
Abstract
Series outline
This is the second part of a two-part series on spectrum of care that encourages practitioners to tailor case management to the patient along a continuum of acceptable options. Part I defined the spectrum of care and broadened its approach beyond initial cost-of-care considerations. This second article introduces strategies for initiating conversations with clients about their needs, wants and expectations specific to healthcare options and case management decisions. It will explore how open inquiry, reflective listening, transparency and unconditional positive regard facilitate dialogue between providers and their clients as they collaborate on decision-making along a spectrum of care.
Relevance
Contextual case management prioritizes interventions that are appropriate for both the patient and the client. To identify and explore which healthcare options represent the best fit for those impacted most by medical decisions, veterinarians need to make space for clients to feel comfortable sharing their perspectives. Clients are more likely to be engaged in decision-making when their insight is actively solicited. They have much to share with us as experts about their cat’s overall health and wellness needs. Inviting clients to contribute to the consultation and being receptive to hearing what motivates their choices helps us to structure conversations around healthcare options. The ability to communicate healthcare options is as vital as the provision of healthcare, if not more so.
Keywords
Introduction
Socioeconomic, geographic and health literacy barriers obstruct healthcare delivery.1–7 Spectrum of care is an approach to the practice of medicine that addresses barriers to positive patient outcomes.3,8–12 Spectrum of care was defined in part I 13 as the practice of customizing care based upon case-specific factors that involve the client, veterinarian and patient (Figure 1).3,8–10,12
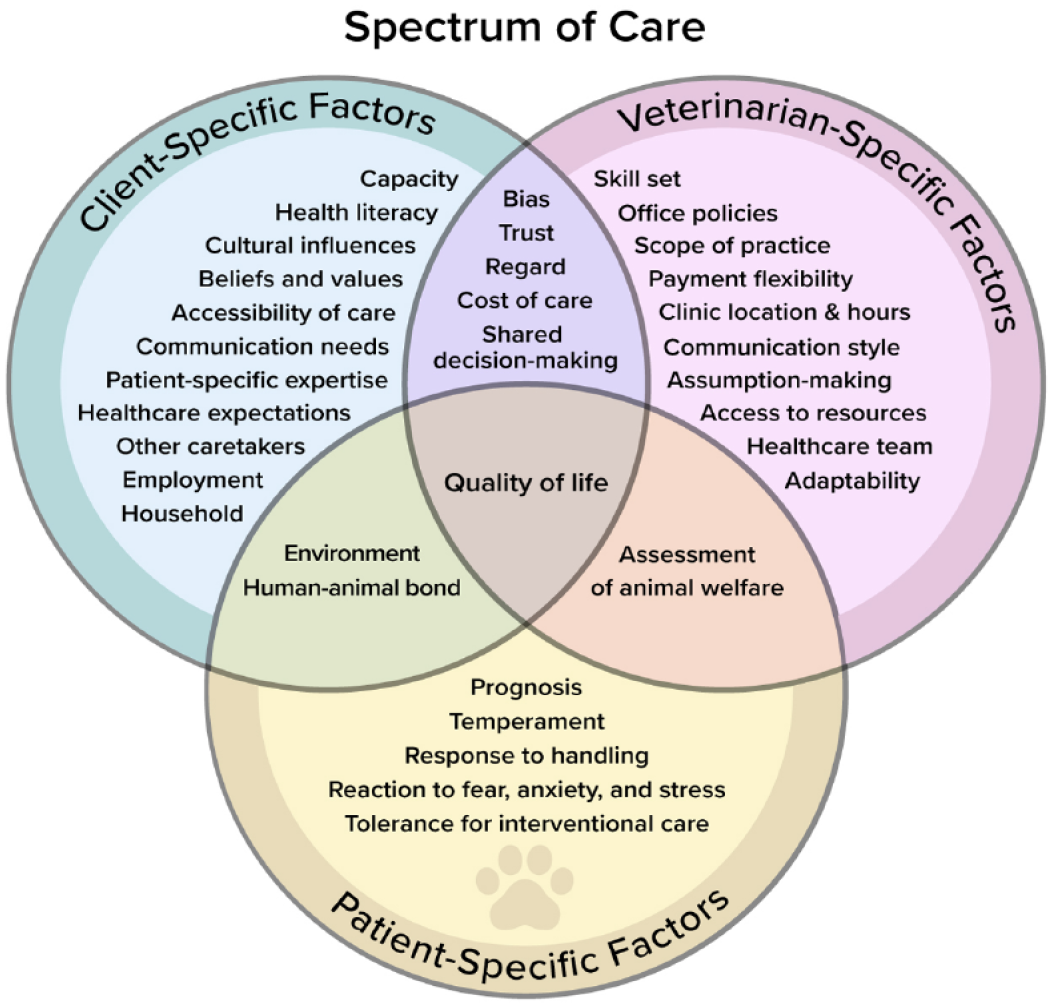
Client-, patient- and veterinarian-specific considerations that factor into the spectrum-of-care approach to the practice of veterinary medicine
By offering a continuum of acceptable options for case management based upon the growing evidence base in the veterinary medical literature, veterinarians can provide contextualized care that is considerate of client needs, wants, expectations and limitations.8,9 Healthcare providers must be able to offer options that they believe are viable and in the best interest of the patient. 9 One challenge that veterinarians face with respect to initiating conversations about a Plan A, B and C approach to patient care is the possibility of being burned by adopting an incremental approach to care. They may fear the possibility of missing a diagnosis in a patient that would have become apparent if they had just performed ‘x’ additional testing. Concern about whether incremental care invites liability may prompt veterinarians to routinely perform extensive testing, even if doing so has little chance of detecting something that could alter case management.
