
Abstract
Practical relevance:
Physical rehabilitation (physiotherapy) involves restoring a patient’s movement and function following an injury, illness or trauma. It can be used for acute and chronic conditions and, in some cases, the techniques are used as a preventive treatment. Some therapies can also provide pain relief, which can be especially helpful when analgesic drugs are contraindicated in a patient. In recent years, there has been increasing interest in the application of physiotherapy to small animals, and while physical rehabilitation has traditionally been used more commonly for canine than feline patients, as cats can benefit just as much as dogs, this trend is changing. A multidisciplinary team is involved and identifying when a cat is painful and prioritizing therapies accordingly is crucial.
Clinical challenges:
Cats are typically not accustomed to regular handling or restraint and tend to become uninterested and frustrated quickly, which means they are often perceived as poor candidates for physiotherapy referral. As well as a cat’s temperament, there are physical factors that may limit or exclude particular therapies; for instance, a cat’s level of cardiovascular health. There can also be much variation with the success of different therapies - what works well in one individual might have no effect in another.
Aims:
This article, the first in a two-part series, discusses the most common painful conditions in cats that can benefit from physical rehabilitation, as well as the importance of prioritizing the type of therapy depending on the individual patient. Part 2 discusses individual therapies and exercises for physical rehabilitation.
Keywords
Introduction
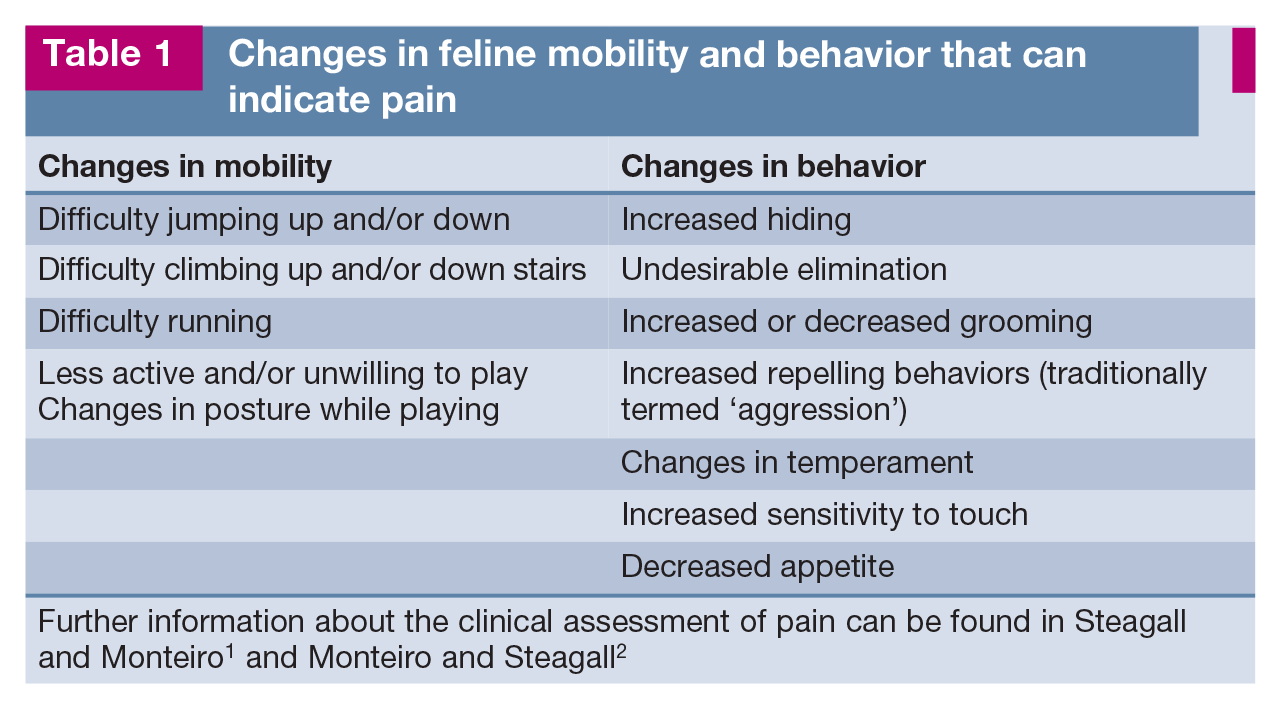
Feline physical rehabilitation (physiotherapy) involves the diagnosis and management of patients with painful (Table 1) or functionally limiting conditions. The goal is treatment of injury or illness to decrease pain and restore function. The objective is achieving the highest level of function, mobility, independence and quality of life for the patient.
