
Abstract
Practical relevance:
Feline aortic thromboembolism (FATE) is commonly encountered in clinical medicine, especially in emergency situations. This often devastating syndrome usually develops secondarily to severe heart disease, and has short- and long-term consequences.
Clinical features:
The clinical presentation of FATE is consistent with peripheral ischemic neuropathy, usually in both pelvic limbs. Diagnosis is relatively straightforward, but can be assisted with Doppler ultrasound, point-of-care ultrasound or infrared thermal imaging.
Recent advances and future prospects:
Interpretation of survival rates in cats with FATE has been hampered by historically high admission euthanasia, but recent studies suggest a survival rate with supportive care of 30-40%. Moreover, with advances in post-FATE thromboprophylaxis, median survival times of over 1 year are being achieved. Future directions include use of thrombolytic agents and treatment of common FATE sequelae such as acute kidney injury and reperfusion injury.
Outline:
This article, aimed at small animal veterinarians, including emergency practitioners, reviews key aspects of the clinical presentation, diagnosis and treatment options for FATE, with a view to guiding client and veterinarian decision-making. Three case studies are included to illustrate the practical application of information presented in the review.
Evidence base:
There are limited prospective studies on FATE, although the recent literature reflects a resurgence in clinical research interest in the past few years. Advances in FATE treatment will benefit many cats and it is important that research efforts continue to identify appropriate treatment modalities.
Introduction
Feline aortic thromboembolism (FATE), also known as 'saddle thrombus', is probably the most common form of thromboembolism seen in clinical veterinary medicine.1,2 It is initiated by the sudden migration of a left atrial thrombus into the systemic arteries, and its prevalence has been reported as 1/175 cases in a tertiary US veterinary center, 1 and 1/379 cases in UK general practice. 3 FATE is a devastating syndrome, with short-term consequences characterized by acute pain, paralysis and rhabdomyolysis in the affected limb(s). 2 FATE also has long-term implications, as many patients are suffering from severe cardiac disease, and recurrence of the syndrome is common.1-3 After several decades that have seen a lack of scientific progress, more data have been published on FATE in recent years, informing on progression, prognosis and treatment options for cats with this clinical syndrome.
Overview of causes of arterial thromboembolic disease
The major cause of FATE is cardiomyopathy, accounting for 90% of cases.1-3 However, and despite a median age of 8-12 years at diagnosis of FATE, only 20% of cats have a known cardio-myopathy at the time. 1 In other words, in 80% of cases, FATE is the first clinical manifestation of cardiomyopathy. It has been shown that around 25% of cats with hypertrophic cardiomyopathy (HCM) will develop FATE. 4 As male cats are predisposed to cardiomyopathy, it is common for FATE cats to be male (75% of cases).1-3
