
Abstract
Objectives
The aim of this study was to assess the complication rates and long-term outcomes, as well as to refine case selection criteria for cats undergoing trochlear ridge augmentation (TRA) using an ultra-high molecular weight polyethylene implant (UHMWPEI) for the treatment of patellar luxation (PL).
Methods
The clinical records from two referral veterinary hospitals were searched for cases that fitted defined inclusion criteria. A short-term assessment was based on examination and radiography at 8 weeks postoperatively. The long-term assessment was carried out at least 2 years postoperatively through examination and radiography, and less commonly via questionnaire.
Results
A total of 44 stifles in 39 patients with PL grade 2 (n = 19), 3 (n = 22) or 4 (n = 3) met the inclusion criteria. TRA using UHMWPEI was associated with minor complications in 20% of cases and major complications in 7% of cases. Minor complications included seroma formation (n = 5), superficial wound infection (n = 2), prolonged discomfort for a few weeks postoperatively (n = 1) and transient postoperative azotaemia (n = 1). After surgical correction of medial PL, one skeletally immature case developed transient grade 1 lateral PL, which resolved without intervention. Major complications comprised implant removal for ongoing lameness (n = 3). Degenerative joint disease, with mineralisation that was often marked, was noted in 26/35 (74%) cases that were available for radiographic follow-up 2 years or more after TRA. Nevertheless, good or very good long-term functional outcomes were achieved for 93% of cases.
Conclusions and relevance
The currently available UHMWPEIs were shown to be suitable for treating PL grades 2, 3 or 4 in cats weighing ⩾3 kg. Delaying TRA until growth is completed is advised. The long-term follow-up suggested that the correction of PL in cats with UHMWPEI was sustained and that good function could be expected in the long term. Mineralisation overlying implants was common, but this was not appreciably correlated with adverse functional consequences.
Introduction
Patellar luxation (PL) is an infrequent orthopaedic condition affecting cats. 1 In affected cats, the patella usually luxates medially and the condition can be unilateral or bilateral. 1 Femoropatellar laxity with palpable patellar subluxation/luxation has been reported in cats without evidence of lameness. 2
Feline PL can be developmental or traumatic in origin.1,3 The cause of developmental feline PL is unknown but may be associated with hindlimb conformation issues, a shallow trochlear sulcus, tibial tuberosity deviation and abnormal femoral condyle development.2,4 Correct patellar tracking requires sagittal alignment of the quadriceps mechanism, patella, trochlear groove and tibial tuberosity. 5 Surgical techniques reported to correct patellar tracking include trochlear sulcoplasty (TS), tibial tuberosity transposition (TTT), retinacular imbrication, soft tissue release, 1 femoral corrective osteotomy, 6 anti-rotational suture 7 and patellar groove replacement. 8
A recent study suggested that cats with high-grade medial PL have decreased tibial torsion, tibial tuberosity displacement and decreased trochlear depth:patellar thickness ratio and may require tibial tuberosity transposition and femoral trochleoplasty. 9
The patella, relative to the femoral trochlea, is larger in cats than in dogs. 10 Recently, CT of the cadaveric feline stifle after TS showed no improvement in patellar recession and decreased patellofemoral contact. 10 It was concluded that TS should be combined with partial parasagittal patellectomy (PPP), 10 although PPP has only been reported in four cats. 11
Major complications have been reported in 20% of cats after PL surgery, especially after TTT. 3
Trochlear ridge augmentation (TRA) using ultra-high molecular weight polyethylene implants (UHMWPEIs) (RidgeStop; Orthomed) has recently been described for the treatment of feline PL without quadriceps realignment with only minor complications, return to near-normal stifle range of motion and resolution of lameness. 12
The aim of the present study was to describe complication rates and long-term outcomes as well as to refine criteria for future case selection for cats undergoing TRA without quadriceps alignment by examining 44 stifles after stabilisation of feline PL.
Materials and methods
Case selection
The medical records of feline patients that underwent TRA surgery for PL at two referral hospitals between 2013 and 2021 were retrospectively reviewed. Surgeons A and B performed 39 and five procedures, respectively. Indications for TRA included lameness or reluctance to jump attributable to PL, inadequate response to conservative treatment, no evidence of septic osteoarthritis and no contraindication to general anaesthesia.
Inclusion required complete clinical records, the presence of lateral or medial PL grades 1–4 13 surgically addressed with TRA, and pre-/postoperative radiographs. The short-term outcome was assessed by re-examination at 8 weeks postoperatively with conscious radiography. The long-term outcome was judged after 2 years or more by postoperative re-examination and conscious radiography in 35 cases and by questionnaire in nine cases. Complications were considered ‘major’ if any surgical revision was required and ‘minor’ otherwise.
The stifle range of flexion (ROF) was judged by goniometry 14 as ‘good’ if it still approximated to the norm of 25°, 15 ‘fair’ if it was 30–50° and ‘poor’ if it was more than 50°.
Trochlear ridge augmentation surgery
All cases were premedicated with acepromazine (ACP; Novartis) 0.08 mg/kg IM and methadone (Comfortan; Dechra) 0.1 mg/kg IM. In addition, each case received clavulanate-amoxycillin (Synulox; Zoetis) 12.5 mg/kg SC and meloxicam (Metacam; Boehringer Ingelheim) 0.2 mg/kg SC preoperatively. Intravenous fluid therapy was provided perioperatively with Hartmann’s solution (Aqupharm 11; Animal Care). General anaesthesia was induced with propofol (Propofol-Lipuro; Virbac) 6 mg/kg IV, and the patient was intubated and maintained with isoflurane (IsoFlo; Zoetis).