Changes in feline mobility and behavior that can indicate pain
Feline physical rehabilitation is a growing area of interest. Many cat caregivers are becoming aware of the benefits that rehabilitation can have for their pet, whether that be through post-injury rehabilitation or for the management of long-term conditions (eg, osteoarthritis [OA]). 4 Implementation requires an excellent understanding of feline behavior, accurate assessment of the cat’s condition and the correct usage of a range of physiotherapeutic modalities. Cats often respond well to rehabilitation techniques and make willing patients, typically enjoying stretching, massage and the mental stimulation of therapeutic exercise in the hospital and at home. 5 ‘Thinking cat’ is important, however, when planning sessions (eg, keeping them short and interesting, and performing them in a quiet, relaxed environment) in order to increase the chances of success.

Conditions benefiting from physiotherapy
Most commonly, cats are referred for physiotherapy for the management of OA, 6 fractures, neurologic conditions, obesity or following articular surgery, such as femoral head and neck excision (FHNE). As stated by Harasen, cats have several advantages over dogs when it comes to physiotherapy, including their light body weight, low rate of angular deformities and relative lack of genetic developmental disease. 7
Osteoarthritis
OA is a common and complex progressive disease. Clinically it is defined as ‘a slowly evolving articular disease characterized by the gradual development of joint pain, stiffness and the limitation of motion’. 7 Pathologically it has been defined as ‘an inherently non-inflammatory disorder of moveable (synovial) joints characterized by deterioration of articular cartilage and by the formation of new bone at the joint surfaces and margins’. 8 The term degenerative joint disease (DJD) 8 is often, incorrectly, used synonymously with the term ‘OA’, when, in fact, ‘DJD’ is an all-encompassing term that includes all types of degenerative pathology in any type of joint. For example, DJD includes OA but also spondylosis deformans of the intervertebral disc (non-synovial) joints, isolated degenerative lesions such as enthesophytes (abnormal bony projections at the attachment of a tendon or ligament), degenerative soft tissue mineralization of structures within joints that might not be part of OA (eg, of menisci, ligaments) and traumatic arthritis. While physical rehabilitation is more commonly used for OA, it is also used for non-OA forms of DJD.
In a study of cats over 6 years of age, 61% had OA in at least one joint and 48% had more than one joint affected. Of the cats that were over 14 years of age, 82% had OA in at least one joint. 9 A study by Lascelles et al of a randomly selected sample of 100 cats aged up to 20 years old found that almost all (92%) had radiographic evidence of DJD and 91% had at least one site of appendicular DJD. 10
Primary OA refers to degenerative changes to the cartilage and joint that occur without a known cause. Secondary OA occurs when pre-existing conditions or factors lead to the breakdown of cartilage in a joint. Examples of secondary OA include cases that develop following joint surgery, trauma or repetitive joint injury such as hip dysplasia. Confirming or ruling out the occurrence of joint trauma during the lifetime of an individual animal is very difficult, however. Many cases of joint trauma may go unnoticed by caregivers, and repetitive low-grade trauma over a period of time may be the important factor. Risk factor analysis in a feline study demonstrated that obesity, outdoor access and a history of trauma may predispose cats to developing caregiver-reported mobility changes associated with DJD. 11
Clinically, patients develop hyperalgesia (ie, a greater than typical level of pain from a stimulus that normally provokes pain) and allodynia (ie, pain caused by a stimulus that does not normally provoke pain). 12 For cats, pain and loss of function are the main clinical signs (eg, decreased activity, decreased ability to perform routine behaviors and decreased socialization; see Table 1). Recognition relies mostly on care-giver-reported changes in behaviors (expression of new behaviors and disappearance of old behaviors) and a screening checklist of behaviors performed at home is available to help identify cats with DJD. 13 During orthopedic examination, cats with DJD are more likely to show behaviors such as resistance, biting, scratching, hissing and vocalizing. 14


A male castrated domestic longhair cat with osteoarthritic pain stretching over a physioroll ball. Courtesy of Robin Downing

A geriatric spayed female domestic shorthair cat that is ready for photobiomodulation (therapeutic laser therapy) of pain. Providing googles for protection from the therapeutic laser is advised for companion animal patients that receive photobiomodulation, as shown here. Courtesy of Robin Downing

