
Abstract
Objectives
Vaccinations should only be given to healthy cats, and deworming before vaccination is generally recommended; however, so far, no study has investigated the influence of intestinal parasitic infection on the immune response in kittens. The aim of this prospective study was to compare the antibody response to feline panleukopenia virus (FPV) vaccination in kittens with and without intestinal parasites.
Methods
Overall, 74 healthy kittens were included. Of these, 17 had intestinal parasites (12/17 Toxocara cati, 6/17 Cystoisospora felis, 1/17 Capillaria species). Both kittens with and without (n = 57) parasites received two primary kitten vaccinations with modified live FPV vaccines in a 4-week interval starting at the age of 8–12 weeks. Anti-FPV antibodies were determined at the beginning of the study (week 0) and at week 8 (4 weeks after the second vaccination) by haemagglutination inhibition. A ⩾four-fold titre increase (week 8 vs week 0) was defined as a response to vaccination. Comparison of the immune response in the kittens with and without intestinal parasites was performed using Pearson’s χ2 test.
Results
Pre-vaccination antibodies were present in 4/17 (23.5%) kittens with intestinal parasites and in 24/57 (42.1%) without parasites. A ⩾four-fold titre increase was seen in 13/17 (76.5%) kittens with parasites compared with 32/57 (56.1%) kittens without parasites. There was neither a significant difference in pre-vaccination antibodies (P = 0.17), nor in vaccination response (P = 0.13) between kittens with and without parasites.
Conclusions and relevance
The results indicate that asymptomatic intestinal infections with endoparasites do not interfere with the immune response to kitten vaccination series. Parasitic infection (at least with T cati, C felis and Capillaria species) is therefore not a reason to postpone important vaccinations.
Keywords
Introduction
Feline panleukopenia virus (FPV) is a non-enveloped, single-stranded DNA virus 1 and causes fatal systemic infection in cats. 2 Morbidity and mortality are very high, especially in kittens.3,4 Vaccination against FPV is strongly recommended in all cats, as part of the ‘core’ vaccination programme. 1 In the first weeks of life, kittens are protected by maternally derived antibodies (MDAs);1,5,6 however, when MDAs decrease, kittens are highly susceptible. Therefore, it is important to ensure that the first vaccination is given at the age of 6–8 weeks with subsequent re-vaccinations every 4 weeks until at least 16 weeks of age, and a booster 6–12 months later to avoid disease in unprotected kittens in which panleukopenia is commonly deadly.1,5 –8
Effective immune response, however, is affected by individual factors, such as health status (eg, infectious and chronic diseases, immunosuppressive drugs), environment, nutrition and stress.1,9 In addition, infections with endoparasites can be associated with a compromised immune system. In human medicine, experimental and field studies showed that both cellular and humoral response after vaccination (eg, against seasonal influenza, hepatitis B, malaria, pulmonary tuberculosis) were compromised in patients with parasitic infection (eg, Litomosoides sigmodontis, Schistosoma japonicum, Trichuris trichiura, various helminths).10 –13 A meta-analysis confirmed that the immune response can be compromised owing to chronic parasitic infections. 14 In dogs, parasitic infections can also negatively influence the immune response and can lead to immunosuppression. 15 This was shown in a study in puppies that suffered from Toxocara canis, Toxascaris leonina and/or Trichuris vulpis infection and had significantly lower anti-rabies antibodies after vaccination than a non-infected control group. 16
So far, studies in kittens comparing the antibody response after vaccination with and without intestinal parasites are lacking, although kittens are commonly infected with protozoan parasites, such as Giardia species, Cystoisospora species and/or with helminths, such as Toxocara cati. 17 The results of a retrospective study in Germany revealed that kittens (aged up to 3 months) were significantly more commonly infected with Giardia species (19.5%), Cystoisospora species (12.8%) and T cati (8.1%) than older cats; 17 for example, kittens can easily be infected with T cati by lactogenic transmission.18,19 Therefore, the European Scientific Counsel Companion Animal Parasites (ESCCAP) guidelines recommend that the deworming of pregnant queens should be performed approximately 7 days before expected parturition and kittens should be dewormed at 3 weeks of age, with a subsequent deworming every 2 weeks until weaning, and then monthly until 6 months of age. 18 This advice, however, is not regularly followed by owners. Although no study has been performed in kittens so far, it is recommended by many experts to deworm kittens before vaccination in order to avoid potentially impaired immune responses.15,16,20 However, the question arises whether in asymptomatic kittens, which are often presented to veterinarians for their first vaccination without previous anti-parasitic treatment, important core vaccinations should indeed be postponed; a delay in vaccination might increase the risk of lethal infectious diseases, such as panleukopenia.
