
Abstract
Objectives
Hyperthyroidism frequently affects middle-to-older-aged cats that can present with cardiorespiratory signs. The effects of hyperthyroidism on cardiac size and function have been previously documented. Anecdotally, pulmonary hyperinflation identified on thoracic radiographs may also be associated with hyperthyroidism; however, there is no literature to support this claim. The goal of this study was to determine any association between hyperthyroidism, pulmonary hyperinflation and cardiomegaly with the following hypotheses: (1) hyperthyroid cats would not have evidence of radiographic pulmonary hyperinflation compared with control cats; and (2) hyperthyroid cats were more likely to have evidence of radiographic cardiomegaly than control cats.
Methods
In this retrospective case-control study, the thoracic radiographs of 52 hyperthyroid cats and 46 non-hyperthyroid cats were evaluated for subjective and objective measurements of pulmonary hyperinflation and cardiomegaly.
Results
There were no statistically significant differences between hyperthyroid and non-hyperthyroid cats for any variable indicative of pulmonary hyperinflation. The mean ± SD vertebral heart score on lateral views for hyperthyroid cats was 7.75 ± 0.53 and for control cats was 7.55 ± 0.54, which was significantly different (P = 0.05). Among all cats, a more severe total elevation in thyroxine (T4) was correlated with a larger vertebral heart score on lateral views (Spearman’s correlation coefficient = 0.23, P = 0.02).
Conclusions and relevance
While the results of this study suggest that hyperthyroid cats are more likely to have a larger vertebral heart score on lateral views than control cats, the clinical relevance of this finding is unclear given the large degree of overlap between hyperthyroid and non-hyperthyroid cats. In addition, among all cats, a greater total T4 elevation was weakly correlated with a larger vertebral heart score. Hyperthyroidism is not associated with radiographic pulmonary hyperinflation and is an unlikely differential for this radiographic finding.
Introduction
Hyperthyroidism is the most common endocrine disorder of middle-to-older aged cats. Excessive amounts of thyroid hormone are produced by the thyroid gland, usually from functional adenomatous hyperplastic tissue. The most common clinical signs include weight loss, polyphagia and hyperactivity. Respiratory clinical signs such as panting and dyspnea are less commonly reported. 1 Diagnosis is accomplished via a combination of thyroid hormone testing, most commonly by evaluation of total thyroxine (T4) concentrations, and consistent clinical signs. 2
Thoracic radiographs may be performed when evaluating hyperthyroid cats for evaluation of non-thyroidal disease or to assess overall health. At Colorado State University, pulmonary hyperinflation is an anecdotal radiographic finding that may indicate hyperthyroidism; however, there is no literature to support this claim. A single study investigating the efficacy and safety of transdermal methimazole found pulmonary hyperinflation in 2/6 hyperthyroid cats that had thoracic radiographs performed. 3 Pulmonary hyperinflation was not specifically assessed in a recent study that investigated radiographic thoracic pathology in hyperthyroid cats presenting for radioiodine therapy. 4 Outside of hyperthyroidism, pulmonary hyperinflation is commonly seen in cats with feline asthma and chronic bronchitis.5–7 In addition, there are few additional reports of diffuse pulmonary hyperinflation in cats including a cat with tracheal anaplastic squamous cell carcinoma 8 and in cats experimentally infected with Dirofilaria immitis. 9
Thoracic radiographs are also commonly performed in cats with known hyperthyroidism to evaluate for cardiomegaly and, conversely, cardiomegaly on thoracic radiographs could prompt investigation for hyperthyroidism. Multiple studies have found an association between hyperthyroidism and echocardiographic left ventricular hypertrophy, left atrial dilation and left ventricular dilation.10–13 Cardiomegaly has also been reported on thoracic radiographs in hyperthyroid cats.3,4,14
The aim of this study was to describe the radiographic pulmonary and cardiac abnormalities in cats affected with hyperthyroidism. Given that respiratory signs are not common with hyperthyroidism, and that pulmonary hyperinflation is a non-specific and relatively uncommon finding in the veterinary field, we hypothesized that there would be no significant association between hyperthyroidism and radiographic pulmonary hyperinflation. In addition, we hypothesized that there would be a significant association between hyperthyroidism and radiographic cardiomegaly, as identified in previous literature.
