
Abstract
Objectives
This article aimed to report on the short- and long-term outcomes after transpelvic urethrostomy (TPU) as a first-line surgery to treat obstructive lower urinary tract disease (OLUTD) in male cats.
Methods
A retrospective review and follow-up owner telephone questionnaire for cats with OLUTD undergoing TPU as a first-line surgery between 2013 and 2019, at a single referral hospital, were performed. A minimum follow-up period of 1 year was required to be included in the study. Short- and long-term complications were defined as those that occurred, respectively, within or after the first 4 weeks postoperatively.
Results
Thirty-eight male cats were included. The short-term complication rate was 18%. Idiopathic lower urinary tract disease (ILUTD) and stomal stenosis (SS) were the two most frequent short-term complications. Long-term complications were reported in 34% of the cats and included ILUTD, urinary tract infection and SS. The mortality rate was 5%. Eighty-two percent of the owners were satisfied with the postoperative outcome. The most common reason for owner dissatisfaction was the occurrence of SS, especially because these complications required multiple surgical revisions to be definitively managed. The long-term quality of life was considered to be good to very good by 89% of the owners. Ninety-one percent of the cats were free of clinical urinary signs at the time of the questionnaire completion.
Conclusions and relevance
TPU can be an acceptable first-line surgical technique to treat cats with OLUTD. Most cats experienced a good to very good quality of life after TPU. Most complications were transient or manageable medically. Most of the major complications were SS, which can be technically challenging to address and may require multiple revision surgeries.
Keywords
Introduction
Urethrostomy is a surgical salvage procedure commonly performed in male cats to manage recurrent or permanent obstructions, or irreversible trauma of the urethra.1–9 Four urethrostomy techniques have been described in cats.10–13 Perineal urethrostomy (PU) is currently the recommended first-line technique for surgical management of obstructive low urinary tract disease (OLUTD).2–4,7,8,10 Prepubic urethrostomy (PPU) allows urinary diversion in cases of perineal or intrapelvic urethral lesions.11,12 Subpubic urethrostomy (SPU) and transpelvic urethrostomy (TPU) have been recommended as salvage procedures in cases of PU failure.13,14 TPU has been shown to be associated with lower morbidity and complication rates than reported with PPU.11–15 TPU has also been reported in nine cats as an alternative technique to PU for distal penile OLUTD. 14
Stomal stenosis (SS) is the most frequent major complication after PU in cats and is reported in up to 17% of these cats.15–18 Although persisting postoperative inflammation resulting from unresolved cystitis or from urethral sphincter impairment have been described as a predisposing factor,10,18–20 the size of the urethral stoma at the end of the surgical procedure appears to be critical in preventing SS after PU.16,18–21 In some studies, SS was associated with improper technique and failure to free the wider intrapelvic urethra from its pelvic attachments to the point where the bulbourethral glands lie at the skin surface.21,22 The diameter of the feline urethra progressively narrows from the mid-pelvic portion to the penis. The preprostatic and postprostatic urethra has been documented to be approximately 2.0 mm in diameter. The average urethral internal diameter is 1.3 mm at the level of the bulbourethral glands, and 0.7 mm at the penis.16,23
TPU provides an approach to the pelvic urethra that allows the stoma to be created at a more proximal location than PU, where the urethra is larger in diameter. 14 This new stoma is also further away from the obstruction site after TPU as the obstruction is more often located in the penile urethra.5,8,10,15,16,21,23 The urethrostomy is then performed at a site where the urethra is more likely to be healthy with a less ulcerated or inflamed mucosa. TPU has the advantage of preventing damage to both the innervation and the vascularisation on the dorsal aspect of the urethra.14,24,25 To date, only two publications including a limited number of cats (11 and eight cats, respectively) have documented the outcomes after TPU in male cats.14,15 Reported complications were idiopathic lower urinary tract disease (ILUTD), urinary incontinence (UI) and urinary tract infection (UTI). In the 19 cats following TPU reported in the literature so far,14,15 only one has developed an obstructive SS, considered as a major complication. 15 Based on the current published data and with the aim of creating a larger stoma to reduce the occurrence of SS, TPU was performed as a first-line procedure for treatment of OLUTD by one surgeon at our institution. To the authors’ knowledge, no large study documenting the clinical outcome of cats that have undergone TPU as a first-line procedure has been published so far.