The aim of the present study was to investigate the prevalence of intestinal parasites in healthy kittens presented for their first vaccination and to compare the antibody response to FPV vaccination in those with and without intestinal parasites.
Materials and methods
Kittens
This prospective study included 74 client-owned kittens that were presented to the Ludwig-Maximilians-Universitaet (LMU) Small Animal Clinic, Centre for Clinical Veterinary Medicine in Munich. The protocol of the present study was approved by the Government of Upper Bavaria (reference number ROB-55.2-2532.Vet_03-18-57) and by the ethical committee (reference number 374-15-09-2023) of the Centre for Clinical Veterinary Medicine, LMU Munich. Each kitten owner signed a consent form before participation. Kittens also participated in another long-term study following vaccination response that has been published elsewhere. 21
Kittens aged 8–12 weeks that had not been vaccinated before and that had not received deworming or any other systemic drugs within the previous 28 days before presentation were included. Further inclusion criteria were an unremarkable history and physical examination, and a negative feline immunodeficiency virus (FIV) and feline leukaemia virus (FeLV) ELISA (SNAP Combo Plus FeLV-antigen/FIV-antibody test; IDEXX Laboratories). Collected data on each kitten included signalment, origin, lifestyle (indoor or outdoor) and housing conditions (single- or multi-animal household) (Table 1). Medical history was obtained and physical examination was performed before each vaccination.
Signalment, origin and housing condition of the 74 client-owned kittens
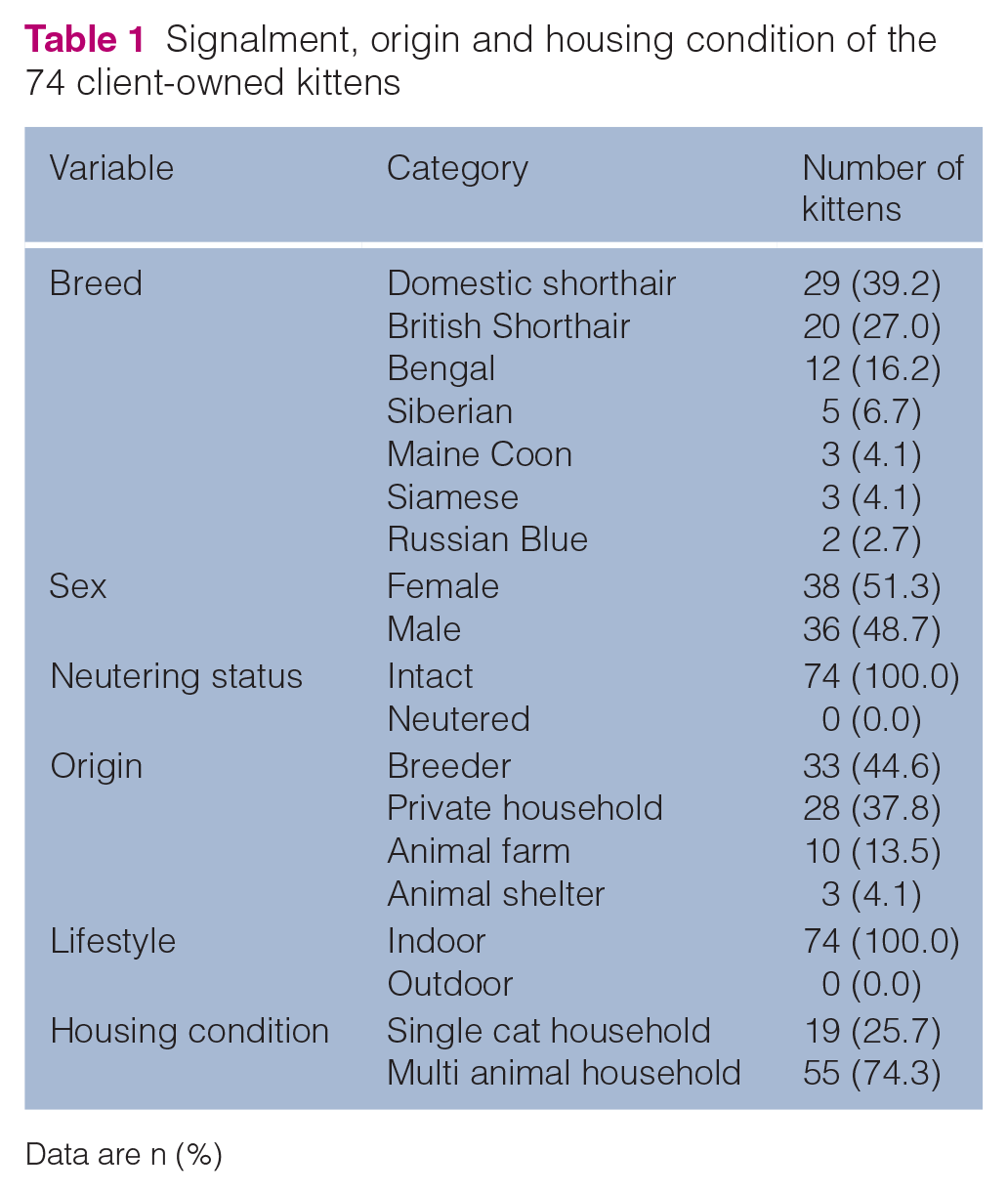
Data are n (%)
Most kittens were purebred (45/74, 60.8%), belonging to different breeds (Table 1). Overall, 55/74 (74.3%) kittens lived with other animals (cats, dogs, rabbits or rats).
Vaccinations