A cat receiving electroacupuncture for osteoarthritic pain. Courtesy of Sheilah Robertson

A cat undergoing acupuncture. Courtesy of Robin Downing
Geriatric cats, especially those with DJD, often present to the rehabilitation veterinarian because of difficulties performing the activities of daily living; for example, going up or down stairs or jumping up to a favorite resting/sleeping area. The goal of the examination and treatment plan is to therefore explore possible therapeutic options that will effectively improve strength, balance and comfort without fatiguing the patient nor worsening any mobility issues at home. Slow, steady progress is the aim of any geriatric rehabilitation plan. The plan must include environmental modifications for the home and nursing care regardless of the relative stability or functionality of the patient. 18
According to Laurie McCauley, it is an ‘absolute precaution that the patient (canine or feline) should feel better, move better, and have better normal daily function when finished with the day’s physiotherapy. If they are lamer, sore after resting, or change transitions or posture for the worse after exercises are done, then the plan needs to change.’ 19 The treatment protocol should therefore consequently be amended to reduce intensity or remove any specific exercises that are triggering clinical regression.
Fractures
The major cause of feline orthopedic injury is vehicular trauma. Other etiologies include falls from a height, animal fights and gunshot wounds. 20 Multiple orthopedic injuries are not uncommon, and there are frequently injuries to multiple body systems.
Assessment of pain is best made subjectively, by a trained observer, based on observation and interaction. Cats in pain typically become inactive, sit at the back of their cage and avoid human interaction. They tend to resent or avoid handling, and may display repelling behaviors. Occasionally a cat will thrash around the cage violently; this reaction is seen more commonly in young animals. 20
Analgesic drugs should be administered to increase comfort and reduce stress in all cats with fractures. The cat’s cardiovascular status should be carefully monitored when analgesics are used. Balanced (multimodal) analgesia is always recommended; this involves the simultaneous administration of two or more analgesic techniques to achieve a synergistic effect, reduce drug dosages and minimize complications. There are many drugs available that can be administered to provide multimodal analgesia in cats, including opioid drugs, α2-adrenergic agonist drugs and non-steroidal anti-inflammatory drugs (NSAIDs), along with local anesthetics and/or an epidural. See the ‘2022 ISFM consensus guidelines on the management of acute pain in cats’ for further information. 21
Management of fractures requires analgesia to allow the cat to be comfortable, but more importantly to allow enough comfort for early return to weightbearing/function and to help with the provision of postoperative physiotherapy. Good analgesia will improve the overall demeanor, as well as food and water intake, of the cat.
Physiotherapy following stabilization of a fracture is strongly advised in all cases to prevent excessive muscle wasting/improve muscle mass, prevent muscle contracture, prevent loss of joint range of motion (ROM), and improve mobility and function (including encouraging early limb function); balance and proprioceptive mechanisms are also stimulated.22,23 Physiotherapy should be introduced, if possible, from the first day postoperatively, and carried out three or four times per day. For the first few days postoperatively, physiotherapy aims to control inflammation and swelling and helps to reduce pain and maintain ROM. Cryotherapy should be used during the acute phase of tissue injury and healing to mitigate the effects of tissue injury. 15 This follows the general rule for deciding when to apply cold vs heat that cryotherapy should be used for the first 24-72 h after acute injury when the acute signs of inflammation are present (swelling, redness, heat and pain). 15 The use of cold compresses for 10-15 mins, passive movements to all relevant joints above and below the fracture site (10-20 repetitions) and massage for 2-3 mins is beneficial in most cases. Limited controlled exercise can be introduced with assistance as required, which may consist of manual facilitation or the use of slings or harnesses depending on the compliance of the cat. 23 After the acute inflammatory phase subsides, gentle massage of the limb muscles (2-3 mins) and the application of heat to the affected site (10-20 mins) can reduce swelling and relieve pain and muscle spasm. Simple exercises to improve balance and proprioception can be introduced at an early stage.