Orthogonal stifle radiographs were obtained. In the uncomplicated PL cases (cases 1–36 inclusive), ROF was preoperatively confirmed as approximately 25° using goniometry.
Parapatellar arthrotomy was performed on the side of the PL as previously described.16,17 A low-profile UHMWPEI (RidgeStop, 1.5; Orthomed) was secured to the ipsilateral femoral trochlear ridge with stainless-steel self-tapping cortical screws. The TRA implant was placed relatively abaxially (because of the depth and breadth of the feline trochlear sulcus and patella) and positioned to optimise the tracking of the patella proximally. 12 UHMWPEIs were placed over any cartilage erosion or remodelled tissue abaxial to the sulcus without debridement (Figure 1). The distal hole was drilled with the relevant 1.5 drill guide (Orthomed). The UHMWPEI was secured with a distal bicortical screw. The proximal hole was drilled directly through the implant without using the drill guide, 12 usually with a Kirschner wire, taking great care to avoid damaging the implant. All screws were 2.4 mm cortical screws placed bicortically, except for four stifles where 2 mm screws were used (cases 18–21) and one stifle where one distal 2.7 mm unicortical screw was used (case 5).
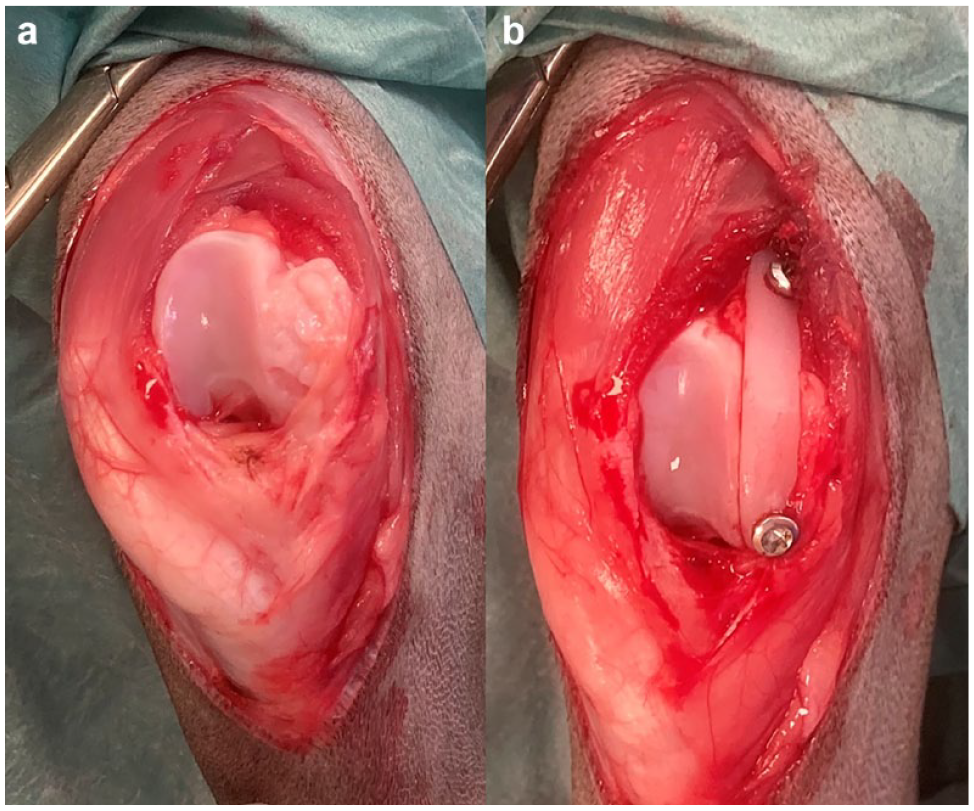
Intraoperative image of stifle 23 (a) before and (b) after trochlear ridge augmentation
No quadriceps realignment techniques were performed. A cranial approach was made to stifle 38 to accurately reduce an articular fracture and the tibial crest was fixed in its original location.
The arthrotomy was closed by closing the retinacular tissues with 2 metric polydioxanone (PDS; Ethicon) using a simple interrupted pattern. No retinacular imbrication or soft tissue release was performed. Subcutaneous tissue and skin were sutured using 2 metric polyglicaprone 25 (Monocryl; Ethicon) using simple continuous patterns. Orthogonal postoperative radiographs were obtained.
Postoperative analgesia included methadone (Comfortan; Dechra) 0.1 mg/kg IV q4h and meloxicam (Metacam; Boehringer Ingelheim) 0.05 mg/kg SC q24h. Once they were scoring low on the Glasgow Composite Measure Pain Scale, 18 patients were discharged with meloxicam (Metacam; Boehringer Ingelheim) 0.05 mg/kg PO q24h for 7 days and clavulanate-amoxycillin (Synulox; Zoetis) 12.5 mg/kg PO for 7 days. Cage rest was advised for 3 weeks postoperatively.