This retrospective descriptive study was designed to evaluate short- and long-term outcomes after TPU on a larger number of cats than previously reported,14,15 when used as the primary surgical treatment for OLUTD.
Materials and methods
The study was approved by the veterinary hospital animal care and use committee.
Clinical files of client-owned cats that had undergone TPU as first-line surgical technique for management of OLUTD between January 2013 and December 2019 were evaluated. Cats having TPU for failed PU, trauma or neoplasia were excluded. A minimum follow-up period of 1 year was required for the cats to be included in the study. Data collected from the medical records included signalment, history, results of physical examination, urinalysis, urine culture, haematology, serum biochemistry, blood electrolyte panel, venous blood gas analysis and diagnostic imaging examination findings. Surgical reports, anaesthesia records and hospitalisation records were reviewed to obtain information about peri- and postoperative treatments, outcomes and complications.
The TPU was performed as previously described by Bernardé and Viguier. 14 All surgeries were performed by one board-certified surgeon (AB) after obtaining owner consent. Urinary calculi collected from the urinary tract were submitted for infrared spectroscopy analysis. Postoperative treatment systematically included intravenous crystalloid fluids and pain management with opiate analgesics (0.01–0.03 mg/kg buprenorphine [Bupaq, Virbac] IV q8h, or 0.1–0.2 mg/kg morphine chlorydrate [Morphine, Lavoisier] IV q4h). Non-steroidal anti-inflammatory drugs (0.05 mg/kg meloxicam [Metacam; Boehringer Ingelheim] SC q24h) was injected to cats with a preoperative serum creatinine concentration under 16 mg/l according to the International Renal Interest Society (IRIS) Acute Kidney Injury Staging system. 26 Amoxicillin/clavulanic acid (Augmentin, GlaxoSmithKline) was given preoperatively at 20 mg/kg IV, and continued postoperatively PO q12h (12.5 mg/kg, [Clavaseptin, Vetoquinol]) when a UTI had been diagnosed pre-operatively, while awaiting urine culture results. An Elizabethan collar was secured in place with a harness immediately after surgery.
All the patients were discharged from the hospital when serum blood urea nitrogen, creatinine and potassium concentrations were within normal limits, and urine outflow and appetite were considered normal. At discharge, detailed oral and written instructions were given to the owners regarding rest, litter type, urthrostomy site cleaning, dietary and drinking recommendations. Analgesic medication was continued depending on patient discomfort at the time of discharge. When a UTI was confirmed, antibiotics were prescribed for a minimum of 4 weeks postoperatively, and a urinary culture was recommended 5–7 days after the end of the antibiotherapy and in case of urinary signs. Owners were instructed to keep their cat at home, to replace the litter material with shredded newspapers, to clean the edges of the urethrostomy site with wet swabs and to apply a thin layer of a petrolatum-based ointment on the wound twice a day until removal of sutures 15 days after the procedure. The Elizabethan collar was to be left in place continuously for at least 1 week after suture removal. Diet recommendations were made based on the results of urinary crystal or calculi when available.