In approximately 10% of cats with FATE, the cause of the thromboembolism is non-cardiogenic. Neoplasia represents the second most common cause of FATE, with pulmonary neoplasia dominating that category. Other, less common causes of feline thromboembolism include infection, inflammatory disease, hyperthy-roidism and administration of corticosteroids or progesterone agonists. 5
Clinical presentation
The clinical diagnosis of FATE is relatively straightforward, with signs mostly consistent with peripheral neuropathy (Figure 1). In approximately 70-75% of cases, both pelvic limbs are involved, whereas 10-15% of affected cats have only one pelvic limb involved; the remaining cases have either right or left forelimb involvement.1-3

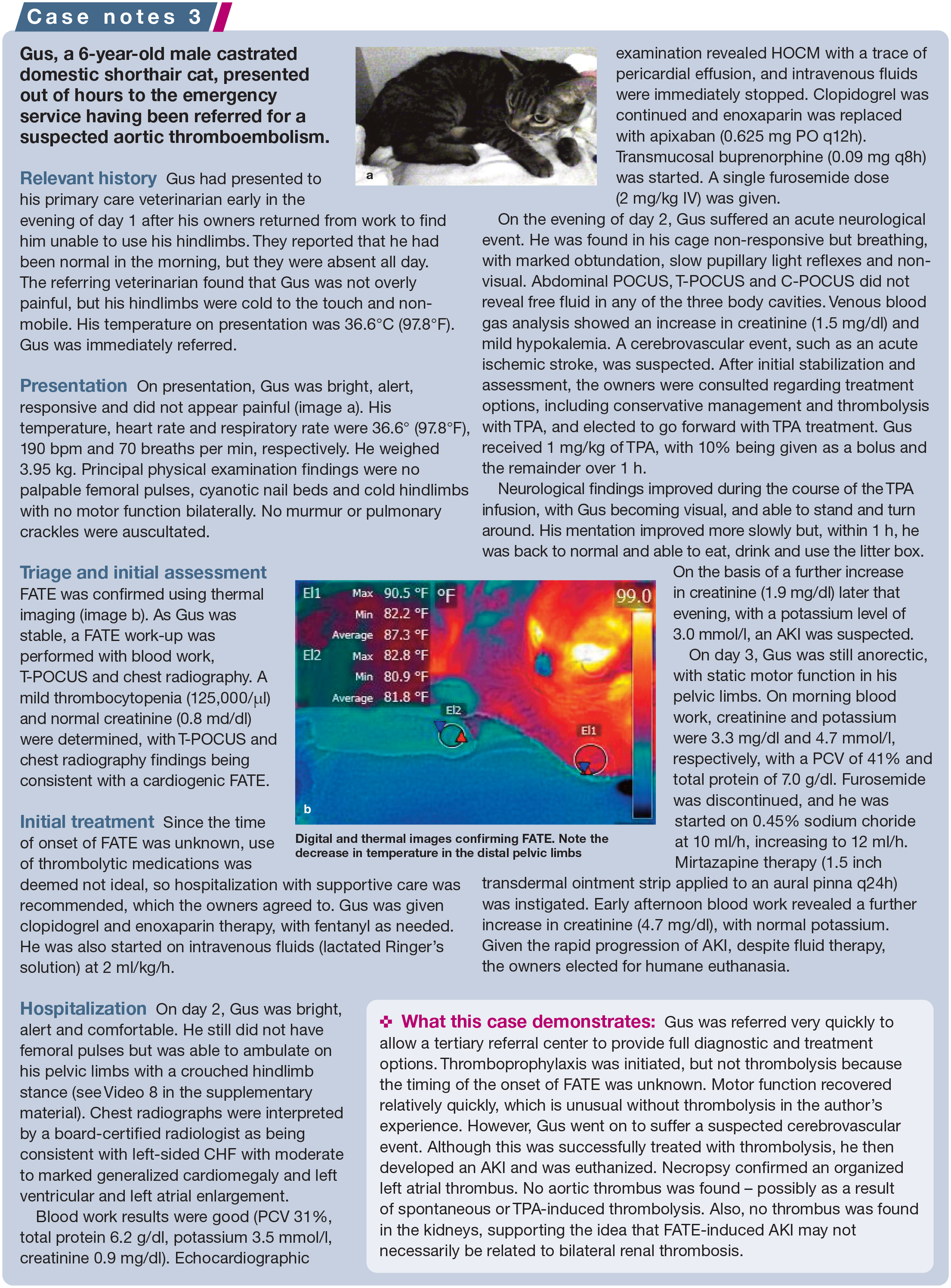
Paralysis in an 11-year-old male castrated domestic shorthair cat with feline aortic thromboembolism (FATE). Note the position of the pelvic limbs. A fentanyl constant rate infusion is being used to manage pain in this patient
Most clinicians diagnose FATE on physical examination using the '5P rule', which characterizes the presenting signs of pallor (ie, purple, cyanotic or pale toes; Figure 2), polar/ poikilothermy (ie, cold extremities), pulselessness, paralysis/paresis and pain. Findings using diagnostic tools include: absence of Doppler flow; direct visualization of a thrombus on ultrasound, infrared thermal imaging or angiography; and a low glucose or high lactate measurement in the affected limb(s) compared with normal limbs.2,6,7 Infrared thermography can also be used to assess reperfusion in affected limbs.

Close-up view of one of the paws of the cat pictured in Figure 1. Note the purple/pale discoloration of the paw pads
As mentioned, 80% of cats with FATE have a hitherto unrecognized cardiomyopathy as a cause of the thromboembolism,1-3 and so it is important to assess for signs of cardiac disease and congestive heart failure (CHF), such as dyspnea, pulmonary crackles and cyanosis. CHF is present in around 50-70% of cats with FATE,1-3 but is not associated with a worse prognosis. Cardiac auscultation abnormalities such as a murmur or gallop rhythm are identified in two-thirds of cases. It is not uncommon (ie, 10-20% prevalence) for vomiting to occur in cats prior to presentation with FATE.1,3
Diagnostic testing
Once a diagnosis of FATE has been established, it is important for the clinician to thoroughly assess the cat for comorbidities. Bedside echocardiography, or cardiac point-of-care ultrasound (C-POCUS; see box), can confirm the presence of a cardiogenic origin of FATE (ie, CHF), and can suggest the presence of a cardiomyopathy. C-POCUS is a screening test and is not a replacement for a complete echocardiographic examination performed by a trained cardiologist. 8 It lacks detailed information on heart morphology and function, and may fail to detect all cardiac abnormalities. It can nevertheless provide emergency clinicians with information that is useful both for treating the cat and for client education.
