
Abstract
Objectives
Partial laryngectomy is an organ-sparing surgical procedure for the removal of laryngeal masses which has not been described in cats. The aim of this study was to report on the surgical procedure and the short- and long-term clinical outcomes of cats that underwent partial laryngectomy.
Methods
Medical records were retrospectively collected over a 4-year period in two institutions. The following data were retrieved: signalment, history, clinical signs, diagnostic test results, surgical procedure, postoperative management, complications and outcome.
Results
Six cats underwent partial laryngectomy. The most common clinical signs in cats with laryngeal masses were stridor (n = 4) and dyspnoea (n = 4). In all cats, a full-thickness portion of one or several laryngeal cartilages was resected, including thyroid cartilage alone (n = 2), thyroid cartilage and arytenoid (n = 2), and arytenoid cartilage and epiglottis (n = 2). The resected laryngeal masses were reported to be lymphoma (n = 3), carcinoma (n = 1), laryngeal cyst (n = 1) and inflammatory laryngeal disease (n = 1). All cats survived the surgical intervention of partial laryngectomy. Four cats showed varying degrees of respiratory distress in the short-term postoperative period. A temporary tracheostomy tube was placed in two cats. No other postoperative complications were noted in the short- or long-term. Four cats were still alive at the time of writing. These cats survived at least 252 days.
Conclusions and relevance
In a small number of cases, our results show that successful long-term outcomes after partial laryngectomy are achievable, with longer survival times than previously reported. Therefore, partial laryngectomy should be considered as a viable treatment option in cats with laryngeal masses.
Introduction
Neoplastic and inflammatory laryngeal masses are uncommon conditions in small animals.1–5 Lymphoma and squamous cell carcinoma are the most commonly diagnosed laryngeal masses in cats, followed by inflammatory laryngeal disease (ILD).1,5,6 The most common presenting sign is dyspnoea. Other reported clinical signs are stridor, dysphonia, coughing, gagging and anorexia.1,3,6 The prognosis for cats with a laryngeal mass depends on the nature of the mass and on its treatment modality. In one study, the median survival time (MST) of cats with a laryngeal mass was 5 days, with 7.4% still alive at 1 year. 1 More specifically, the MSTs for laryngeal lymphoma, carcinomas and inflammatory disease were 107 days, 92 days and 91 days, respectively. 6
Described treatment options include chemotherapy, radiation therapy, permanent tracheostomy, mass removal via laryngotomy and multimodal therapies.1,4,5 In humans, the primary treatment modalities for laryngeal masses are open partial laryngectomy and radiotherapy. 7 Partial laryngectomy (PL) for tumour treatment appears to be an uncommon procedure in domestic animals, and limited information regarding techniques and outcomes is available. Several cases have been reported in dogs, but surgical techniques and results in cats have not yet been published.8,9 The purpose of this study was to report on the presentation, diagnosis, surgical treatments and outcomes of cats that underwent PL. We hypothesised that PL would be well tolerated and could provide long-term survival.
Materials and methods
The medical records of cats that underwent PL to treat laryngeal masses were retrospectively reviewed in two institutions between 2016 and 2020. PL was defined as the removal of the laryngeal mass, including the laryngeal mucosa and a full-thickness portion of one or several laryngeal cartilages. Data, including age, breed, sex, reason for presentation, clinical signs, diagnostic work-up, anatomical location of the mass, surgical procedure, duration of hospitalisation, complications, histopathology results, postoperative adjunctive therapy and outcome, were collected.
Complications were divided into perioperative, short-term and long-term. A complication was outlined as an adverse event related to the surgical procedure. Perioperative complications were defined as complications occurring before, during or after surgery but before extubation. Complications that occurred after tracheal extubation and within 14 days of surgery were defined as short-term complications. Long-term complications were defined as a complication developing 14 days or more after surgery. 10
Furthermore, complications were classified as either major or minor. Complications were defined as major if their management required another surgical intervention, such as a temporary tracheostomy. Minor complications were defined as complications managed without the need for additional surgery.
Descriptive statistics are presented as mean ± SD or percentages for continuous and normal distributed variables, or as median (range) for categorical data.
