
Abstract
Objectives
Radioactive iodine (131I) is the preferred treatment for feline hyperthyroidism but neither the optimal 131I dose nor consistent predictors of post-treatment azotaemia have been determined. The aims of the study were to evaluate the relationships between: (1) 131I dose and survival; and (2) pretreatment and post-treatment serum creatinine concentration.
Methods
Medical records of hyperthyroid cats treated with 131I at a single referral hospital were reviewed. Information regarding signalment, body weight, pretreatment and post-treatment serum total thyroxine concentration (TT4), serum creatinine concentration, 131I dose and survival were determined. Multivariable Cox proportional hazards analysis was used to identify variables associated with survival. Multivariable linear regression analysis was used to identify variables associated with post-treatment serum creatinine concentration.
Results
One hundred and ninety-eight (79 male, 119 female) cats were treated for hyperthyroidism with 131I (median dose 138 MBq; interquartile range 92–168). Median survival time was 1153 days (range 16–1871). Post-treatment serum creatinine (P <0.001) and age (P = 0.049) were significantly associated with survival. Every 10 µmol/l increase in post-treatment serum creatinine concentration and every year increase in age was associated with a 1.07-fold (confidence interval [CI] 1.04–1.11) and 1.17-fold (CI 1.00–1.37) increase in the daily hazard of death, respectively. Pretreatment serum creatinine concentration was directly, and post-treatment serum TT4 concentration was inversely, associated with post-treatment serum creatinine concentration. Every 1 μmol/l increase in pretreatment serum creatinine concentration was associated with an increase in post-treatment serum creatinine concentration of 0.7 μmol/l (SE 0.17; P <0.001). Conversely, every 1 nmol/l decrease in post-treatment serum TT4 concentration was associated with a 1.2 μmol/l (SE 0.61; P <0.001) increase in post-treatment serum creatinine concentration.
Conclusions and relevance
Post-treatment serum TT4 concentration was associated with post-treatment azotaemia, which was associated with survival. Although 131I dose was not directly associated with survival, dosing strategies that minimise post-treatment hypothyroidism and azotaemia could improve patient survival.
Introduction
Hyperthyroidism is the most common endocrine disorder in cats and radioactive iodine (131I) is considered the gold standard treatment.1,2 Regardless of dose or route of administration, a single treatment of 131I is effective in >90% of cats.2–8 Survival times for cats with hyperthyroidism treated with 131I range from 2 to 5 years.2,3,5,8–10 Cats treated with 131I have a longer median survival time than cats treated with medical management, even when post-treatment methimazole is required. 9
There are several pre- and post-treatment factors associated with survival of cats with hyperthyroidism. Pretreatment factors, including increased age, low body weight, sex (male cats), abnormal urine protein:creatinine (UPC) ratio, hypertension (systolic blood pressure >170 mmHg), pre-existing azotaemia and increased plasma fibroblast growth factor-23 are adversely associated with survival.3,5,8–12 Pre-existing azotaemia reduces overall survival, regardless of treatment options (131I or methimazole alone). 9 In contrast, the development of azotaemia after hyperthyroid treatment did not adversely impact on survival in euthyroid cats in one study. 10 However, iatrogenic hypothyroidism was associated with an increased incidence of azotaemia,11–13 and the combination of post-treatment azotaemia and iatrogenic hypothyroidism does adversely affect survival times. 11
There is no universal dosing scheme for 131I. Doses can vary based on tracer studies or use of a scoring system, which is determined by the severity of clinical signs, subjective size of the abnormal thyroid glands and serum total thyroxine (TT4) concentration. Alternatively, a predetermined fixed dose can be administered.2,6 A common approach is the administration of a fixed standard dose of 131I (148–185 MBq), regardless of the degree of hyperthyroidism or the size of the thyroid gland.6,14 Given the association of iatrogenic hypothyroidism with post-treatment azotaemia and subsequent adverse effect on survival, low 131I dose (70–111 MBq) protocols have been proposed for treatment of mild-to-moderate hyperthyroidism.15–17 Cats treated with a low dose of 131I had a reduced incidence of iatrogenic hypothyroidism and azotaemia. 4 While it is hypothesised that lower 131I doses will result in greater overall survival, the relationship between 131I dosing and overall survival has yet to be evaluated.
