
Abstract
Objectives
The objective of the study was to identify whether venous blood gas (VBG) variables may serve as a predictor of inflammatory lower airway disease (ILAD) in cats presenting with respiratory distress. A secondary objective of this study was to compare the diagnostic utility of patient signalment, history and physical examination findings, as compared with VBG variables.
Methods
The medical records of cats presenting with respiratory distress secondary to ILAD (54 cases) and non-ILAD (121 controls) were retrospectively reviewed.
Results
No admission VBG variables were predictive of a final diagnosis of ILAD. Comparatively, multivariable analysis identified a history of a cough (P <0.001), increased respiratory rate (P = 0.001), the presence of an abdominal component to respiration (P = 0.007) and the absence of pleural effusion (P <0.01) to be independently associated with a final diagnosis of ILAD. Cats with a history of a cough and an abdominal component to respiration had 7.86 and 5.81 greater odds of being diagnosed with ILAD, respectively. Cats with pleural effusion had 7.43 lower odds of having this final diagnosis. For every 10 breaths/min increase in respiratory rate, cats had 1.48 greater odds of being diagnosed with ILAD. Cats diagnosed with ILAD had a survival rate of 94% (95% CI 84–99%) vs 61% (95% CI 51–70%) for non-ILAD controls (P <0.001).
Conclusions and relevance
The results of this study found patient history and physical examination findings to be more useful predictors of a final diagnosis of ILAD in comparison with VBG variables at presentation. A history of a cough, an abdominal component to respiration and a lack of pleural effusion were found to be significant predictors of this diagnosis. Further investigation into the role of respiratory rate in ILAD is warranted.
Introduction
Dyspnea, or labored and difficult breathing, is a complex neurophysiologic phenomenon, and is a common presenting complaint in critically ill animals. 1 Animals that are presented with acute breathing difficulties are particularly sensitive in nature and the stress of a hospital visit may result in physiological decompensation owing to limited pulmonary reserves. 2 Cats pose a particular challenge as they are notorious for hiding their illness and often are presented in a later stage of disease.3–5 As a result, cats are often evaluated in vulnerable states and may be prone to respiratory arrest. Performing an efficient triage evaluation, establishing an accurate diagnosis and initiating a rapid stabilization plan for cats presenting with apparent dyspnea is of utmost importance to the emergency veterinarian.3,5,6
Numerous studies have investigated various features of apparent feline dyspnea to aid in the identification of underlying disease processes.3,5–8 However, the vast majority of these studies have focused on the identification of cats with cardiac-related respiratory signs secondary to congestive heart failure (CHF).9–13 Despite these recent contributions to the literature, there has been a paucity of veterinary studies focusing on one of the major differential diagnoses for respiratory distress in the cat: inflammatory lower airway disease (ILAD). 5
ILAD, encompassing both feline asthma and chronic bronchitis, is a group of complex pathologic conditions of the airways. While feline asthma is characterized by reversible bronchoconstriction, airway hyperreactivity and increased mucus production thought to be associated with a type I hypersensitivity reaction to aeroallergens, chronic bronchitis is typically defined as a 2-month history of a persistent cough in the absence of another identifiable cause.14–17 Cats with feline asthma or chronic bronchitis both have the potential to present with acute respiratory distress, though this is more commonly considered to be characteristic of feline asthma.3,7,14,17–20 Ultimately, the diagnosis of ILAD is based on a combination of historical and physical examination findings, radiographic, bronchoscopic and bronchoalveolar lavage abnormalities (if performed), and response to therapy. As there has yet to be established a pathognomonic finding associated with the diagnosis of ILAD, various investigators have sought to identify clinically relevant biomarkers to aid in rapid disease identification. 7 Immunoglobulins,16,20–22 gaseous breath components,23,24 exhaled breath condensates23,25–27 and inflammatory proteins 19 have all been investigated in relation to aiding in the identification of ILAD; however, significant limitations have prohibited the clinical application of many of these markers in the emergency setting.7,15
Recent investigations in people have evaluated the potential role of venous blood gas (VBG) variables as a screening tool and outcome predictor in the emergency department (ED) for various pathologic respiratory conditions resulting in acute respiratory distress such as chronic obstructive pulmonary disease and asthma.2,28–35 Lund et al found that a high level of venous total carbon dioxide (TCO2) at hospital admission was a significant independent predictor of 1-year hospital readmission and death in a heterogenous population of human patients presenting with acute dyspnea. 28 However, the utility of VBG analysis in acute exacerbations of respiratory disease has been questioned and its role in the ED remains an area of active investigation.31–35 In the veterinary field, increasing venous partial pressure of CO2 (PvCO2) levels at hospital admission have recently been found to be associated with increased mortality in premature calves with respiratory distress syndrome. 36 The diagnostic and prognostic value of venous CO2 variables has yet to be investigated in animals with respiratory distress and these variables may have utility in disease states such as ILAD where ventilation may be affected by marked bronchoconstriction and mucus production.14–16 Anecdotally, the study authors have recognized that some cats ultimately diagnosed with ILAD have an elevated PvCO2 at admission.
