
Abstract
Objectives
Radioiodine (RAI) treatment for hyperthyroidism is becoming increasingly available in the UK. Pretreatment assessment is commonly performed, as patient handling is limited once RAI has been administered. The aims of this study were to determine the prevalence of thoracic pathology using thoracic radiography in hyperthyroid cats referred for RAI treatment and to determine the value of this technique pretreatment.
Methods
The hospital databases were searched for hyperthyroid cats referred for RAI treatment at the Feline Centre, Langford Vets, between January 2012 and July 2016. Radiographs were reviewed by Diplomates of the European College of Veterinary Diagnostic Imaging at the time of treatment and each set of radiographs was subsequently reviewed by one radiologist for the study. Cardiorespiratory signs were recorded, if present, and any change in treatment plan or suitability for RAI treatment was documented.
Results
Two hundred and fifty-two cats were included in the study. Thoracic pathology was identified in 77% (n = 194/252) of the cats, of which 59% (n = 115/194) had pulmonary abnormalities with bronchial and bronchointerstitial patterns most frequently; 57% (n = 111/194) had skeletal abnormalities and 43% (n = 84/194) had cardiac abnormalities, with mild-to-moderate cardiomegaly most prevalent. Other abnormalities included sternal lymphadenomegaly (7%; n = 13/194), mediastinal pathology (3%; n = 5/194), oesophageal pathology (2%; n = 4/194) and pleural space disease (0.5%; n = 1/194).Twelve cases (6%) had a change in their treatment plan as a result of thoracic radiographic abnormalities, of which five subsequently underwent RAI treatment.
Conclusions and relevance
A low prevalence of significant thoracic pathology was identified on radiographs in hyperthyroid cats referred for RAI treatment. Incidental thoracic abnormalities were found much more commonly; hence, results of thoracic radiology need to be combined with the clinical picture, to decide whether further investigations or alterations to the treatment plan are required pre-RAI.
Introduction
Hyperthyroidism is the most common endocrine disease in the cat population, 1 and is often seen in middle-aged and older cats.2–6 The treatment options include antithyroid drugs, thyroidectomy, dietary iodine restriction and radioiodine (RAI) treatment. The last is considered to be the gold standard treatment and is increasingly available in UK centres.4,6 Many centres routinely perform a pretreatment assessment in order to identify concurrent diseases that might affect the patient’s treatment options, long-term prognosis and suitability for RAI treatment. Previous studies have shown that comorbidities are frequently found in older cats and that subclinical concurrent diseases are very common in hyperthyroid cats referred for RAI treatment.7–9 The ability to identify any significant concurrent diseases is of importance, as patient handling is limited once RAI treatment has been administered and progression of concurrent diseases during that time is possible. Additionally, RAI treatment is more expensive as a one-off cost and may not be the ideal treatment choice if other diseases are life-limiting. At the Feline Centre, the current isolation period is 7–10 days post-RAI injection, dependent upon dose. The average UK hospital isolation times range between 7 and 14 days with handling restrictions typically extending for a further 2–3 weeks at home; significantly shorter isolation periods apply in some other countries (eg, the USA and Australia). 10
The pretreatment assessment varies between centres and not all routinely include thoracic radiology. Previous studies have evaluated the prevalence of concurrent abdominal diseases in hyperthyroid cats referred for RAI treatment and the usefulness of abdominal ultrasound examination as part of the pretreatment evaluation.8,9,11 However, there is limited published information about concurrent thoracic disease in hyperthyroid cats referred for RAI treatment. Cats are particularly good at hiding clinical signs of a cardiorespiratory disease until late in the disease process; therefore, subclinical cardiorespiratory pathology might be present and only become apparent at the advanced stages of the disease. Thoracic radiography may identify occult thoracic pathology. Additionally, tachypnoea and dyspnoea may be caused by hyperthyroidism; however, there are no pathognomonic features to distinguish this from other causes. 12
The aims of this study were to determine the prevalence of thoracic pathology using thoracic radiography in hyperthyroid cats referred for RAI treatment and to evaluate the value of this technique pretreatment.