Each kitten received a primary vaccination series against infections with feline herpesvirus (FHV), feline calicivirus (FCV) and feline panleukopenia virus (FPV) (combined modified live virus [MLV] vaccine containing attenuated FPV strain PLI IV with a viral titer of ⩾103.5 cell culture infective dose 50%, Purevax RCP; Boehringer Ingelheim), starting at the age of 8–12 weeks with subsequent re-vaccinations every 4 weeks (three vaccinations in total) until at least 20 weeks of age and a booster 1 year later (Figure 1).1,5 –8 The immune response to vaccination against FCV or FHV was not a subject of the present study.
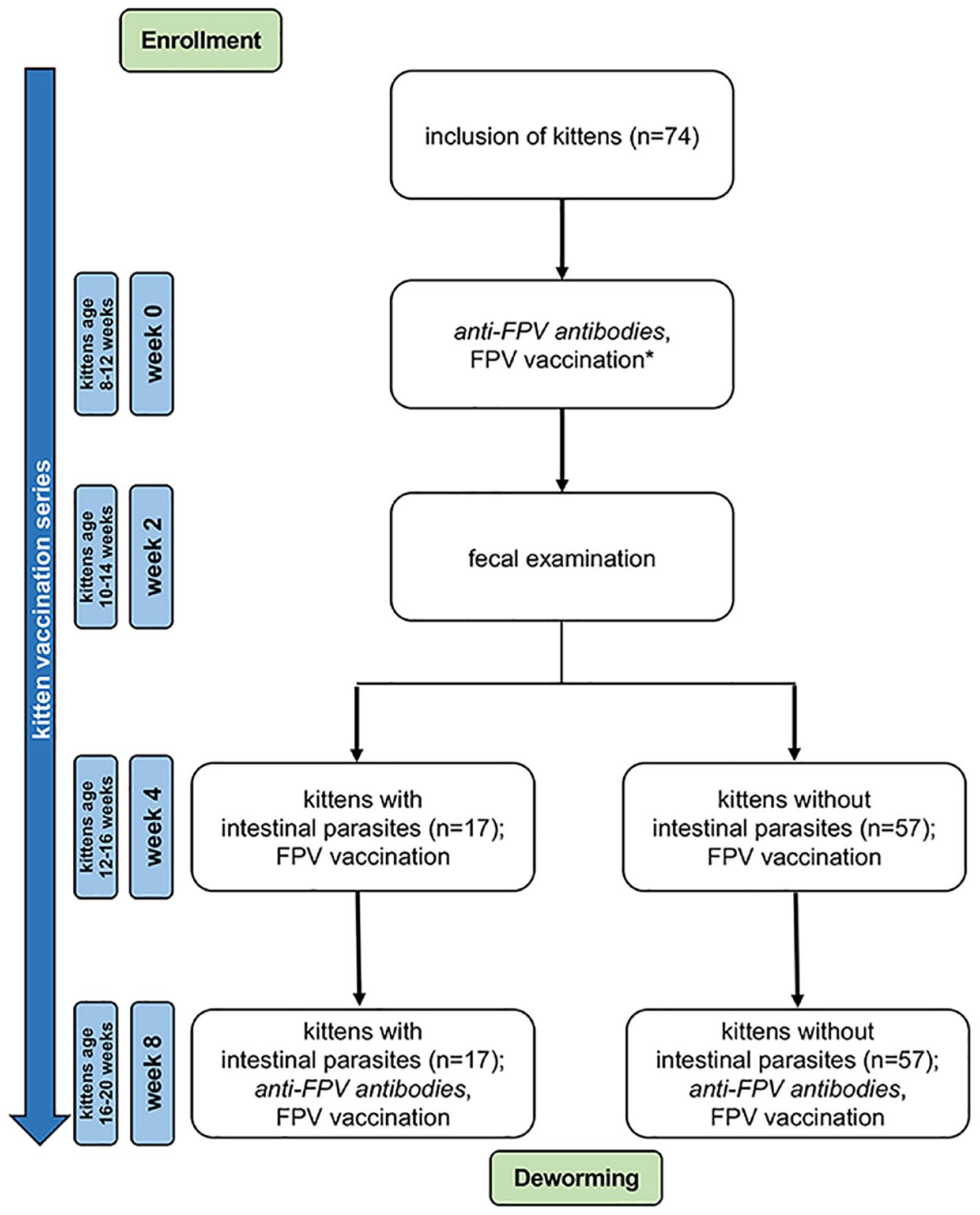
Flow diagram illustrating the study course (enrolment, inclusion, vaccination, antibody testing and allocation process) for kittens with and without intestinal parasite infection (based on faecal examination). *Feline panleukopenia virus (FPV) vaccination: combined modified live virus vaccine containing attenuated FPV strain PLI IV with a viral titre of ⩾103.5 cell culture infective dose 50% (Purevax RCP) as well as feline herpesvirus and inactivated feline calicivirus. Italic text refers to the measurement of anti-FPV antibodies in blood by haemagglutination inhibition
Vaccines were stored refrigerated, brought up to room temperature 15 mins before injection 22 and were administered subcutaneously in the left lateral abdominal wall using a 2 ml syringe with a 23 G needle.
Kittens were observed for immediate adverse reactions for 15 mins. In addition, owners were instructed to record the occurrence of possible vaccine-associated adverse events (VAAEs; eg, swelling and/or pain at the injection site, fever, lethargy, hypo-/anorexia, vomiting).
Detection of anti-FPV antibodies by haemagglutination inhibition