Therefore, the primary objective of this study was to identify whether admission VBG variables may serve as a predictor of a final diagnosis of ILAD in cats presenting with acute respiratory distress. A secondary objective of this study was to investigate other additional predictors of ILAD such as patient signalment, history and physical examination findings as compared with admission VBG variables. We hypothesized that PvCO2, TCO2 and bicarbonate (HCO3‒) levels would be significantly higher and venous pH and base excess would be significantly lower in apparently dyspneic cats diagnosed with ILAD compared with cats that were presented with other causes of respiratory distress. Additionally, we hypothesized that alterations in VBG variables at presentation would be more useful than patient history, signalment and physical examination findings to predict a diagnosis of ILAD.
Materials and methods
Medical records of all cats admitted to the Mathew J Ryan Veterinary Hospital, University of Pennsylvania were searched via the hospital records database from July 2009 to July 2019 with a discharge keyword diagnosis of ‘asthma’ to establish a case population of cats that were presented to the emergency service with ILAD-related respiratory distress. Respiratory distress secondary to ILAD was defined as cats that showed a clinical response (ie, improved respiratory rate and effort) to corticosteroid and or bronchodilator therapy, 14 had three-view thoracic radiographs where a diagnosis of ILAD (ie, feline asthma) was prioritized as per a board-certified radiologist,14,17,37,38 and where the attending clinician reported a final diagnosis of ILAD or feline asthma within the medical record.
The university hospital’s radiology report database was subsequently searched during the same time period for reports of thoracic radiographs with a search term of ‘dyspnea’, ‘respiratory distress’ or ‘respiratory effort’ to yield a preliminary control group population. All radiology reports included a patient history that was provided at the time of the radiology request. Manual inspection of all patient records was then performed to obtain a control population of apparently dyspneic cats presenting to the emergency service with non-ILAD etiologies. In control cases of respiratory distress with an unknown etiology, ILAD was excluded as a differential owing to lack of radiographic findings supportive of the diagnosis, no response to bronchodilator or steroid therapy and no indication of ILAD at follow-up visits.
Inclusion criteria for both case and control groups consisted of admission through the emergency service, apparent dyspnea noted by the triage nurse or clinician at presentation a VBG obtained at presentation and thoracic radiographs obtained within 24 h of presentation. Cats were excluded from the study if they died or were euthanized prior to obtaining a VBG and thoracic radiographs, were presented in cardiopulmonary arrest or if the medical records were inadequate. Cases of ILAD that had been previously diagnosed prior to presentation to the emergency service were also excluded from the study. Cats that were presented with apparent dyspnea secondary to a spontaneous pneumothorax were excluded from the control group owing to their potential association with an underlying diagnosis of feline asthma. 39 Comparison groups were defined as ILAD-related (cases) and non-ILAD-related respiratory distress (controls).
Data recorded for all cats included breed, sex, reproduction status, age, weight, whether there was a history of a cough, rectal temperature, heart rate, respiratory rate, the presence of an abdominal component to respiration (eg, an expiratory push), wheezes and the presence of a heart murmur and/or a gallop sound. Normal heart rate, respiratory rate and rectal body temperature were defined as 160–220 beats/min, 40 <40 breaths/min 40 and 38.1–39.2°C, 41 respectively, for all cats.
In cats that had a point-of-care (POC) thoracic ultrasound performed, the presence or absence of pleural effusion was recorded. 42 Cytologic findings were recorded if an endotracheal wash was performed. VBG variables recorded at presentation included pH, PvCO2, lactate, TCO2, base excess of extracellular fluid (BE) and HCO3‒. The final diagnoses of all cats in the control group were recorded.
Survivors were defined as all cats that survived to discharge, excluding those that returned to the hospital within 24 h for euthanasia pertaining to ILAD-related disease. Non-survivors were defined as cats that either died or were euthanized in addition to those that returned to the hospital within 24 h for euthanasia pertaining to respiratory-related disease. Cats that were discharged against medical advice or transferred to another veterinary hospital were excluded from survival outcome analysis.
Statistical analysis was performed with a commercially available computer program (STATA IC, version 15.1; StataCorp). The Shapiro–Wilk test was used to assess continuous variables for normality. Descriptive statistics consisted of the mean ± SD for normally distributed variables and the median (range) for variables that were not normally distributed. The count and percentage were used to report frequency data. Fisher’s exact test was used to compare all proportions. Continuous variables were compared between groups using the two-sample independent t-test for normally distributed variables and the Wilcoxon rank-sum test for data that were not normally distributed. The Wilson estimator was used to calculate 95% confidence intervals (CIs) for percentages equal to 0% and 100%; the binomial exact method was used to calculate 95% CIs for all other proportions. For all comparisons, P <0.05 was considered statistically significant.