The overall survival time was considered as the number of days from surgery to the date of death or last contact.
Results
Six cats met the inclusion criteria. Of these cats, the most common breed was domestic shorthair (n = 3). Other breeds were Oriental Shorthair, British Shorthair and a Siamese cat (one each). All cats were >6 years old (median 9 years; range 6–11). Two cats were spayed females and four cats were castrated males. All cats were presented for upper respiratory clinical signs. The most common presenting complaints were stridor (n = 4) and dyspnoea (n = 4). Other abnormal findings were anorexia (n = 3), loss of voice, cough, enlarged tonsils (two each) and gagging (n = 1).
Diagnostic work-up and staging
Preoperative laryngoscopy and CT were used as adjunctive tools to evaluate the origin of the presented clinical signs (n = 4). Laryngoscopy or CT were used as the sole diagnostic tool in one case each. Laryngoscopy revealed the extent and the surface appearance of the mass (Figure 1).
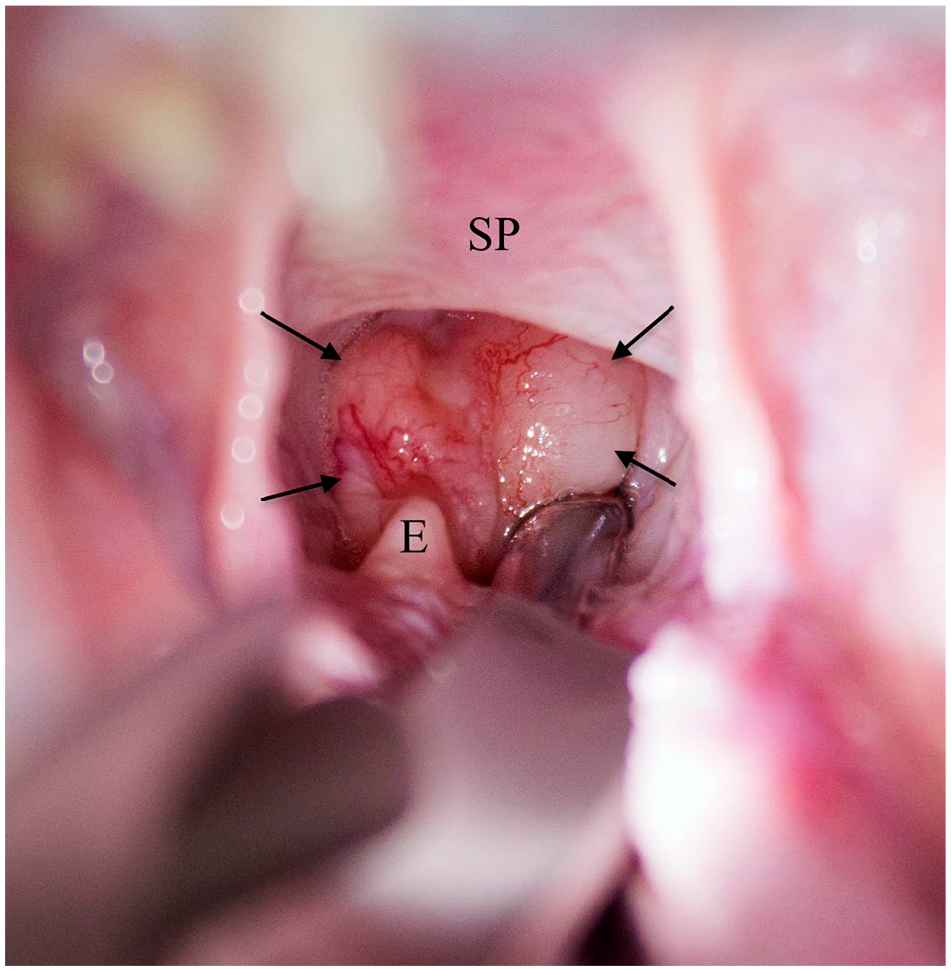
Transoral view of the laryngeal mass (arrows) in cat 1.
