
Abstract
Objectives
The aim of this study was to determine whether an association existed between cephalometric measurements, maxillomandibular dental arch distances and the occurrence of traumatic malocclusions in the mandibular soft tissues of cats.
Methods
Cats that had presented for dental consultations and that underwent cone-beam CT during diagnostic assessment were included in the study and categorised as cases and controls in a 1:2 ratio. Cases were designated as cats with a clinical diagnosis of malocclusion causing trauma to the buccal mandibular soft tissues or pyogenic granuloma secondary to the trauma, and controls were designated as cats with the absence of such diagnoses and without a history of other musculoskeletal anomalies in the head. Cephalometric measurements, including skull and facial indexes, as well as distances and angulations between dental crowns and crown tips, were calculated and analysed statistically.
Results
In total, 72 cats (24 cases and 48 controls) were included in the study. Cephalometric measurements revealed a significant association between the skull and facial indexes and the occurrence of traumatic malocclusions in the caudal teeth. Brachycephaly was a strong predictor of the occurrence of traumatic malocclusions. In addition, the space between crown tips and teeth angulations was a contributing factor to the trauma.
Conclusions and relevance
Cats with traumatic malocclusions in the cheek teeth tend to present a narrower interdental space between the maxillary and mandibular carnassial teeth, mostly attributed to skeletal and dental malocclusion. These findings can be used to help raise awareness about this disease in cats and its association with brachycephaly. Cut-off values have been proposed and could be used in the selection of cats by breeders to reduce the occurrence of this disease.
Introduction
Dentition is closely linked to dental occlusion in cats; therefore, malalignment of the teeth can result in significant trauma to the oral cavity and development of diseases. 1 In cats, traumatic malocclusions occur secondarily to impingement of the maxillary fourth premolar teeth in mandibular soft tissues, along with the presence of pyogranuloma. 2 However, the specific characteristics of this condition are not yet fully understood.
The potential causes of this disease include acquired or congenital malocclusion, abnormal laterolateral mobility of the mandible, occlusal drift of the premolar and molar teeth, and/or alveolar bone expansion. 3
Malocclusion often occurs in some breed head types wherein the normal dentition–occlusal relationship is misaligned. 4 Predisposition of malocclusion has been reported in oriental and brachycephalic cats, 5 especially for distal traumatic malocclusions. 6 A high prevalence of malocclusions,7,8 together with maxillary premolar displacement, has been reported in brachycephalic cats. 8
The aim of the present study was to investigate whether an association existed between cephalometric measurements, maxillomandibular dental arch distances and the occurrence of traumatic malocclusions in the mandibular soft tissues of cats.
Materials and methods
Inclusion criteria
Cats that had presented for dental consultations between 2017 and 2022 and had undergone thorough clinical assessments, diagnostic imaging with whole-mouth radiography and cone-beam CT (CBCT) were included in the study. All cats were required to have complete permanent dentition, without a history of other musculoskeletal anomalies of the head.
Exclusion criteria
Cats that had a history of trauma to the head or maxillofacial surgery previously were excluded from the study. Cats with missing teeth relevant for the present study as well as those that had previously undergone odontoplasty or orthodontic treatment for conditions similar to those in the present study were excluded.
Ethics statement
The study included client-owned cats, and all owners agreed to the standard-of-care treatment. Written informed consent was obtained from the owners for the participation of their animals in this study. Ethical review and approval were not required for the animal study according to Polish Regulations (Art.1 ust.2 pkt1 Dz. U.2015 poz. 266).
Groups
The cats were divided into two groups: cases and controls. The number of controls was double that of cases (case-to-control ratio: 1:2). Cases (group A) were designated as cats with clinical diagnoses of malocclusion causing trauma to the buccal mandibular soft tissues or with pyogenic granuloma secondary to the trauma. Controls (group B) were designated as cats with the absence of such diagnoses and without a history of other musculoskeletal anomalies in the head.