Based on studies to date, it is difficult to predict which cats will develop post-treatment azotaemia. In earlier studies, pretreatment serum creatinine concentration was not a reliable predictor of post-treatment azotaemia in hyperthyroid cats.18–20 Measurement of pretreatment glomerular filtration rate (GFR) did not consistently predict the development of post-treatment renal failure.19,21 Conversely, pretreatment serum creatinine was independently associated with post-treatment azotaemia in larger cohorts of hyperthyroid cats treated with 131I or medical therapy.10,12
The aim of this study was to evaluate the relationship between 131I dose and survival. Given the association of iatrogenic hypothyroidism with post-treatment azotaemia and reduced survival, it was hypothesised that 131I dose would be associated with survival. A secondary aim was to re-evaluate the relationship between pretreatment serum creatinine and post-treatment serum creatinine concentration in cats treated with oral 131I.
Materials and methods
The medical records of hyperthyroid cats treated with 131I at the Small Animal Specialist Hospital, NSW, Australia between July 2015 and March 2020 were reviewed. A diagnosis of hyperthyroidism was based on appropriate clinical signs (eg, weight loss, polyphagia, polydipsia and polyuria) and a serum TT4 concentration above the reference interval (RI). Serum TT4 concentration was measured at commercial reference laboratories (IDEXX Laboratories and Vetnostics, Australia). Pretreatment data obtained from the medical records included age, sex, breed, body weight, serum TT4 concentration, serum creatinine concentration, packed cell volume, date of treatment and 131I dosage. Thioureylene medications and iodine-restricted diets were discontinued 2 weeks prior to treatment. The dose of 131I was determined for each hyperthyroid cat by a single internal medicine specialist based on a modified variable dosing system that included severity of clinical signs, serum TT4 and palpable thyroid gland size, as previously described.3,22 Cats with mild disease received a low 131I dose (74–130 MBq), cats with moderate disease received a mid-range 131I dose (130–168 MBq) and cats with severe disease received a high 131I dose (180–210 MBq). After 131I was administered orally, the cats were kept in individual cages in a designated radiation isolation ward and were discharged after 5–7 days. Post-treatment evaluation comprising a physical examination, serum TT4 and serum creatinine concentration was performed between 6 and 12 weeks after treatment at referring veterinary clinics. Post-treatment data were obtained by means of telephone conversations or questions emailed to referring veterinarians.
Statistical analysis
Descriptive statistics were determined for pretreatment and post-treatment clinicopathological parameters. Where a pretreatment serum TT4 was reported as >150 nmol/l but a definitive result was not available, this individual value was excluded. Low post-treatment serum TT4 was defined as a serum TT4 concentration <10 nmol/l as thyroid-stimulating hormone (TSH) was inconsistently available.
Survival time was calculated from the day of 131I treatment to the date of death or euthanasia. If these data were not available in the medical record, the owner or the referring veterinarian was contacted by telephone. If the cat had died but the exact date of death was unknown, the month of death was recorded and it was assumed that the cat died on the first of that month for the purposes of survival analysis. Cats were censored if they were still alive at the end of the follow-up period (July 2020) or at the last known consultation date.
A Kaplan–Meier survival curve was created and median survival time determined for all cats.23,24 A multivariable Cox’s proportional hazard model was used to evaluate the relationship between 131I dose and survival, accounting for the potential confounding variables of age, sex, breed (domestic or pedigree), pretreatment and post-treatment serum creatinine, and serum TT4 concentration. Explanatory variables associated with survival with an initial P value of <0.2 in bivariable analysis were selected for inclusion in the multivariable model. A backwards step-wise approach was used. Explanatory variables that were not statistically significant were removed from the model one at a time, beginning with the least significant, until the estimated regression coefficients of the variables retained were significant (P <0.05). The results of the final model are reported in terms of adjusted hazard ratios for each significant explanatory variable. The assumption of a linear relationship between serum creatinine and the logarithm of hazard was tested and confirmed using the Martingale residuals from the final Cox model. The assumption of proportional hazards was assessed by plotting the Schoenfeld residuals as a function of time.