Serum samples were collected for the measurement of pre- and post-vaccination anti-FPV antibodies (at week 0 and week 8) (Figure 1), frozen at −80°C and shipped on dry ice to the Institute of Animal Hygiene and Veterinary Public Health, Veterinary Faculty, University of Leipzig, Germany. Kittens’ sera were heat-inactivated at 56°C for 30 mins. Microtitre plates were prepared, inoculated, diluted, incubated and analysed as described by Rehme et al. 23 An anti-FPV titre <10 was regarded negative, anti-FPV titres ⩾10 were considered positive. Kittens with a ⩾four-fold titre increase were defined as ‘adequately responding to vaccination’. 24
Faecal examination
Owners of the kittens were instructed to collect three faecal specimens on three consecutive days 2 weeks after the first RCP vaccination (week 2) (Figure 1). Owners received tubes for faecal collection; faecal samples were sent directly by owners to the private Veterinary Laboratory Freiburg for parasitological examination. Each sample was analysed within 4–5 days after defecation.
The three samples from each cat were mixed thoroughly. Samples were examined by a conventional flotation method using 336 mg/ml zinc sulphate (ZnSO4) with a specific gravity 1.30 to concentrate eggs of helminths, oocysts from coccidia and cysts of Giardia species. In detail, approximately 5 g of faecal material were suspended with 15–20 ml ZnSO4flotation solution, sieved using a strainer (300 µm mesh aperture) into a 15 ml centrifuge tube until a convex meniscus was formed, covered with a cover slip and centrifuged (1500 g for 5 mins). After centrifugation, the cover slip with the supernatant floated material was transferred onto a slide and examined by light microscopy using magnifications of 100 × and 400 ×. In addition, all samples were analysed by a modified Baermann funnel technique to detect first-stage larvae (L1) of lungworms, as previously described. 25 Eggs of the genus Capillaria species were not differentiated owing to inadequate morphological characteristics.