Long-term telephone interviews with the owners were conducted by one of the authors (CD). A questionnaire was used as a guiding framework to conduct the interviews and was adapted from Ruda and Heiene’s study (see the appendix in the supplementary material). 27 Direct conversation by telephone gave an opportunity for open discussion with the owners. Owners were asked about the frequency and severity of clinical signs. The authors defined mild urinary signs as moderate dysuria, pollakiuria, occasional hematuria or periuria. Severe urinary signs were defined as stranguria, oliguria or anuria, or UI. Intermittent clinical signs referred to few discontinuous episodes of micturition abnormalities followed by progressive resolution of the signs over time. Frequent urinary signs referred to discontinuous numerous episodes (more than 10 per month), or continuous evidence of micturition abnormalities. Minor complications were defined as those that did not require another surgical procedure and could be managed with medical treatment. 15 Major complications were defined as those that required surgical intervention, or that resulted in death or euthanasia. 15 The time interval between surgery and recurrence of lower urinary tract disease (LUTD) was recorded. Short-term complications were those that occurred within 4 weeks postoperatively. 15 Long-term complications were those that occurred after 4 weeks postoperatively. 15 The owners were also asked about the quality of life (QOL) of their cat after the TPU and about their satisfaction after the surgery.
Results
Thirty-eight cats were included in the study. Twenty-nine cats (76%) were domestic shorthair or domestic longhair cats, and nine (24%) were pure-breed cats. Thirty-four cats (89%) were neutered males and four cats (11%) were entire at presentation. The median age at the time of surgery was 6 years and 11 months, ranging from 5 months to 15 years and 9 months. Body weight ranged from 2.7 to 8.6 kg, with a median value of 5.7 kg. The median body condition score was 6/9 according to the WSAVA Global Nutrition Committee scoring, 28 ranging from 3/9 to 9/9.
All the cats in the study underwent TPU either for reobstruction after one episode of OLUTD (26/38 cats, 68%), or for reobstruction after two or more previous OLUTD episodes (12/38 cats, 32%). The obstruction at the time of the TPU was attributed to urethral urolithiasis in 14 cats (37%), to matrix-crystallin plugs in nine cats (24%), to UTI in seven cats (18%) and to ILTUD in eight cats (21%). Uroliths causing OLUTD were either struvites (57% of the cats) or calcium oxalate (43% of the cats). Matrix-crystallin plugs were struvite crystals in 67% of the cats and calcium oxalate crystals in 33% of the cats. Immediate preoperative urinary bacterial culture was positive in 7/25 cats. Bacteria isolated were Escherichia coli in 4/7 cats, Staphylococcus species in 2/7 cats and Enterobacter cloacae in 1/7 cats, all being sensitive to amoxicillin/clavulanic acid.
The median hospitalisation duration after surgery was 3 days (range 1–10). The median duration of follow-up was 3 years and 1 month, ranging from 1 year to 6 years and 7 months.
Short-term complications were encountered in 7/38 cats (18%). UTI was diagnosed in 1/38 cats (3%). No underlying cause of recurrence of clinical urinary signs could be identified in 3/38 cats (8%). Those complications were considered as minor as defined previously. Two cats (5%) were presented with SS. One of these cats underwent surgical revision with no further complications. The other cat was euthanased due to financial constraints. Premature loosening of some of the interrupted sutures was identified 1 week after TPU in one cat (3%). Sutures were replaced under general anesthesia with no debridement, and no further wound-related problem was reported in this cat. Neither urolithiasis nor UI were identified during the short-term follow-up period (Table 1). The short-term mortality rate was 3% (1/38 cats).