Activity must be restricted while the fracture is healing, and cage (or small room) rest is essential until bony union is complete. Flooring must be non-slip and there should be no available opportunities for running or jumping. Caregivers must be made aware of exercise restrictions once the cat is discharged for home care.
Neurologic conditions
There is a wide range of feline spinal cord and peripheral nerve conditions, and the effective treatment of the neurologic patient often represents one of the greatest challenges to the veterinary team. Disturbances to the neural system can affect an animal’s mobility, pain, proprioception, balance, strength, coordination and function, all of which need to be addressed to achieve a good outcome. 23
Feline neurologic conditions that can benefit from physical rehabilitation include intervertebral disc disease, fibrocartilaginous embolism, brachial plexus avulsion, trauma and tail pull injuries. 24

Neurologic patients - typically those with severe spinal or generalized lower motor neuron disorders - often present as recumbent. 25 Recumbency can cause secondary problems associated with the respiratory system, bladder and bowel function, skin and musculoskeletal system. The ability to eat and drink can be affected and there can also be a significant effect on a patient’s demeanor. There are therefore several factors related to the nursing care of these cats that, alongside physiotherapy, are important in order to achieve the best outcome for the cat (see the ‘Nursing care for the neurologic cat’ box).
The goal with neurologic patients is to challenge them without causing excessive neuromuscular fatigue. Further, while providing praise and encouragement is recommended for all physical rehabilitation patients, neurologic patients may require additional encouragement where they have severe mobility issues. The purpose of therapeutic exercises for the neurologic cat is to stimulate proprioceptive tracts to aid body positional awareness and balance, improve muscular strength and attempt to pattern a correct gait as nerves recover. Typical objectives in neurologic rehabilitation are to minimize pain, re-establish normal neural pathways, prevent secondary complications and, if possible, return the animal to independent function. Therapy also aims to counteract the effects of inactivity and it is essential to prevent worsening of neurologic function or pain in patients with spinal instability. A program that is painful or stressful for the patient is unlikely to be effective, may cause the patient to display repelling behaviors and will potentially damage the human-animal bond between the caregiver and the patient. 27
Femoral head and neck excision (femoral head osteotomy)
FHNE is a salvage procedure performed to alleviate or eliminate the pain associated with a diseased or injured coxofemoral joint and to improve the joint’s mobility and function. 28 In cats, FHNEs have been reported for the management of femoral head and neck fractures, including femoral capital physeal fractures, coxofemoral luxations, acetabular fractures and OA. 19 The aim of FHNE is to remove the femoral head and sufficient femoral neck to create a smooth surface that can glide over the lateral aspect of the acetabulum and caudal ilium.
The importance of evaluating the cat’s quality of life after the procedure from the care-giver’s daily observations, in addition to changes in objective measurements, should not be overlooked. 28 The evaluation of lifestyle changes, such as willingness to jump, has been recommended for the assessment of lameness in cats. 29
After FHNE arthroplasty, a few days’ (approximately 1-3 days) rest should be encouraged while the soft tissues heal. During this period, simple physical rehabilitation techniques such as cryotherapy and photo-biomodulation may be used for additional pain control. Following this initial healing period, these patients must be encouraged to use the limb as frequently as possible, otherwise the fibrous tissue that forms during the immediate postoperative period will be restrictive and will severely limit the ROM of the coxofemoral joint. Physical rehabilitation is therefore critical to maximize function in the postoperative period. Initial exercises should include PROM exercises and walking, with more active exercises being moved on to within 2-3 weeks. 30 The protocol should be patient-specific, particularly for those with other orthopedic disease or comorbidities. 30 Appropriate, often multimodal, analgesia in the postoperative period is critical to ensure patient comfort and to facilitate physical rehabilitation.