Materials and methods
The study population was obtained by searching the hospital databases for hyperthyroid cats referred for RAI treatment at the Feline Centre, Langford Vets, University of Bristol, between January 2012 and July 2016.
The inclusion criteria comprised hyperthyroid cats that had undergone RAI suitability assessment with thoracic radiographs, with the thoracic radiographs and medical records available for review. Diagnosis of hyperthyroidism was based on serum concentration of total thyroxine above the upper reference limit for the laboratory used and compatible clinical signs. Screening of case histories had been performed before accepting the referral to exclude obviously unsuitable cases; for example, insulin-dependent diabetic cats, cats with International Renal Interest Society stage 4 chronic kidney disease or thymoma. The RAI referral included an assessment visit to determine suitability of the patient for treatment, typically 4 weeks in advance of treatment, including serum biochemistry, haematology, urinalysis, systolic blood pressure measurement, echocardiography, thoracic radiography and abdominal ultrasound.
Thoracic radiographs were obtained under sedation with a minimum of two views, but usually three, including a left and right lateral and a dorsoventral view of the thorax. At the time of assessment, radiographs were initially reviewed by Diplomates of the European College of Veterinary Diagnostic Imaging (ECVDI). For the purposes of this study each set of radiographs was reviewed once again by a single ECVDI radiologist. Abnormalities on thoracic radiographs were classified by system (pulmonary, cardiac, pleural, mediastinal, skeletal, lymph node, oesophageal and skin).
For each case, age, sex, breed, presence of cardiorespiratory signs (eg, cough, tachypnoea, dyspnoea, stertor, stridor, adventitious pulmonary sounds, heart murmur), echocardiography results, record of definitive diagnosis for thoracic pathology, any change in treatment plan and suitability for RAI treatment, were documented. Change in treatment plan was defined either as further investigations for the radiographic abnormalities (eg, repeat radiographs after a set period of time, bronchoalveolar lavage, bronchoscopy, ultrasound examination, electrocardiography, CT, fine-needle aspirates of thoracic lesions, etc) prior to RAI administration or as treatment of the concurrent disease that had been identified with thoracic radiology. Cases were categorised as: (1) suitable for RAI with no treatment plan change; (2) suitable for RAI following treatment plan change owing to thoracic pathology ± other system pathology; (3) suitable for RAI following treatment plan change for other (non-thoracic) pathology; (4) unsuitable for RAI owing to thoracic pathology ± other system pathology; and (5) unsuitable for RAI owing to other (non-thoracic) pathology.
The exclusion criteria were lack of access to thoracic radiographs and/or medical records for review and cases with severe comorbidities, identified either during the physical examination or with other diagnostic tests, where thoracic imaging was not performed, owing to patient prognosis or instability for sedation. Data were recorded in Microsoft Excel and descriptive statistics performed. Data for thoracic pathology system abnormalities were summated and the percentage was calculated for each category.
Ethical approval
Ethical approval was granted by the Animal Welfare and Ethics Review Body at the University of Bristol (VIN/19/029).
Results
Two hundred and eighty-five cases were initially identified. Of these, 33 were excluded due to lack of thoracic radiographs. Of the 252 included, 109/252 (43%) were neutered males and 143/252 (57%) were neutered females. Cats had a median age of 12 years (range 6–18 years). Common breeds were domestic shorthair (n = 205) and domestic longhair (n = 31). Other breeds included Ragdoll (n = 4), British Shorthair (n = 4), Maine Coon (n = 3), British Longhair (n = 1), Abyssinian (n = 1), Cornish Rex (n = 1), Balinese (n = 1) and Norwegian Forest Cat (n = 1).