Medical and dental procedures
All cats underwent thorough general and oral clinical examinations with assessments for occlusion before anaesthesia. All animals were qualified for general anaesthesia for reasons related to oral and/or dental problems.
After the induction of general anaesthesia, all cats were examined clinically. Whole-mouth radiography and CBCT (NewTom; 5G XL) were performed. For CBCT, volumetric assessment of the dentition was performed in the same high-resolution mode (10 × 10 cm with 0.15 mm layers) and high-energy enhancement. All scans were evaluated by a board-certified veterinary dentist experienced in CBCT imaging (JG). The scans were analysed using NNT Viewer software (version 10.1; QR SRL).
Dental treatment was performed in all cases, when indicated. The following treatments were performed: odontoplasty; extractions; excisional biopsies of any granulation or proliferative tissues; and laser ablation, if needed.2,3
Variables
The cephalometric parameters of the skull and facial indexes that were assessed and recorded were as follows: facial length; facial width; skull length; and skull width. Anatomic landmarks used for such measurements are presented in Table 1. The skull and facial indexes were calculated as previously reported. 8
Dimensions and parameters of anatomic landmarks measured in each cat

The measurements between dental landmarks are as follows (Figure 1a–c):
Distances (in mm) between the crown tips of 104–204, 304–404, 107–207, 108–208, 308–408 and 309–409 were calculated. In the case of 309 and 409, the distal crown tip was used for such measurements.
The space between the crown tips of 108–308, 208–408, 108–309, 208–409, 107–308 and 207–408 were determined as the difference between the previous measurements (107–207, 108–208, 308–408 and 309–409) at the point of interest, then divided by 2, to reflect the maxillomandibular dental space between each crown.
Angulation between the palatal plane and the tooth crown axis. The tooth crown axis was defined as the line between the middle point of the crown base and the crown tip. Angulation was calculated for teeth 107, 108, 207, 208, 308, 309, 408 and 409.
In the cats in group A, three grades of severity were defined for mandibular soft-tissue lesions secondary to malocclusion (Table 2 and Figure 2a–d). The number of lesions (1–4) in teeth 107, 108, 207 and 208 was recorded.

Assessment of the tooth crown axis for tooth angle determination and distances (in mm) between crown tips for (a) 104–204 and 304–404; (b) 107–207 and 108–208; and (c) 308–408 and 309–409
Categories of the malocclusion pathological consequences