A second challenge that veterinarians face is the exponential rise in an ever-evolving body of knowledge, and the ongoing struggle to stay current. 14 When information is not easily accessible, veterinarians may continue to practice as they were taught. For example, veterinarians unfamiliar with the 2019 report by the International Society for Companion Animal Infectious Diseases may continue to advise clients to culture urine after completing antibiotic therapy for a simple urinary tract infection.14,15 Old practices die hard and the veterinary profession tends not to challenge dogma. 14 Efforts to increase the visibility of updates in research have led to the creation of resources that support a spectrum-of-care approach, including the Evidence-Based Veterinary Medical Association, 16 Royal College of Veterinary Surgeons Knowledge 17 and the University of Nottingham’s Centre for Evidence-Based Veterinary Medicine. 18
Access to new information about the efficacy of alternative healthcare options is insufficient to drive the spectrum of care forward. Options must be communicated to the client in a way that provides context as well as a detailed account of pros and cons, expected and unexpected outcomes, anticipated impact on patient diagnosis and prognosis, the cost:benefit ratio and what next steps should be taken if the patient requires additional support. 9
Exploring options with clients has historically been challenging for the veterinary profession. 14 One-fifth of veterinarians who participated in a large-scale study in 2018 disclosed that they did not offer treatment alternatives to owners of underserved pets. 1 Of the veterinarians who participated in a 2022 cross-sectional study, 30% disagreed that ‘all treatment options should be presented to owners’. 19 Which options are introduced by veterinarians to clients and how information is presented influence the direction of the consultation. 14
The emergence of communication as a key influencer in the consultation room
Research in human healthcare demonstrates that patients are guided by doctors’ recommendations,20–24 and it is thought that veterinarians exert the same influence.9,14 Options should be presented by the provider without allowing assumptions to influence information disclosure. 14 The veterinary client deserves to be informed of diagnostic and therapeutic modalities, the costs of associated care, anticipated follow-up, expected patient outcomes, the benefits of treatment and the potential for adverse effects.9,14 Evidence must be provided to support forward action so that the client can make informed decisions. 14 Dialogue is central to decision-making because it allows different perspectives to be shared and opportunities to clarify questions or misconceptions. In this way, dialogue provides the scaffolding for both informed consent and shared decision-making (SDM).14,25 SDM occurs when ‘clinicians and patients make decisions together using the best available evidence’. 26 This approach is not new to healthcare. Medical publications about SDM date back at least as far as 1980, when Schain acknowledged that ‘the vision of the parental physician as unilateral authority. . . is dimming. The picture is being supplanted by a new image. . . of personalism and a concept of “shared responsibility”’. 27 It was believed that collaboration between provider and patient could improve healthcare satisfaction. 27
Recent research suggests that SDM also drives veterinary client satisfaction with services. 28 However, past studies assessing veterinarian–client–patient interactions using the Roter Interaction Analysis System have demonstrated that veterinarians tend to monologue in the consultation room and underutilize communication skills that contribute to client engagement and partnership.29–31 If we are to empower clients with SDM, then we must lean into communication skills that encourage clients to share their perspectives and priorities with respect to healthcare delivery. 32
Communication was once considered a ‘soft skill’ in healthcare 33 that was not seen as influential in shaping patient outcomes.34–36 This perspective pervaded medical education until the 1980s, when research on healthcare satisfaction demonstrated that human patients valued displays of care and compassion by physicians more so than content area expertise.37,38 When patients felt that providers communicated effectively, they were more likely to be compliant and experience improved physical, physiologic, mental and emotional health outcomes.34,38–44
The veterinary profession has been slower to embrace communication skills training.33,34,45–48 Veterinarians assumed that on-the-job training would develop essential interpersonal skills. 45 Subsequent research demonstrated that a significant fraction of board complaints against veterinarians are communications-based49–52 and that many veterinarians are challenged by clinical conversations45,53–58 about cost of care, 59 inappropriate client behavior, 60 patient weight 61 and dietary modifications. 62 Workplace stress is often exacerbated by ineffective communication between team members,63–65 and has been magnified by the COVID-19 pandemic.66–68
Today’s veterinary clients expect to be included as team members in the delivery of healthcare.34,35,38 Clients seek acceptance as part of the healthcare team.33,69 They want their voices to be heard.33,69 Nowhere is their insight more critical than during times of decision-making in contextualized care, when a continuum of acceptable options is explored.
