
Abstract
Objectives
The aim of this study was to characterise and describe patterns of temporomandibular joint (TMJ) injuries occurring in cats using CT.
Methods
A cross-sectional study was carried out in adherence with the STROBE guidelines. Among the medical and CT records of 79 cats, 158 TMJs were reviewed in a collaborative study between six institutions.
Results
TMJ injuries were most commonly unilateral, representing 70.9% of cases. The mandibular condyle was fractured in 88 cases (55.7%) of the 158 TMJs observed. Of those, 84.0% were intra-articular condyle fractures, with the medial half of the mandibular condyle over-represented. Luxations occurred in 32.9% of cases, which was 19.0% of all evaluated TMJs. Rostrodorsal luxations were most common representing 87.0% of all luxations. Temporal bone fractures were observed in 30.4% of all cases, which was 18.4% of TMJs. The majority of fractures were of an unknown cause. When the cause was determined, road traffic accident (RTA) was the most frequent, followed by animal interaction, other external forces (sharp or blunt force) and high-rise trauma. Bilateral injuries were 13.1 times more likely to occur in high-rise trauma (P = 0.01) and temporal bone fracture was significantly associated with RTAs (P = 0.016). No other significant associations were observed between cause of injury and the resulting TMJ injury pattern.
Conclusions and relevance
Various TMJ injury patterns can occur in cats as a result of trauma. Intra-articular fractures of the medial half of the mandibular condyle occur most commonly. Although unilateral injuries are more frequent, high-rise trauma tends to present with bilateral lesions. Further studies with a larger sample size should be performed to better understand TMJ patterns of injury and how they relate to possible causes.
Introduction
Fractures involving the temporomandibular joint (TMJ) account for between 50% and 56% of all maxillofacial fractures.1–3 The most frequent cause depends on the studies reported, and include road traffic accident (RTA)2,3 and high-rise trauma. 1 Although these studies described mandibular injuries in some detail, TMJ injuries were only assessed using plain film radiography.1–3 Considering the reported 10% prevalence of ankylosis after TMJ trauma 1 there is a need to further understand, in more detail, which TMJ injuries might lead to ankylosis, in order to guide the preoperative decision-making. In human oral and maxillofacial surgery, CT is the preferred method of imaging complex fractures as it allows the high-quality assessment of the cortical bone. 4
TMJ fracture patterns in cats have not been previously characterised by CT despite several publications reporting maxillofacial trauma in this species.2,3,5 Therefore, the aim of this study was to use CT to classify TMJ fracture configurations in cats and to understand how that relates to cause.
Materials and methods
A cross-sectional study was carried out in adherence to the STROBE checklist. 6
CT scans and the clinical records of cats presenting with a TMJ injury were retrospectively reviewed from six international university veterinary hospitals. Cats had to have presented with suspected or witnessed trauma and have no history of prior trauma or documented skeletal abnormalities.
Records from clinical cases with a diagnosis of maxillofacial trauma were consulted retrospectively, from 2007 to 2021: 34 cases were from the University of London’s Royal Veterinary College (2010–2020), 18 from the College of Veterinary Medicine, Cornell University (2007–2020), 10 cases from the Faculty of Veterinary Medicine, University of Lisbon (2020–2021), eight cases from the College of Veterinary Medicine, University of Minnesota (2008–2021), five cases from the School of Veterinary Medicine, University of Wisconsin-Madison (2010–2020) and four cases from the Louisiana State University School of Veterinary Medicine (2007–2019).
The CT equipment used included the Aquilion 64, Aquilion 16 and Astelion 16 (Toshiba Medical Systems); Aquilion ONE Genesis Edition (Canon Medical Systems); and the GE Light Speed 16 and 8 (GE Healthcare).
Clinical variables including age and weight and cause of the injury were analysed.