Materials and methods
The medical record database at Colorado State University Veterinary Teaching Hospital was searched between 1 January 2010 and 1 September 2019 for cats that had thoracic radiographs and thyroid hormone testing performed within 2 weeks of each other. A minimum of two orthogonal radiographic views of the thorax were required for inclusion. Cats were excluded if they presented for coughing, respiratory distress or had comorbidities such as acromegaly that may have affected cardiac size. Cats with radiographic studies that were suspicious for pulmonary neoplasia, pleural effusion and congestive heart failure were also excluded as they may affect the respiratory status of the patient. Total T4 levels were evaluated by Colorado State University Veterinary Diagnostic Laboratories. Patients with a total T4 value >4.8 µg/dl were included in the affected hyperthyroid population. Patients with total T4 values <4.8 µg/dl were included in the control group. The case history, including previous treatments for hyperthyroidism, signalment, primary presenting complaint, presence of a murmur or gallop rhythm, blood pressure, total T4 values and imaging findings were recorded.
A board-certified veterinary radiologist (AM) and a radiology resident (VY) reviewed the thoracic radiographs for pulmonary hyperinflation, cardiomegaly and abnormal pulmonary patterns via consensus. In order to anonymize the images, the hyperthyroid and non-hyperthyroid cats were combined into one group and arranged numerically by patient medical record number. The list was then randomly rearranged using the ‘Randomize range’ feature in Google Sheets. Once rearranged, a new medical record number was assigned to each cat. Original identifying medical record number and signalment were removed from the radiograph images and relabeled with the newly assigned medical record number. Only new medical record numbers were available during interpretation, such that the authors were unaware of the hyperthyroid status of that patient at the time of image evaluation. All radiographic studies were reviewed using DICOM image processing application software (Intellispace PACS Radiology 4.4; Philips Medical Systems).
Pulmonary evaluation
Radiographs were evaluated subjectively for the presence or absence of diaphragmatic flattening on lateral views, increased convexity of the diaphragm with visible diaphragmatic attachments on ventrodorsal (VD) or dorsoventral (DV) views, increased distance between the diaphragm and cardiac silhouette and pulmonary hyperlucency that would suggest pulmonary hyperinflation, as previously described (Figure 1). 15

Representative images illustrating the absence of (top) and presence of (bottom) diaphragmatic flattening and increased distance between the diaphragm and cardiac silhouette. In the bottom image, the diaphragm has lost its concave shape and is more caudally located relative to the cardiac silhouette. The diaphragm in the top image has normal convexity and location relative to the heart
To complement subjective interpretation, objective evaluation for pulmonary inflation was calculated with lung-to-vertebral body ratios using a previously described method. 7 Two ratios were obtained on the VD view preferentially, or the DV view if this was the only option available: (1) the thoracic width at the level of T7:width of T7; and (2) the maximal width of the lung field:width of T7. Two ratios were calculated on the best positioned lateral view: (3) maximal length of the lung field:length of T7; and (4) length of the lung field from the most cranial margin of the lung to the intersection of the diaphragm and caudal vena cava:length of T7 (Figure 2).

Method for objective calculation of lung inflation ratios in cats on radiographs as previously described. 7 On the best positioned lateral view (left), two ratios were obtained: (1) maximal length of the lung field (a) divided by the length of T7 (c); and (2) length of the lung field from the most cranial margin of the lung to the intersection of the diaphragm and caudal vena cava (b) divided by the length of T7 (c). On the ventrodorsal (VD) view (right), two ratios were obtained: (3) thoracic width at the level of T7 (d) divided by the width of T7 (f); and (4) maximum width of the lung field (e) divided by width of T7 (f). This measurement was performed on the dorsoventral view as opposed to the VD view for two cats
The subjective presence or absence of an abnormal pulmonary pattern was also recorded and categorized as a bronchial, interstitial, alveolar or mixed pulmonary pattern. If a pattern was identified, it was graded as mild, moderate or severe, and focal, multifocal or diffuse.
Cardiac evaluation
Radiographs were evaluated objectively for cardiomegaly using vertebral heart scores (VHS) and cardiac short-axis measurements performed by one author (VY), as previously described. 16 VHS were calculated on the best positioned lateral view, termed VHS lateral, and best positioned VD or DV view, termed VHS VD/DV. Subjective evaluation of left atrial enlargement was also performed, to complement the objective evaluation. Left atrial enlargement was identified as increased convexity of the caudodorsal cardiac margin on lateral views, and increased convexity along the left cranial-to-mid margin of the cardiac silhouette on the VD or DV view (Figure 3). VD views were preferentially chosen for evaluation; DV views were only used if they were the only option available).