Variables potentially significant in univariable analyses (P <0.2) were considered for inclusion in a multivariable logistic regression model to look for an independent association with the final diagnosis of ILAD. Variables were evaluated for multicollinearity using Spearman’s rank correlation coefficient with a critical rs value of <0.7. The addition of second-degree polynomials for the variables of interest was performed to assess for linearity in the logit form. Backwards stepwise logistic regression was subsequently performed. Confounding was set at ⩾20% change in any remaining covariate and significance was evaluated at the 0.05 alpha level for the null hypothesis that the effect (slope) of the covariate was 0. Covariates with P values >0.2 from the univariable logistic regression were sequentially added into the intermediate model to determine significance (P <0.05), resulting in the main-effects model.
A 5% significance level was then used to sequentially reassess the linearity of covariates and the presence of significant two-way interactions in the main-effects model. Regression diagnostics were then used to assess the final main-effects model. The link test for model specification, Pearson’s χ2 and Hosmer–Lemeshow χ2 were used to evaluate the goodness-of-fit of the model at the 0.05 alpha level. The final model was graphically assessed with standard residuals and a receiver operating characteristic curve. Associations between significant variables and the primary outcome were reported as odds ratios, representing a greater or lesser likelihood of being diagnosed with ILAD.
Results
A computer search of the hospital records database from July 2009 to July 2019 yielded 523 cats that were presented to the ED with a discharge keyword diagnosis of ‘asthma’. A computer search of the hospital’s radiology report database during the same time period yielded 378 cats with reports of thoracic radiographs with a search term of ‘dyspnea’, ‘respiratory distress’ or ‘respiratory effort’. A total of 469 and 257 cats were excluded from the case and control groups, respectively. Reasons for exclusion are outlined in Figure 1. Subsequently, a total of 54 ILAD cases and 121 non-ILAD controls were included in the study.
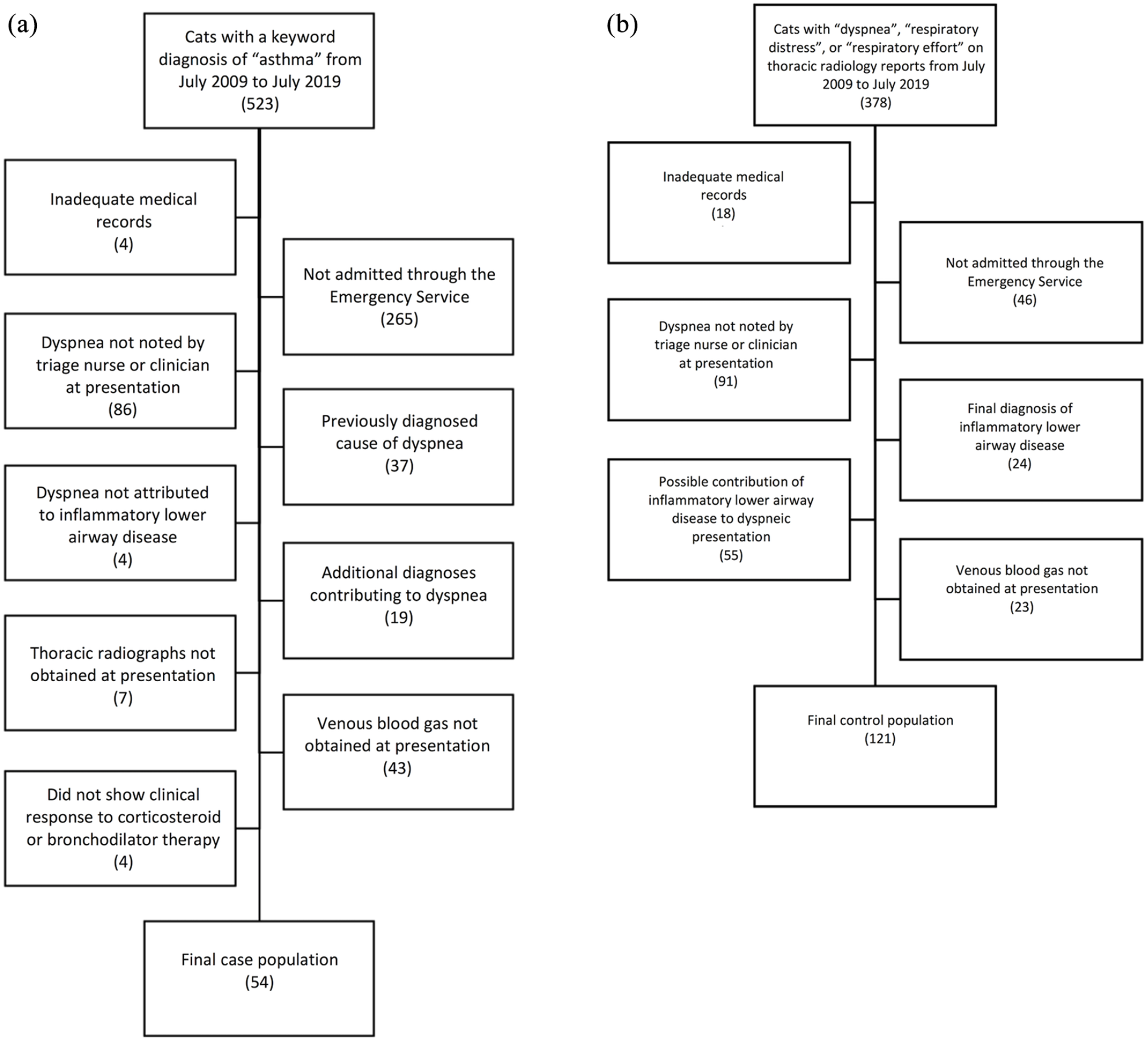
Flow diagram showing the selection process for (a) cats presenting to the emergency service with respiratory distress secondary to inflammatory lower airway disease; and (b) non-inflammatory lower airway disease-related respiratory distress controls
