surgery in 20.8% of cases, which is higher than the 9.5% observed in our study. CT is considered more accurate than radiography for detecting thoracic foreign bodies and/or their migration tract, and it is widely used for this purpose in both human and veterinary medicine.2,13,26 However, factors such as the foreign body’s composition, size, location, surrounding inflammation, migration or degradation can make detection challenging. 13 In a study by Eiras-Diaz, 13 only 46.6% of dogs with a confirmed foreign body had any suspicion of one on CT images. In our study, CT review of one of the two surgically confirmed foreign bodies did not raise suspicion in any of the three reviewers. Therefore, our findings agree with previous literature in dogs, which suggests that CT alone may have limited value in definitively diagnosing or excluding the presence of intrathoracic foreign bodies. 27 Similarly, it is possible that foreign material may be missed even during surgery. As such, the prevalence of foreign bodies recorded in our study population may be underestimated. Another confounding factor is that our study did not assess long-term outcome. In four cats, retrospective CT review raised the suspicion of a foreign body that was not confirmed. It is possible that these, and potentially other patients, could have experienced disease recurrence due to undetected foreign material.
CT is a highly effective modality for diagnosing pneumothorax, 13 and in a large portion of the cats in our population, at least a small volume of pleural gas was detected. The authors primarily attribute this finding to thoracocentesis and thoracic drain placement procedures carried out before CT. However, intrathoracic pathology, such as gas-producing bacteria or lung damage due to pneumonia or foreign bodies, could also partially explain these results.
The prognosis for feline pyothorax in the literature is highly variable, with mortality rates in the range of 7–38%.3,14,28 The lack of consensus on the standard therapy and multiple potential underlying aetiologies confounds the survival data in cats with pyothorax. Our study suggests good survival to discharge rates for both medically and surgically treated cats. There are currently no studies analysing the connection between the clinical presentation, imaging studies, pleural fluid analysis and treatment options (medical vs surgical) with the short- and long-term survival of these patients.3,4 Unfortunately, at this stage our data are not able to contribute significant new information to this analysis, but this study forms a starting point for our group to continue to investigate this.
The present study has some limitations, mainly because of its retrospective design. There was no standardised clinical approach to the management of pyothorax, and variability in the timing of CT acquisition after hospital admission may have influenced certain findings, including – but not limited to – the severity of pleural pannus and the distribution of pleural effusion. The CT review criteria agreed were largely subjective, mimicking clinical conditions; however, this limits the accuracy of the findings. Histopathological confirmation of lesions such as pneumonia and abscessation was not obtained, as it was not recommended during the patients’ hospitalisation. In addition, the authors acknowledge that there is limited correlation between the retrospective CT review and the clinical decision-making that occurred at the time of presentation. As such, it was not considered appropriate to attempt to correlate the CT findings identified with treatment choices. In a condition with varying guidance regarding optimal management, interdisciplinary discussions within a multidisciplinary hospital setting have a substantial influence in guiding treatment decisions. Without access to the content of these clinical discussions, an important piece of context is missing. This highlights the opportunity for future studies involving internal medicine, critical care and surgical teams to discuss treatment decision-making criteria and the role of CT in guiding this decision.
Conclusions
Our study described the CT findings and short-term outcome in a population of cats with pyothorax. The most common CT findings include bilateral pleural effusion, intrathoracic lymphadenomegaly, pleural thickening and pannus formation. Pneumonia was observed in a large proportion of the cats and foreign bodies were uncommon. There was a high survival to discharge rate in both the medically and surgically treated patients, with a comparable length of hospitalisation. The study also indicates that pyothorax behaves differently in feline and canine patients.
Footnotes
Acknowledgements
The authors are grateful to Dr Natalie Finch for the valuable contributions during the initial steps of this research project.
Author note
The abstract of this paper was presented in part at the 2024 EVDI Congress.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.