CT images of 79 cases were reviewed by three authors and a consensus was reached. A total of 158 TMJs were evaluated individually. TMJ injury classification was adapted from Arzi and Lantz7 and from Neff et al, 8 and classified according to the following criteria: presence of subluxation; luxation (rostrodorsal vs ventrocaudal); or fracture. Fractures were classified as extra-articular or intra-articular. Intra-articular fractures were classified into type A = lateral 1/2, type B = medial 1/2, type C = comminuted, type D = simple with mandibular fossa (MF) fracture and type E = comminuted with MF fracture (Figure 1). Extra-articular fractures were classified into without override, with lateral override, with medial override or comminuted (Figure 2). Fracture of the temporal bone that makes up the mandibular fossa was also recorded (Figure 3). Finally, unilateral or bilateral occurrence was recorded.

Intra-articular temporomandibular joint fractures in axial slice (a) of the lateral half, (b) medial half, (c) comminuted, (d) simple with mandibular fossa fracture and (e) comminuted with mandibular fossa fracture

Extra-articular temporomandibular joint fractures (a) with lateral override in coronal slice, (b) with medial override, (c) without override and (d) comminuted
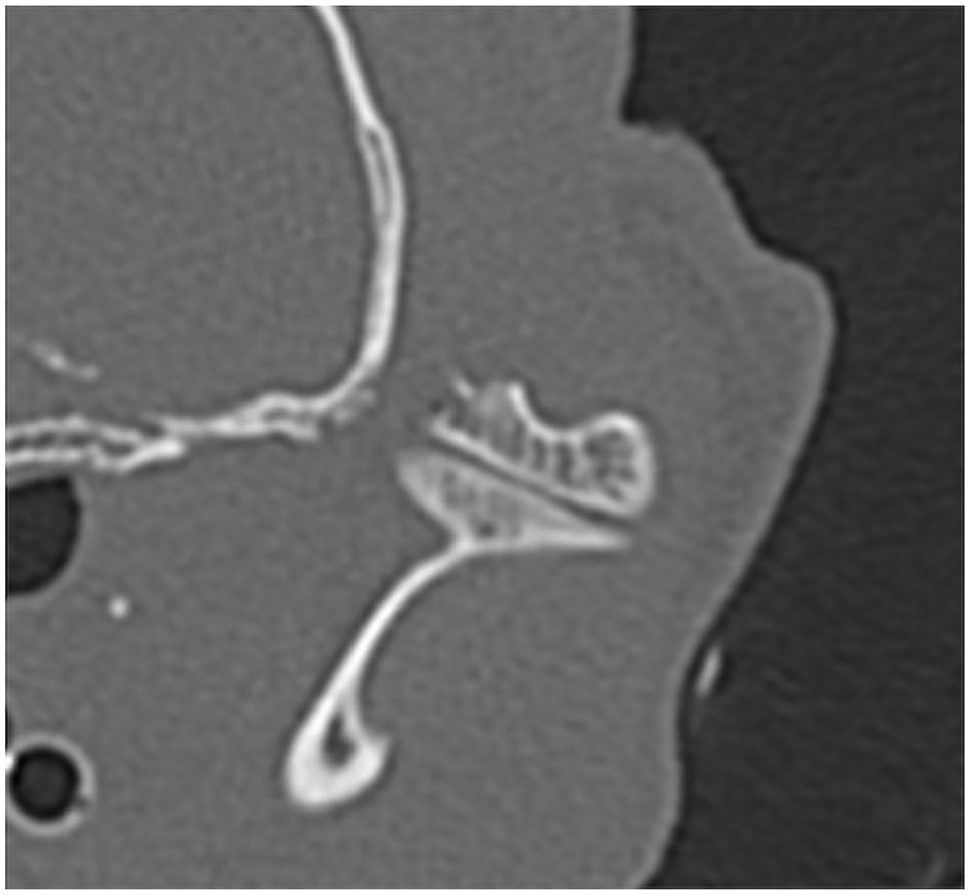
Axial slice of a fracture of the temporal bone at the level of the mandibular fossa
Results were evaluated using commercial software packages for the calculation of descriptive (Microsoft Excel for Mac version 16.49) and inferential statistics (IBM SPSS Statistics for Mac version 26). Categorical variables were expressed as frequencies. χ 2 tests or Fisher’s exact tests were used to assess the association between injury patterns. To determine the effects of cause on injury patterns, univariate logistic regression was used. A P value <0.05 was considered significant for a 95% confidence interval.