Statistical analysis
Data were analysed using R statistical software version 3.6.3 (R Foundation for Statistical Computing). Pearson’s χ2 test was used to compare the following: (1) presence of pre-vaccination anti-FPV antibodies in week 0; (2) antibody responses of kittens (week 8 vs week 0); and (3) differences in occurrence of VAAEs between kittens with and without intestinal parasites after vaccination. The normality of data was examined using the Shapiro–Wilk normality test and the homogeneity of variance across groups was checked using the Levene’s test. Because of a mostly non-normally distributed data, the median and interquartile range were calculated to describe data, and the Mann–Whitney U-test was used to compare anti-FPV antibody titres between kittens with and without intestinal parasites. Results with a P value <0.05 were considered statistically significant.
Results
Prevalence of intestinal parasites
Two weeks after the first RCP vaccination (vaccination at 8–12 weeks, faecal collection at the age of 10–14 weeks), 17/74 (22.97%) examined faecal samples were positive for at least one intestinal parasite. Coinfection was observed in 2/17 (11.8%) kittens. The most commonly detected eggs were stages of T cati in 12/17 (70.6%) samples, oocysts of Cystoisospora felis in 6/17 (35.3%) samples and Capillaria species in 1/17 (5.9%) samples. Cysts of the Giardia species were not found in any of the faecal samples.
Response to vaccination
Tables 2 and 3 summarise the response to vaccination of all kittens. Of the kittens with intestinal parasites, 4/17 (23.5%) had pre-vaccination anti-FPV antibodies ⩾10 at week 0 (median antibody titre: 240; range 160–320). Post-vaccination anti-FPV antibodies ⩾10 at week 8 were detectable in 15/17 (88.2%) kittens with intestinal parasites (median antibody titre: 1280; range 10–5120). A ⩾four-fold increase after vaccination was detectable in 13/17 (76.5%) kittens (median antibody titre at week 0: 0 (range 0) and at week 8: 2560 (range 640–5120). No VAAEs were reported by the owners of kittens with intestinal parasites after the vaccination in weeks 0 and 8.