Short-term complications in 38 cats after transpelvic urethrostomy as a first-line surgery
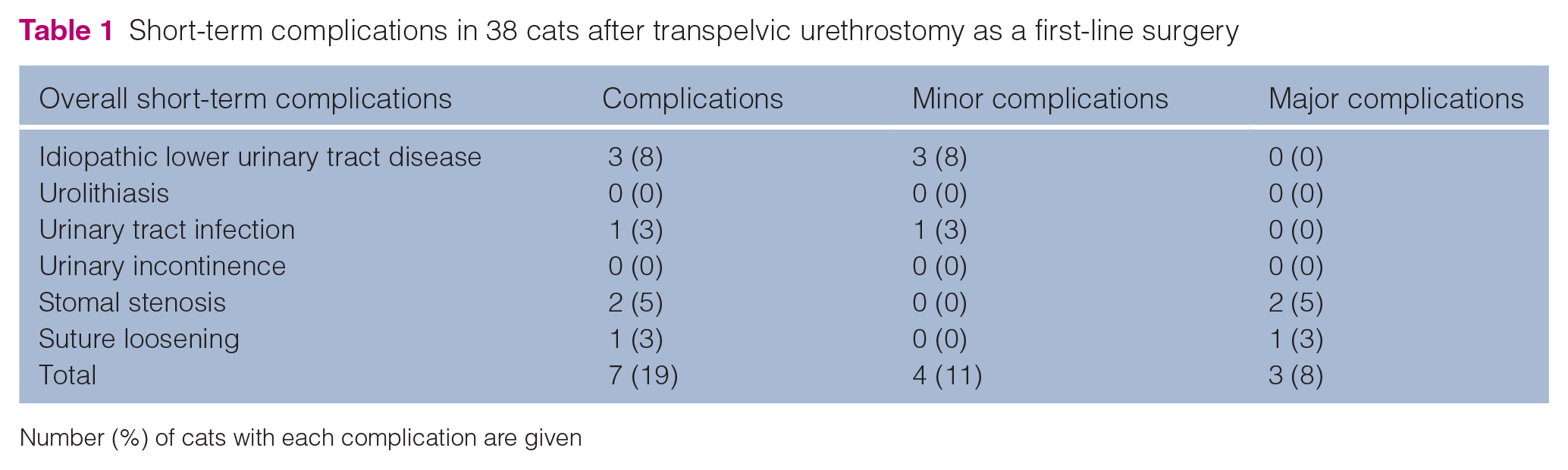
Number (%) of cats with each complication are given
Long-term complications occurred in 13/38 cats (34%), with two cats having multiple long-term complications, resulting in a total of 15 long-term complications.
Nine out of 38 (24%) minor long-term complications were detected. UTI was evidenced by positive bacterial culture in 5/38 cats (13%), 3 to 48 months after TPU. No underlying cause of recurrence of clinical urinary signs could be identified in 4/38 cats (11%) by a veterinarian. Two of these four cats still had clinical signs (dysuria, pollakiuria in one cat; dysuria, hematuria, periuria in one cat) at the time of the telephone interviews.
Major long-term complications occurred in 16% (6/38) of the cats. One cat (3%) with recurrence of bladder urolithiasis underwent a cystotomy 1 year after the TPU. Recurrence of the OLUTD signs was secondary to SS in 4/38 cats (11%). These four cats underwent a revision TPU in our hospital. Finally, one cat (3%) died 2 months after TPU owing to septic shock caused by an E coli UTI. No UI was reported during the long-term period (Table 2).
Long-term complications in 38 cats after transpelvic urethrostomy as a first-line surgery
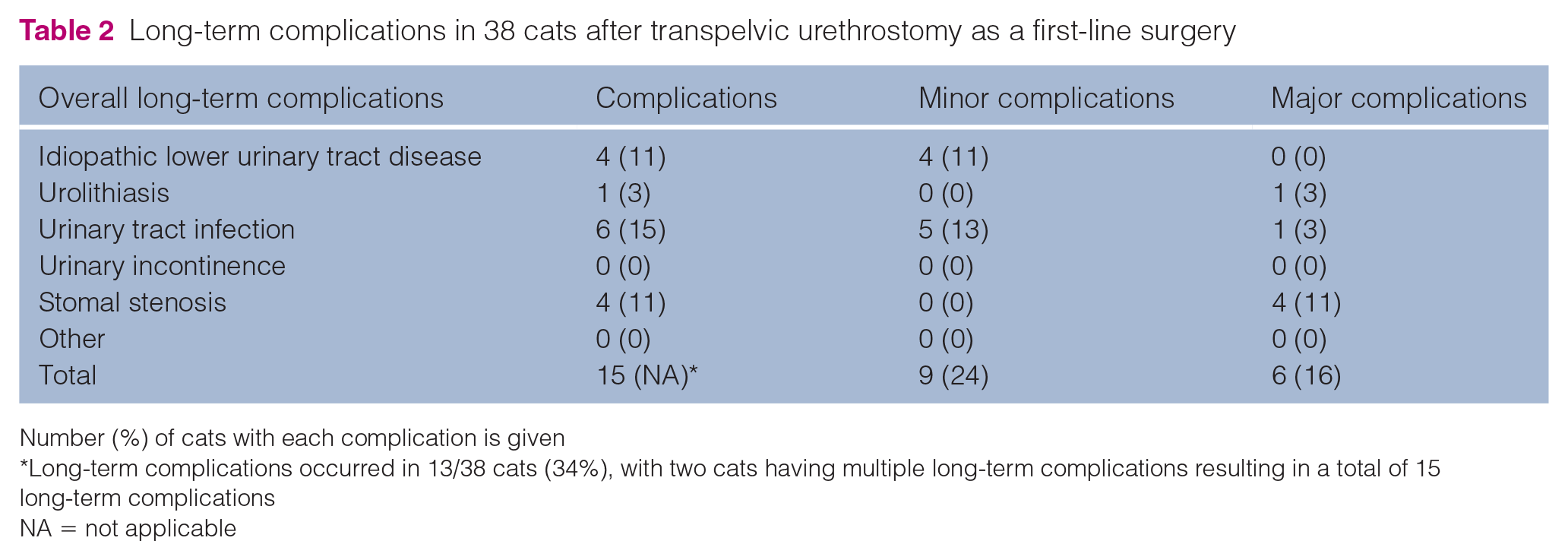
Number (%) of cats with each complication is given
Long-term complications occurred in 13/38 cats (34%), with two cats having multiple long-term complications resulting in a total of 15 long-term complications
NA = not applicable
Thirty-eight percent of the long-term complications occurred between 1 month and 4 months postoperatively, 22% between 4 months and 19 months and 39% more than 19 months after surgery. Thirty-two cats were still alive at the time of the long-term owner interviews. The cause of death was directly related to urinary issues in two cats. The overall mortality rate after TPU as a first-line surgery was 5% (2/38 cats).