Communication strategies to navigate spectrum-of-care clinical conversations
Spectrum of care offers a unique lens through which to understand the dynamics of the veterinarian–client–patient relationship (VCPR). Spectrum of care invites the clinician to transition from their ‘sage on the stage’ role to a ‘guide on the side’. 5 Spectrum of care embraces a team approach to healthcare delivery and the client is central to that team. At the end of the day, it is about relationships and how to engage the caregiver in dialogue about how best to approach cat care. This requires a bilateral transfer of information, with an opportunity for all to share and clarify their understanding of each other’s point of view so that they are on the same page about moving forward. To achieve this degree of mutual understanding, strategic implementation of select communication skills is invaluable. Over 70 communication skills have been identified within the Calgary-Cambridge Guide (CCG), a consultation model that was adapted from Silverman, Kurtz and Draper’s collective work in human healthcare70,71 for use in veterinary medicine by Radford et al 50 in 2003. Two of these skills are particularly relevant to spectrum-of-care conversations: open-ended inquiry and reflective listening. This article will address the applications of both and then introduce two supplemental skills: transparency and unconditional positive regard.
Open-ended inquiry, perspective-taking and perspective-seeking
As veterinarians, we bring knowledge into the consultation room about animal behavior and welfare, health and wellbeing, illness and disease progression, diagnosis and prognosis. What we do not know when we initiate a VCPR is who we will meet on the other side of the consultation table. To maximize information sharing with our client, we must actively solicit and understand individual narratives across a diverse clientele. 72 This requires us to step outside our own agendas to exhibit professional curiosity about another person’s past experiences, present needs and future expectations concerning healthcare delivery. 72 When we encourage others to elaborate beyond a ‘yes’ or ‘no’, we are inviting them to disclose critical information in their own words without leading them down a certain path. 73 This gives us the opportunity to acknowledge, affirm and address their perspectives as we collaborate on case management decisions.
Perspective-taking and -seeking also require us to draw upon cultural humility and recognize that our clients view their patients’ care journeys through a unique lens that may be influenced by personal, familial, cultural and societal perspectives on their relationships with animals, the function and inherent value of the individual patient, as well as the uniqueness of their bond. 72 These aspects of the VCPR are not often explored, yet the veterinarian must stretch beyond their own sense of self to recognize and accept that the client also operates from within their own distinct worldview. The only way to make sense of another’s world view is to actively solicit and take on that individual’s perspective in a way that inspires dialogue and partnership. 72
Open-ended inquiry is the way in which we engage in such solicitation. Statements or questions that elicit the client’s perspective start with: 74
What. . .
Tell me. . .
Share with me. . .
For example: 74
‘What concerns you most?’
‘Tell me what’s weighing on you.’
‘Share with me what’s going through your mind right now.’