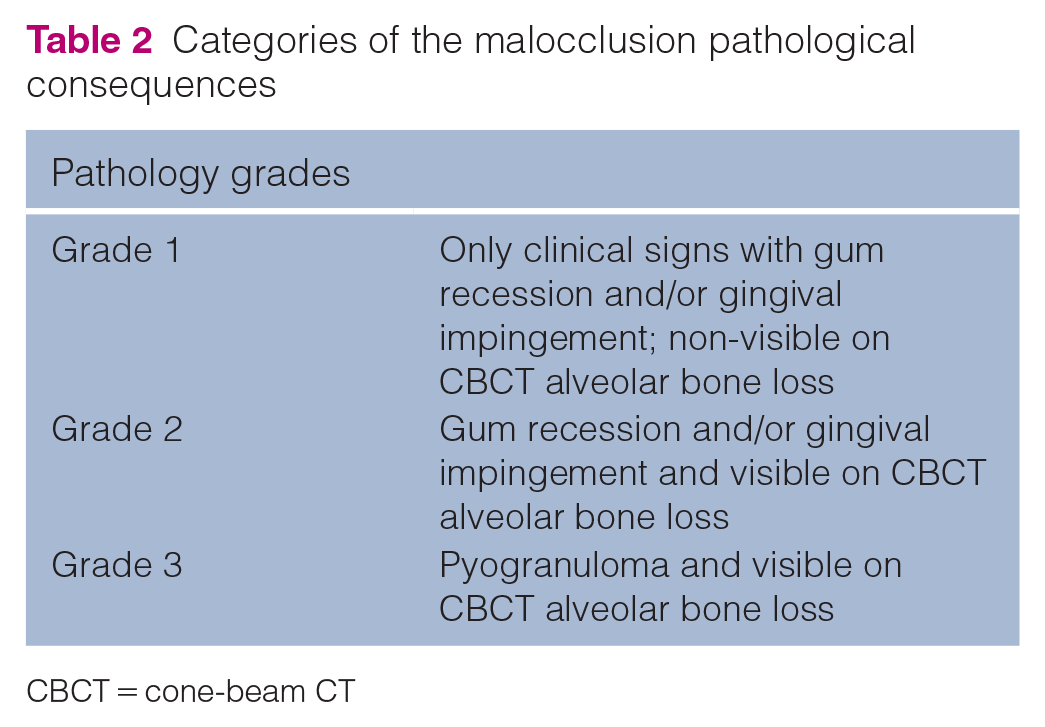
CBCT = cone-beam CT

(a) Photographs, (b) clinical three-dimensional reconstructions of CBCT scans, (c) radiography and (d) coronal slice images in CBCT showing the three grades of severity of lesions in the mandibular soft tissues secondary to the malocclusion. CBCT = cone-beam CT
Statistical analysis
Statistical analysis was performed using the commercial data analysis software system Statistica (version 10, StatSoft) and SPSS Statistics (version 26, IBM). Quantitative data were evaluated for conformity with a normal distribution using the Shapiro–Wilk test. Differences between the case and control subgroups were determined using the Student’s t-test or the Mann–Whitney test. To evaluate the discriminatory value of the skull and facial indexes for occlusion owing to traumatic malocclusions, a receiver operating characteristic (ROC) curve analysis was performed. A cutoff value was defined if the area under the ROC curve (AUC) was considered acceptable, and the value was determined maximising both sensitivity and specificity. P <0.05 was assumed to be statistically significant in all conducted tests.
Results
A total of 72 cats were included in the study. Their mean age was 58.74 ± 53.4 months (age range 6–236), and 39 (54.2%) were males and 33 (45.8%) were females; their mean weight was 4.57 ± 1.45 kg (range 2.35–9.0).
In group A (case group; n = 24 cats), the mean age of the cats was 48.92 ± 56.53 months (age range 6–236), and 13 were males (seven intact) and 11 were females (four intact); their mean body weight was 5.15 ± 1.41 kg (range 2.82–9.0). Among the 24 cats, there were 14 British Shorthair (BSH), two domestic shorthair (DSH), five Maine Coon and one each of British Longhair (BLH), Persian and Selkirk Rex.
In group B (control group; n = 48 cats), the mean age of the cats was 63.65 ± 51.67 months (age range 6–216), and 26 were males (10 intact) and 22 were females (seven intact); their mean body weight was 4.27 ± 1.4 kg (range 2.35–8.5). Among the 48 cats, there were 30 DSH, six BSH, four Maine Coon, three Ragdoll and one each of Scottish Fold, Persian, Thai, BLH and Norwegian Forest Cat.
No significant differences in age were observed between both groups, except group A cats had a significantly higher body weight than those in group B (P = 0.0079).
The average skull and facial indexes were 0.78 and 2.04 for group A cats and 0.71 and 1.86 for group B cats, respectively. The skull index in group A was significantly greater than that in group B (P = 0.0007), and the facial index showed significant differences (P = 0.0002) (Table 3).