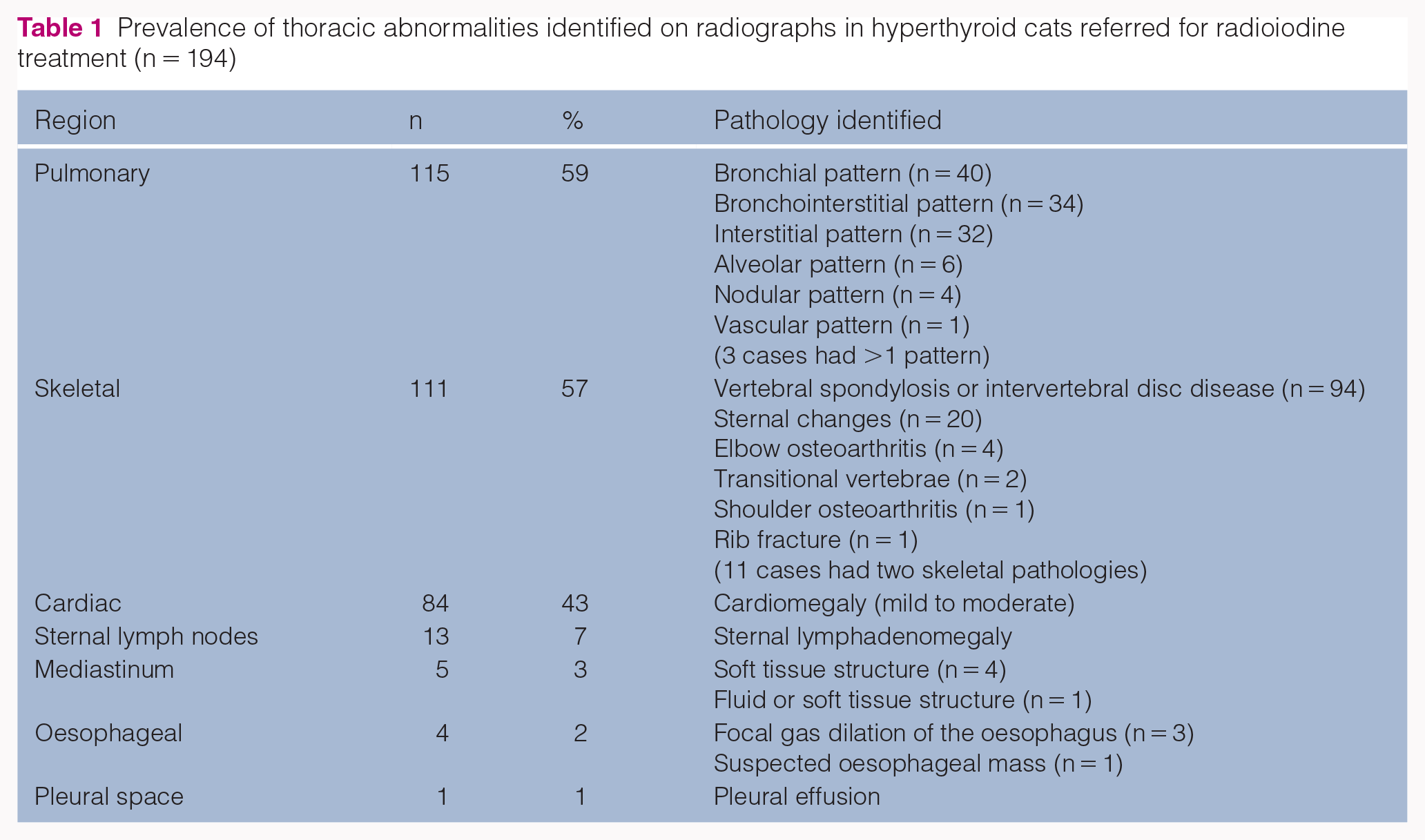
Concurrent thoracic pathology was identified radiographically in 77% (n = 194/252) of the cases, with pulmonary, cardiac and skeletal abnormalities being the most common findings (Table 1). In 59% (n = 115/194), pulmonary abnormalities were identified, with bronchial and bronchointerstitial patterns being the most frequent. In 57% (n = 111/194), skeletal abnormalities were noted, with intervertebral disc disease (IVDD) or spondylosis and sternal abnormalities being the most common findings. Cardiac abnormalities were found in 43% (n = 84/194) of the cases, with mild-to-moderate cardiomegaly being most prevalent (Figure 1). Other abnormalities included sternal lymphadenomegaly in 7% (n = 13/194), mediastinal pathology in 3% (n = 5/194) and oesophageal pathology in 2% (n = 4/194), where there were three cases with mild focal gas dilation of the cranial oesophagus and one possible oesophageal mass. Mediastinal abnormalities included the presence of a soft tissue structure in the mediastinum in 4/5 cases (2%, n = 4/194); the differential list in these cases included cyst, lymphoma, thymoma and ectopic thyroid tissue. In 1/5 cases (0.5%; n = 1/194) the mediastinal changes identified appeared to reflect fluid or soft tissue; differentials included were mediastinal fluid, lymphadenomegaly and mediastinitis. One cat (1%) had a small pleural effusion. In three cases skin lesions were identified; differential diagnosis included abscess, granuloma, neoplasia and haematoma. However, skin abnormalities were not included further, as they were considered to be extrathoracic.