Follow-up
Cases were re-examined after 2–3 weeks and the short-term outcome was judged at 8 weeks postoperatively with an orthopaedic examination and radiography. The long-term follow-up was judged not less than 2 years postoperatively, typically with an orthopaedic examination and radiography (n = 35). The long-term outcome was assessed via questionnaire in nine cats because the owners of cases 9, 18–21, 28 and 41 did not feel that the clinical signs justified transporting their pets, and cases 43 and 44 had died of unrelated causes. Except for cases of major complications requiring further surgery, chemical restraint was not used for any follow-up examinations or radiography. Radiography was performed with the patient standing, using a handheld radiographic generator (Nomad Pro 2; Dexis).
Results
The 39 cats (18 male, 21 female) were aged 0.5–13 years (mean 4, median 2) and weighed 2.5–6.0 kg (mean 4.2) (Table 1). In total, 31 cats (36 stifle surgeries) underwent TRA to treat PL with no associated fractures, ligamentous injury or previous attempts at PL surgery, and these cats were aged 0.5–13 years (mean 3.4, median 2) and weighed 2.5–6.0 kg (mean 4.1). These uncomplicated PL cases included 20 domestic shorthairs, three Maine Coons and two British Blues.
Patient characteristics
Individual case details: stifles 1–36 = uncomplicated PL; case 37 = revision of TS; cases 38–40 = previous fracture in the same limb; cases 41–44 = associated cruciate ligament injury. Rows in italics denote PL managed either conservatively or with a surgical technique other than TRA (cat A); signalment boxes in bold highlight cases with bilateral TRA
Cases 1, 2, 5 and 6 were previously reported 12
Delay was considered in case 12, but deemed inappropriate on account of severity of presenting signs
CaCLR = caudal cruciate ligament rupture; CrCLR = cranial cruciate ligament rupture; CrMinXR = mineralisation evident in the cranial stifle; DJD = degenerative joint disease; DLH = domestic longhair; DSH = domestic shorthair; d/wk/mo/y = days, weeks, months or years, respectively; ESF = external skeletal fixation; F = fair; Fe = female; G = good; LL = lateral left PL; LR = lateral right PL; LRS = lateral retinacular suture (50 lb crimped leader line); M = male; ML = medial left PL; MR = medial right PL; neg, mild, mod, sev = negligible, mild, modest or severe radiographic DJD, respectively, as assessed, on a lateral stifle radiograph where this was available at least 2 months after TRA; NSAIDs = non-steroidal anti-inflammatory drugs; P = poor; PDS = polydioxanone; PL = patellar luxation; RI = retinacular imbrication; R/O = removal of; ROF = range of flexion; S,R = seroma, resolved; SWI,R = superficial wound infection, resolved; TRA = trochlear ridge augmentation; TS = trochlear sulcoplasty; TT = tibial tuberosity; TTT = tibial tuberosity transposition; VG = very good
PL treated with TRA was graded as medial or lateral (in 40 and four stifles, respectively), and graded after Singleton 13 as 1, 2, 3 or 4 (in 0, 19, 22 and three stifles, respectively).
Of the 23/31 cats with bilateral uncomplicated PL, only five (22%) needed surgery on both stifles during the study period, although contralateral TRA has since been recommended for cat T. Two cats (cats C and O) had bilateral TRA under one general anaesthetic; three cats (K, M and AA) had staged bilateral TRA surgeries and one cat (A) had had a previous TTT surgery in the contralateral limb.
The limbs of 3/44 stifles had fractures before the PL diagnosis: a tibial plateau fracture, 7 months before TRA (stifle 38); a distal femur Salter-Harris fracture, 6 weeks before TRA (stifle 40); and a tibial diaphyseal fracture that had occurred 1 year before bilateral PL was noted (stifle 39).
Of the 44 stifles, two had prior PL surgery elsewhere. One had had retinacular imbrication and a fabella-patella polydioxanone suture placed several years before PL recurred in conjunction with cranial cruciate ligament (CrCL) rupture (stifle 41), and one had TS with retinacular imbrication elsewhere, 1 month before revision with TRA (stifle 37).
Four of the 44 stifles had concurrent cruciate ligament disease (stifles 41–44). One had a complete caudal cruciate ligament (CaCL) rupture and one had a partial CrCL rupture. These were not specifically addressed alongside the TRA. Two complete CrCL ruptures were addressed with crimped lateral retinacular sutures (LRS). Stifle 41 had historic PL surgery including retinacular imbrication, and then had LRS at the time of TRA (Figure 2). Stifle 44 had TRA 7 weeks after LRS.

(a,a1) Preoperative, (b,b1) immediate postoperative and (c,c1) 14 months postoperative mediolateral and craniocaudal radiographs of stifle 41. Note the presence of intra-articular mineralisation (panel c, red arrow) and a crimp tube securing a lateral retinacular suture to address cranial cruciate ligament instability (panels b and c)
Outcome
The outcome was considered ‘very good’ if there was patella stability, no reported lameness, enthusiastic jumping and symmetrical hindlimb muscle mass. The outcome was judged ‘good’ if there was patella stability and markedly improved limb use without intermittent carriage, but if mild/occasional lameness/stiffness and/or reduced inclination/ability to jump were noted. The outcome was judged ‘fair’ if mobility was improved, but if there was nevertheless some significant persistent lameness. The outcome was judged ‘poor’ if the patella remained unstable or if mobility was no better than preoperatively.