The connection between open inquiry and spectrum-of-care conversations is perhaps most familiar when discussing the cost of care. In Box 1, the author provides an example of how open inquiry can prompt the client to articulate financial concerns that can then be discussed in concert with dialogue about healthcare options. Note that open inquiry requires the clinician to pay attention not only to verbal statements made by clients, but also to non-verbal cues that might suggest discomfort, inviting further discussion.
Example of how open-ended inquiry and perspective-taking connect to spectrum of care through financially driven client-based concerns

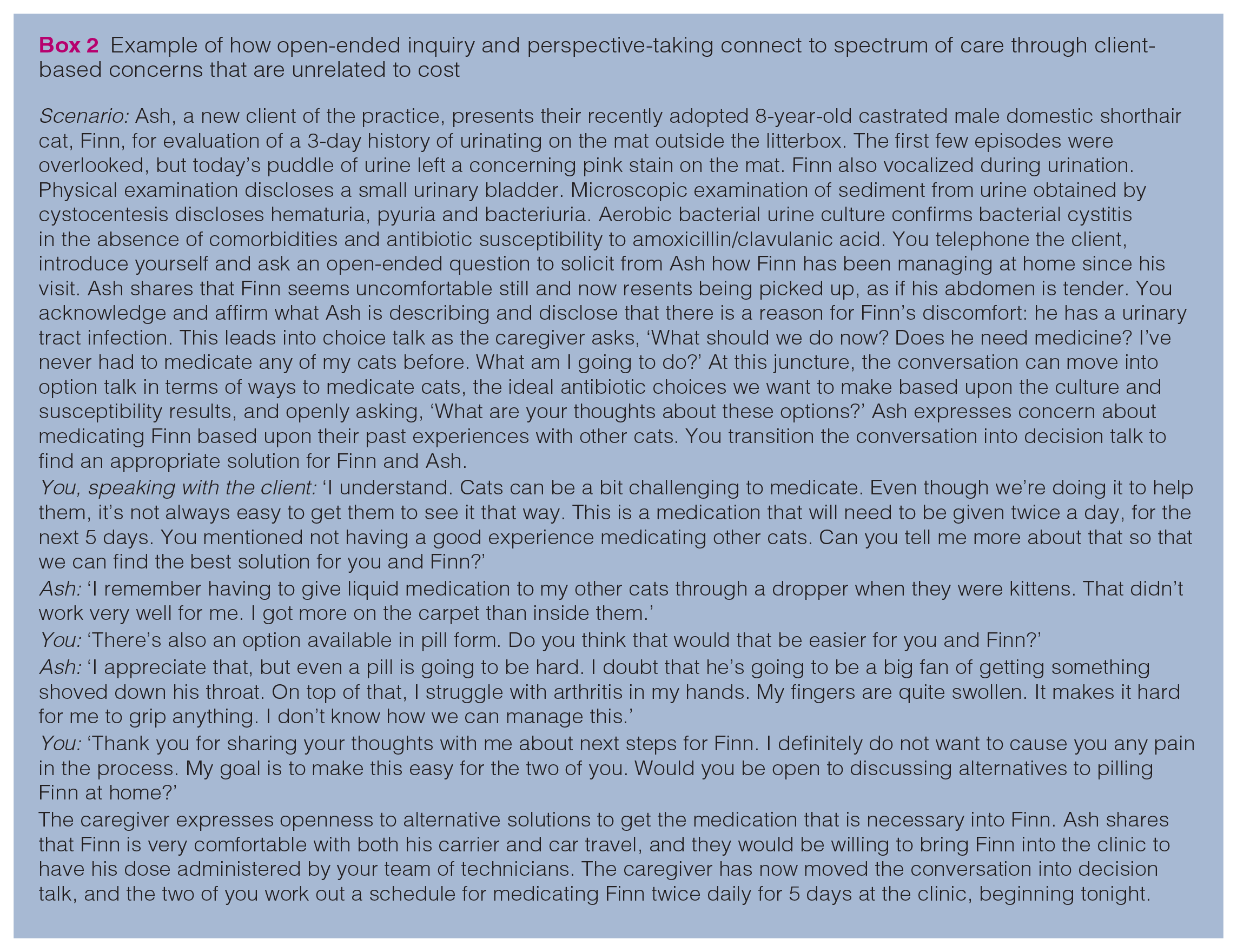
The cost of care has been cited as a primary reason why clients do not seek veterinary care, 75 and veterinarians acknowledge that the client’s burden of financing care frequently limits the types of diagnostic and therapeutic interventions that can be pursued.7,59,76–79 However, it is important to recognize that cost is not the only barrier to healthcare delivery, despite assumptions on our part that it might play a significant role. Open-ended inquiry reminds us to stay curious and to ask clients what concerns them most, rather than assume we know the answer. Through open-ended inquiry, we may glean valuable insight from our client in terms of what additional considerations we might need to address in our delivery of a continuum of healthcare options. In Box 2, the author provides an example of how open inquiry can prompt the client to articulate concerns that are unrelated to cost of care.
Example of how open-ended inquiry and perspective-taking connect to spectrum of care through client-based concerns that are unrelated to cost
Reflective listening
When we present a continuum of acceptable care options to our clients, we are initiating an exchange of ideas and inviting them to consider each. In the process, communication becomes a feedback loop. 80 Dialogue exchange is necessary to achieve mutual understanding so that our client can contribute to and ultimately make informed decisions concerning healthcare delivery. 80 For this frisbee-like approach to be productive, each participant must take turns to be the sender of information and the recipient. 80 In other words, one person listens when the other is speaking. 80 Roles reverse as often as is needed to relay appropriate messaging. 80
Listening is an active process that challenges us to hit the pause button on our own stream of thoughts and shift our focus on to someone else. Effort is required to invest in what another person is saying, reflect on the information exchanged, and prioritize another individual’s needs above our own.80–84 Eliciting the client’s perspective is effective only if, after tasking the client with sharing their thoughts with us, we actively hear them. Active listening, also known as reflective listening, is one of the most powerful displays of connectivity that a provider can offer within the consultation room. ‘I’m listening’ conveys to the speaker that they have found a safe harbor in which emotions can reside. ‘It is the kind of connection that comes from being present with another, from giving our full attention so that we may listen not only with our minds, but with our hearts as well.’ 85
Reflective listening often takes the form of certain words or phrases that the listener relays back to the speaker. These include the following: 80
‘It sounds like. . .’
‘What I’m hearing you say is. . .’
‘I am sensing that. . .’
‘So, your main concern is. . .’
We can apply this communication skill to spectrum-of-care conversations. In Box 3, the author provides an example of how we might use reflective listening to clarify that we have understood our client’s reservations about the proposed care plan.