Prevalence of thoracic abnormalities identified on radiographs in hyperthyroid cats referred for radioiodine treatment (n = 194)

(a) Dorsoventral, and (b) left and (c) right lateral views of the thorax of a hyperthyroid cat that was excluded from radioiodine treatment owing to cardiac disease. There is marked cardiomegaly, evidence of pulmonary venous congestion and possible early oedema. This cat had a grade II/VI systolic, left apical heart murmur and was tachypnoeic upon presentation, with a respiratory rate of 60–80 breaths per min
Overall, 234 cases were suitable for RAI with no change in treatment plan. Of the cases with thoracic radiographic abnormalities, 12 cases (6%; n = 12/194) had a change in their treatment plan in relation to thoracic pathology, of which five subsequently had RAI treatment (Table 2). The remaining seven cases (4%; 7/194) were considered to be unsuitable candidates for RAI; six were excluded due to thoracic pathology primarily (suspected or confirmed neoplasia [n = 3], case example shown in Figures 2 and 3, cardiac disease [n = 2], bronchitis and cardiac disease [n = 1]). The seventh case was diagnosed with neutrophilic bronchitis along with hepatocellular and pancreatic carcinoma; RAI treatment was excluded due to the abdominal pathology (non-thoracic pathology category). The reasons for not treating these patients included poor prognosis associated with the identified disease, concerns about possible progression of the concurrent disease during isolation, loss to follow-up and a change in the owner’s decision to treat. Four of these cases were euthanased.