Age, physical examination, history of a cough and VBG variables for ILAD cases and non-ILAD controls are summarized in Table 1. Of the ILAD cases, 29 (54%; 95% CI 40–67) cats were castrated males, 21 (39%; 95% CI 26–53) cats were spayed females, two (4%; 95% CI 0–13) cats were intact males and two (4%; 95% CI 0–13) cats were intact females. Thirty-nine cats were domestic shorthairs (DSH), 10 cats were domestic longhairs (DLH) and two cats were Siamese. There was one cat each of the following breeds: Maine Coon, Bengal and Russian Blue. Non-ILAD controls consisted of 67 (55%; 95% CI 46–64) castrated male cats, 39 (32%; 95% CI 24–41) spayed female cats, eight (7%; 95% CI 3–13) intact male cats and seven (6%; 95% CI 2–12) intact female cats. Eighty-six cats were DSH, 17 cats were DLH, eight cats were classified as other, four cats were Maine Coons, four cats were Persians and two cats were Oriental Shorthairs. There was no difference in sex or breed between cases and controls.
Age, physical examination, history of a cough and venous blood gas variables for cases presented to the emergency service with respiratory distress secondary to inflammatory lower airway disease (ILAD; n = 54) and for controls presented to the emergency service with non-ILAD-related respiratory distress (n = 121)

Non-parametric distribution, Wilcoxon rank sum test
Parametric distribution, two-sample independent t-test
HR = heart rate; RR = respiratory rate; PvCO2 = venous partial pressure of CO2; TCO2 = total carbon dioxide; BE = base excess of extracellular fluid; HCO3‒ = bicarbonate
Cats with ILAD were significantly younger (P <0.001) and more likely to have a history of a cough (P <0.001) and an abdominal component to respiration (P = 0.033) than non-ILAD controls at the univariate level. Cases of ILAD were also less likely to have a gallop sound (P = 0.031) and pleural effusion identified on POC ultrasound or thoracic radiographs (P <0.001) than controls. At the univariate level, cats with ILAD had lower rectal temperatures (P = 0.012), higher heart rates (P = 0.003), higher respiratory rates (P = 0.003) and higher venous pH (P = 0.01) than non-ILAD controls. There was no significant difference with respect to the presence of wheezes or a heart murmur on physical examination, PvCO2, lactate, TCO2, BE or HCO3‒ concentrations between cases of ILAD and non-ILAD controls.
Of the 54 cases of ILAD, 29 (54%) cats had a pure bronchial pattern and 20 (37%) cats had a bronchointerstitial pattern on three-view thoracic radiographs. Of the remaining five cats, two had a mild interstitial pattern with suspected mucus plugging, one had a mild generalized interstitial pattern, one had marked pulmonary hyperinflation, despite no bronchial pattern and one had a patchy alveolar pattern with peri-bronchial cuffing. Nine (17%) of the ILAD cases were noted to have evidence of peri-bronchial cuffing. Tubular, nodular or amorphous soft-tissue opacities suspected to be secondary to mucus plugs were noted in 13 (24%) cats. Hyperinflation was present in 10 (19%) cats and suspected collapse of the right middle lung lobe was identified in 16 (30%) cats.