Overall, 6/38 cats (16%) developed SS after TPU. Revision surgery was required in all six cats, as SS was responsible for recurrence of OLUTD. However, one cat was euthanased due to financial constraints. Five cats underwent revision surgery at our institution. SS was definitively resolved after the first revision surgery in 2/5 cats (40%). Two revision surgeries were required in 2/5 cats (40%) and three revision surgeries were performed in 1/5 cats (20%) due to the reoccurrence of obstructive SS. For the total of nine revision surgeries performed, an elliptical incision was performed around the stenosed stoma. Fibrotic tissues were dissected until healthy urethral mucosa could be reached. In 1/9 revision surgeries, a cranial extension of the ostectomy was performed to reach healthy urethral mucosa. The urethrostomy was then performed by suturing the skin to the mucosa.
Owners were totally satisfied with the outcome after TPU in 82% of the cases. The most common reason for owner dissatisfaction was the occurrence of SS. Long-term QOL was rated as good to very good in 34/38 cats (90%), moderate in 2/38 cats (5%) and poor to very poor in 2/38 cats (5%) by their owners. All cats that experienced severe urinary signs because of SS or UTI, leading to death or euthanasia, and cats with persistent ILUTD were considered by their owners to have a moderate to very poor QOL after surgery. Most of the cats (29/32, 91%) showed no urinary clinical signs at the time of the study, with a median time of 2 years and 1 month (range 2 months to 5 years and 4 months) since the last reported episode of LUTD.
Discussion
This study is the first to document outcomes of male cats for which TPU was performed exclusively as a first-line surgical procedure to manage OLUTD. In the population reported in the present study, the TPU was associated with an overall short-term complication rate of 18% and a long-term complication rate of 38%. The majority of these complications were transient or managed medically. Most cats showed no urinary clinical signs at the time of long-term follow-up and a majority of the owners reported a good to very good QOL for their cats.