Summary of hyperthyroid cases with abnormalities on thoracic radiography that had a change in their treatment plan in relation to thoracic pathology

RAI = radioiodine treatment; y = years; FN = female neutered; DSH = domestic shorthair; ECG = electrocardiography; TT4 = total thyroxine; RI = reference interval; CHF = congestive heart failure; MN = male neutered; IRIS = International Renal Interest Society; CKD = chronic kidney disease; DLH = domestic longhair; FNA = fine-needle aspiration; BAL = bronchoalveolar lavage; FeLV = feline leukaemia virus; Ag = antigen; FIV = feline immunodeficiency virus; Ab = antibody; BLH = British Longhair; bpm = beats per minute

(a) Dorsoventral and (b) right lateral views of a hyperthyroid cat with suspected pulmonary neoplasia. This cat was intermittently open-mouth breathing at home (hyperthyroidism was uncontrolled). On the lateral view, there is a well-defined soft tissue nodule in the caudal lung field, which is not apparent on the dorsoventral view. This nodule was further investigated with a CT scan, which showed a few more nodules that were not quite obvious on the radiographs (see Figure 3)
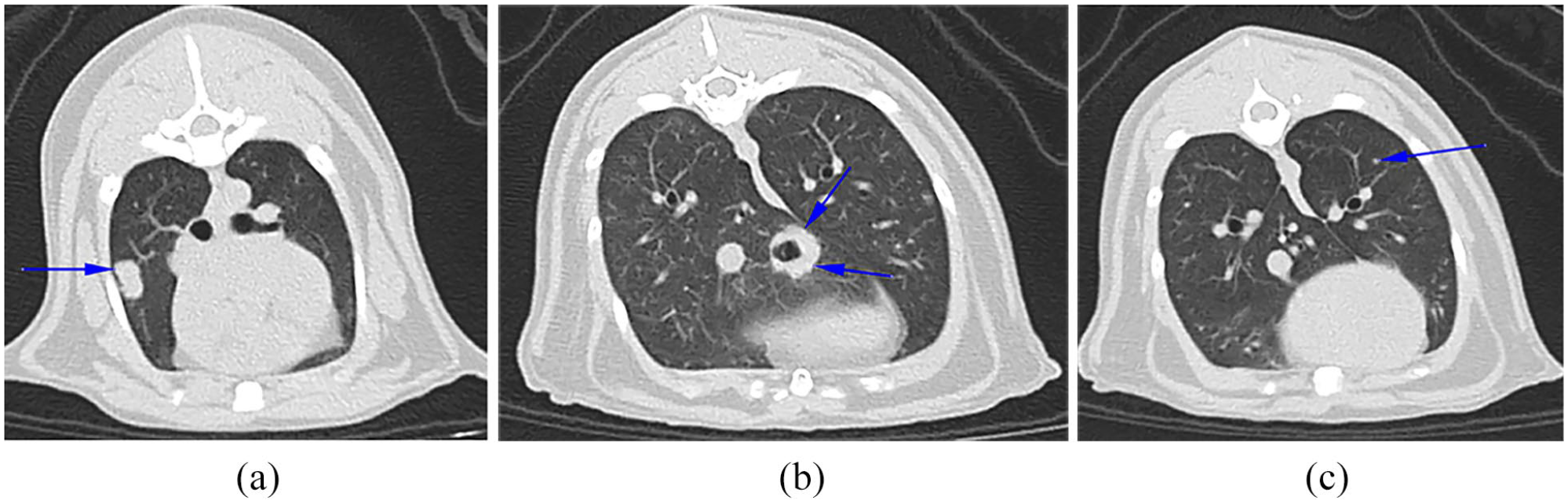
CT scan images of the same patient’s thorax as shown in Figure 2. Multiple soft tissue-attenuating nodular lesions (blue arrows) are present within the parenchyma of the right middle lung lobe (a), the accessory lung lobe (b) and the left cranial lung lobe (c). The owners decided to not pursue further investigations and elected for euthanasia
Five further cats with thoracic radiographic abnormalities were not suitable to receive RAI owing to non-thoracic pathology (abdominal neoplasia [n = 3], portosystemic shunt and triaditis [n = 1], and neutrophilic lymphadenitis and nephritis [n = 1]). One additional cat with thoracic radiographic abnormalities was diagnosed with carbimazole-induced immune-mediated haemolytic anaemia (IMHA) but received RAI once this had been treated. Change in treatment plan was not primarily related to thoracic radiographic abnormalities in this group (Figure 4).

Flowchart demonstrating the categorisation of hyperthyroid cats referred for radioiodine (RAI) treatment based on outcome in relation to system pathology. PSS = portosystemic shunt; IMHA = immune-mediated haemolytic anaemia
Of the 12 cases that had a change in their treatment plan related to thoracic radiographic abnormalities (Table 2), two had no cardiorespiratory signs upon presentation; 10 had systolic heart murmurs and six were tachypnoeic and/or dyspnoeic (in hospital and/or at home). One cat had a mediastinal mass but no respiratory signs. Of the cases with thoracic radiographic abnormalities, 18% (n = 35/194) had respiratory signs upon arrival or during hospitalisation and 73% (n = 142/194) presented with a heart murmur.