Multivariable linear regression analysis was performed to evaluate the potential relationship between pretreatment serum creatinine concentration and post-treatment serum creatinine concentration while accounting for the potential confounding factors of age, sex, breed, pretreatment and post-treatment serum TT4. Cats with persistent hyperthyroidism (serum TT4 above the RI) after treatment were excluded from this analysis. Potential explanatory variables with an initial P value of <0.2 were entered into a multivariable logistic regression model. To select variables most associated with post-treatment serum creatinine concentration, a backward stepwise approach was used. Explanatory variables that were not statistically significant were removed from the model one at a time, beginning with the least significant, until the estimated regression coefficients of the variables retained were significant (P <0.05). Model assumptions were reviewed. 25 Correlations between significant linear predictors and post-treatment serum creatinine concentration were determined using Spearman’s correlation coefficient.
Results
One hundred and ninety-eight cats (119 females and 79 males) were treated with 131I between June 2016 and March 2020 (Table 1).
Descriptive statistics of 198 cats treated with 131I

n = 194
n = 129
n = 170
n = 135
n = 165
IQR = interquartile range; TT4 = total thyroxine; PCV = packed cell volume
Pretreatment data
The median age of the study population was 13.1 (interquartile range [IQR] 11.1–14.7) years. Pretreatment serum creatinine in 195 cats ranged from 30 to 230 μmol/l (median 90; IQR 70–115). Pretreatment serum TT4 in 170 cats ranged from 54 to 477 nmol/l (median 105; IQR 82–150). Cats were treated with 131I doses between 77 and 210 MBq (median 138; IQR 92–168). Based on the modified scoring system, 89/198 (45%) cats received a low 131I dose, 78/198 (39%) received a moderate 131I dose and 31/198 (16%) cats received a high 131I dose.
Post-treatment data
Post-treatment serum TT4 was available in 135 cats. The median post-treatment serum TT4 was 23 nmol/l (IQR 19–29). Five cats had persistent hyperthyroidism. Five cats were identified as hypothyroid based on a serum TT4 of <10 nmol/l (3.7%). Post-treatment serum creatinine level was available for 129 cats. The median post-treatment serum creatinine was 145 µmol/l (IQR 120–195). Sixty cats (46.5%) had serum creatinine concentrations <140 µmol/l, while 69 cats (53.5%) had a serum creatinine concentration >140 µmol/l after treatment. Two cats developed severe azotaemia within 3 months of 131I treatment. The first cat developed ureteral obstruction and pyelonephritis 1 month after 131I treatment (serum creatinine 760 µmol/l). The second cat developed acute kidney injury of unknown aetiology 2 months after 131I treatment (serum creatinine 480 µmol/l).
Survival analysis
One hundred and thirty-two cats were alive, eight cats were lost to follow-up and censored at discharge, and 58 cats died with a median survival time of 1153 days (Figure 1). 131I dose (P = 0.95) was not significantly associated with survival when assessed independently in bivariate regression analysis (see Table S1 in the supplementary material). In the final Cox regression model, every year increase in age was associated with a 1.17-fold (95% confidence interval [CI] 1.00–1.37) increase in the daily hazard of death (P = 0.0496) and every 10 µmol/l increase in post-treatment serum creatinine was associated with a 1.07-fold (95% CI 1.04–1.11) increase in the daily hazard of death (P <0.001) (Table 2).