Results
CT scan slice thickness and pitch for all examinations ranged from 0.3 to 1.3 mm and from 0.5 to 1 mm, respectively.
Demographics and classification of injuries
Of the 79 clinical cases included in the study, 49 were male (62%) and 30 were female (37%). One case did not have a recorded age. Mean ± SD age and weight were 5.02 ± 3.96 years and 4.48 ± 1.39 kg, respectively.
Unilateral injuries were present in 56 cases (71%) and bilateral injuries in 23 cases (29%). TMJ luxation was observed in 26 cases (32.9%) and subluxation was observed in 17 cases (21.5%). Some type of fracture occurred in 68 cases (86.1%). Mandibular condyle fractures were found in 67 cases (84.8%) and temporal bone fracture in 24 (30.4%). Intra-articular fractures occurred in 61 cases (77.2%) and extra-articular in 26 cases (32.9%).
When assessing the 158 TMJs individually, 220 total injuries were identified, including coexisting mandibular fractures (see Table 1 in the supplementary material). Thirty were luxations (19.0%) and 17 were subluxations (10.8%). Of the 30 luxations observed, 26 (87%) were rostrodorsal and four (13.3%) caudoventral. In four cases, the luxation injuries were bilateral and were all rostrodorsal on both sides. Caudoventral luxations were always unilateral.
The mandibular condyle was fractured in 88 cases (55.7%) of the 158 TMJs observed. In the 88 mandibular condyle fractures, a total of 105 injury types were observed. Of those, 76 were intra-articular and 29 were extra-articular. In 15 mandibular condyles intra- and extra-articular fractures were simultaneously observed. The relative probability of mandibular condyle fracture patterns is illustrated in Figure 4. With regard to intra-articular fracture type, medial intra-articular fractures were the most common (30/105 fractures [28.6%]). With regard to extra-articular fractures, comminuted fractures were the most common and represented 20/105 fractures (19.0%) (Figure 4). Temporal bone fractures (including or not glenoid fossa) were observed in 31/158 TMJs (19.6%). Fractures beyond the condylar neck were registered as coexisting mandibular fractures, observed in 32 cases (40.5%).

Relative probability of 105 mandibular condyle fracture patterns
No significant associations were found between the following variables: luxation, fracture of the pars squamosa of the temporal bone, and extra-articular and intra-articular fractures. There was also no significant association with the presence of coexisting mandibular fractures. However, intra-articular fractures were significantly associated with the presence of temporal bone fracture (odds ratio [OR] 3.2, 95% confidence interval [CI] 1.35–7.54; P = 0.008).
Cause of injury
A considerable number of the fractures were of unknown cause (n = 25 [31.6%]). When cause was determined, RTA was the most frequent (n = 26 [32.9%]), followed by animal interaction (n = 13 [16.5%]), external sharp or blunt force (n = 8 [10.1%]) and high-rise trauma (n = 7 [8.9%]) (see Table 2 in the supplementary material).
No significant associations were found between the cause of injury (RTA, high-rise trauma, animal interaction or other external force) and its pattern (luxation, subluxation, the presence of temporal bone fracture, intra-articular fracture, extra-articular fracture and coexisting mandibular fractures). However, bilateral injury was significantly associated with high-rise trauma (OR 13.13, 95% CI 1.85–92.96; P = 0.01) (Table 1).