The author recommends using C-POCUS and thoracic POCUS (T-POCUS) for rapid assessment of cardiac and thoracic structures. Chest radiography can be performed upon stabilization to assess for the presence of CHF or pulmonary neoplasia.
Baseline blood work (chemistry panel or venous blood gas analysis) is important to establish renal values and assess for renal dysfunction and/or early reperfusion. Findings may include azotemia, elevated creatine kinase, hyperkalemia and metabolic acidosis. Testing can be performed relatively quickly and without sophisticated equipment, and parameters should be serially monitored every 6-12 h during hospitalization.
Prognosis
The prognosis for cats with FATE has traditionally been considered poor, but 'poor' is rarely defined. FATE also has been associated with euthanasia rates as high as 90%, which seem to be clinician- or clinic-related.1,3,9 A recent prospective multicenter investigation of cats with bilateral pelvic limb paralysis (the BLASTT study) reported an overall 37.5% discharge rate, with a 95% confidence interval of 22.5% to 52.5%, with some cats experiencing >1 year survival. 2 This aligns with findings from retrospective studies, which have shown a survival rate of between 27% and 45% for cats suffering from bilateral FATE;1,3,10-13 however, interpretation of findings is hampered by vastly different inclusion criteria (ie, one limb affected vs bilateral syndrome), in-hospital treatment, medications dispensed at discharge and outcome data between different retrospective studies.1-3,11,12,14-16 It should be noted that, despite most studies having been conducted in university settings or referral hospitals, mortality of cats hospitalized or treated for FATE remains high.2,9,15


When considering the prospects for patients (see 'Prognostic factors' box), it is again important to note that, until recently, studies have mostly been retrospective in nature; and, while some have identified outcome factors, many reported non-survivor admission characteristics, which differ from actual prognostic factors. Moreover, while euthanasia rates had been increasing over the past few decades -the rationale being that treatment options were limited, and both the short- and long-term prognosis was very poor - more recent research investigating thrombolysis and long-term treatment options has challenged this notion.2,9,15,16 