Short-term minor complications were detected in 11% of the cats in the present study. In Bernardé and Viguier’s report, which included some cats for which TPU had been performed as a salvage procedure, the short-term minor complication rate was 18%. 14 The short-term minor complication rate after TPU documented by Seneviratne et al15 was three times higher (57%) than in the present study. This particular study included only seven cases of TPU that had been performed because of a failed PU or a proximal urethral lesion. 15 In Seneviratne et al’s study, all the cats had been hospitalised until the time of suture removal or returned to the referral hospital for suture removal, contrary to the present study where the median hospitalisation time was 3 days (range 1–10), and where some of the cats went to the referring veterinarian for suture removal. This increased monitoring in Seneviratne et al’s study may have contributed to detection of more minor complications by the veterinarians. 15
ILUTD and UTI were the most frequently encountered short-term minor complications after TPU in the present study, detected in 8% and 3% of the cats, respectively. Both complications have been identified in previous studies related to TPU.14,15 Several contributing factors to ILUTD and UTI after PU have been proposed, such as unresolved preoperative infection, non-normalised urine outflow, preoperative traumatic urethral catheterisation, widening and shortening of the urethra and neuropraxia.4,5,16,22,29–32 The same predisposing factors may also be a concern with TPU. As urine culture was not systematically performed at the time of initial presentation in most studies related to feline urethrostomies, including the present study, it is difficult to evaluate the potential influence of undiagnosed preoperative UTI on postoperative ILUTD and UTI after PU or TPU.14,15,33 Use of preoperative urethral catheters is assumed to predispose to UTI and ILUTD after PU.4,16,22,29–32 As catheterisation of the urethra is also commonly performed before and during TPU,14,15 it could also be a predisposing factor to postoperative ILUTD or UTI. Although TPU results in even more pronounced widening and shortening of the urethra when compared with PU, the rates of short-term postoperative UTI and ILUTD were not higher in the present study than previously described for PU.16,20,22,27,29–32
Short-term UI has been reported in 9 to 28.6% of cats after TPU,14,15 and was not observed in any of the cats in the present study. No dissection of the dorsal aspect of the urethra is required during TPU, which might protect the dorsal urethral innervation.14,16,24 The dorsal recumbency may also prevent iatrogenic sacrococcygeal nerve injuries that could potentially occur when cats are placed in ventral recumbency. Indeed, a cadaveric study has demonstrated that a larger degree of reduction in vertebral canal diameter was seen in the sacrococcygeal vertebral segments of cats placed in ventral recumbency compared with those placed in dorsal recumbency when performing a PU. 25 The clinical impact of positioning-dependent iatrogenic nerve injury could not be confirmed in a more recent study performed by the same team. However, some limitations were highlighted by the authors, such as the lack of statistical significance due to the small population or the relatively low sensitivity of the performed neurological examination. 34
Major short-term complications occurred in 8% of the cats in our study, two of them being an SS. A similar rate (14%) of major short-term complications was reported by Seneviratne et al, all being related to SS. 15 Although none of the short-term complications reported in Bernardé and Viguier’s study could be considered as major, as defined in our study, one of the cats had developed an SS during the short-term period. 14
This study reports an overall long-term complication rate of 34% after a TPU performed as a first-line surgery for treatment of OLUTD. This is similar to the long-term complication rate reported in Seneviratne et al’s study (33%). 15 Long-term complications were only reported in 18% of the cats in Bernardé and Viguier’s study. 14 This difference may be explained by a shorter median follow-up duration in Bernardé and Viguier’s study (median 19 months, range 9–42), 14 compared with Seneviratne et al’s report (median 29.5 months, range 2–125) 15 and to the one in the present study (median 37 months, range 12–79 months). In the present case series, 39% of the long-term complications occurred after 19 months. Minor long-term complication rates were similar among the three studies. ILUTD and UTI were the only two minor complications reported.14,15
The mortality rate related to TPU was low (5%), which is consistent with previous studies.14,15 Contrary to the studies of Bernardé and Viguier14 and Seneviratne et al,15 in which no major complications were reported over the long-term follow-up period, 17% of the cats experienced major long-term complications after TPU in the present study. Sixty-seven percent (4/6) of these major long-term complications were related to SS, which was challenging to address and, in some cases, required multiple revision surgeries.