Kaplan–Meier curve of survival times for 198 hyperthyroid cats treated with 131I
Multivariable Cox regression analysis of factors affecting survival of cats treated with 131I (n = 198)
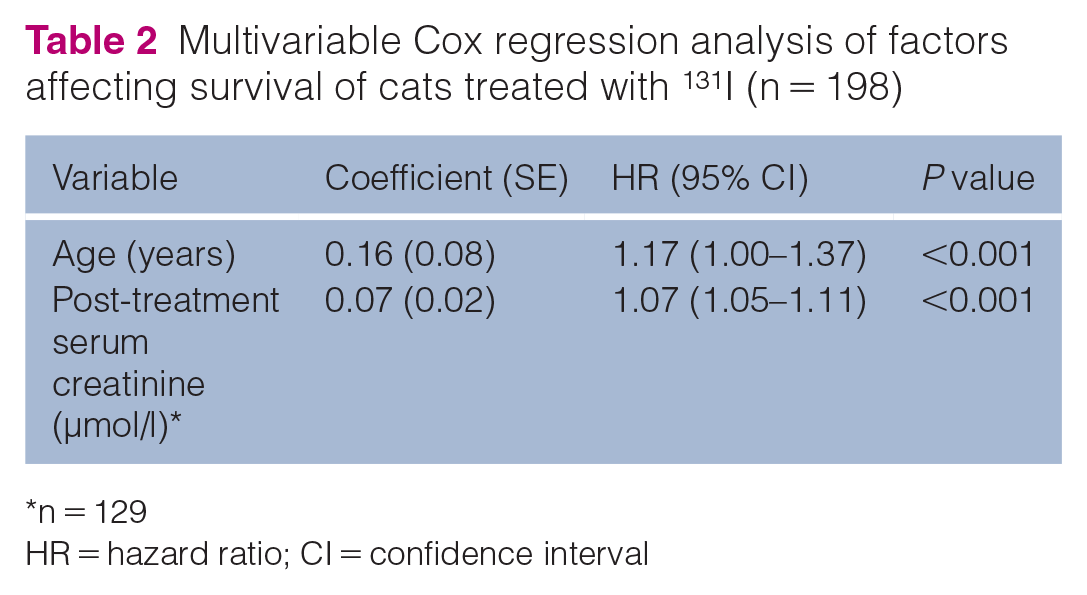
n = 129
HR = hazard ratio; CI = confidence interval
Predictors of azotaemia
Five cats with persistent hyperthyroidism were excluded from this analysis. Three outliers were removed to ensure the final model fulfilled the assumptions of linear regression models. Bivariate analysis of the potential predictors of post-treatment azotaemia is displayed in Table S2 in the supplementary material. Pretreatment serum creatinine concentration and post-treatment serum TT4 were significantly associated with post-treatment creatinine concentration (Table 3). Every 1 μmol/l increase in pretreatment serum creatinine was associated with an increase in post-treatment serum creatinine of 0.7 μmol/l (SE 0.17; P <0.001). Every 1 nmol/l decrease in post-treatment serum TT4 was associated with a 1.2 μmol/l (SE 0.61; P <0.001) increase in post-treatment serum creatinine concentration.