Comparison of the humoral immune response of kittens (n = 74) with and without intestinal parasites after modified live virus vaccination against feline panleukopenia virus (FPV) using Pearson’s χ2 test

Data are n (%)
Based on owner reports
Pre-vaccination anti-feline panleukopenia virus (FPV) antibody titre at week 0, post-vaccination anti-FPV antibody titre at week 8 and number of kittens with an at least ⩾4-fold titre increase when comparing week 8 with week 0
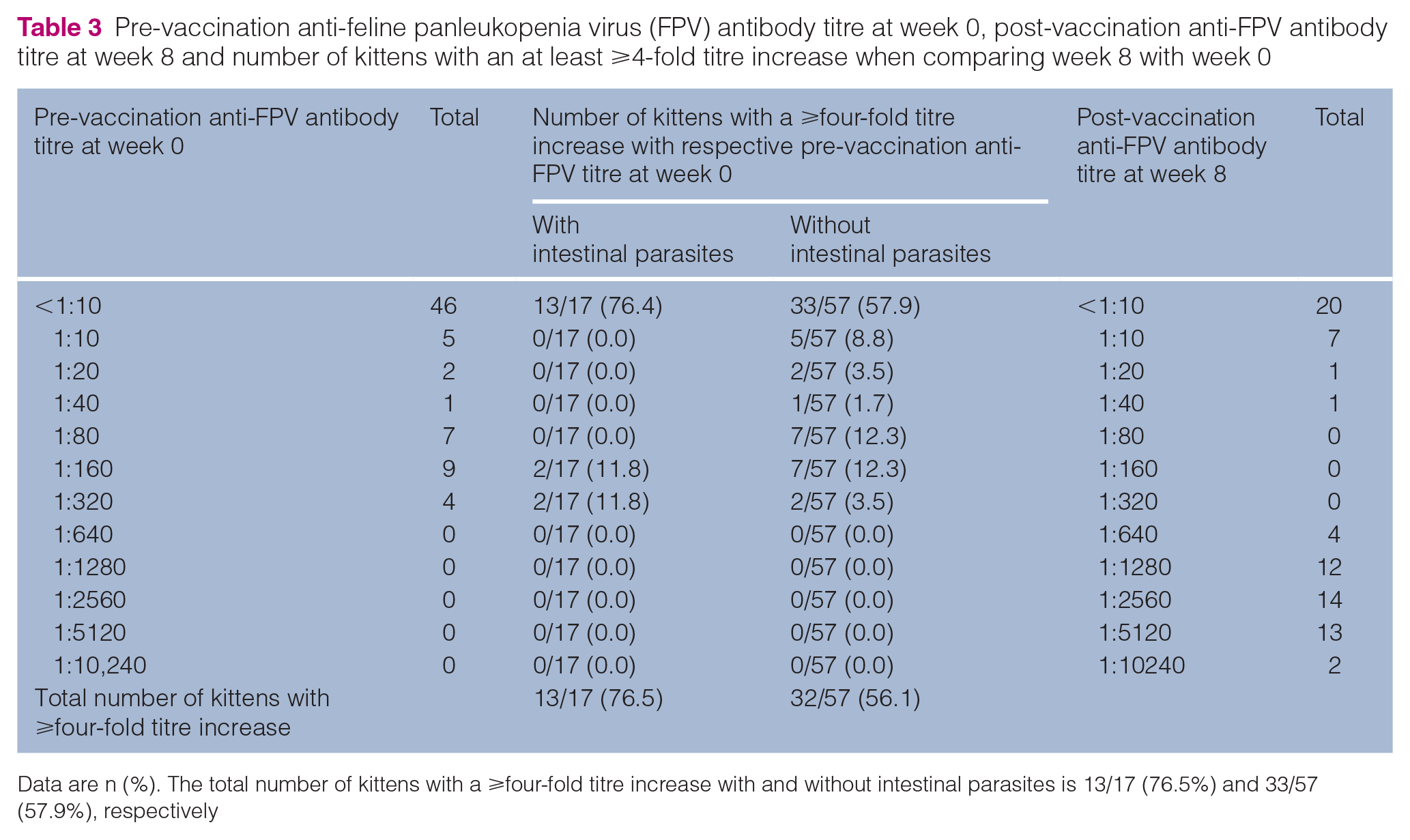
Data are n (%). The total number of kittens with a ⩾four-fold titre increase with and without intestinal parasites is 13/17 (76.5%) and 33/57 (57.9%), respectively
Pre-vaccination anti-FPV antibodies ⩾10 were present in 24/57 (42.1%) kittens without intestinal parasites (median antibody titre: 80; range 10–320). Post-vaccination anti-FPV antibodies ⩾10 at week 8 were detectable in 39/57 (68.4%) kittens without intestinal parasites (median antibody titre: 2560; range 10–10,240). Response to vaccination was observed in 32/57 (56.1%) kittens without intestinal parasites (median antibody titre at week 0: 0 [range 0–10] and at week 8: 2560 [range 640–10,240]). In 9/57 (15.8%; week 0: 8/57, week 8: 1/57) kittens without intestinal parasites, VAAEs were described by owners, including a slightly reduced general condition with reduced activity (n = 8) or mild gastrointestinal signs (n = 1) after vaccination for a few days.
Comparison between kittens with and without intestinal parasites
There was neither a significant difference in the presence of pre-vaccination anti-FPV antibody titres at week 0 (P = 0.17) nor in the presence of post-vaccination anti-FPV antibody titres at week 8 (P = 0.11) between kittens with and without intestinal parasites (Table 2). Furthermore, there was no significant difference in the response to vaccination (P = 0.13) (Table 2). In addition, the median anti-FPV antibody titres did not differ significantly between kittens with and without intestinal parasites neither at week 0 (P = 0.42) nor at week 8 (P = 0.61) (Figure 2). The occurrence of VAAEs in correlation with the response to vaccination was not significantly different in both groups (P = 0.08) (Table 2).