Four (7%) ILAD cats had an endotracheal wash performed; two (50%) showed eosinophilic inflammation and one (25%) showed mixed inflammation. One (25%) ILAD cat had mild hemosiderosis on endotracheal wash cytology in the absence of eosinophilic or neutrophilic inflammation. Three (2%) non-ILAD cats had an endotracheal wash performed, two (67%) of which showed neutrophilic inflammation. One of the non-ILAD cats with neutrophilic inflammation was diagnosed with chronic suppurative pneumonia. The other cat had evidence of moderate diffuse pulmonary edema with interstitial congestion on post mortem suspected to be secondary to severe systemic inflammation associated with either suppurative cholangitis or intestinal small-cell lymphoma. The third non-ILAD cat was diagnosed with pulmonary carcinoma and had a negative endotracheal wash culture.
The final diagnoses listed on the discharge notes of all non-ILAD cats in the control group are summarized in Table 2. Cats were permitted to have more than one final diagnosis. Of the non-ILAD control cats with a final diagnosis of CHF (n = 35 [29%]), three (9%) cats had a history of a cough.
Final diagnoses listed on the discharge notes of all control cats presented to the emergency service for non-inflammatory lower airway disease-related respiratory distress (n = 121)*
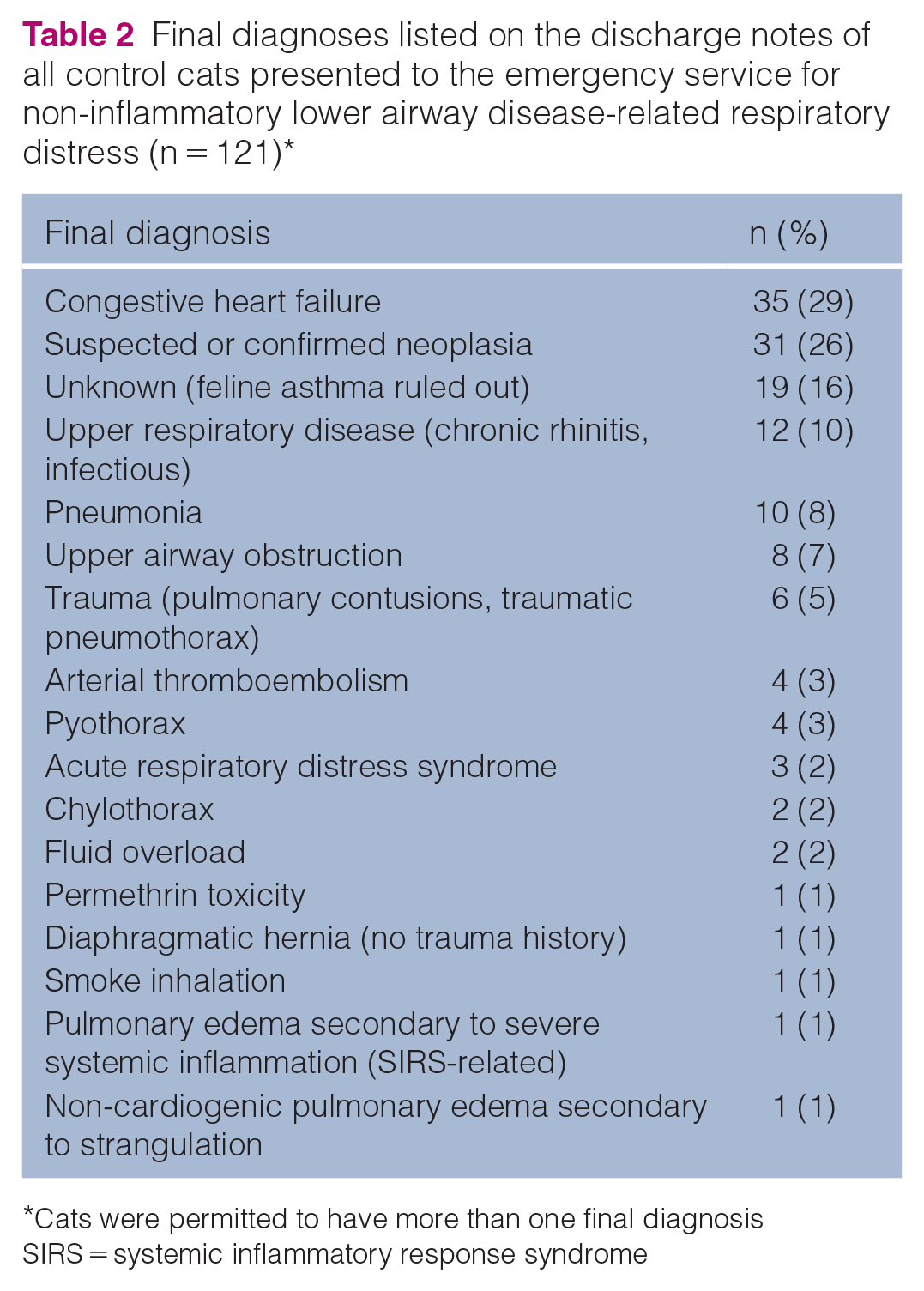
Cats were permitted to have more than one final diagnosis
SIRS = systemic inflammatory response syndrome
Four (7%) cases of feline ILAD had scant pleural effusion noted at presentation following POC ultrasound assessment. Possible scant pleural effusion was noted on thoracic radiographs in two (50%) of these cats, while this was not noted for the other two cats. None of these cats required a needle thoracocentesis. Three (75%) of these cats had complete cardiac evaluations including an echocardiogram and were assessed not to be in CHF, nor was there any evidence of pleural effusion on echocardiogram. The remaining cat did not have an echocardiogram performed, although pleural fluid was noted to have completely resolved on re-check with POC ultrasound within 24 h. All four cats responded to medical therapy of feline ILAD. Comparatively, 47 (39%) of the non-ILAD control cats had pleural effusion of various severity noted at presentation on either POC ultrasound, thoracic radiographs or both.