CT confirmed the location and established the size of the mass (Table 1). The mean tumour size (length, width and height) was 12 × 7 × 11 mm3.
Summary of imaging findings, diagnosis, treatment and outcome of six cats treated with partial laryngectomy

Euthanased
AC = arytenoid cartilage; TC = thyroid cartilage; E = epiglottis; ST = short-term complication; NA = not available; COP = cyclophosphamide, vincristine and prednisolone; ILD = inflammatory laryngeal disease; AB = antibiotics
Preoperatively, cytology samples were taken in three cases and a grab biopsy in one case. In two cases cytology results were consistent with lymphoma, which was later confirmed by histopathology. In cat 4, cytology showed a benign epithelial tumour; however, histological examination yielded a diagnosis of lymphoma. The biopsy of cat 3 was consistent with carcinoma.
Work-up for metastatic disease included CT of the head, neck and thorax (n = 4) or thoracic radiographs (n = 2). All cats were free of pulmonary metastatic disease and aspiration pneumonia. Cervical lymph nodes were enlarged in two cats, but were not sampled (cats 3 and 4).
Pretreatment
In two cases, prednisolone was administered prior to surgery. Cat 4 received prednisolone (0.5 mg/kg q12h PO [Prednicortone; Dechra]) 3 weeks before surgery, owing to the assumption of a benign process. The mass decreased in size after 1 week of prednisolone, leading to the remission of clinical signs but regrew when the prednisolone dosage was reduced.
Cat 6 received prednisolone (1 mg/kg q24h PO) and amoxicillin clavulanate (12.5 mg/kg q12h PO [Kesium; Ceva]) 2 days before surgery, to address its respiratory distress.
Description of technique
Premedication consisted of a combination of midazolam (0.2 mg/kg IV [Dormicum; Roche]) and methadone (0.2 mg/kg IV [Comfortan; Dechra]) in three cats. Two cats received only buprenorphine (0.02 mg/kg IV [Vetergesic; Ceva]) and one cat only methadone (0.2 mg/kg IV). All cats were preoxygenated prior to induction. Four cats were induced with propofol (2–6 mg/kg IV to effect [Propofol-Lipuro; BBraun]) and two cats with alfaxalone (0.5–4 mg/kg IV to effect [Alfaxan Multidose; Jurox]). General anaesthesia was maintained with isoflurane (IsoFlo; Zoetis) in oxygen and fentanyl boluses (0.001–0.005 mg/kg IV [Fentadon; Dechra]) were administered as needed.
All cats received a course of cefuroxime (22 mg/kg q90 min IV [Zinacef; GSK]) at induction. Dexamethasone (0.2 mg/kg IV [Dexadreson; MSD]) was administered in two cases.
For the PL, the patients were positioned in dorsal recumbency with a slightly hyperextended neck. A ventral midline incision was made over the larynx. The paired sternohyoid muscle were separated and retracted. The cricothyroid ligament and the thyroid cartilage were incised on their ventral midline (Figure 2a). Stay sutures were placed to facilitate retraction (Figure 2b). For better exposure of the mass, the endotracheal tube was removed, and the cats were reintubated through the ventral laryngotomy with a sterile tracheal tube or an oesophageal feeding tube. Additional stay sutures or small Gelpi retractors were placed on the thyroid cartilages to improve exposure of the laryngeal lumen and mass (Figure 3a). Resection of the mass involved partial resection of the thyroid cartilage (n = 2), epiglottis and arytenoid cartilage (n = 2), or thyroid cartilage and arytenoid cartilage (n = 2) (Figure 3b). Marginal resection of the laryngeal masses was performed using fine Mayo scissors, leaving 2–3 mm margins of normal mucosa wherever possible. Care was taken to manipulate the mucosa as little as possible to reduce postoperative oedema.