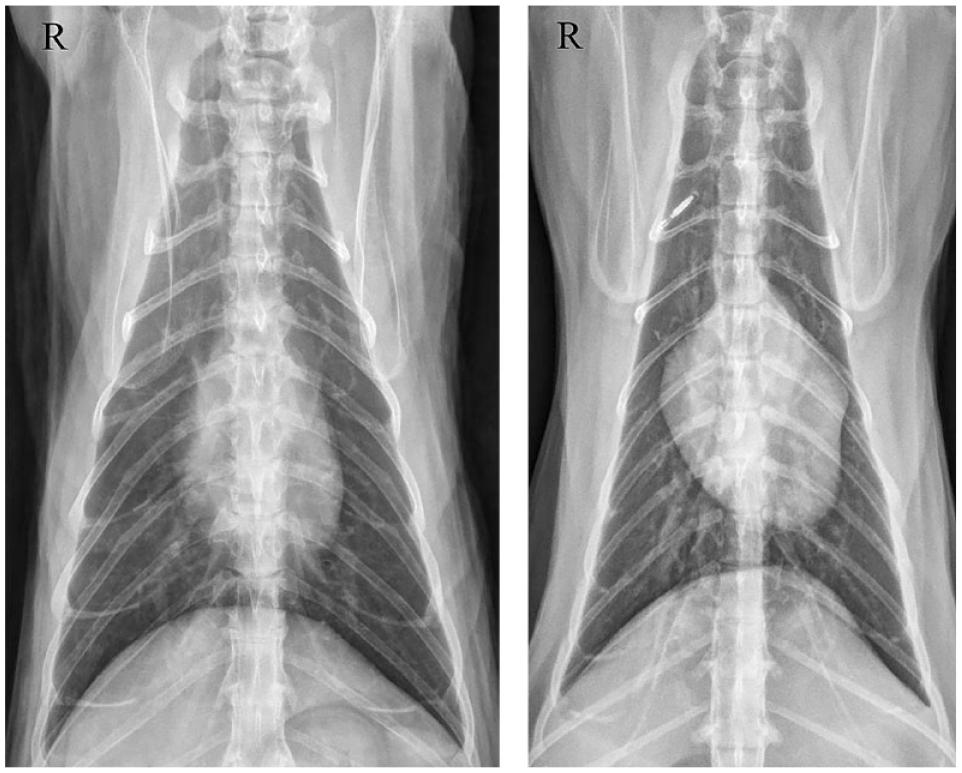
Representative ventrodorsal views illustrating the absence of (left) and presence of (right) left atrial and auricular enlargement. Note the increased convexity along the cranial-to-mid aspect of the left side of the cardiac silhouette
Statistical analysis
Statistical analysis was performed by one author (SR). χ2 analysis was performed to evaluate the statistical significance between categorical variables. If the numbers were <5, a Fisher’s exact test was used. Continuous data were compared between two groups using a Student’s t-test when data were normally distributed. Otherwise, a Wilcoxon two-sample test was used. Correlation was evaluated between two continuous variables using a correlation coefficient or Spearman’s rho when data were not normally distributed. A P value <0.05 was used to evaluate statistical significance. SAS v9.4 (SAS Institute) was used for all statistical analysis.
Results
Initially, there were 52 affected hyperthyroid cats and 51 control cats. Of the 15 control cats that had echocardiograms performed at the time of radiography, five were removed from the evaluation as they had definitive evidence of structural heart disease, resulting in a total of 46 control cats. Of the three hyperthyroid cats that had echocardiograms performed at the time of radiography, two had evidence of ventricular wall thickening, one of which also had left atrial enlargement. The median age of the hyperthyroid cats was 13 years (range 4–18); the median age of the control cats was 13 years (range 6–17). Of the hyperthyroid cats, 28/52 (53.8%) were male castrated and 24/52 (46.2%) were female spayed. Of the control population, 21/46 (45.7%) were male castrated and 25/46 (54.3%) were female spayed. The most common clinical signs in both groups were gastrointestinal signs, including weight loss, inappetence and vomiting (44/52 [84.6%] of hyperthyroid cats; 33/46 [71.7%] of control cats). The median total T4 value within the hyperthyroid group was 10.6 µg/dl (interquartile range [IQR] 7.85–15.7) and within the control group was 1.72 µg/dl (IQR 1.22–2.34). In seven cats, the total T4 value exceeded the maximum reportable value of 24 µg/dl. Radiographs were most commonly performed as part of a thorough work-up for gastrointestinal disease, pulmonary metastasis assessment and wellness care. Ninety-five of 103 (92.2%) cats had three orthogonal views for radiographic evaluation. Ninety-four of 98 (95.9%) cats had VD views, 2/98 (2%) cats had DV and VD views, and 2/98 cats (2%) had DV views.