If the cat survives the FATE episode and can be discharged with appropriate oral medica-tions, 15 long-term survival may be much higher than previously thought. Indeed, retrospective studies have shown that survival times after discharge could be up to 350-500 days, with the use of rivaroxaban and clopidogrel producing the highest survival times and lowest re-embolization rates.1,4,11,15 Thus, in facilitating decision-making, veterinarians must ensure each client has a fair understanding of the causes of FATE, long-term prognosis (especially with cardiac disease) and treatment options, including the impact of thrombolysis, thrombo-prophylaxis and euthanasia on the natural course of disease.

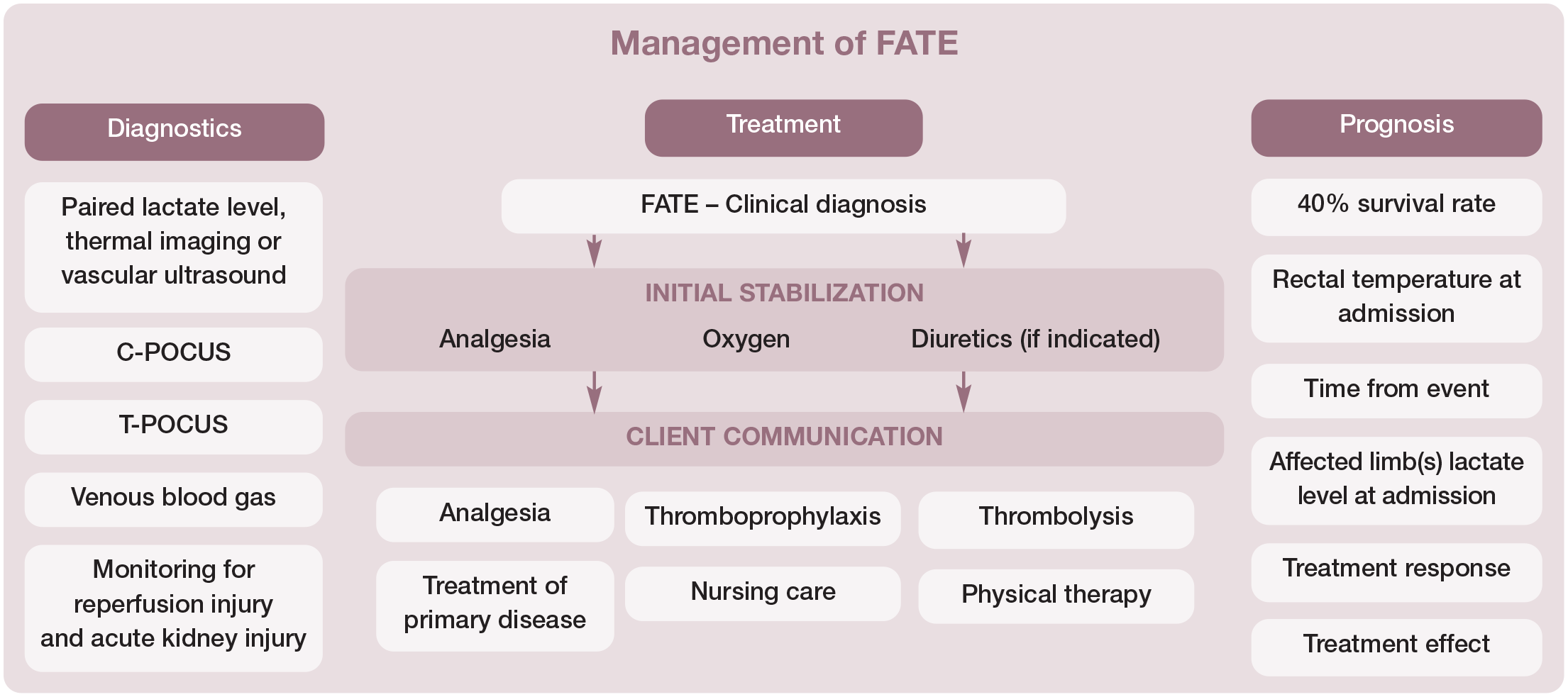
Emergency treatment
Emergency treatment of FATE revolves around analgesia, treatment of the primary disease (eg, HCM), nursing care and throm-boprophylaxis, and may also include thrombolysis and promotion of the collateral circulation (see Table 1 and 'Management of FATE' algorithm).
Medical treatments for FATE
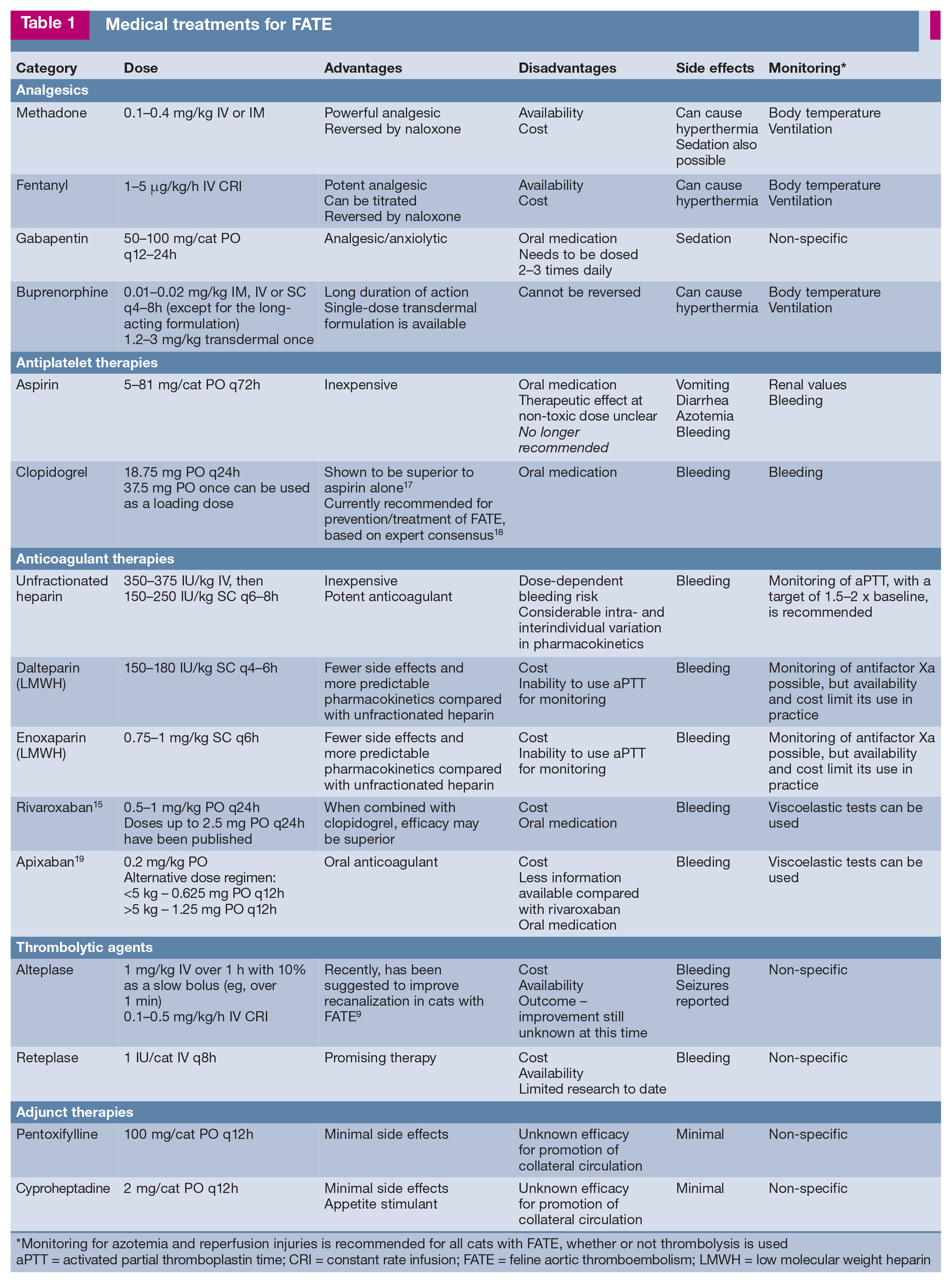
Monitoring for azotemia and reperfusion injuries is recommended for all cats with FATE, whether or not thrombolysis is used
aPTT = activated partial thromboplastin time; CRI = constant rate infusion; FATE = feline aortic thromboembolism; LMWH = low molecular weight heparin
Analgesia
Pain control is important for FATE patients. Analgesia with a pure [i-agonist is recommended, and the author's preference is initial treatment with methadone, followed by a constant rate infusion (CRI) of fentanyl (1-5 [ig/kg/h IV), titrated to effect (Table 1). Other opioids, such as oxymorphone, hydromor-phone or buprenorphine, can be used if the preferred options are not available. Many cats arriving very distressed and in obvious pain can readily be managed with short-acting opioids, which allows for further investigation and stabilization, and client communication. After initial stabilization, and ideally in the light of objective measures (eg, Feline Grimace Scale),20-22 additional sedation, analgesia and anxiolytics may be needed.
Treatment of primary disease
Assessment of the cat for cardiac disease and the presence of CHF is important for emergency stabilization. The majority (ie, 90-95%) of FATE patients are suffering from cardiac disease, including HCM and hypertrophic obstructive cardiomyopathy (HOCM), with 50-70% of patients having concurrent CHF.1,3 Therefore, treatment of cardiomyopathy and CHF should be instituted, where appropriate. 23