All cases but four (2%) underwent echocardiography. In 71% (n = 177/248) of these cases, cardiac abnormalities were identified, the most common being left ventricular hypertrophy, left atrial enlargement and diastolic dysfunction. In 25% (n = 62/248) of the cases there was evidence of cardiac disease upon echocardiography, but no concurrent thoracic radiographic abnormalities. In 9% (n = 23/248) of the cases there were abnormalities upon thoracic radiography suggestive of cardiac disease, but no concurrent echocardiographic abnormalities. In 19% (n = 48/248) of the cases there were abnormalities suggestive of cardiac disease, both on echocardiography and thoracic radiography. In 56% (n = 142/252) of the cases included in the study a heart murmur was identified upon auscultation and 77% (n = 110/142) of these had echocardiographic cardiac abnormalities.
Discussion
This study showed a high prevalence of concurrent thoracic pathology in hyperthyroid cats at the time of RAI assessment, with 77% of cats presenting a variety of abnormalities on their thoracic radiographs. This finding was expected as the study population comprised middle-aged to older cats. The most common abnormalities were pulmonary changes and predominantly bronchial patterns; the percentage of cases with bronchial or bronchointerstitial patterns was more than expected. The clinical significance in most of these cats was undetermined as there were no respiratory signs and/or further investigations were not performed. These pulmonary patterns could be reflective of occult airway disease being more common in older cats than previously appreciated. Alternatively, it could be representative of prior insult to airways or ageing, with bronchointerstitial patterns reported more commonly in cats >12 years than in young adult cats. 13
Cardiac abnormalities were also frequent, which is not surprising in view of the fact that hypertrophic cardiomyopathy is often seen secondary to hyperthyroidism in cats and is more common in older cats. 14 One study showed that hypertrophic cardiomyopathy (HCM) prevalence increases with age and that the positive predictive value of a heart murmur indicating HCM was 17.9–42.6% (higher in old cats). 12 Even though cardiac disease is better evaluated with echocardiography, not all centres that offer RAI have a cardiologist available. In these situations, thoracic radiography would be the main available imaging tool for assessment of significant cardiac disease. In this study 24% of cases with echocardiographic evidence of cardiac disease had no concurrent thoracic radiographic abnormalities. This discrepancy may be due to concentric hypertrophic changes that may not cause an increase in the overall size of the heart. This highlights the fact that significant cardiac disease may be missed on thoracic radiography. Plasma N-terminal pro-brain natriuretic peptide can also be used as a screening test for cardiomyopathy in cats that present with clinical signs of cardiac disease, such as heart murmur or dyspnoea, as well as in asymptomatic cats. 15 This could be used in conjunction with thoracic radiography when echocardiography is not an option for assessing hyperthyroid cats.