Pulmonary radiographic results
Radiographically 8/52 (15.4%) hyperthyroid cats and 5/46 (10.9%) control cats had diaphragmatic flattening. Seven of 52 (13.5%) hyperthyroid cats and 7/46 (15.2%) control cats had increased distance between the cardiac silhouette and diaphragm. No cat had visible diaphragmatic attachments or diffuse pulmonary hyperlucency. There was no statistical difference between hyperthyroid and control groups for the presence of diaphragmatic flattening (P = 0.56), or increased distance between the cardiac silhouette and diaphragm (P = 0.80). There was also no statistical significance between the four ratios of lung inflation on the VD or lateral views (all P ⩾0.11) between the hyperthyroid and control groups.
A bronchial pattern was found in 13/52 (25%) of the hyperthyroid cats and in 8/46 (17.4%) of the control population. An interstitial, alveolar or mixed pattern was not identified in any cat. The presence of a bronchial pattern was not statistically different between the two groups (P = 0.46). There was also no difference in severity (P = 1.0) or distribution (P = 1.0) of the bronchial pattern between the two groups.
Cardiac radiographic results
Hyperthyroid cats had a mean ± SD VHS lateral of 7.75 ± 0.53 and control cats had a mean VHS lateral of 7.55 ± 0.54, which was statistically significant (P = 0.05). Hyperthyroid cats had a mean VHS VD/DV of 8.47 ± 0.96 and cardiac short-axis of 3.62 ± 0.41. Control cats had a mean VHS VD/DV of 8.38 ± 0.92 and cardiac short-axis of 3.61 ± 0.44. There was no significant difference between VHS VD/DV (P = 0.43) and cardiac short-axis (P = 0.94) values between the hyperthyroid and non-hyperthyroid groups. Among all cats, a more severe total T4 elevation was weakly correlated with a larger VHS lateral (Spearman’s correlation coefficient = 0.23, P = 0.02), but not a greater VHS VD/DV (P = 0.25) or cardiac short-axis (P = 0.56) (Figure 4).

Scatterplot demonstrating the weak correlation between total thyroxine (T4) elevation and vertebral heart score lateral (Spearman’s correlation coefficient = 0.23, P = 0.02). Cats who had total T4 values greater than the maximum reportable value of 24 µg/dl were assigned a total T4 of 24 µg/dl
Of the control cats, 2/46 (4.3%) and 1/46 (2.2%) cats had evidence of left atrial enlargement on the lateral view and VD view, respectively. Of the hyperthyroid cats, 4/52 (7.7%) and 12/52 (23.1%) cats had evidence of left atrial enlargement of the lateral view and VD view, respectively.
Discussion
In this population, hyperthyroidism was significantly associated with a greater VHS on lateral views (P = 0.05), and, among all cats, a more severe elevation in total T4 was correlated with a larger VHS lateral (Spearman’s correlation coefficient = 0.23). However, the relevance of these findings is unclear, as, in this study, the VHS lateral values for hyperthyroid cats (mean 7.75 ± 0.53) exhibited a large degree of overlap with the control cats (mean 7.55 ± 0.54) and with the previously reported normal feline VHS (mean 7.5 ± 0.3 16 or 7.56 ± 0.54 17 ). The mean VHS values for hyperthyroid cats is also lower than the previously identified VHS lateral cutoff of 7.9 as having high diagnostic accuracy in distinguishing cats with left-sided cardiac disorders and moderate-to-severe left atrial enlargement. 17 Potentially, in cats with more severe hyperthyroidism, there is more severe left-sided cardiac disease, which could be reflected as a larger VHS on lateral views, but the correlation between total T4 and VHS lateral values in this study is weak.