Treatment of cardiac disease and CHF involves oxygen supplementation, judicious use of furosemide, and oxygen therapy; other cardiac treatments may be warranted. Readers are referred to consensus guidelines on cardiomyopathies from the American College of Veterinary Internal Medicine for further information. 23 The recommendation that furosemide be used judiciously relates to the fact that many cats with FATE are dehydrated on presentation; overly aggressive use of diuretics can worsen a pre-renal component of acute kidney injury (AKI).
The author recommends assessing renal function with venous blood gas analysis or a biochemistry panel at admission and closely monitoring renal values. The need for diuretics and control of CHF should be carefully balanced in cats with pre-existing azotemia or even borderline high creatinine values.
Thromboprophylaxis
Anticoagulant therapy is recommended to decrease the risk of the thrombus worsening. Options include unfractionated heparin (UFH), low molecular weight heparin (LMWH), aspirin, clopidogrel or a novel oral anticoagulant such as rivaroxaban or apixa-ban (Table 1).
The Consensus on The Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE) guidelines, published in 2019, provide current recommendations for a cat with cardiac disease and acute FATE. 18 Although comprising mainly expert opinion rather than evidence-based recommendations, the CURATIVE guidelines suggest that administration of clopidogrel in combination with LMWH can be considered in cats at risk of FATE. The recommendation would be clopidogrel (18.75 mg PO q24h) and one of the LMWHs, dalteparin or enoxaparin (Table 1). Enoxaparin in cats can be used at a dose of 0.75-1 mg/kg SC q6h to reduce inter-individual variation in peak anti-Xa activity. 18 Recently, based on results from the FAT CAT 17 and SUPER-CAT studies (B Brainard, personal communication, 2023) and a retrospective investigation from Lo et al, 15 a combination treatment with clopidogrel and rivaroxaban/ apixaban appears to be the preferred long-term treatment option.15,24
See the box 'Thromboprophylaxis: summary of guidance' and the later section 'Prevention of future episodes of FATE' for further information and discussion.