Comparison of the median anti-feline panleukopenia virus (FPV) antibody titres between kittens with and without intestinal parasites at week 0 and at week 8. (a) Anti-FPV antibody titres at week 0 before the first vaccination. Kittens with intestinal parasites (green; n = 17) and without intestinal parasites (orange; n = 57). No significant differences in anti-FPV antibody titres between the two groups were determined using the Mann–Whitney U-test (P = 0.42). (b) Anti-FPV antibody titres at week 8 (4 weeks after the second vaccination). Kittens with intestinal parasites (green; n = 17) and without intestinal parasites (orange; n = 57). No significant differences in anti-FPV antibody titres between the two groups were determined using the Mann–Whitney U-test (P = 0.61)
Discussion
Kittens are more often infected with helminths and protozoa than older cats,26,27 especially at the age of approximately 3 months, a time point at which the risk of infection increases (eg, with ascarids, coccidia and Giardia species). 26 To protect kittens from infection and the resulting gastrointestinal signs, regular deworming of queens and kittens is recommended by expert groups; 18 however, kittens are often presented for their first vaccination without being adequately dewormed. This raises concerns since intestinal parasites could influence the immune response to vaccination in infected kittens; yet postponing core vaccinations would pose a significant risk for kittens, especially for fatal feline panleukopenia.3,4
It is known that the immune system of cats suffering from chronic diseases (such as chronic kidney disease, neoplasia, long-term glucocorticoid treatment) is impaired. As shown previously, affected cats are more likely to lack antibodies against FPV compared with healthy cats and therefore might not be adequately protected against feline panleukopenia. 28
Various studies in mouse models10,29 –32 as well as in human medicine13,33 –35 found that an underlying helminth infection negatively affects the vaccination response.14,36 –38 The effectiveness of most vaccines is primarily achieved by stimulating the T-helper-1 (Th1) response within the host’s immune system while helminth infections promote mainly the Th2 immune response; mutual inhibition among Th1 and Th2 cells is thus the most likely explanation how helminth infections can influence the vaccination response.11,13,32,39 –41
There are only few studies in veterinary medicine about the influence of intestinal parasite infection on the immune system 15 and the response after vaccination.16,42 –44 Studies in cats have not been performed yet. Therefore, the present study is the first study that evaluated the antibody response to vaccination in kittens with and without intestinal parasites using FPV vaccination as a model. The results suggest that parasitic infections (at least with T cati, C felis and Capillaria species) do not interfere with the antibody response to FPV vaccination since there was no significant difference between post-vaccination anti-FPV antibody titres, response to vaccination and median anti-FPV antibody titres between infected and non-infected cats. This is in contrast to a study in dogs involving 14 puppies (aged 4 months) suffering from clinically manifest infection with T canis (8/8), T leonina (6/8) and/or T vulpis (2/8), which showed that the puppies had significantly lower anti-rabies antibody titres after vaccination than puppies from a non-infected healthy control group (6/14). Furthermore, immunosuppression in the infected puppies was confirmed by a functional phagocytes test and a lymphocyte proliferation activity test that revealed a significantly lower phagocytic activity and a significantly suppressed proliferation activity of lymphocytes. 16 A negative influence of intestinal infections on immune system activity in dogs has also been demonstrated by an older field study, which found a significant decrease of total immunoglobulin concentrations and number of neutrophilic granulocytes in client-owned dogs with giardiasis (6/28, 21.4%) in comparison with non-infected clinically healthy (client-owned and research) dogs. 15
The most likely reason for the contrary results between the above-mentioned study on puppies 16 and the present study could be the individual health status of the animals. Although all kittens from the present study were clinically healthy (unremarkable history, no gastrointestinal signs and healthy in physical examination), all infected puppies from the above-mentioned study had clinical signs, such as diarrhoea, poor growth rate and/or weak body condition. 16 In general, it is known that health status 28 as well as nutritional status 45 can be associated with an impaired immune response. On the other hand, the results of the present study suggest that parasitic intestinal infections per se do not automatically result in impaired antibody responses. This is comparable: (1) to a study on the antibody response to FPV vaccination in cats with asymptomatic retrovirus infections (FIV or FeLV); 46 and (2) to studies on the antibody response to canine parvovirus vaccination in dogs with underlying but well-controlled chronic diseases (eg, hypothyroidism 47 and hyperadrenocorticism 48 ). Therefore, it can be assumed that in the absence of clinical signs, the immune system appears to be able to respond adequately to FPV vaccination despite the presence of infectious agents or chronic diseases.
The type of vaccine is an important stimulus for the immune response to vaccination. The advantage of MLV vaccines is that they are able to replicate in the host49,50 and produce a stronger, long-lasting immune response when compared with inactivated vaccines.51,52 Therefore, it could be hypothesised that the modified FPV vaccine that was used in the present study induced an immune response in the kittens, while the puppies from the aforementioned study might have had a less pronounced immune response as they were vaccinated with an inactivated rabies vaccine. 16 Furthermore, it has to be considered that most of the previous studies revealing an influence of helminth infection on the vaccination response collected data for vaccinations against pathogens other than non-enveloped DNA viruses, for which a cell-mediated response is very important. In contrast, for non-enveloped DNA viruses, such as parvoviruses, an antibody response is more important. Thus, the type of pathogen for which the vaccination is against, and the immune response required to that pathogen, might influence whether a response to vaccination is affected by parasite burden.