Example of how reflective listening can be applied to spectrum-of-care conversations

Transparency
Historically, transparency in human healthcare referred to the medical team’s disclosure of medical errors. 86 Acknowledging errors helped patients and their families understand what went wrong and why, and how errors could be remedied.86–89 The definition of transparency in human healthcare has since broadened to encompass the expectation by human patients that healthcare providers will deliver accurate, truthful information90–93 about diagnosis, prognosis, treatment options, risk: benefit ratios and the potential for adverse outcomes.90–92,94 Access to information and timely updates can enhance patient coping, wellness, satisfaction and psychological adaptation.90,95–101
Few publications in the veterinary medical literature have examined what information is preferred by cat-owning veterinary clients and why. In one focus group study, clients shared their need not to have information withheld from them. 33 In a separate study by Stoewen et al, 90 in-person interviews were conducted with clients who sought care for dogs with life-limiting cancer from a tertiary referral center. Participants shared that they expected to be given truthful information about all aspects of their pets’ disease process. 90 They ‘did not want the situation “sugar-coated”, “buttered-up” or “made prettier” than it really was. Instead, they wanted “the straight goods”, “the truth”, “the facts – good or bad” so they could “deal with it as best they [could] to avoid surprises” and “disappointment”, and “be prepared”’. 90
Because they actively require measures to explore the client’s perspective, including information needs, spectrum-of-care conversations are a vital opportunity to address client expectations with transparency. In Box 4, the author provides an example of how we can incorporate the communication skill of transparency into spectrum-of-care conversations.
Example of how transparency can be incorporated into spectrum-of-care conversations

Unconditional positive regard
The practice of unconditional positive regard suggests that veterinarians accept clients for who they are and meet them where they are, rather than hold them to impossibly high standards. 86 Focus group studies that involve veterinarians disclose their tendency to misjudge a client’s willingness to provide what they perceive to be the best care. 59 Participating veterinarians acknowledged that such assumption-making influences the healthcare options that they identify and explore, despite recognizing the impact of misperceptions on the VCPR. 59 Veterinarians shared that judgment often centers around the perceived affordability of care, and that it works both ways: veterinarians may both over- and underestimate how price-conscious clients are. 59 One veterinarian in a focus group study by Coe et al 59 recalled a consultation in which ‘I did not even give them a cost because it looked like that was what they wanted to do, and then cost became an issue later on’.
Cost aside, veterinarians acknowledge that judgment also extends to choices that clients make with respect to healthcare decisions. 102 Participating veterinarians in a second focus group study by Coe et al 102 admitted the challenge of accepting a client’s choice irrespective of whether ‘it’s a good one, bad one or sideways’. There is an expectation of veterinarians by clients that they support and validate decisions, even when veterinarians disagree. 102 Cat owners in particular want the veterinary team to understand that they are well intentioned, even if their actions may not always be medically appropriate. 33
Yet, fear of judgment may prevent clients from participating in open, honest dialogue about patient care. They may worry about full disclosure if they feel that their actions will be held against them. Clients need to be reassured that we recognize that their words and actions reflect care, even when they are misguided. When interpersonal challenges arise, veterinarians should shift focus on to common ground: what do they and the client both wish to achieve and how can they work together to that end? 86 The only way to move forward with patient care is with client consent, and that requires partnership. Partnership is reinforced by eliciting the client’s perspective, then actively listening as the client shares it. However, clients seek more than just to be heard. They seek validation and affirmation. They want to know that you understand and accept why they did what they did. 86
Demonstrating regard for our clients’ past actions may take the form of: 86
‘I can only imagine that you felt trapped between a rock and a hard place. You did the best you could in a difficult situation.’
‘I understand why you made the choices you did; I might have done the same thing in your situation.’
‘You said you wished you had done more. What matters most is that you brought your cat here during their time of need. Let’s work together to figure out how to help best.’
Demonstrating regard for our clients’ current choices may take the form of:
‘Your decision isn’t easy; thank you for leading with your heart and considering what is best for your cat.’
‘I see that you are struggling with this decision, and I value the care that you are investing to determine what is best for you and your cat.’
‘I appreciate that you want to do right by your cat.’