Association between skull and facial index (SD) with study groups

Standard deviation in brackets
The distances and spaces between the crown tips are summarised in Table 4. The distances between the crown tips for teeth 107–207, 108–208 and 309–409 in group A were significantly greater than those in group B (P = 0.0010, <0.0010 and <0.0010, respectively). The mean space between the crown tips of 107–308 and 207–408 was 0.39 ± 0.51 mm in group A and −0.210 ± 1.44 mm in group B, which showed significant differences (P = 0.041). The mean space between the crown tips of 108–308/208–408 was 2.04 ± 0.50 mm in group A and 2.97 ± 0.53 mm in group B, which showed significant differences (P <0.001). The mean space between the crown tips of 108–309/208–409 was 0.076 ± 0.43 mm in group A and 0.110 ± 0.60 mm in group B, which showed non-significant differences.
Axial distances (mm) and spaces between crown tips in both groups*

Data are mean ± SD
(C-E)/2, (D-E)/2 and (D-F)/2 reflect the maxillomandibular dental space between each crown
ns = non-significant
The angulation values are presented in Table 5. All angles determined were significantly different between the groups. The angulation of teeth 108, 208, 308 and 408 in group A was significantly lower than that of group B (P = 0.0086, 0.0003, 0.0003 and 0.0010, respectively). By contrast, group A cats had a higher angulation for tooth 207 than group B cats (P <0.0010). No significant differences in angulation values were observed for teeth 309 and 409 between the groups.
Tooth angulation (°) to the palatal plane in both groups, assessed between the palatal plane and the tooth crown axis (defined as the line between the middle point of the crown base and the crown tip)

Data are mean ± SD
Median (min –max), Mann-Whitney U test
Mean (SD), Student t test
ns = non-significant
Traumatic impingement was mainly caused by cusps of 108 and 208, and the mean severity grade was 2.17 and 2.13, respectively. Teeth 107 and 207 caused trauma at severity grades of 1.04 and 1.20, respectively (Table 6). In group A, the mean number of lesions was 3.208 (range 2–4). Figure 3 shows the relative frequency chart of trauma grade caused by third maxillary premolars (107 and 207) and fourth maxillary premolars (108 and 208).
Distribution and grades of trauma in the oral cavity caused by malocclusion


Grade 1 = 1 point; grade 2 = 2 points; grade 3 = 3 points

Relative frequency chart of the severity grades of trauma caused by the third maxillary premolars (107 and 207) and fourth maxillary premolars (108 and 208)
In group A, the three-dimensional scan showed thinning or complete osteolysis of the palatal process of the maxillary bone at the level of mandibular molar occlusion in the palate. Among the 24 cats in group A, seven had this anomaly. Among the seven cats, one had involvement of four mandibular teeth (308, 408, 309 and 409) and six others had involvement of two mandibular teeth (309 and 409) (Figure 4). In group B, none of the cats had this anomaly.
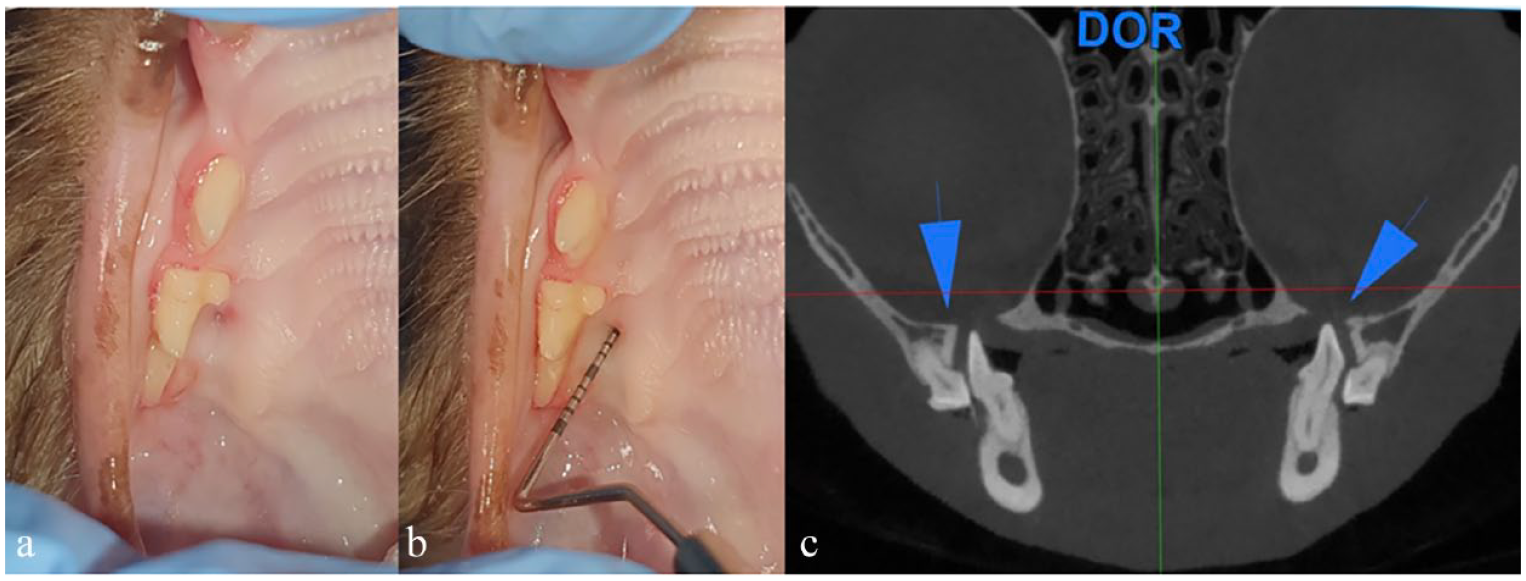
Palatal impingement in a cat with malocclusion as an additional finding: (a) clinical appearance of impingement; (b) periodontal probe inserted into impingement; and (c) coronal slice in cone-beam CT showing osteolysis of the palatal process of maxillary bone bilaterally (blue arrowheads)