One (2%; 95% CI 0–10) ILAD cat and two (2%; 95% CI 0–6) non- ILAD control cats were discharged against medical advice. None (0%; 95% CI 0–7) of the ILAD cats and two (2%; 95% CI 0–6) non-ILAD control cats were transferred to another veterinary hospital for continued care. Two (4%; 95% CI 0–13) of the ILAD cats and none (0%; 95% CI 0–3) of the non-ILAD control cats were returned to the hospital within 24 h for euthanasia pertaining to respiratory-related disease. Consequently, 53 cases of ILAD and 117 non-ILAD controls were included in survival outcome analysis. Fifty (94%; 95% CI 84–99) cats diagnosed with ILAD and 71 (61%; 95% CI 51–70) cats with non-ILAD-related respiratory distress were classified as survivors (P <0.001, Fisher’s exact test). Of the three (6%; 95% CI 1–15) ILAD non-survivors, all three (100%; 95% CI 29–100) cats were euthanized. Of the 46 (39%; 95% CI 30–49) non-ILAD non-survivors, 43 (93%; 95% CI 82–99) cats were euthanized and three (7%; 95% CI 1–18) cats died naturally (P = 1.0).
Following univariate analysis, variables included for assessment in the multivariable logistic regression model included age, a history of a cough, rectal temperature, heart rate, respiratory rate, the presence of an abdominal component to respiration, wheezes, a heart murmur, gallop sound, pleural effusion, venous pH, lactate, TCO2, BE and HCO3‒. All continuous variables of interest were linearly related to the outcome of a final diagnosis of ILAD. Respiratory rate was divided by a factor of 10 for inclusion in the model to evaluate changes of 10 breaths/min for clinical relevance. Venous TCO2, BE and HCO3‒ were identified as collinear following assessment for multicollinearity. As a result, the potential significance of each variable was independently assessed in three serial model developments, all of which yielded an identical final main effects model. Following multivariable analysis, a history of a cough (P <0.001), respiratory rate (P = 0.001), the presence of an abdominal component to respiration (P = 0.007) and absence of pleural effusion (P = 0.01) were found to be independently associated with a final diagnosis of ILAD. No admission VBG variables were associated with a final diagnosis of ILAD. Rectal body temperature persisted in the final model as a significant confounder of respiratory rate and pleural effusion, although it was not found to be independently associated with a final diagnosis of ILAD (P = 0.429). Cats with a history of a cough and an abdominal component to respiration noted on physical examination had 7.86 and 5.81 greater odds of being diagnosed with ILAD, respectively. For every 10 breaths/min increase in respiratory rate at presentation, cats had 1.48 greater odds of being diagnosed with ILAD, while cats with pleural effusion at presentation had 7.43 lower odds of having this final diagnosis. Model diagnostics demonstrated reasonable fit (Pearson’s χ2 P = 0.123; Hosmer–Lemeshow χ2 P = 0.753; area under receiver operating characteristic curve = 0.876) with a final model pseudo-R2 value of 0.352. Repeat analysis excluding cats with an unknown final diagnosis from the control group did not result in any changes to the predictors found to be independently associated with a final diagnosis of ILAD.
Discussion
The aim of this retrospective study was to identify whether admission VBG variables may serve as predictors of a final diagnosis of ILAD in cats presenting with acute respiratory distress. Additionally, this study served to investigate whether VBG variables were useful diagnostic predictors of ILAD, compared to patient signalment, history and physical examination findings.