Multivariable linear regression analysis of variables associated with post-treatment azotaemia
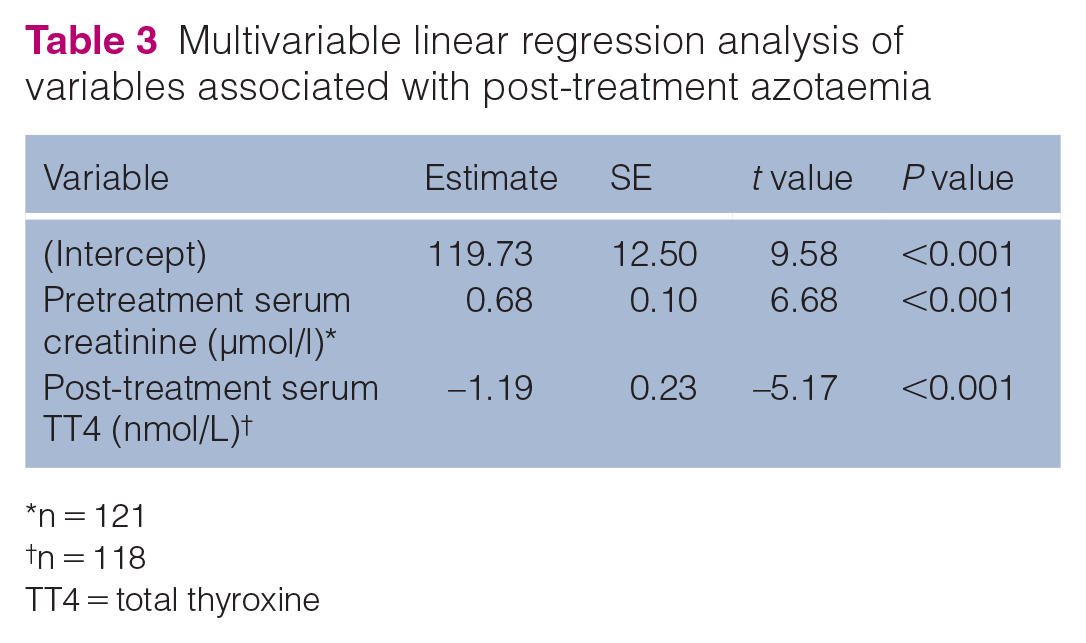
n = 121
n = 118
TT4 = total thyroxine
Pretreatment serum creatinine concentration had a moderate positive correlation with post-treatment serum creatinine concentration (r = 0.54; P = 0.0496) (Figure 2). Post-treatment serum TT4 concentration has a moderate negative correlation with post-treatment serum creatinine concentration (r = −0.41; P <0.001) (Figure 3).
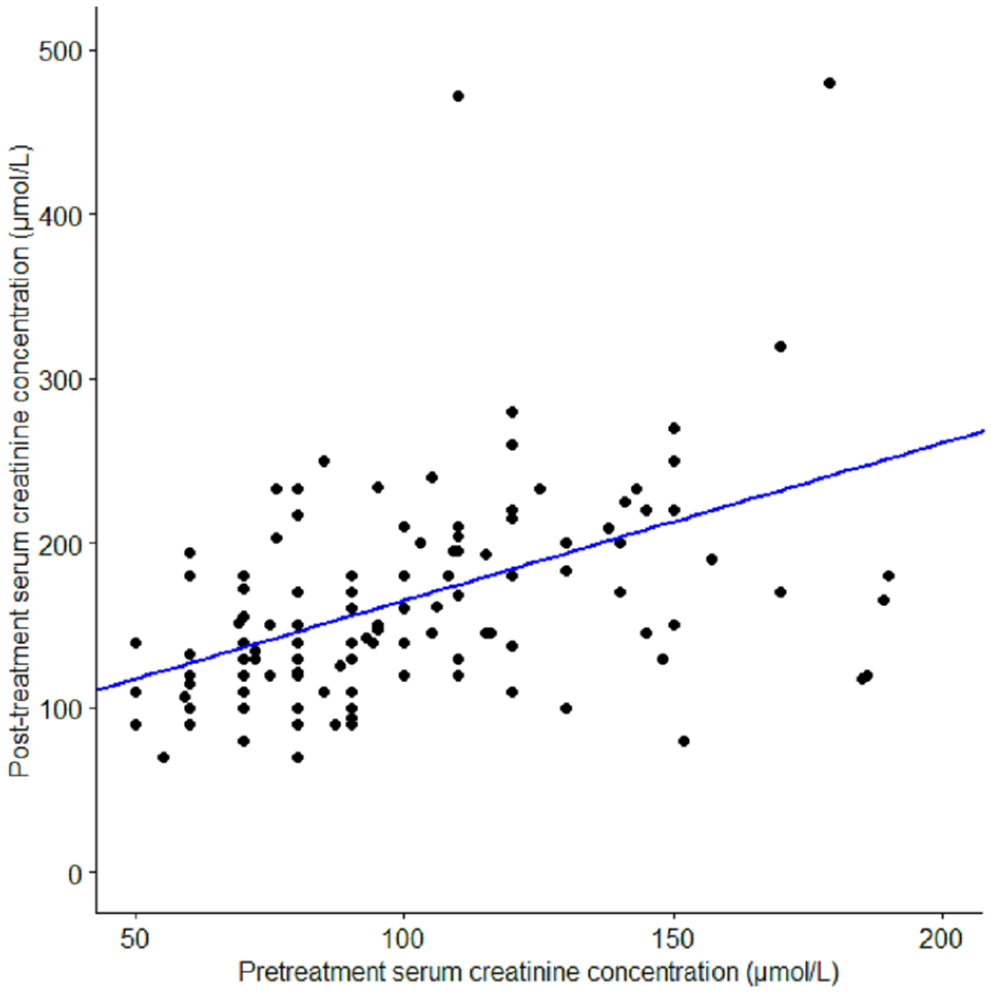
Correlation (Spearman’s correlation coefficient) between pretreatment serum creatinine concentration and post-treatment serum creatinine concentration in 124 hyperthyroid cats treated with 131I (r = 0.54, P <0.001)

Correlation (Spearman’s correlation coefficient) between post-treatment total thyroxine (T4) concentration vs post-treatment serum creatinine concentration in 121 cats with hyperthyroidism treated with 131I (r = −0.41, P <0.001)
Discussion
Age and post-treatment serum creatinine concentration adversely affects the survival of hyperthyroid cats treated with 131I. Pre-existing azotaemia influences survival in hyperthyroid cats; 9 however, our results contrast with a previous study where cats which developed azotaemia after treatment had a similar survival time to non-azotemic cats as long as hypothyroidism is avoided. 26 The differences may be due to differences in methodology (evaluation of serum creatinine as a continuous variable rather than use of an absolute criteria [serum creatinine >177 μmol/l]) for azotaemia, treatment methods (radioiodine, medical management and surgery) or incidence of post-treatment hypothyroidism. 26