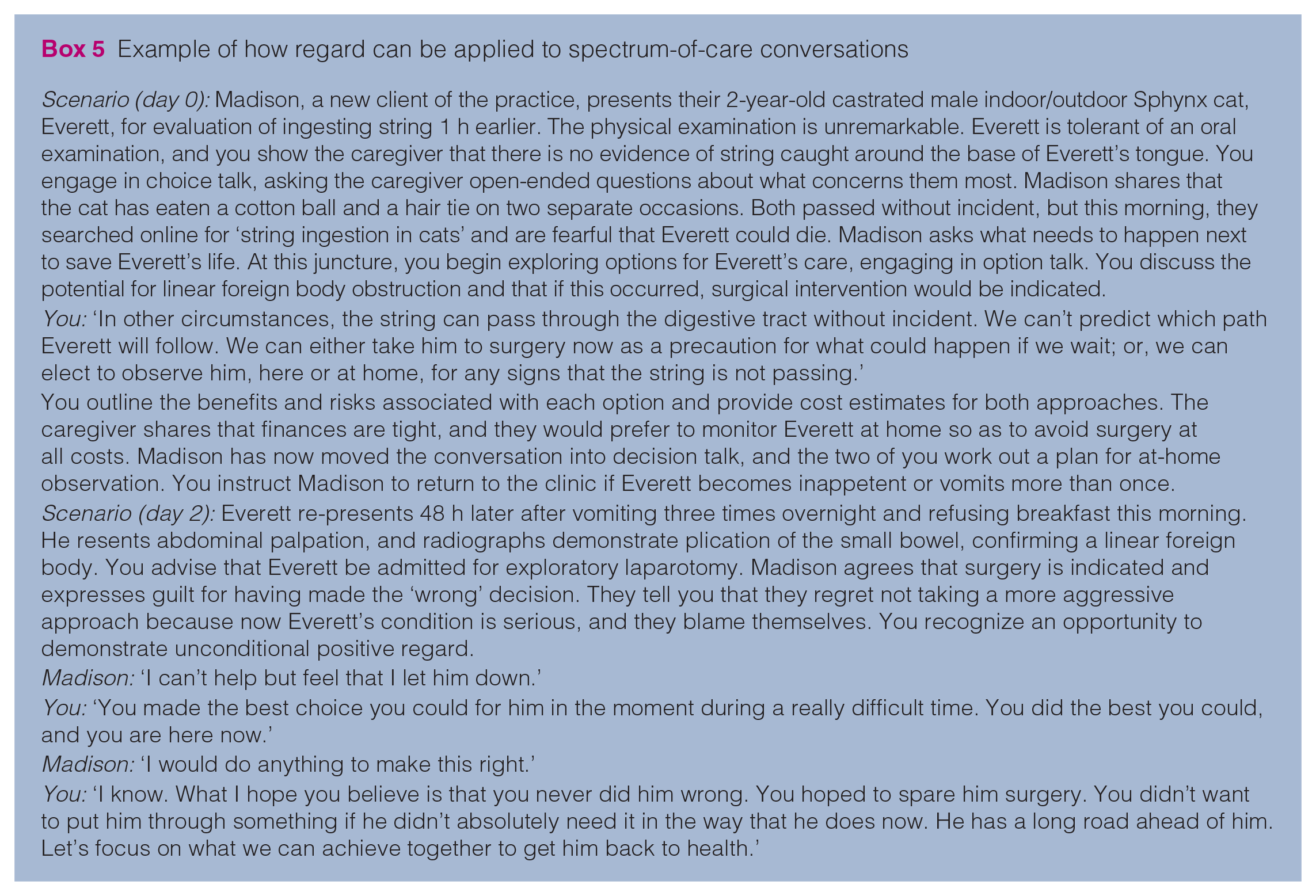
We can apply this communication skill to spectrum-of-care conversations by being accepting of choices that clients make, even if we might be inclined to make different choices were we in their shoes. In Box 5, the author provides an example of how regard might be employed in clinical practice.
Example of how regard can be applied to spectrum-of-care conversations
Leveling up: additional communication-based spectrum-of-care considerations
This article has introduced several foundational communication skills that facilitate spectrum-of-care conversations by promoting two-way exchange of information in which the client can both share and be heard. The client’s thoughts, beliefs, concerns and expectations are invaluable because these details fill in the gaps that we clinicians cannot discover without perspective-seeking and the client’s willingness to disclose. Disclosure requires a safe, supportive space in which clients feel that judgment from the veterinary team has been replaced with regard.
Spectrum-of-care conversations task us to rethink our understanding of patient care and the ways in which we prioritize it:
How can we offer contextualized care?
How can we broaden the selection of options that we offer to clients to incorporate their needs, wants and expectations?
How can we expand our evidence base to investigate the efficacy of alternative approaches to traditional gold standard care?
How do we convey the value of care, irrespective of which option the client selects?
Is it important to acknowledge that someone’s plan A might be someone else’s plan B or even plan C for reasons that we might not even consider until we participate in a dialogue exchange to discover the context for which one approach to care is appropriate and desirable.
How can we restructure the way we think about and deliver options so that options are presented with an open mind? Should we move beyond our default model of identifying plans as A, B and C, and instead consider a three-step model of SDM? Recent work by Janke et al 29 analyzed audiovisual recordings from 60 veterinarians and 909 of their clients. An analysis of these interactions suggested that healthcare providers infrequently practice SDM. 29 Veterinarians are legally and ethically obligated to elucidate the pros and cons of each option, including the risks associated with a ‘wait and see’ approach. 103 Yet, many clients feel that they are not given an opportunity to exercise choice. 102 Choice is particularly essential to clients who are navigating end-of-life decision-making. 104 Clients who participated in a 2017 study by Corah et al 104 expressed a need for reassurance that their decisions to euthanize were supported. Training the entire veterinary team how to apply SDM to consultations could prove useful, potentially raising client satisfaction with healthcare delivery and improving client adherence.29,105
Elwyn et al 106 suggested that when collaborating on patient care we can move from initial preferences to informed preferences by engaging clients in SDM at three levels:
Choice talk
Option talk
Decision talk.