Odds ratio of bilateral injury according to cause

OR calculated using the unknown cause as reference
P values in bold are statistically significant
OR = odds ratio; CI = confidence interval; RTA = road traffic accident
Distribution of the causes of TMJ injuries are illustrated in Figure 5. Mandibular condyle fractures were the most frequent TMJ injury for all causes. Mandibular condyle fractures of the medial half were the most frequently registered lesion secondary to all causes, especially high-rise trauma. Temporal bone fractures and coexisting mandibular injuries were observed in all causes except in high-rise trauma. In RTA cases, the most frequently seen lesion was temporal bone fracture. Of all temporal bone fractures where cause was established (21 in total), 69.6% were due to RTAs; this association was significant (P = 0.016).
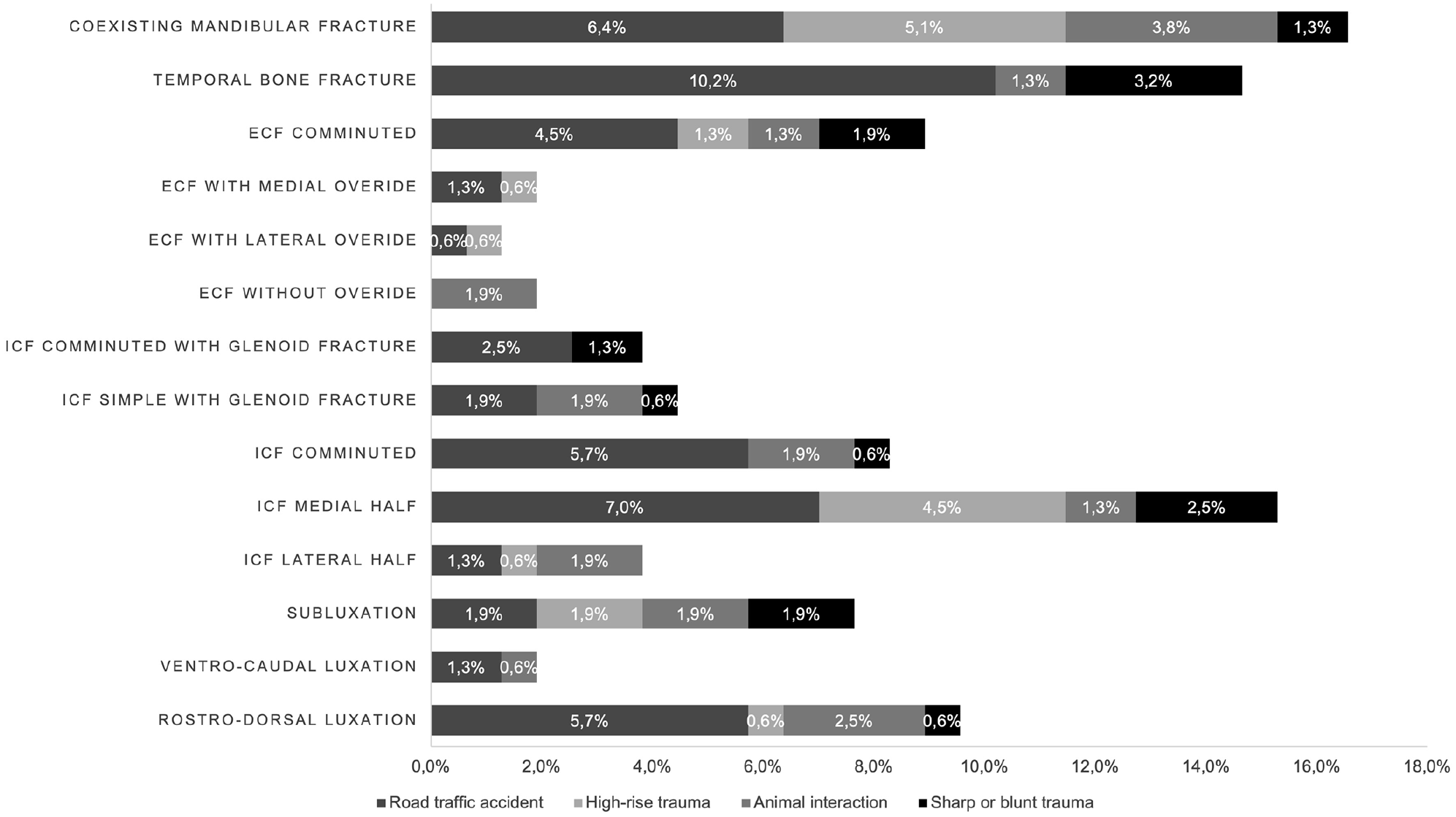
Distribution of injuries according to cause in 108 temporomandibular joints with 157 injuries (injuries of unknown causes were excluded from the distribution). ECF = extra-articular condylar fractures; ICF = intra-articular condylar fractures
Discussion
This study is the first to report and characterise TMJ injury patterns with regard to cause, using CT. Prior to this, these injuries had only been reviewed using plain film radiography. 1 CT allowed a more detailed evaluation of the different injury configurations that were missed or underestimated in previous studies. CT is considered superior to plain radiography for evaluation of the TMJ as it allows a three-dimensional assessment of lesions, overcoming the superimposition of anatomical structures.5,9,10 The cases were collected by six separate institutions, all of which are referral practices. The prevalence of the injuries reported here cannot reflect the true prevalence of these injuries in first opinion practices, albeit traumatic maxillofacial injuries are common in cats. 1
RTA was the most frequently reported cause of TMJ injury, followed by animal interaction, external force and high-rise trauma. While RTA was the most frequently reported cause of maxillofacial trauma in an English study, 3 a study from Turkey reported high-rise trauma as the most common cause. 1 These differences are likely to be the result of regional differences in the home environment and lifestyle. For example, urban areas with multilevel buildings can increase the risk of high-rise trauma. In our case series all the high-rise trauma cases were reported from the same institution, located within an urban area, which supports this speculation (see Table 2 in the supplementary material).