Thrombolysis
Recent expert consensus has suggested that thrombolytic agents can be considered for treatment of acute (<6 h duration) FATE following an assessment of the risks and benefits in individual cats. 27 Evidence available for inclusion in the systematic review leading to this consensus guidance included:
✜ A 1987 abstract involving six cats from the University of California, Davis, where TPA was used at 0.25-1 mg/kg/h IV as a CRI, providing a total of 1-10 mg/kg. The discharge rate from the hospital was reported as 43%, but included 3/6 cats (ie, 50%). 13
✜ A 2010 uncontrolled prospective study investigating the TPA alteplase in 11 cats with FATE. 28 Cats were enrolled within 12 h of the onset of clinical signs, and an additional TPA dose was administered to 36% of cases (4/11 cats). In 6/9 (67%) cats, there was return of pulses and improved limb function, although only three (27%) of the 11 cats were discharged from the hospital.
✜ A 2019 retrospective study comparing a thrombolysis group receiving the TPA alteplase (n = 16) with a robust control group treated without thrombolysis. It showed no worsening in survival rate, as well as similar complication rates (ie, AKI and reperfusion injury), between the groups. 29
Since the consensus guidance was published, the earlier mentioned BLASTT study, a prospective, randomized, placebo-controlled investigation using alteplase for FATE, showed a survival to discharge rate of 45% for the TPA group and 30% for the placebo group, though the study lacked power to detect a statistical difference. 2 In 2022, a relatively large retrospective study comparing TPA-treated cats with non-TPA-treated cats, published as an abstract, showed a positive impact of thrombolysis on functional recovery and arterial recanalization. 9 However, TPA did not provide a survival benefit in that study, and the reported overall survival was approximately 35%. 9 Finally, another abstract published in 2022 reported a 90% survival to discharge rate for cats with bilateral FATE receiving reteplase (a third-generation TPA). 16
Most studies use a treatment regimen for thrombolytic agents similar to the one for acute ischemic stroke: a total dose of 1 mg/kg, with 10% of the dose administered as a slow bolus, and the rest over 1 h.2,9,29 In pediatrics, a CRI at a dosage of 0.1-0.5 mg/kg/h is used, with careful monitoring of reperfusion and complications. 30
Nursing care
Nursing care is extremely important for cats with FATE. Physical therapy involving passive range of motion and leg warming can be attempted if tolerated by the patient. Hospital stays are usually 2-5 days but, based on early reports of clinical FATE, 31 an interval of 2-6 weeks is to be expected before seeing improvement in neuromuscular function and ambulatory ability in cats exhibiting spontaneous resolution. Moreover, distal extremity necrosis, dry gangrene and muscle retraction may develop in some cats (around 5% of cases 31 ) showing initial spontaneous resolution (Figure 5), necessitating amputation. Attention to nutrition, elimination and stress reduction is vital for optimal recovery.

Self-mutilation 3 months after recovery from FATE. The cat, who suffered from severe cardiomyopathy, underwent pelvic limb amputation and recovered well
Ancillary treatments
Complications, especially AKI and reperfusion injury, develop frequently (see 'Ongoing care'), regardless of whether thrombolysis is attempted. In terms of AKI, it is now believed that bilateral renal thrombosis is uncommon, and we know that the clinical syndrome of FATE can be induced with vasoconstricting agents without a physical clot.2,32 Therefore, the focus of the next step in research on FATE is to investigate drugs to promote the development of collateral circulation, such as vasodilators and/or antioxidants.
There are several candidates. Pentoxifylline is an antioxidant, anti-inflammatory drug and vasodilator with red blood cell deformability (ie, rheology) properties.33,34 Cyproheptadine, when administered before thrombus formation, preserves collateral circulation and prevents paralysis; this drug is a serotonin antagonist and antihistamine, and is commonly used as an appetite stimulant.35,36 Other potentially useful agents include cilostazol, an antiplatelet drug and vasodilator, and flunar-izine, a calcium channel blocker.