The overall rate of postoperative SS requiring a second surgery was 0–14% in previous reports on TPU and 16% in the present study. Proposed contributing factors for SS after PU include lack of surgeon experience, failure of the surgeon to reach the pelvic urethra, excessive tension on sutures, poor apposition between the skin and the urethral mucosa, and inflammation or trauma by licking or rubbing at the stoma.4,10,16,18–20 In the present study, all TPUs were performed by the same experienced board-certified surgeon. The pelvic urethra, which is almost three times wider than the penile urethra at the location where TPU is performed, had been reached with certainty. 14 TPU provides an approach to the pelvic urethra that allows the stoma to be located further away from the obstruction site, on a healthy part of the urethra, especially when the obstruction is located in the penile urethra. However, the overall postoperative rate of SS after TPU appears to be similar to those reported in many publications on PU (3–17 %).15,16,21,22,29 SS occurring after TPU seems to be a challenging postoperative complication, with some cats requiring multiple revision surgeries in our study. Surgical revision after a failed TPU is technically difficult as local tissues are deeply modified secondary to chronic inflammation and fibrosis of the local subcutaneous tissues and urethra. To create a new stoma proximal to the abnormal tissue, the ischiatic ostectomy can be extended cranially in order to reach a healthy part of the pelvic urethra, which was performed in the surgical revision of one cat in the present study. However, the pelvic ostectomy should be limited as pubic fracture has been described after extended TPU in one case report. 35
This study reports good to very good owner-rated long-term QOL after TPU in 89% of the cats, and 82% of the owners were totally satisfied with the outcome. Most cats (91%) were disease-free at the time the owners completed the questionnaire. The median time since the last clinical signs of LUTD was 2 years and 1 month (range 2 months to 5 years and 4 months). These findings are consistent with Seneviratne et al’s study, 15 which reported a good long-term QOL in 83% of the cases after TPU. However, 5% of the owners in the present study considered the QOL of their cats to be poor or very poor after TPU compared with the 0% reported by Seneviratne et al. 15 SS and persistent ILUTD were the reasons for which QOL was considered as poor.
This study has several limitations, with some related to its retrospective nature. The lack of direct examination at our hospital during the follow-up period may have led to an underestimation of short-term complications. The fact that the long-term follow-up was based on a delayed owners’ questionnaire may have led to some bias. Because the study was conducted over a 7-year period, some omission of information or some degree of inaccuracy of the owners’ answers may be suspected.
Conclusions
Results suggest that TPU is an acceptable first-line surgical technique to treat cats with OLUTD. Most of the cats were free of clinical urinary signs after TPU at the time of the study. Most clients were totally satisfied with the outcome. The main postoperative complications were ILUTD, UTI and SS. Most of those complications were transient or manageable conservatively. However, SS leading to failed TPU was the most frequent major complication reported in the present study. Revision surgery after SS can be challenging with multiple revision surgeries required in a small number of cats.
Supplemental Material
Appendix
Owner questionnaire about the outcome of their cat after TPU as a first-line surgery
Footnotes
Author note
CD contributed to the conception of the work, the acquisition, analysis and interpretation of data; wrote the manuscript; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
FB contributed to revising the manuscript critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AB contributed to the conception of the work, carried out all the surgeries; wrote the manuscript and revised it critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Supplementary material
The following file is available online:
Appendix: Owner questionnaire about the outcome of their cat after TPU as a first-line surgery.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.