Pretreatment serum creatinine concentration was significantly associated with post-treatment serum creatinine concentration and there was modest direct correlation between the two variables. Hyperthyroidism results in an increased GFR, potentially masking underlying chronic kidney disease.19,21 In earlier studies, neither pretreatment serum creatinine concentration, serum TT4, urea or urine specific gravity (USG) were reliable predictors of post-treatment azotaemia in hyperthyroid cats.18–20 These studies only included a small number of cats (n <40) treated with 131I.18–20 In contrast, pretreatment serum creatinine was independently associated with post-treatment azotaemia in a larger cohort of hyperthyroid cats treated with 131I. 12 Using a cut-off for serum creatinine concentration of 1.3 mg/dl (114.9 µmol/l), the reported sensitivity and specificity for pretreatment serum creatinine concentration to predictpost-treatment azotaemia (serum creatinine >2.1 mg/dl; serum creatinine >186.7 µmol/l) was 79% and 84%, respectively. 12 Serum symmetric dimethylarginine was found to be a highly specific but poorly sensitive marker for predicting post-treatment azotaemia, whereas USG was highly sensitive but poorly specific. 12 Based on this study, pretreatment serum creatinine concentration can be used as a guide to the likelihood of post-treatment azotaemia.
Post-treatment serum TT4 concentration was inversely correlated with post-treatment serum creatinine concentration, likely due to normalisation of GFR after resolution of hyperthyroidism or the development of iatrogenic hypothyroidism. The number of cats with low post-treatment serum TT4 in this study was small, but the clinical significance of subclinical hypothyroidism (low normal or normal serum TT4 with high TSH) is unknown in cats and was not fully evaluated in this study. However, the association of post-treatment serum TT4 concentration with serum creatinine concentration suggests the potential significance of low normal serum TT4 concentration in cats after treatment for hyperthyroidism warrants further evaluation.