Ongoing care
Ongoing care for a cat following a FATE episode may be best suited to a 24/7 veterinary facility with solid expertise in nursing care and a multispecialty medical team. Indeed, studies on cats with bilateral FATE have shown that they commonly suffer from complications such as reperfusion injury (20-50% prevalence) and AKI (30%), regardless of whether thrombolysis is attempted.2,29 Sudden death is relatively uncommon (10-15%) and usually occurs during the first 12 h. 2

Approximately 40% of cats with FATE who develop complications will survive if appropriate treatment is instituted. 2 The author recommends monitoring kidney function and potassium values early and serially in order to identify possible complications and treat accordingly, possibly by adjusting the diuretic dose. Intravenous fluids may be needed to manage AKI if it develops during treatment, and can be challenging to balance with cardio-myopathy. It should be noted that, although AKI in FATE cases has traditionally been thought to be due to thrombosis of one or both renal arteries, chronic renal infarction was the most common renal abnormality observed at necropsy in the BLASTT study. 2 This information, coupled with the relatively high packed cell volume (PCV) and total protein levels seen at admission in cats with FATE, raises the question of whether pre-renal azotemia or exacerbation of chronic renal disease is the main cause of AKI in FATE cases. Therapeutic measures such as judicious fluid therapy, careful use of diuretics or venodilator (eg, cilostazol) treatment may warrant consideration. It is possible that such complications may be mitigated with drugs targeted at vasodilation, antioxidation and development of collateral circulation such as pentoxifylline or cyproheptadine.33,35 As mentioned, further studies are needed to investigate the potential benefits of these medications.
If FATE is treated, cats usually improve within 24-48 h in terms of their ambulation status and/or the presence of pulses. However, some studies have shown that only 50% of cats with FATE will survive 48 h, so a survival bias is probable, whereby cats who improved survived, whereas cats who did not improve or developed complications may have been euthanized. 2 If an improvement is not noted within 24-48 h, the long-term prognosis and options such as amputation and/or devices for ambulation assistance should be discussed. 37

Prevention of future episodes of FATE
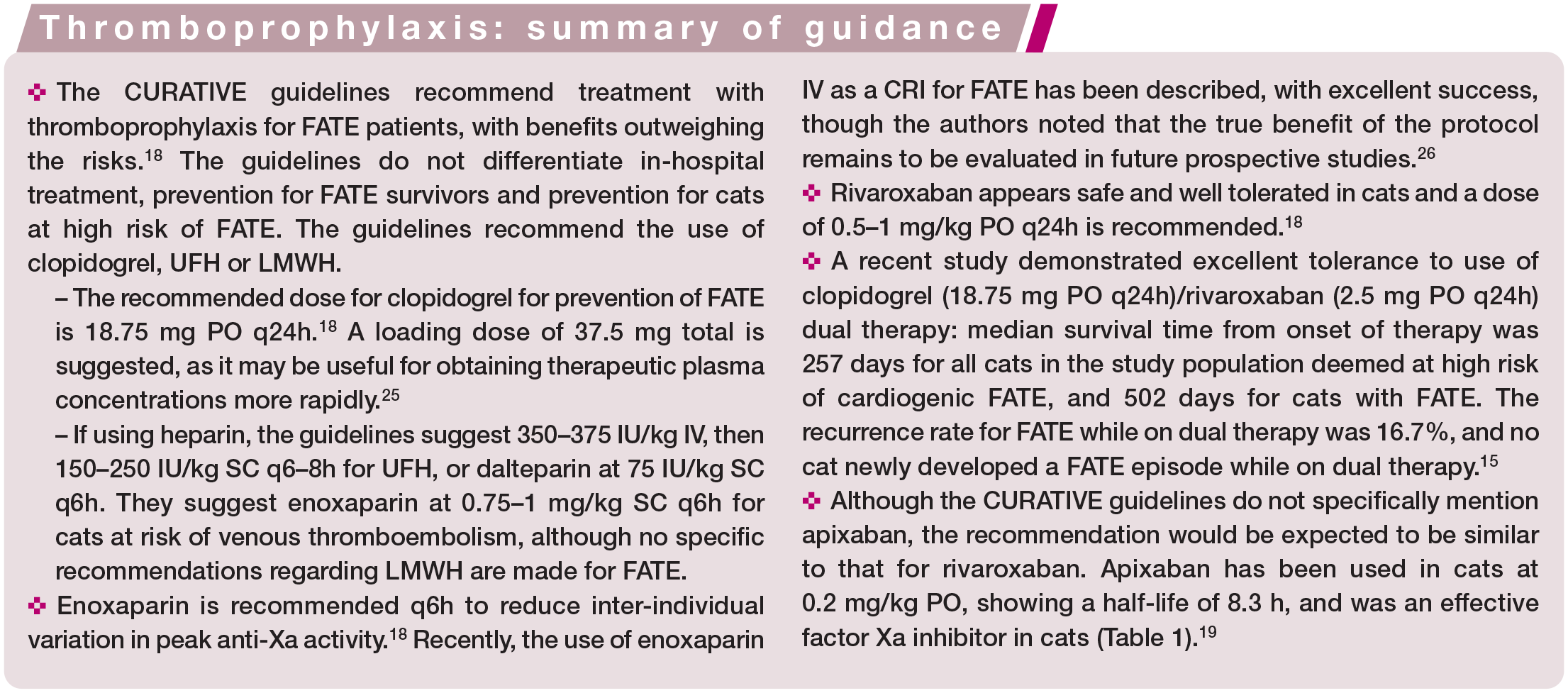
The ideal long-term management for cats with FATE is unclear at this point. The CURATIVE guidelines, which as mentioned do not differentiate between hospitalized patients, FATE survivors or cats at high risk, recommend long-term use of clopidogrel, UFH or LMWH. The recommended dose for clopidogrel for prevention of FATE is 18.75 mg PO q24h. 18 If using heparin, the guidelines suggest an initial SC dosage for UFH of 250 IU/kg q6h or dalteparin at 75 IU/kg SC q6h. Finally, rivaroxaban appears safe and well tolerated for long-term use in cats, with a recommended dosage of 0.5-1 mg/kg PO q24h. 18