Trends were observed between the cause of trauma and injury pattern. In RTA cases, most of the defined types of TMJ injuries were observed. The same was true for blunt trauma and animal interaction. The variability of TMJ injuries is likely to be the result of the direction of force, velocity and severity of the impact. Conversely, we reported less variability in TMJ injuries in high-rise trauma, which were significantly more likely to be bilateral. In these cases, intra-articular fractures (comminuted or of the medial half) and extra-articular fractures (comminuted or with lateral override) were mostly observed. This lower injury variability is most likely due to the specificity in force direction, which is always in the rostrocaudal direction. In one previous study, the author also observed fewer TMJ injuries per cat in high-rise trauma, compared with RTA. 1 Interestingly, the same author reports a significantly higher number of isolated and bilateral TMJ injuries, namely caudal luxation or condylar process fractures, in high-rise trauma. 1 In our study, ventrocaudal luxations were not observed in high-rise trauma. On the contrary, all cases of luxation were rostrodorsal and in a lower proportion compared with other causes. Luxations were more frequently observed in RTAs and animal interactions.
The classification adopted was able to accommodate all TMJ injury patterns encountered in this case series. Differences between fractures of the mandibular head and condyle can be difficult to distinguish in cats because the condyle neck is very short. Therefore, TMJ injury classification was adapted from the Arbeitsgemeinschaft für Osteosynthesefragen – Craniomaxillofacial (AOCMF), 8 considering the recommendations by Arzi and Lantz using intra- and extra-articular fractures instead of intra- and extracapsular. 7 Additionally, the term ‘luxation’ rather than ‘dislocation’ was used.
Intra-articular fractures occurred more frequently than extra-articular fractures. The medial half the mandibular condyle was the most frequent intra-articular fracture. Comminuted fractures were more often extra-articular. These observations suggest that the medial half of the mandibular condyle and the neck, albeit very short, are less resistant to load. The mandibular condyle has thinner cross-sectional areas at the level of the neck and, consequently, can be less resistant to direct or indirect force. As the TMJ functions as a shock absorber that dissipates transmitted forces, 11 it seems logical that this area might be a weak anatomical point. The observation of this fracture type as an isolated injury in 11 cases also supports this theory.