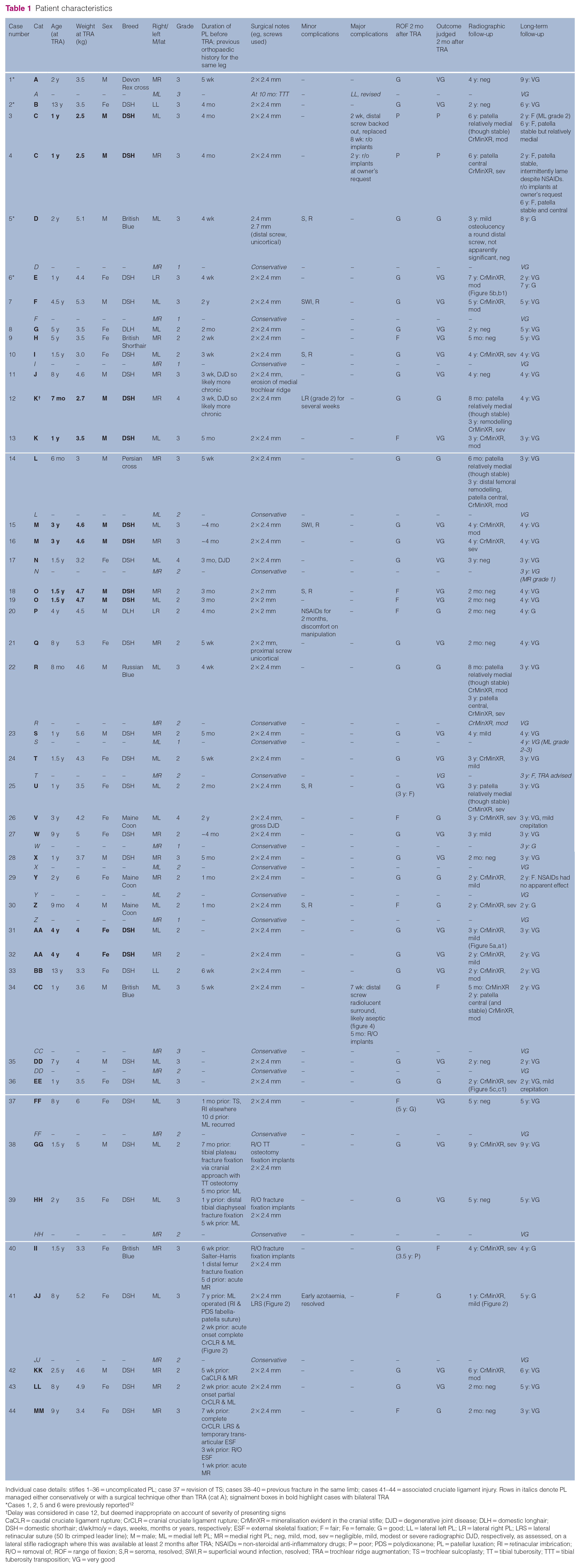
Eight weeks after TRA, all patellae were stable over the trochlear sulcus and short-term outcomes were judged as very good (n = 29), good (n = 11), fair (n = 2) with some residual persistent lameness and poor (n = 2) with no significant improvement in mobility.
Long-term outcomes after 2–9 years (mean 4, median 4) were generally similar to the judgement after 8 weeks; however, two long-term outcomes were moderately downwardly revised (stifles 6 and 29). In 10 cases, the long-term outcome had improved, usually by just one increment. In stifles 12, 14 and 22, the three youngest patients, which were only 6–8 months old at the time of TRA, the outcome was good at 8 weeks but improved to very good by 6–8 months postoperatively. The short- and long-term outcomes are detailed in Figure 3.
Summarised short- and long-term outcome showing data for (a) all 44 stifles and (b) stifles in cats weighing 3 kg or more
The ROF in stifles only changed between the short-term and long-term assessments in three cases: ROF increased in case 37 but decreased in cases 25 and 40. When comparing ROF after 8 weeks with long-term outcome, the following was noted: where the short-term ROF was good (n = 32), the long-term outcome was very good in 88% (n = 28), good in 9% (n = 3) and fair in 3% (n = 1); where the short-term ROF was fair (n = 10), the long-term outcome was very good in 70% (n = 7) and good in 30% (n = 3); and both cases with poor ROF 2 months postoperatively only had a fair long-term outcome. The Spearman’s rank correlation coefficient test was performed to evaluate the correlation between ROF 2 months postoperatively and long-term functional outcomes (Spearman rank correlation +0.375). The relationship was positive and considered to be weak to moderate.
The two surgeries that resulted in a ‘poor’ outcome after 8 weeks (stifles 3 and 4) were both in the smallest patient in the series weighing 2.5 kg (cat C). Postoperative mobility was not improved. The ROF of both stifles was reduced, probably because of the implant bulk. Implants were removed from one side 7 weeks postoperatively and PL recurred. Contralateral implants were removed 2 years postoperatively and PL did not recur. In both stifles, the long-term outcome improved to ‘fair’. Because of the early experiences with cat C and a second cat operated when weighing 2.7 kg (stifle 12), cats weighing <3 kg were no longer considered as candidates for UHMWPEIs.