To complement objective evaluation, subjective assessment of cardiomegaly was also performed to mimic clinical practice. More hyperthyroid cats had evidence of left atrial enlargement on the VD view (n = 12/52; 23.1%) vs control cats (n = 1/46; 2.2%). However, as evaluation of cardiac chamber enlargement is highly subjective, especially in cases with mild left atrial enlargement, and as intra- and inter-observer evaluation was not assessed in this study, statistical analysis of subjective left atrial enlargement was not performed. Rather, objective VHS and cardiac short-axis measurements were calculated as a substitute for assessment of cardiomegaly. With the addition of subjective evaluation of cardiomegaly, and testing for inter- and intra-observer agreement for such subjective measures, a significant association may be found between hyperthyroidism and cardiomegaly, as previously reported.3,4,14
The results of this study indicate that pulmonary hyperinflation is not identified more commonly in hyperthyroid cats than non-hyperthyroid cats. As there is no significant association between hyperthyroidism and pulmonary hyperinflation, hyperthyroidism is an unlikely differential for radiographic pulmonary hyperinflation. Radiographic features of pulmonary hyperinflation in people include diaphragmatic flattening, depression of the diaphragm (akin to this study’s variable of increased distance between the cardiac silhouette and diaphragm) and visualization of diaphragmatic attachments. 18 These radiographic signs in humans are similar to those infrequently identified in cats in this study. In people affected with hyperthyroidism, the skeletal and intercostal muscles are weakened, which may make a larger contribution to respiratory clinical signs than cardiac abnormalities. 19 This could also occur in cats but potentially to a degree not appreciated radiographically.
The only pulmonary pattern found in hyperthyroid cats in this study was a bronchial pattern, as opposed to a previous study, which found bronchial, bronchointerstitial, interstitial, alveolar, nodular, vascular and mixed patterns in hyperthyroid cats presenting for radioiodine therapy. 4 In addition, only 13/52 (25%) of the hyperthyroid cats in this study had an abnormal pulmonary pattern, whereas 115/194 (59%) of the cats in the previous study had an abnormal pulmonary pattern. However, when excluding other types of pulmonary patterns, the prevalence of a bronchial pattern was similar between our study (n = 13/52; 25%) and the previous study (n = 40/194; 21%). The lack of other pulmonary patterns in our study is likely due to the differences in population between the two studies. This study purposefully excluded patients that presented for coughing, respiratory distress and pulmonary edema. Radiographic pulmonary edema may present as bronchial, interstitial and alveolar patterns in feline patients.20,21 In addition, coughing and respiratory distress may indicate underlying infectious or inflammatory pulmonary disease that could manifest with similar radiographic pulmonary patterns. This differs from the cats that were excluded from the radioiodine study, including those with stage 4 chronic kidney disease, thymoma or insulin-dependent diabetes, as they were deemed unsuitable for radioiodine therapy.
Limitations
There were several limitations to this study. The sample size was small and there may have been insufficient power to detect other significant differences between the control and hyperthyroid groups. Also, at Colorado State University, efforts are consistently made to acquire radiographs at peak inspiration, but this can be highly variable and sometimes unachievable.
Another limitation of this study was the lack of concurrent echocardiography to confirm the presence of structural heart disease in cats with radiographic cardiomegaly and exclude control cats that may have had preclinical cardiomyopathies. The initial goal was to evaluate hyperthyroidism, thoracic radiographs and echocardiography, but with the retrospective nature of the study, only a small number of cats (3/52 hyperthyroid cats, 10/46 control cats) had echocardiograms performed at the time of radiographs, precluding meaningful assessment of echocardiographic findings.
The population at Colorado State University also reflects a referral study population; however, hyperthyroidism is most commonly diagnosed in general practice. The retrospective nature of this study limited the ability to obtain thoracic radiographs at the time of diagnosis, and several of these patients had previous medical treatment of hyperthyroidism with methimazole or diet therapy for an unknown period of time prior to presentation. A previous study showed that methimazole had no effect on echocardiographic variables; however, 12 and thus is unlikely to affect radiographic cardiomegaly, which is more insensitive to cardiac changes than echocardiogram. Even with potential prior treatment, all patients in this study also had confirmed unregulated hyperthyroidism as evident by a persistently elevated total T4. Our control population was not followed to determine if the cats developed hyperthyroidism over time, but lack of hyperthyroidism at the time of thoracic radiographs was confirmed by total T4 testing in this group.
Conclusions
Hyperthyroid cats are more likely to have an increased VHS on lateral views compared with non-hyperthyroid cats and, among all cats, a greater total T4 is correlated with a larger VHS on lateral views. However, the relevance of these findings is unclear, as there is great overlap between the VHS of hyperthyroid and control cats, and only a weak correlation between VHS and total T4 is present. Radiographic pulmonary hyperinflation is not associated with feline hyperthyroidism and is an unlikely differential for this radiographic finding.
Footnotes
Author note
This publication was presented in part as an abstract at the 2021 American College of Veterinary Radiology Annual Scientific Meeting.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.