Obesity
The proportion of pets with obesity, which is clinically defined as a multifactorial disease caused by excessive adiposity sufficient to contribute to disease,31,32 has been steadily increasing for decades. In 2022, 61% of cats were classified as overweight or having obesity. 33 Not all caregivers are aware of the overweight or obese state of their cat, however, with one study finding that just under a third (28%) of cats’ caregivers considered the pet’s body condition ‘normal’ when their veterinary professional scored their body condition as 6-9 (overweight to obesity). 33 There is growing evidence that obesity in dogs and cats increases the risk of many non-communicable diseases, including skin and respiratory disorders, and renal dys-function. 34 Further, obesity increases the risk of metabolic and endocrine disorders (eg, diabetes), orthopedic diseases (eg, OA, cranial cruciate ligament disease) and some types of cancer, and decreases life expectancy.35-38 pet obesity results in reduced quality of life, 38 significant pain and suffering, and increased economic costs for caregivers, accounting for an estimated 20% of all pet insurance claims. 39
Major risk factors for feline obesity include age, sex, breed, gonadectomy, indoor confinement, feeding primarily a dry food diet, free-feeding and feeding frequency, over-estimating food portions, caregiver misperceptions and even the human-animal bond.40-42
Obesity treatment and management is a slow, often unsuccessful, process that can include caloric energy restriction, veterinary therapeutic diets for weight loss, feeding management strategies and exercise for cats (see the ‘‘Thinking cat’ to encourage exercise in overweight or obese patients’ box).40,41
Two pounds or 0.9 kg above a cat’s ideal weight increases the risk of developing serious medical conditions. Unfortunately, once a cat is overweight or obese, the question is no longer ‘if’ a condition will develop secondarily to the excess weight but how many conditions and how soon. 43 Some of the common disorders associated with excess weight include:
✜ Type 2 diabetes - an obese cat is estimated to be at least three times more likely to develop this disease compared with a cat of normal weight
✜ Heart and respiratory disease
✜ OA
✜ High blood pressure
✜ Many forms of cancer - especially intraabdominal cancers
Overweight and obese cats are expected to live shorter lives than their fitter, leaner body weight counterparts. Heavy cats tend to physically interact less with their caregivers and are less energetic and playful. Because they typically lie around more, illness can be easily overlooked as their lethargic state is not noted to be different to their normal activity level.

Prioritizing therapies for feline physical rehabilitation
Prioritization of the different therapies to meet the individual cat’s specific needs and goals, considering and/or addressing any pain and dysfunction, should be carried out in the initial consultation and subsequent therapy sessions. Each session should have a list of questions (see examples below) and goals that the veterinarian and rehabilitation practitioner agree upon, especially in relation to how to reduce the amount of pain a cat is experiencing:
✜ Is hydrotherapy the most important?
✜ Is acupuncture the most important?
✜ Is photobiomodulation the most important?
✜ Are there any specific therapeutic exercises that are the most important?
As an example, a geriatric cat may not be able to move well; the patient may be painful and / or weak. A painful cat will not be willing to participate in exercise that creates more pain. The cat may not be able to take oral analgesics because of concurrent disease. This is where the prioritization of therapies is critical. A plan may include starting with acupuncture, massage, therapeutic laser and mild stretching. Several sessions of this plan may be required before being able to include an individual exercise.
Key Points
✜ Physical rehabilitation for cats is different than for dogs. The basic therapeutic principles remain the same, but there is a much greater need to make the plan creative, fun and easy to follow and to be of short intervals to accommodate the cat’s attention span, which, in the author’s experience, is much shorter than that of dogs.
✜ Physical rehabilitation is most typically used for the management of OA, fractures, neurologic conditions, following articular surgery (eg, FHNE) and obesity.
✜ The different therapies should be prioritized to meet an individual cat’s specific needs and goals, considering and/or addressing any pain and dysfunction.
Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and / or publication of this article.
Funding
The author of this commissioned Clinical Spotlight review received an honorarium; as for all JFMS articles, this Clinical Spotlight article went through peer review.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.