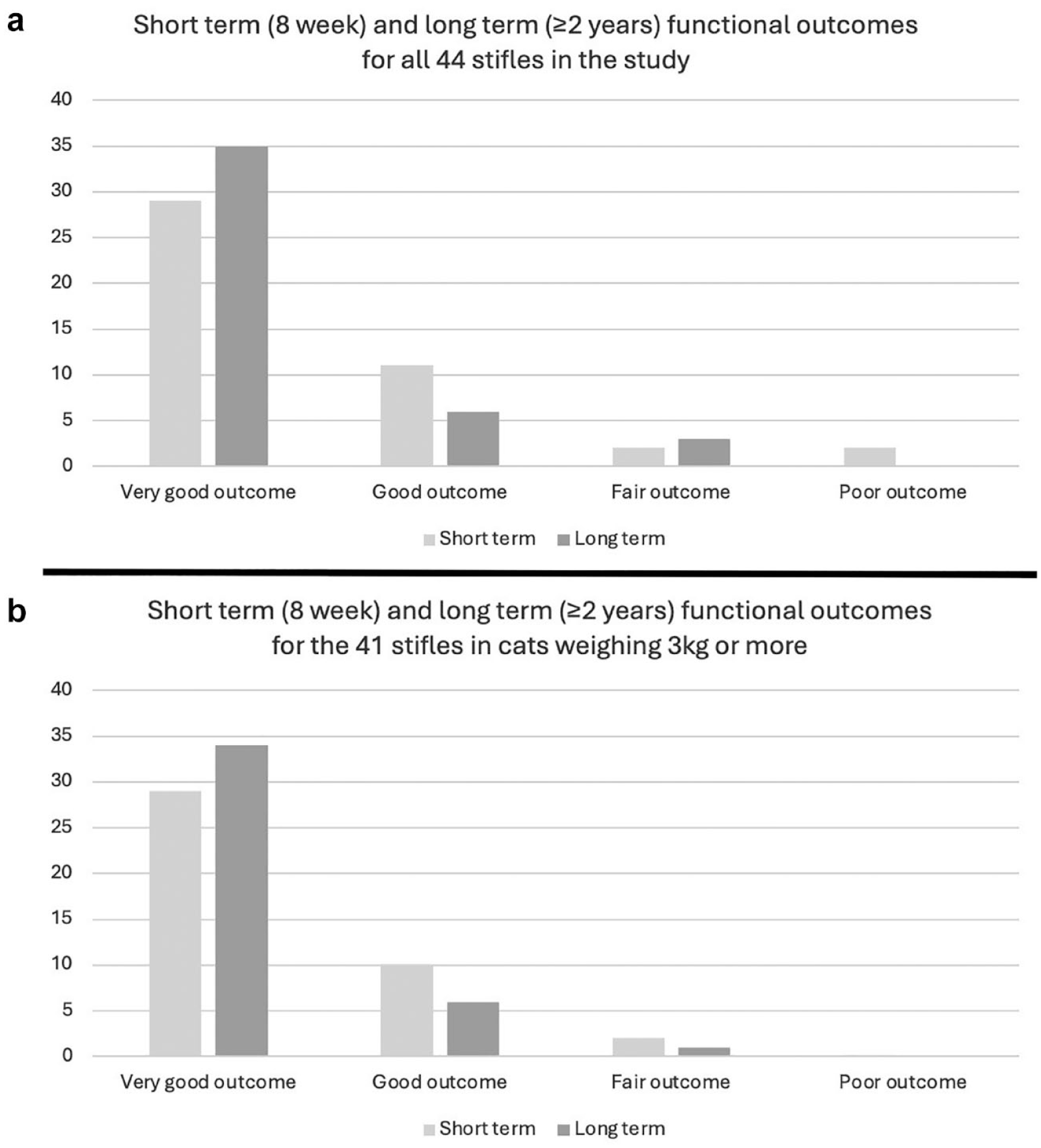
In case 34, the outcome was judged ‘fair’ after 8 weeks. The intermittent non-weight bearing lameness reported preoperatively did not occur postoperatively, but persistent low-grade lameness postoperatively and radiolucency around the distal screw (Figure 4) led to implant removal after 5 months. PL had not recurred at the long-term follow-up, 2 years after TRA.
(a) Immediate postoperative and (b) 8 weeks postoperative mediolateral radiograph of stifle 34 demonstrating radiolucency surrounding the distal screw (red arrows)
Of 44 TRAs performed in 39 cats, three implants were removed, representing a 7% incidence of major complications. Of 41 TRAs performed in 38 patients weighing ⩾3 kg, the incidence of major complications was 2.5% with just one implant removed.
Minor complications affected 20% of cases and included transient seromas (n = 5), superficial transient wound infections (n = 2), temporary low-grade PL in the opposite direction (n = 1), prolonged discomfort on manipulation for a few weeks postoperatively (n = 1) and transient azotaemia postoperatively (n = 1). In the weeks and months after surgery, three cases showed transient periods of recurrent lameness that resolved after anti-inflammatory therapy.
Three cases with medial PL, including two of grade 3 (stifles 14 and 22) and one of grade 4 (stifle 12), were treated at 6–8 months of age while the patients were skeletally immature. In all cases, the patella remained stable but became progressively more medially positioned in the months after surgery. Stifle 30 was operated at 9 months of age and the patella remained axially located after surgery.
One distal screw, intentionally placed unicortically, developed a radiolucent surround (stifle 5). One proximal screw was unintentionally placed unicortically (stifle 21). Nevertheless, outcomes were good and very good respectively. Some radiolucency developed around a bicortical distal screw (stifle 34) and implants were ultimately removed. One distal screw placement was considered overly distal (stifle 17), but the long-term outcomes were both still very good. No implant breakage or implant-associated infection was noted.
A very good outcome was achieved when TRA was used to revise a case that had previously been treated with a TS (stifle 37), even though significant articular damage was evident at the time of revision.