Temporal bone fractures were the least frequent TMJ injury (18.3% of 158 TMJs). The squamous portion of the temporal bone appears to have higher resistance to fracture. The force vector and direction of the trauma are also relevant in the occurrence of fracture or luxation. Temporal bone fracture was significantly associated with RTAs, being the most frequently seen injury, compared with the complete absence of this kind of injury in high-rise trauma. These observations suggest that the squamous portion of the temporal bone seems to be more resistant to a perpendicular vector, which occurs in high-rise trauma, and less resistant to more oblique vectors of force in RTAs. The impact of the perpendicular/frontal vectors of force seen in high-rise trauma is felt simultaneously in the two temporal bones, potentiating the resistance to fracture, and the predisposition to bilateral injuries, which are also observed in these cases. In comparison, the force vectors in RTAs are more variable and more oblique in direction.
In approximately one-third of the cases evaluated in this study, TMJ luxation or subluxation was observed. Of these, the great majority were rostrodorsal luxations, similar to a previous study. 1 Furthermore, all caudoventral luxations were unilateral and bilateral luxations were all rostrodorsal. This fact reinforces rostral luxation as the most likely to occur and this may be explained by the joint angle and congruence, as well as the mandibular fossa, offering resistance to the caudal dislocation of the mandibular condyle.
Limitations of this study were a direct consequence of the number of cases and the intrinsic variability associated with the multi-institutional concept and retrospective data analysis. Variations of CT algorithms (slice and pitch) between institutions were also a factor and in three cases led to small anatomical gaps that could have inhibited a proper assessment. More standardised CT algorithms would have negated this limitation.
Conclusions
Unilateral TMJ injury patterns, especially intra-articular fractures of the medial half of the mandibular condyle, occur most frequently in cats following trauma. In cases of high-rise trauma these injuries tend to be bilateral.
Further studies using a larger number of cases should be performed in order to better understand TMJ patterns of injury.
Supplemental Material
sj-docx-1-jfm-10.1177_1098612X211066654 – Supplemental material for CT characterisation and classification of feline temporomandibular joint trauma: a case series of 79 cats
Supplemental material, sj-docx-1-jfm-10.1177_1098612X211066654 for CT characterisation and classification of feline temporomandibular joint trauma: a case series of 79 cats by Lisa A Mestrinho, Sónia SF Sebastião, Maciej A Zwierucho, Aaron Lutchman, Lorrie Gaschen, Stephanie Goldschmidt, Graham Thatcher, Yu Izumisawa and Richard L Meeson in Journal of Feline Medicine and Surgery
Supplemental Material
sj-docx-2-jfm-10.1177_1098612X211066654 – Supplemental material for CT characterisation and classification of feline temporomandibular joint trauma: a case series of 79 cats
Supplemental material, sj-docx-2-jfm-10.1177_1098612X211066654 for CT characterisation and classification of feline temporomandibular joint trauma: a case series of 79 cats by Lisa A Mestrinho, Sónia SF Sebastião, Maciej A Zwierucho, Aaron Lutchman, Lorrie Gaschen, Stephanie Goldschmidt, Graham Thatcher, Yu Izumisawa and Richard L Meeson in Journal of Feline Medicine and Surgery
Footnotes
Acknowledgements
The authors thank Santiago Peralta and Nadine Fiani for their contribution to this study. This manuscritpt is dedicated to Maciej Zwierucho, an exceptional young man, who sadly passed away during this research.
Supplementary material
The following files are available online: Table 1: Distribution of injuries according to cause in 158 temporomandibular joints. Table 2: Distribution of causes and injury extent per institution.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Part of this work was supported by FCT - Fundação para a Ciência e Tecnologia IP, grant UIDB/00276/2020 (LM).
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.