These recommendations were mainly based on the FAT CAT study, a multicentric, prospective, randomized investigation published in 2015, 17 as well as expert opinion. The FAT CAT study demonstrated that clopidogrel was superior to aspirin for prevention of recurrence of FATE, as well as for overall survival. However, a criterion for enrollment into the study was a cardiogenic FATE that had been stable for between 1 and 3 months. 17 Since then, the SUPER-CAT study, a similarly designed investigation comparing clopidogrel with rivaroxaban, has been performed, with preliminary results presented at the 2023 American College of Veterinary Internal Medicine (ACVIM) forum (B Brainard, personal communication, 2023). In that study, there were no statistically significant differences in the recurrence rate of FATE between rivaroxaban (median 513 days) and clopido-grel (median 663 days), nor in the median time to death between rivaroxaban (296 days) and clopidogrel (335 days).
In recent studies, cats with FATE and cardiac thrombi or 'smoke' present in the left atrium showed an excellent response to the use of clopidogrel/rivaroxaban dual therapy, with a synergistic effect being noted between the two drugs.15,24 Median survival time from the initiation of therapy was 257 days for all cats, and 502 days for cats with FATE. The FATE recurrence rate in cats on dual therapy was 16.7%, while no cat newly developed FATE while on dual therapy. 15 On the basis of these findings, it seems logical to adopt a dual therapy approach using clopidogrel and a novel oral anticoagulant such as rivaroxaban or apixa-ban, although more research is need to assess clinical efficacy more broadly.
Key Points
✜ FATE is a syndrome that warrants reconsid eration by the veterinary community.
✜ Recent years have seen advancements in preventive as well as in-hospital treatments, including thrombolytic therapies and promising thromboprophylactic treatments.
✜ Although the prognosis should remain guarded, there are now options available to clinicians for the treatment of FATE. Approximately 40% of cats will survive, with some single centers reporting 80–90% survival rates for bilateral FATE, and prospective and retrospective studies showing median survival times of up to 500 days.
✜ Treatment of cats with FATE nevertheless remains challenging and complications are common. A team approach to decision-making involving the client is important.
Footnotes
Supplementary material
✜ Video 1: Right parasternal short-axis ventricular ('mushroom') view in a cat with HCM. Courtesy of Kaitlin Abbott-Johnson.
✜ Video 2: Right parasternal short-axis view at the level of the heart base showing an increased LA:Ao ratio in a cat with HCM. Courtesy of Kaitlin Abbott-Johnson.
✜ Video 3: Right parasternal long-axis view showing the right ventricle and right atrium in the near field, and left atrium and left ventricle in the far field, in a cat with HCM. Courtesy of Kaitlin Abbott-Johnson.
✜ Video 4: Cat (featured in 'Case Notes 2') at admission showing clinical signs of FATE. Videos 5-7 document the clinical progression.
✜ Video 5: Full echocardiography performed on the cat in Video 4 shows severe HCM with spontaneous echo contrast and two organized thrombi in the left atrium.
✜ Video 6: Clinical signs and ambulation status in the cat in Videos 4 and 5, at 6 h post-thrombolysis with TPA.
✜ Video 7: Clinical signs and ambulation status in the cat in Videos 4-6, at 72 h post-thrombolysis with TPA.
✜ Video 8: Cat (featured in 'Case Notes 3') ambulating on his pelvic limbs after treatment with supportive care without thrombolysis.
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in ]FMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.