A total of 36 stifles were re-radiographed 1 year or more after TRA (35 of them were 2 years or more after TRA). The severity of the radiographic DJD changes, enthesiophytosis and mineralisation in the cranial joint was subjectively assessed from a lateral radiograph by one author as negligible, mild, moderate or severe. Figure 5 gives an indication of radiographs that were typical of those scored as mild, moderate and severe, respectively. Of the 36 cases, 11 (31%) had long-term radiographic changes graded as severe; of these cases, the long-term outcomes were very good for eight (73%) cases, good for two (18%) and fair for one (9%) case. Nine of the 36 cases (25%) had long-term radiographic changes graded as moderate; of these cases, the long-term outcomes were very good for seven (78%) cases, good for one (11%) and fair for one (11%) case. Seven of the 36 cases (19%) had long-term radiographic changes graded as mild; of these cases, the long-term outcomes were very good for five (71%) cases, good for one (14%) and fair for one (14%). The remaining nine (28%) cases had negligible radiographic changes indicative of DJD; of these cases, the long-term outcomes were very good for eight (89%) cases and good for one (11%) case (Figure 6). The Spearman’s rank correlation coefficient test was performed to establish if there was any correlation between the severity of radiographic changes at least 1 year postoperatively and long-term functional outcomes. No meaningful correlation was recognisable (Spearman’s rank correlation −0.123).
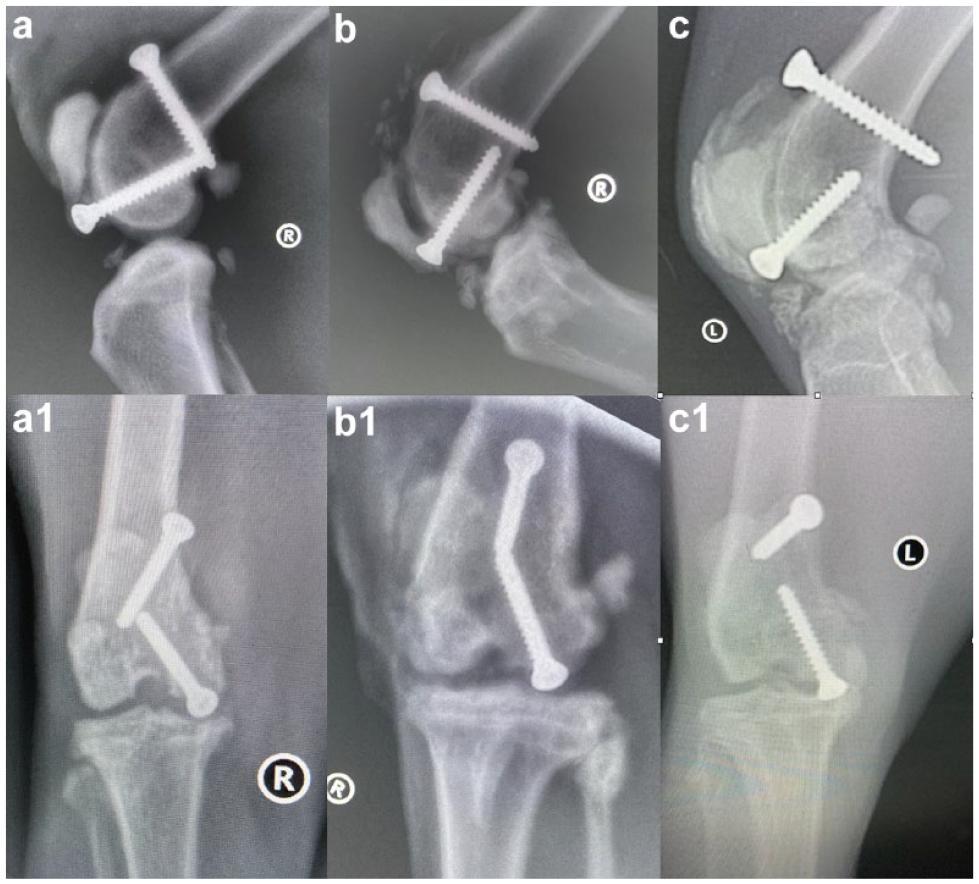
Mediolateral and craniocaudal radiographs showing (a,a1) relatively mild degenerative joint disease/mineralisation changes in stifle 31, 3 years after trochlear ridge augmentation (TRA), (b,b1) moderate changes in stifle 6, 7 years after TRA and (c,c1) severe changes in stifle 36, 2 years after TRA
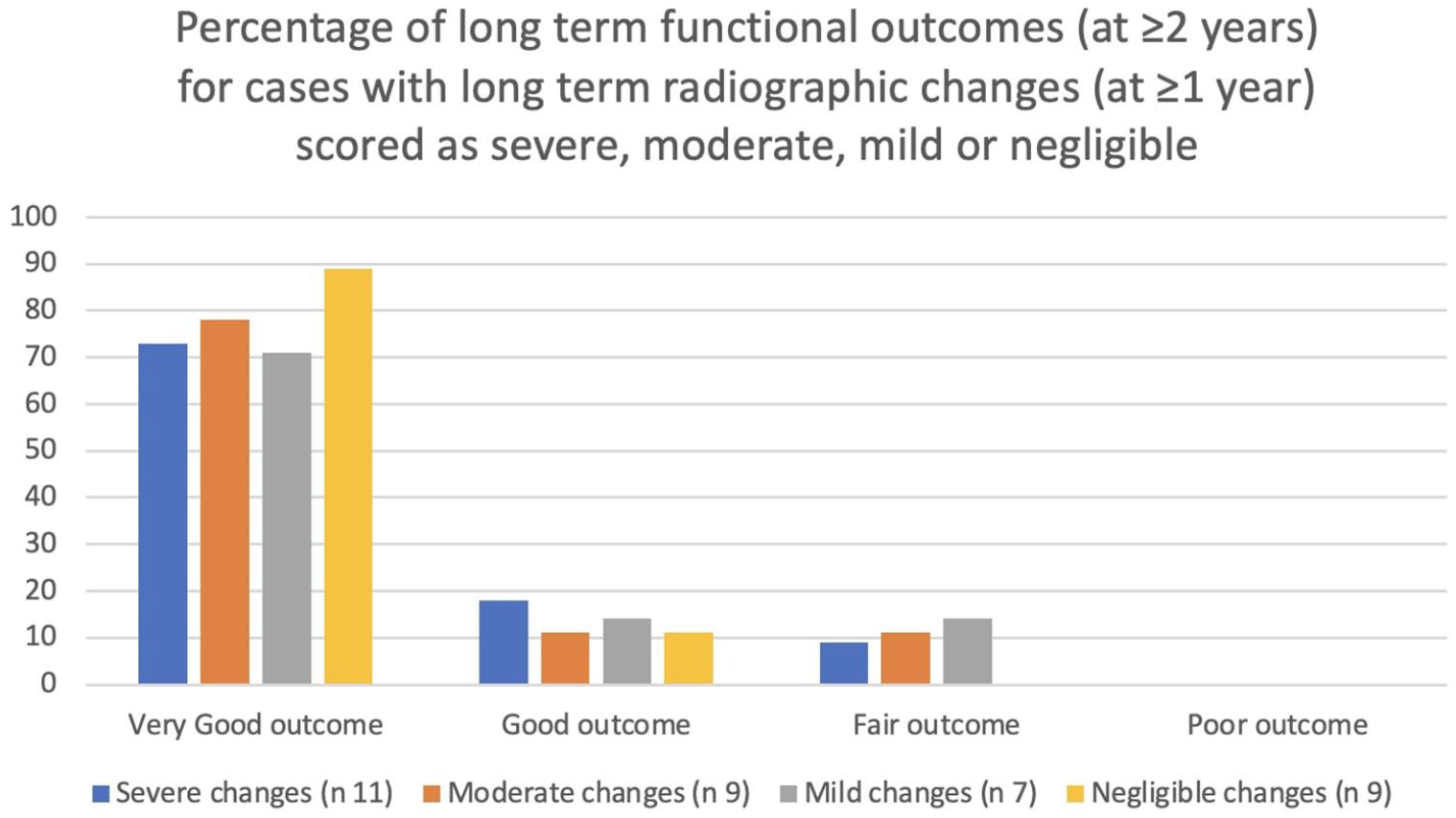
Summarised long-term functional outcomes compared with long-term radiographic changes
Discussion
TRA has only been reported relatively recently in cats.12,19 The importance of patient size when considering TRA for feline PL cases became evident given the minimum UHMWPEI size currently available. The smallest cat operated on (C) weighed 2.5 kg and experienced two of the three major complications in the series. The next smallest cat (K) weighed 2.7 kg at 7 months of age. It