Post-treatment serum creatinine concentration was adversely associated with survival and post-treatment serum TT4 was adversely associated with post-treatment serum creatinine concentration. Consequently, the relationship between 131I dose and survival appears an indirect one, potentially mediated by hypothyroidism and its effects on renal function. Iatrogenic hypothyroidism is a well-known complication of 131I treatment. The incidence of iatrogenic hypothyroidism may be influenced by the 131I dose administered, the length of the follow-up and the diagnostic criteria for hypothyroidism. The reported incidence of iatrogenic hypothyroidism varies greatly (<25% to 79%).3,7,10,12,15,16,19,22,27 A recent study demonstrated that a low dose 131I (2 millicurie, 74 MBq) was as effective as a higher dose 131I (4 millicurie, 148 MBq) in treating mild-to-moderate hyperthyroidism (serum TT4 <167 nmol/l) with a success rate of >95%, a reduced frequency of iatrogenic hypothyroidism (both overt and subclinical) and lower serum creatinine concentration in the low-dose group. 15 One study suggested that an 131I dose of 2 millicurie (74 MBq) would be sufficient to treat most cats with hyperthyroidism. 17 Minimising iatrogenic hypothyroidism and subsequent post-treatment azotaemia by improving 131I dosing protocols could potentially improve the survival of cats treated for hyperthyroidism.
131I treatment is highly effective in restoring euthyroidism in cats diagnosed with hyperthyroidism. The success rate (>90%) and median survival time in this study is comparable to the current literature,3,8,9,26,28 and the result supports the contention that oral 131I is as effective as parenteral 131I administration.2,4,7 The main disadvantages of oral 131I administration are increased risk of exposure to radiation by the personnel handling the cats and the risk of vomiting after administration, which may lead to environmental contamination and treatment failure.
The present study has a number of limitations. First, other factors known to affect survival, such as blood pressure and UPC ratio, were not evaluated. Secondly, the dose of 131I was determined based on the severity of hyperthyroidism, which might have resulted in a potential bias. Cats with more severe disease or higher pretreatment serum TT4 concentration would have received a higher dose of 131I based on the variable dosing system that we used in our practice. Our bivariate analysis showed that neither 131I dose nor pretreatment serum TT4 were independently associated with survival. Among this cohort, cats with more severe disease did not appear to have an increased risk of death. This observation is consistent with previous literature where serum TT4, a marker of disease severity, was not associated with survival.9,10 It is possible that serum TT4 is an inadequate marker of disease severity and other variables, potentially chronicity, muscle condition score or cardiovascular complications, would be more appropriate variables to assess in future studies. A limitation of this study is that we have not evaluated other variables such as goitre size and chronicity of disease, which could also influence the severity of hyperthyroidism and 131I dose. Serum creatinine concentrations can be influenced by hydration status and muscle condition. In addition, the post-treatment serum creatinine concentrations were determined in samples collected at referring veterinary clinics using different biochemistry analysers, which could have resulted in considerable variation. 29 The lack of post-treatment TSH measurement is another limitation of this study as we were unable to differentiate iatrogenic hypothyroid cats from those with non-thyroidal illness.
Conclusions
131I dose is not directly associated with survival, but post-treatment serum TT4 correlates with post-treatment serum creatinine concentration, which is associated with survival. Pretreatment serum creatinine concentration has value in predicting post-treatment azotaemia. 131I dosing strategies that minimise post-treatment hypothyroidism and azotaemia could improve patient survival.
Supplemental Material
Table S1
Bivariate Cox regression analysis of factors affecting survival of cats treated with 131I (n = 198)
Supplemental Material
Table S2
Bivariate linear regression analysis of variables associated with post-treatment azotaemia (n = 129)
Footnotes
Supplementary material
The following files are available online:
Table S1: Bivariate Cox regression analysis of factors affecting survival of cats treated with 131I (n = 198).
Table S2: Bivariate linear regression analysis of variables associated with post-treatment azotaemia (n = 129).
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (owned or unowned) and followed internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. For any animals or humans individually identifiable within this publication, informed consent for their use in the publication (verbal or written) was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.