While it was hypothesized that PvCO2, TCO2 and HCO3‒ levels would be significantly higher and venous pH and BE levels would be significantly lower in apparently dyspneic cats diagnosed with ILAD compared with cats that were presented with other causes of respiratory distress, this study found no significant difference between the case and control group populations for these variables of interest. Furthermore, despite the wide range of values identified in both groups for VBG variables, the median PvCO2 and BE and mean TCO2 and HCO3‒ were relatively unremarkable values for both populations of interest. Additionally, we hypothesized that alterations in VBG variables at presentation would be more useful than patient history, signalment and physical examination findings to predict a diagnosis of ILAD. The results of this study are inconsistent with this hypothesis and rather our study results support that the patient history and physical examination findings as more useful clinical tools compared with VBG variables at presentation.
Recurrent episodes of coughing have been reported as one of the most common clinical presentation of ILAD in previous studies.17,37,38,43 Additionally, paroxysmal coughing is often cited as a defining feature of the disease paired with episodes of respiratory distress.14,15,39 To our knowledge, the clinical implication of a historical cough has yet to be evaluated in a heterogenous group of cats presenting with apparent dyspnea. Consistent with these reports, we found that cats with a history of a cough were significantly more likely to be diagnosed with ILAD, compared with any other cause of respiratory distress. The development of a cough in ILAD has been attributed to tracheobronchial inflammation, stimulation of epithelial cough mechanoreceptors, excessive airway secretions and bronchoconstriction.40,44
CHF was the most common final diagnosis of control cats accounting for 29% of control cases in this study. This is consistent but slightly lower than previous descriptive heterogenous studies of feline respiratory distress where CHF is the most common reason for respiratory distress accounting for up to 65% of the cases.5,9,44 In differentiating ILAD from CHF, it is important to note that cats with cardiac-associated apparent dyspnea rarely have a history of coughing. 45 Our study confirmed this finding with significantly more asthmatic cats (54%) having a history of cough compared with the control cases (17%) (P <0.001). Although coughing is considered to be a rare clinical finding in CHF, a recent study reported a history of coughing in 25% of their population of dyspneic cats diagnosed with CHF; 9 in our study, we found a much lower rate of cough identified in only 9% of the control cats with CHF, which supports a low frequency of this finding. Therefore, based on our study results, a historical cough reported in a cat that is presented for apparent dyspnea should increase the suspicion for a final diagnosis of ILAD.
Increased respiratory effort at the end of expiration has been reported in association with lung hyperinflation, a finding commonly associated with ILAD.14,15,17,38,39 Globally, the appreciation of an abdominal component to the respiration, regardless of the pattern, has typically been attributed to increased work of breathing. However, an ‘expiratory push’ has more commonly been used to describe the breathing pattern observed in cases of ILAD in the face of increased expiratory resistance secondary to bronchoconstriction and excess mucus production. 14 Similarly, in a previous study in cats, the presence of apparent expiratory dyspnea has been found to be significantly associated with lower airway disease localization. 3 The present study found that cats with an abdominal component to respiration noted on physical examination were more likely to be diagnosed with ILAD. While the retrospective nature of the study and inconsistent recording in the medical records precluded the ability to reliably investigate a specific expiratory component to respiration, the finding of an abdominal component to respiration may have been due to an expiratory push and apparent expiratory dyspnea as was noted in the aforementioned study.
Although respiratory rate has been previously deemed an inutile physical examination finding in the localization of respiratory disease,3,5 the present study identified a significant independent association between increasing respiratory rate at presentation and a final diagnosis of ILAD. However, the difference in median respiratory rate of asthmatic cases was 8 breaths/min higher than that of the non-ILAD controls, which has questionable clinical relevance particularly when accompanied by a relatively low odds ratio. While a retrospective assessment of 90 cats presenting to a referral hospital for dyspnea found no difference in respiratory rate between cardiac, respiratory, neoplastic and traumatic etiologies, 5 an increased respiratory rate has been suggested as a possible indicator of respiratory compromise attributed to a cardiac etiology. 46 Dickson et al 9 provided support for this claim as a respiratory rate greater than 80 breaths/min was found to be a useful predictor of apparent cardiac-associated dyspnea at the univariate level in a recent retrospective study of cats in primary practice, although this variable was removed upon further multivariate analysis. 9 In a different study, fast and shallow breathing was noted to be more common in cats that were ultimately diagnosed with no respiratory abnormalities, compared with cats with underlying respiratory pathology in a heterogenous population of cats presenting with respiratory distress. 3 The authors of the study suspected that this finding may have been related to anxiety, pain or shock. 3 Further research is needed in order to draw definitive conclusions pertaining to the significance of respiratory rate in differentiating between causes in cats that are presented for apparent dyspnea and the authors caution extrapolation of the findings of our study.