During the initial phase of the consultation, choice talk, we let the client know that choices exist. 106 To facilitate this discovery phase, we engage in perspective-taking and -seeking to identify client preferences, beliefs, opinions and values. We are transparent about how much time the client has to make the decision and we are clear about whether decisions can be staged.
Option talk allows us to revisit each option and share information. 106 We take the opportunity to assess the client’s baseline knowledge and expand upon it with respect to what choices are available to them, including a cost:benefit analysis. The client in turn is encouraged to share their expertise and point of view. Clients are experts on the patient, the environment, their time commitment/constraints, their emotional investment and the financial resources available to them. Our primary goal during this stage is to support decision-making by delivering a continuum of care options presented in an equitable manner.
Decision talk, the final stage of SDM, requires us to focus on what matters most to the client/patient dyad and link the client’s priorities to the option set. 106 We summarize each option and its implications. We screen for questions and check the client’s understanding to determine whether additional information is needed for the client to decide. If so, we provide the missing data. If not, we partner with the client to come to a mutual agreement.
This process may take one or more consultations to complete and requires us to make use of our four communication skills:
Open-ended inquiry
○ Find out how much the client wants to be involved in decision-making. ○ Value client input and invite it. ○ Explore concerns, values, hopes and constraints. ○ Invite questions.
Reflective listening
○ Check for understanding. ○ Align client preferences with options.
Transparency ○ Provide information about options, including risks, benefits and costs.
Regard ○ Give space. ○ Respect the client’s decision and the journey it takes to get there.
Put it in writing: documenting key highlights of the dialogue
Fear of increased liability may complicate a veterinarian’s decision to offer a spectrum of care. 107 The reality is that any approach to case management can be subject to criticism. Even gold standard approaches to clinical cases can yield negative client reviews, board complaints or even lawsuits. 107 The best approach to mitigate the risk of negative consequences stemming from case management is to be thorough in documenting client communication. 107 This includes embedding client communication notes within medical records. Recall that client communication notes in medical documentation are not limited to summaries of face-to-face conversations, but also include telephone and electronic means of correspondence. It has been said in human healthcare that ‘if it isn’t charted, it didn’t happen’. 108 Records should report which options were given, as well as a summary of the risks vs benefits of each intervention. 107 These details are protective from a liability standpoint. If a board complaint is filed, then the record speaks for itself. There is a record of what was said and done, and why.
Beyond legal purposes, client communication notes are also invaluable prompts for busy practitioners who may not recall the details of conversations with clients days, weeks or months after they took place. Similarly, notes relay critical information about the medical provider’s actions and thoughts to other members of the healthcare team. A written record serves as a reminder of what has been discussed and why decisions were made. 109 In the event that case management requires an adjustment, all one has to do is re-examine the medical record to identify what next steps will be taken. This is particularly true of case management that hinges on incremental care. If treatment ‘v’ does not yield ‘x’ results, then the next step may be either to transition to treatment ‘y’ or go back to the drawing board and perform diagnostic ‘z’.
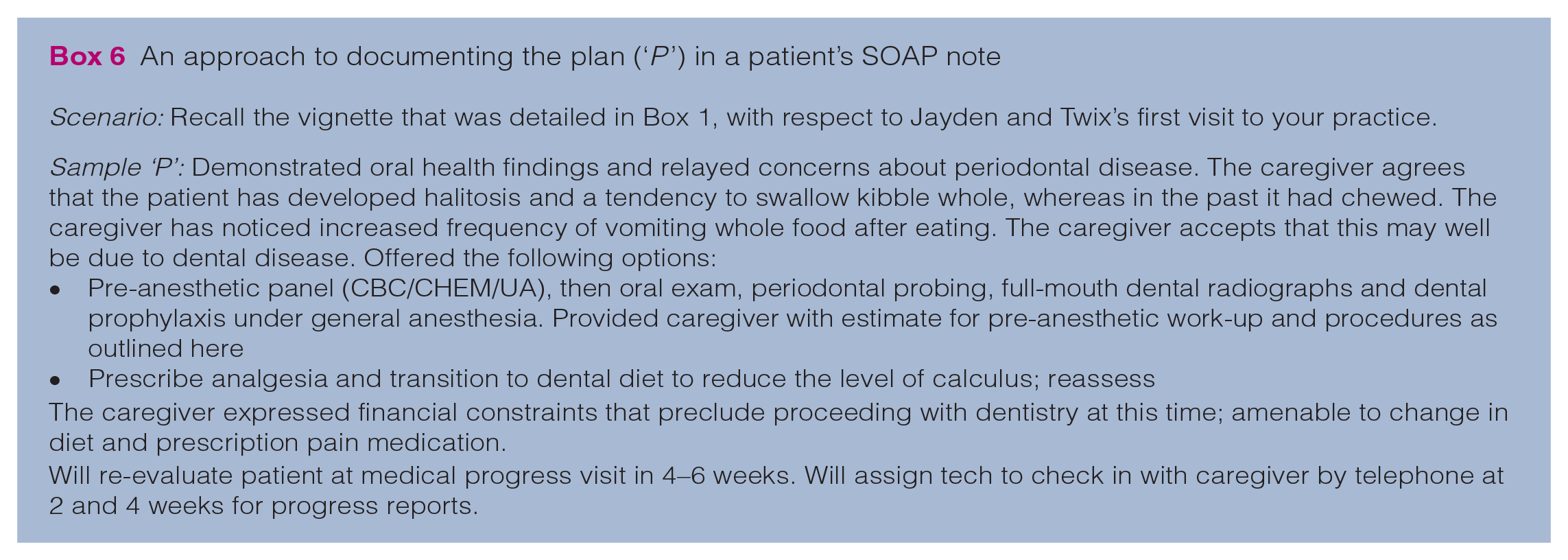