A lack of detectable anti-FPV antibodies (<1:10) was observed in 46/74 kittens at week 0 (13/17 infected and 33/57 non-infected kittens; no significant difference between groups) and 20/74 kittens at week 8 (2/17 infected and 18/57 non-infected kittens; no significant difference between groups) (Table 2), which might be explained by the interference of vaccination with MDAs, since it is known that even low titres of MDAs can impede the antibody response with the consequence that no adequate protective titre after vaccination can be achieved. 53 Therefore, it can be assumed that MDAs had an influence on the antibody response in the present study. The results of the present study underline the importance of kitten vaccinations series at least up to 16 weeks of age as recommended by expert groups1,5 –8 to generate solid protection against FPV infection. An inadequate response due to individual genetic variations might be another reason (resistance to vaccination),50,54 which cannot be completely ruled out.
Vaccination in asymptomatic kittens infected with intestinal parasites did not result in a higher prevalence of VAAEs. A reduced general condition was the most commonly observed VAAE in the present study, which is commonly associated with the replication of MLVs (eg, FPV, FHV) in cats. 50 It could be assumed that parasite-infected kittens are more frequently affected by gastrointestinal VAAEs than non-infected kittens as a result of the replication of parasites and the additional vaccine virus replication in the gastrointestinal tract; 1 however, gastrointestinal VAAEs were very rare in the present study. In general, in other studies, it was also shown that asymptomatic, chronically ill animals did not have significantly more VAAEs than healthy controls.46 –48 As a result, kittens that do not show clinical signs of intestinal parasite infection (eg, abdominal pain, diarrhoea, nausea, malabsorption) 55 but have not yet been dewormed should still be vaccinated against important core components to minimise the risk of infections with high morbidity and mortality.
In general, intestinal parasites, particularly T cati, have a significant impact on the environment 56 and can affect the health of both cats and humans. 57 It should be noted that recommendations to vaccinate kittens without deworming do not contradict the deworming guidelines. Regular deworming is highly recommended, especially in outdoor cats. 18 Surveys from Germany and all over Europe revealed that many owners do not regularly deworm their cats (according to the recommendations of the ESCCAP group);58 –60 therefore, it is important that veterinarians provide individual deworming recommendations to owners. 18
A major limitation of the present study was that it investigated the antibody response in kittens under field conditions in which MDAs are commonly present.8,61 Thus, the results of the study were influenced by MDAs but this was the case for both the infected kittens and the non-infected controls. Another limitation of the present study was that only anti-FPV antibodies were measured as a correlate of protection. Cell-mediated immunity might also play a role in providing protection; therefore, an absence of an increase in antibody titre is not necessarily associated with a lack of protection. However, to prove true protection, challenge studies are needed, which cannot be performed under field conditions with privately owned cats.
Conclusions
Asymptomatic intestinal parasitic infections did not interfere with the antibody response to the kitten vaccination series. A parasitic infection (at least with T cati, C felis and Capillaria species) is therefore not a reason to postpone vaccination against important core components in clinically healthy kittens, such as vaccination against FPV. Nevertheless, veterinarians should continue to make owners aware about regular deworming strategies.
Footnotes
Acknowledgements
The authors thank Mrs Nadja Leinecker from the Institute of Animal Hygiene and Veterinary Public Health, University of Leipzig, for her expertise and processing the samples. We thank Boehringer Ingelheim and especially Jean-Philippe Tronel, Ingelheim Rhine, Germany for partially financing this study.
Author note
These results were presented as an abstract at the annual meeting of the European Society of Comparative Gastroenterology (EuroGut) in Edinburgh, UK, 2023 and at the annual Congress of the European College of Veterinary Internal Medicine (ECVIM) in Barcelona, Spain, 2023.
Conflict of interest
Parts of this research were funded by Boehringer Ingelheim, Ingelheim Rhine, Germany. Boehringer played no role in the collection and interpretation of data or in the decision to submit the manuscript for publication. There is no commercial conflict of interest of the authors as the information generated here is solely for scientific dissemination.
Funding
This research was partially funded by Boehringer Ingelheim, Ingelheim Rhine, Germany.
Ethical approval
The work described in this manuscript involved the use of non-experimental (client-owned) animals and procedures that differed from established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient. The study therefore had prior ethical approval from an established committee as stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.