The ROC curve analysis showed that the skull index was a significant predictor of traumatic malocclusions in the caudal teeth (P <0.001), with an AUC of 0.773. The cutoff value for the skull index was 0.7331, with a sensitivity of 79.2% and a specificity of 79.2% (1 – specificity = 0.208) (Figure 5). The ROC curve analysis showed that the facial index was a significant predictor of traumatic malocclusions in the mandibular soft tissues (P <0.001), with an AUC of 0.772. The cut-off value for the facial index was 1.96, with a sensitivity of 83.3% and a specificity of 72.9 (1 – specificity = 0.271) (Figure 5).

Receiver operating characteristic curves of the skull index (green) and facial index (blue) for discriminating between the presence and absence of caudal teeth malocclusion
Discussion
Malocclusion can occur because of differences in jaw length and/or width, malalignment of the teeth or a combination of these issues, 1 and it is associated with significant morbidity, requiring treatment. 9
This study was conducted to evaluate malocclusion of the premolars and molars through morphometric measurements to understand which specific features lead to malocclusion. Theoretically, the traumatic impingement of the third and fourth maxillary teeth in the periodontium of the mandibular teeth could be caused by several factors, either isolated or combined: palatoversion of the reduction of maxillary premolars of the maxilla; buccoversion of the mandibular premolars and molars; or skeletal anomalies in the absence of dental deviations, such as deviation of normal anysognatism.
CBCT was used to perform the morphometric measurements since it is superior in the assessment of bone height and teeth details. 10 Although radiography was performed during diagnosis and treatment, these imaging modalities were not used to assess morphometry parameters, as standard two-dimensional radiography can lead to distortion and overlapping of the structures.11,12
In this retrospective case–control study, cases and controls were selected based on data from retrospective dental records. This approach could have led to bias, as only animals with dental disease were included and they were different from the general population. However, malocclusions are developmental problems, and many dental diseases, such as dental trauma or periodontal diseases, are acquired. Animals that do not manifest the anomaly (ie, pre-molar/molar malocclusion) would be suitable candidates for assessment in the control group, as they are potential healthy animals, without any developmental anomalies. At the same time, for this study, it was necessary for the animals in the control group to have undergone CBCT. The increase in the ratio of controls to cases (2:1 ratio) in this study helped increase the statistical power of the findings. Regardless of the efforts to reduce confounding factors and increase homogeneity in both groups by matching age and sex, there was an over-representation of brachycephalic cats in the cases group that could not be matched in the same proportion in the control group. This was an important limitation that must be acknowledged, since it may impact some results. Indeed, it was very difficult to find control individuals with brachycephalic conformations and that were free of malocclusions.