The greatest odds ratio identified in the multivariate model for the prediction of a final diagnosis of ILAD was associated with the absence of pleural effusion at presentation. To our knowledge, pleural effusion has yet to be reported in association with ILAD and it was found to be only a rare finding in the present study. Pleural effusion is typically reported secondary to hemothorax, chylothorax, pyothorax, cardiac disease, neoplasia, lung lobe torsions, feline infectious peritonitis or vasculitis in cats. 5 However, this finding has also been reported in cases of feline primary parenchymal disease such as pneumonia.8,47 The presence of scant fluid within the pleural space of the ILAD cats in the present study may have been a variation of normal; alternatively, it may have occurred secondary to vascular leakage associated with a systemic inflammatory response. Additionally, these POC thoracic ultrasound examinations were performed by a veterinarian in the emergency service and findings were not confirmed by a board-certified radiologist, the findings were not repeatable on echocardiogram evaluations and only 2/4 cats had possible scant pleural effusion, also noted on thoracic radiographs. Consequently, the presence of pleural effusion may have been incorrectly identified.
The overall survival rate for cats with feline ILAD-related respiratory distress was 94% in this study which was significantly higher than the 61% survival rate in non-ILAD cats. This finding highlights that despite the presence of apparent dyspnea at emergency presentation, a diagnosis of ILAD has a very good prognosis for survival to discharge. While there is a scarcity of data reporting survival rates specific to ILAD-associated respiratory distress, one study found a similar excellent prognosis with 92% of cats diagnosed with feline bronchial disease surviving to discharge, although this study likely included less severely affected cats as apparent dyspnea was not an inclusion criterion. 18 Finally, a slightly lower survival rate of 80% with 4/5 cats surviving to discharge was found in a small case series of cats that developed pneumothorax secondary to asthma. 39
This study is primarily limited by its retrospective nature and reliance on accurate medical records over a relatively prolonged time period. As a concrete definition of ILAD is lacking within the literature, the definition used for case inclusion in this study is not without limitations. Only a small percentage of cats had an endotracheal wash performed and none of the ILAD cats underwent bronchoscopic studies, limiting the utility of these diagnostic tools as inclusion criteria. Additionally, owing to the retrospective nature of the study, additional contributions to the clinical signs observed in the ILAD group such as secondary bacterial pneumonia and parasitic infections could not definitively be ruled out. However, medical records were carefully reviewed in an attempt to exclude cases where additional diagnoses were thought to be potential contributors to the observed clinical signs. Furthermore, the control group is inherently limited by the search mechanism used in this study. A bias for a higher illness severity among non-ILAD controls was likely present which may contribute to the outcome differences and may have an impact on reported VBG variables. Among the control group, 19 (17%) cats were included with an unknown final diagnosis, despite the exclusion of ILAD. The majority of these cases were presented with respiratory distress, had unremarkable thoracic radiographs and improved without specific intervention. In addition, there was no evidence of feline asthma or chronic bronchitis noted upon review of future hospital visits for these cases. The presence of unremarkable thoracic radiographs has been previously reported in cases of feline asthma and therefore inclusion of these cases among the control group serves as a potential limitation in the event that these cats had underlying ILAD that was not detected. 48 However, repeat analysis following exclusion of cats with an unknown final diagnosis did not result in any changes to the predictors found to be independently associated with a final diagnosis of ILAD. With respect to both case and control groups, this study, owing to its retrospective nature, was unable to reliably grade the varying degrees of apparent dyspnea at presentation.
All cases included in the study had a VBG obtained at presentation which introduced an immediate selection bias. It is possible that cases considered too unstable for intravenous catheter placement and VBG sampling were inadvertently excluded, which may have contributed to the relatively high survival rate found in this study. Furthermore, given the traditional thought that a historical cough may be associated with ILAD, a bias may have existed among attending clinicians toward this diagnosis and is an inherent limitation of the association between a historical cough and ILAD found in this study. Additionally, VBG sampling may not have occurred immediately at emergency presentation as cats may have been placed directly into an oxygen cage and bronchodilator therapy may have been administered prior to blood sampling, which may have affected the results. Flow-by oxygen was also likely provided at the time of blood sampling as this is standard of care in our hospital for cats with respiratory distress which may have additionally affected the VBG results.
Conclusions
ILAD remains a complex and prevalent condition that has the potential to manifest itself in severe life-threatening respiratory distress in cats. Obtaining a rapid diagnosis and instituting stabilization measures, such as initiation of bronchodilator therapy, is essential to the successful management of these cases. The results of this study have found that admission VBG variables are not predictive of a final diagnosis of ILAD. A patient history of a cough, the physical examination finding of an abdominal component to breathing efforts and the absence of pleural effusion on POC ultrasound were found to be more useful predictors of a final diagnosis of ILAD in comparison with VBG variables at presentation. While higher respiratory rates were associated with a final diagnosis of ILAD, the clinical application of this finding remains questionable and requires further investigation. Additional large-scale prospective and multicenter studies are required to further elucidate the complexities of ILAD in cats and aid in the establishment of additional diagnostic predictors and biomarkers applicable to the veterinary emergency and critical care setting.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.