was the only case where PL temporarily occurred in the opposite direction postoperatively, probably reflecting the relative bulk of the implant until further growth had occurred. The 7% (3/44) incidence of major complications reduced to only 2.5% (1/41) in patients weighing ⩾3 kg. The major complications were all technically unchallenging explantations. The incidence and technical challenge of major complications after feline TRA compared very favourably with major complications reported in 20% of cases after techniques including TS and TTT. 3 Meaningful comparison of TRA with the four published PPP cases was not possible. 11
Patella reluxation might be expected after UHMWPEI removal, and that was seen after explantation 7 weeks postoperatively in stifle 3. However, PL did not recur after explantation 5 months and 2 years postoperatively in stifles 34 and 4, respectively. Despite rating as a major complication, PL was nevertheless resolved if the UHMWPEI explantation was delayed.
Based on the five cats that underwent bilateral TRA surgeries (C, K, M, O and AA), the authors advise staging bilateral procedures. Some cats take a few days to mobilise after TRA. The risk of another anaesthetic in cats that are young and otherwise healthy is generally acceptable.
After the early experiences with cats C and K, the authors recommend that TRA be reserved for patients weighing ⩾3 kg unless smaller implants become available. For the remaining discussion, only the 42 TRAs in 38 cats weighing ⩾2.7 kg will be considered.
Concurrent TTT has been recommended alongside TRA for canine PL of grades 3–4. 20 Three cats with medial PL (two grade 3 and one grade 4) were reported to return to apparently normal function after TRA and concurrent TTT. 19 In the current series, TRA without TTT gave good or very good short- and long-term outcomes for grade 4 PL (3/3) and for grade 3 PL (18/20 after 8 weeks and 20/20 when judged long term).
Quadriceps mechanism misalignment might be expected to increase axial loading on UHMWPEI surfaces causing wear, with long-term adverse effects. The authors speculate that the natural laxity of the feline patella, even without quadriceps mechanism realignment, might reduce the UHMWPEI loading compared with dogs. Regardless, 41 TRA prostheses remained in situ and were followed for 2–9 years (mean 4), with 40 (98%) enjoying good or very good long-term outcomes.