The cats in the cases group had a significantly higher body weight than those in the control group. Weight-related differences could have resulted from incident or differences in breed types, as BSH and Maine Coons were predominant in the cases group (n = 19) when compared with those in the control group (n = 10).
Skull and facial indexes were assessed to evaluate the presence of possible skeletal malocclusions, and distances between the crown tips and angulations evaluated dental malocclusions to identify the presence of a frequent pattern of malocclusion. The results suggest that both skeletal and dental discrepancies contribute to traumatic malocclusion in the caudal teeth. Undoubtedly, brachycephaly is a significant contributor to malocclusion, as skull and facial indexes were significantly different between the groups. Furthermore, both skull and facial indexes were good predictors of the occurrence of traumatic malocclusion in the caudal teeth. This study proposes 0.7331 as the cut-off for the skull index and 1.96 for the facial index. Brachycephaly is a cranial dysmorphology strongly linked to similar genetic disarrangements encountered in some forms of craniosynostoses in humans. 13 As the skull and facial indexes increase, the risk of occurrence of malocclusion in the caudal teeth is high. These cut-off values can be used by breeders to select phenotypes with less severe malocclusions.
The results also suggest that dental malocclusions are a strong contributing factor to the occurrence of traumatic malocclusion, as maxillomandibular spaces and angulations were significantly different between the groups. As axial distances in cats carrying this malocclusion were significantly higher in group A but consistent, the angulation of the third and fourth maxillary premolars was significantly more acute in this group. The cats in this group present maxillary premolar angulations, which favour the impingement in the mandibular tissues, as the angulations contribute to a reduction in the maxillomandibular dental space. This study theorises that such cats have a wider maxilla but at a more angulated position, at the expense of the angulation of the palatine bone. This finding is also supported by the observations reported here, as our study showed bone resorption in the medial aspect of the maxillary teeth in the palatal process of the maxilla. This anomaly seems to result from traumatic malocclusions of the molar mandibular teeth to the palate and palatine process of the maxillary bone.
The relationship between malocclusion and trauma to the periodontal tissues has been widely described in human dentistry.14–16 However, some studies have reported the lack of an association between malocclusion and progression of periodontal lesions. 17
Periodontal injury is one of the consequences of severe malocclusion in humans, affecting quality of life. The associated pathological conditions of this injury include gingival surface injury, reduction of alveolar bone density and clinical attachment loss. 18 All these problems were identified in the cases group. The most severe grade of malocclusion in the present study resulted in the development of pyogranuloma. This pathology has been described in studies of humans but with a lack of association with occlusal trauma. 19
Conclusions
Traumatic malocclusion in the mandibular soft tissue is related to both skeletal and dental malocclusions. Brachycephaly is a significant feature contributing to the increase in caudal teeth malocclusions. Skull and facial indexes could serve as a discriminative predictor of dental anomalies. The cephalometric cut-off values reported in this study can serve as an important tool for the community of cat breeders in the selection of cats for breeding.
Footnotes
Acknowledgements
The authors would like to thank the veterinary nurses who were members of the research team: Joanna Warzecha, Natalia Hućko-Pietka and Justyna Matusińska.
Correction (April 2025):
This article was updated to correct the cut-off value for the facial index to 1.96 in the Results section and the Discussion section.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.