In 56% (n = 142/252) of the cases, a heart murmur was identified upon auscultation and 77% (n = 110/142) of these also had cardiac abnormalities upon echocardiography. This is a higher proportion than in the study by Watson et al, 16 where half of the hyperthyroid cats referred for RAI treatment had cardiac abnormalities upon echocardiography. In the same study, a heart murmur was identified upon auscultation in 63% of the cases with mild hyperthyroidism and in 90% of the cases with severe hyperthyroidism. In the present study, the percentage of cats with heart murmurs was lower but still >50%. Of the cats that had a heart murmur, 23% did not have any echocardiographic cardiac abnormalities. This highlights the fact that the presence of a heart murmur is not always a reliable indicator of cardiac disease in feline patients; conversely, the absence of a heart murmur does not exclude cardiac disease. This is in agreement with previous studies involving hyperthyroid and non-hyperthyroid cats.17,18
The results from this study identify the potential merit of thoracic radiology in cases undergoing an RAI assessment, as abnormal thoracic findings were found in three-quarters of the study population. However, as only 5% (n = 12/252) had a change in treatment plan based on thoracic radiographs, the results need to be combined with the clinical picture to allow the clinician to decide whether further investigations or alterations to the treatment plan are required (including whether RAI is suitable). Thoracic radiography is also of value when it comes to interpreting findings from other pretreatment screening tools, such as those found on abdominal ultrasound examination when neoplasia is a differential; for example, gut wall thickening, liver nodules, etc. In this study, four cases were excluded from having RAI treatment owing to abdominal neoplasia. In these cases, thoracic radiography enabled assessment for metastatic disease. Furthermore, in a cat that was diagnosed with IMHA, thoracic radiography was used to investigate for other triggers for IMHA. In these cases, even though thoracic radiography did not identify significant thoracic pathology, it was still considered to be a valuable diagnostic tool by excluding pathology.
This study has shown that cats presenting for RAI treatment frequently have occult pathology; most of the cases (86%) with abnormalities on their thoracic radiographs had no suggestive clinical signs reported by the owner or referring veterinarian. The majority of the pathologies (eg, bronchial/bronchointerstitial patterns, vertebral spondylosis and IVDD) were considered incidental. However, the significance of these findings could be underestimated, owing to current understanding of these changes in the aged cat population and/or lack of appreciation of the impact on the cat. This study also emphasises the challenge in identifying those cases that could have severe concurrent disease based on clinical presentation alone. Of the 12 cases that had a change in their treatment plan, two did not have any cardiorespiratory signs upon presentation; however, thoracic radiography identified one as having a large mediastinal mass and the second had a pulmonary nodule. In the remaining 10 cats that had pathology that warranted a change in treatment plan or excluded RAI, the indication for thoracic radiography, rather than a routine screening, could have been justified by examination; for example, investigation of heart murmur, tachypnoea and dyspnoea. However, equally, these signs could have been attributed to hyperthyroidism alone. In the remaining two cases that did not have cardiorespiratory signs upon presentation, screening thoracic radiography was useful, as it diagnosed primary thoracic disease and provided additional information where abdominal disease was present. From the 12 cases that had a change in their treatment plan, five subsequently had RAI treatment. In these cases the change in treatment plan was important as it helped identify and/or treat concurrent diseases, allowing further stabilisation to minimise the risk of deterioration during the isolation period post-RAI.
Limitations of our study include the retrospective data collection and low percentage of cases where a definitive diagnosis for the thoracic pathology was reached; thus, the clinical significance of some findings remains undetermined. In the majority of cases, the primary clinician did not consider these abnormalities to be significant enough to preclude RAI treatment, after combining them with the cat’s history and clinical picture. The study population is a referral population and does not consider those cats that are excluded from referral for RAI treatment, such as cats that are found to have clinically significant concurrent disease, identified by their first-opinion veterinarian precluding referral. On this basis, the prevalence of significant concurrent thoracic disease in hyperthyroid cats may be higher in the population of cats for which RAI is not considered. A further limitation is the use of radiography for screening, which is less sensitive than CT, as CT is the accepted gold standard for thoracic imaging. However, CT is more expensive and not available in every clinic so it would be difficult to justify its use in every case.
Conclusions
Pretreatment thoracic radiology can identify significant concurrent thoracic pathology in hyperthyroid cats referred for RAI treatment. The prevalence of thoracic pathology was high; however, the thoracic radiographic abnormalities considered clinically relevant for patient suitability for RAI treatment was low. Therefore, it is important that the radiographic results are combined both with the clinical picture and the results of other screening tests, to allow the clinician to ascertain whether a patient is a suitable candidate for RAI or not.
Footnotes
Author note
The preliminary findings of this study were presented at the 2017 EVDI Spring Meeting in Birmingham.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not necessarily required.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.