DJD progresses after TRA placement. 12 Progression would be expected even with conservative management of PL. 21 Radiographic assessment of DJD progression was crude, and the authors recognise that their grading of functional outcome and radiographic signs was somewhat arbitrary, but the dramatic changes that were apparent in many of the radiographs that were taken at the long-term follow-up were not associated with similarly dramatic adverse long-term functional outcomes or progressive functional deterioration. Patient GG was radiographed 9 years after a serious intra-articular fracture and had radiographic changes that were graded as severe, yet that patient had very good function and was still a prolific hunter and jumper. The unoperated stifle of cat R still had very good function despite developing significant DJD radiographically.
Mineralisation frequently occurred over the cranial joint compartment in the regions of the insertion of the CrCL or joint capsule overlying the UHMWPEI (Figures 2 and 5). The authors speculate that this might have been some combination of reaction to the presence of the foreign material of the UHMWPEI, reaction to UHMWPEI wear particles or DJD relating to the underlying condition or the surgery.
In stifle 37 where TRA revised a previous surgery for PL with TS and retinacular imbrication, the functional long-term outcome was nevertheless very good despite considerable articular trauma preceding the TRA. There was surprisingly little DJD radiographically evident 5 years later. TRA successfully managed PL that followed tibial and femoral fractures. Together with LRS, TRA successfully managed PL associated with complete CrCL rupture.
To the authors’ knowledge, this is the only study that evaluates function after TRA using UHMWPEIs in a relatively large number of cats affected by PL over a long period. In dogs, a custom-made trochlear ridge prosthesis for the treatment of PL was recently described. 22 Successful outcomes were achieved in 59/60 cases. 22 Nevertheless, because of the relatively short follow-up (mean 3.8 months), assessment to establish the progression of DJD was not possible. 22 It is not uncommon to see progression of DJD in cats presenting with PL. 1 Loughin et al 1 could not assess whether traditional techniques for the correction of PL in cats delay or decrease the progression of DJD. A prospective study comparing a cohort of cats treated using traditional techniques1,6,7 with those treated using TRA is necessary to compare the clinical outcomes and the progression of DJD.
Compliance with postoperative exercise restriction was not verifiable. TRA is intuitively more tolerant of poor compliance than osteotomy techniques. TRA avoids introducing the inherent temporary mechanical weaknesses and obvious stress risers that are introduced to the system by traditional osteotomy techniques, such as TTT and TS. In the event of poor postoperative owner compliance with suboptimal exercise restriction, avoiding having introduced such weaknesses would likely be advantageous.
It has been demonstrated that the majority of physes in cats are closed by 9 months of age. 23 Four juvenile patients received TRA (stifles 12, 14, 22 and 30). In the three youngest, aged 6–8 months, the patella was stabilised but became progressively more abaxially located towards the side of the original PL over subsequent months. Further growth probably led to the TRA progressively locating abaxially, or developmental abnormalities underlying the PL may have progressed. Distal femoral remodelling was evident in cases where TRA had occurred during growth. In all three cases, the long-term outcome was improved compared with the short-term outcome at 8 weeks. The authors suggest that TRA should be delayed until ⩾9 months of age, if possible.
The original TRA technique described unicortical distal screw placement. 20 TRA is forgiving of unicortical placement, but the authors advocate bicortical placement of TRA screws to optimise stability and reduce the risk of aseptic screw loosening. 12 In stifle 5, the unicortical distal screw developed a radiolucent surround 3 years postoperatively. In stifle 21, the proximal screw failed to engage the transcortex and was not repositioned. Nevertheless, the outcomes were very satisfactory. Intraoperative radiography is advisable to verify screw placement before closure.
During UHMWPEI development, 2 mm screws sometimes broke when trialled with 1.5 RidgeStop implants in canine patients (unpublished data, Orthomed). The authors largely used 2.4 mm screws. Smaller 2 mm screws minimise soft tissue drag over the better-recessed screw heads and might be adequate in cats where UHMWPEI loading may be less, as previously speculated. Surgeon B successfully used 2 mm screws in four stifles.
Further studies with CT could better evaluate postoperative mineralisation while post-mortem histopathology could better evaluate the effect of UHMWPEI wear particles. However, the former would obviously require chemical restraint in patients with questionable clinical justification, and owner consent could prove problematic for both.
Conclusions
TRA can be considered for PL in cats weighing ⩾3 kg. TRA does not require prolonged postoperative confinement. The placement of permanent intra-articular prostheses requires scrupulous asepsis. TRA has given very satisfactory long-term outcomes with a low incidence of major complications in managing developmental PL, traumatic PL associated with CrCL ruptures, PL after fracture fixations and PL revision after TS. TRA without concurrent TTT successfully managed grade 3 and grade 4 PL. Where TRA was performed before growth was completed, the UHMWPEI became progressively relatively abaxially located towards the side of the original PL in the months after surgery. PL may not recur if explantation is delayed for 6 months. Long-term UHMWPEI wear remains a potential concern. Progression of radiographic signs of DJD was noted in 75% of cases. Long-term outcomes were very satisfactory in 90% or more of cases.
Footnotes
Acknowledgements
The authors thank Simon Roche, Toby Gemmill and Luisa de Riso of Linnaeus for advice while preparing early drafts of the manuscript, and also Dr Ian Graham Handel, Jack Fawsitt and Junaid Butt for advice in preparing the manuscript and for statistical advice.
Conflict of interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TH was involved with the original commercial development of RidgeStop prostheses.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.