Medical documentation in veterinary practice typically takes the form of subjective objective assessment plan (SOAP) notes. 109 There is no universal approach to SOAP notes. Expectations for medical documentation often vary between practices, based upon veterinarian and employer preferences, and between states, provinces and countries, depending upon regional law. Historically, it has been considered best practice to document when any diagnostic or treatment recommendation is declined, or if a patient is discharged to the care of a client against medical advice (AMA). 110 In the author’s experience, there is a tendency for medical providers to document any action on the client’s part as being AMA other than the client’s adoption of gold standard care. This is concerning in such cases where clients have been offered a selection of options from which to choose and they choose an incremental care approach to case management. Labeling their actions as AMA when in fact they made an appropriate choice, just not one that the provider may have preferred, runs the risk of attaching judgment to a client’s actions (or deliberate inaction). The author’s preference in such situations would be to communicate in writing which options were discussed. Then, the veterinarian can place the emphasis on the client’s final decision and rationale, rather than making declined options a focal point, except in those instances in which the chosen course of action is inappropriate. In Box 6, the author suggests an approach to how to effectively document the agreed-upon plan.
An approach to documenting the plan (‘P ’) in a patient’s SOAP note
An exception to this approach would be if the veterinarian perceives that client decision-making is unethical or inhumane. In this instance, it is incumbent upon us to prevent and relieve animal suffering through ethical practice. 111 Our professional obligation and oath dictate that we be transparent with clients about our limitations with respect to case management and share when we cannot ethically proceed with what has been asked of us by them. Written documentation should mirror what words were exchanged during the consultation, and identify what, if any, next steps (eg, mandatory reporting) must be taken in accordance with local law. The client should be informed of these steps so as not to be caught off guard, and documentation should capture that this information was conveyed. Sometimes we are challenged by situations that are not blatant animal abuse and cruelty, but instead involve decisions that we cannot honor. In this circumstance, it is essential that we disclose our boundaries respectfully, casting judgment aside, so that we can then partner with the client to find resources who may be better equipped with capacity to assist (eg, referrals to colleagues for a second opinion).
Such exploration should also take care to dive deep into the ethics of not treating. We can each name examples of when diagnostics and/or therapeutics are declined for the benefit of the patient. Although often these declinations are documented as a blight in the client’s medical record, it is vital that we rethink this approach and recognize the unspoken truth that sometimes withholding one or more types of treatment is in fact putting the patient’s welfare first. Accordingly, ethical considerations surrounding end of life have most recently been explored in hospice and palliative care. The 2023 AAFP/IAAHPC Feline Hospice and Palliative Care Guidelines propose that case management in such situations be guided by respect for autonomy, non-maleficence, beneficence and equity in therapeutic recommendations. 112 This bioethical framework guides clinical decision-making by applying context and thereby consideration for each specific case as its own entity. 112
Final comments
Spectrum of care is a means by which we as a profession can make care more accessible across the board. At the heart of spectrum of care is a desire to drive patient care forward by deepening the VCPR. By engaging our clients in partnership and initiating open channels of communication, we can see patient care (and our clients’ need for support) through another’s lens. When we take on this newfound perspective, we are better able to provide contextualized care for the patient and client.
As we look to expand the role that spectrum of care plays in veterinary practice, as well as in veterinary medical education, we need to broaden our evidence base and support research that investigates alternative options to classic treatment plans. Evidence is needed to confirm that approaches are acceptable, equitable and in the best interest of the patient. It may also be helpful to consider formulating spectrum-of-care guidelines for veterinarians to draw upon, particularly those early career practitioners who have not yet gathered appreciable clinical experience to serve as their guide.
Footnotes
Acknowledgements
The author thanks multimedia specialist Eric Beasley for partnership in co-designing Figure 1. The author also wishes to thank Teresa Graham Brett, Associate Dean of Diversity and Inclusion, for her partnership in co-designing the longitudinal Professional Skills coursework at the University of Arizona College of Veterinary Medicine pre-clinical curriculum, which prioritizes the conceptual framework surrounding spectrum of care.
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.