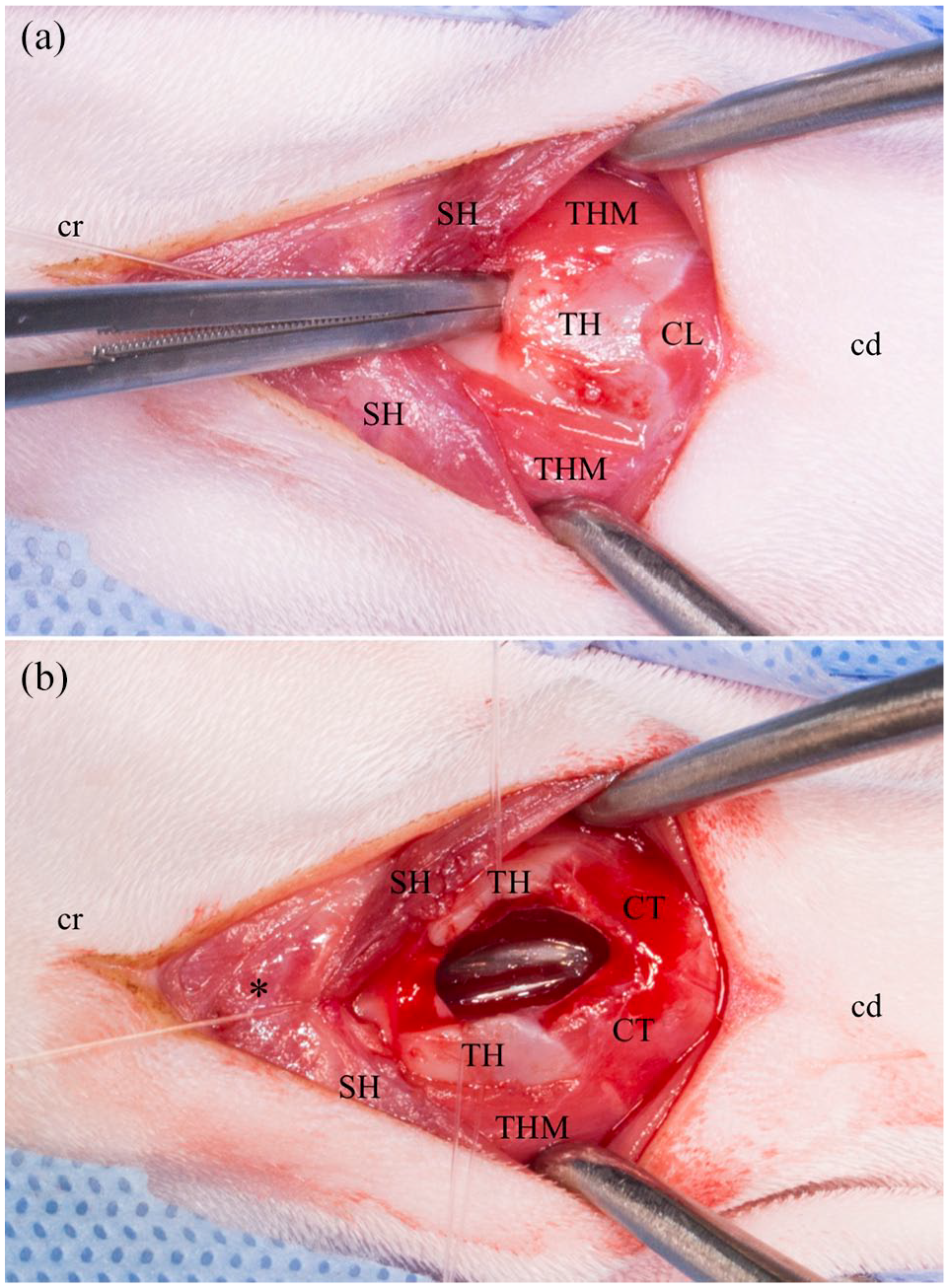
(a) Ventral approach to the larynx. The cranial border of the thyroid cartilage was palpated and elevated (Debakey forceps) before being incised in the midline. (b) The thyroid cartilage was incised on its ventral midline and kept open with stay sutures. *Basihyoid bone; cr = cranial; cd = caudal; SH = sternohyoid muscle; TH = thyroid cartilage; THM = thyrohyoid muscle; CL = cricothyroid ligament; CT = cricothyroid muscle
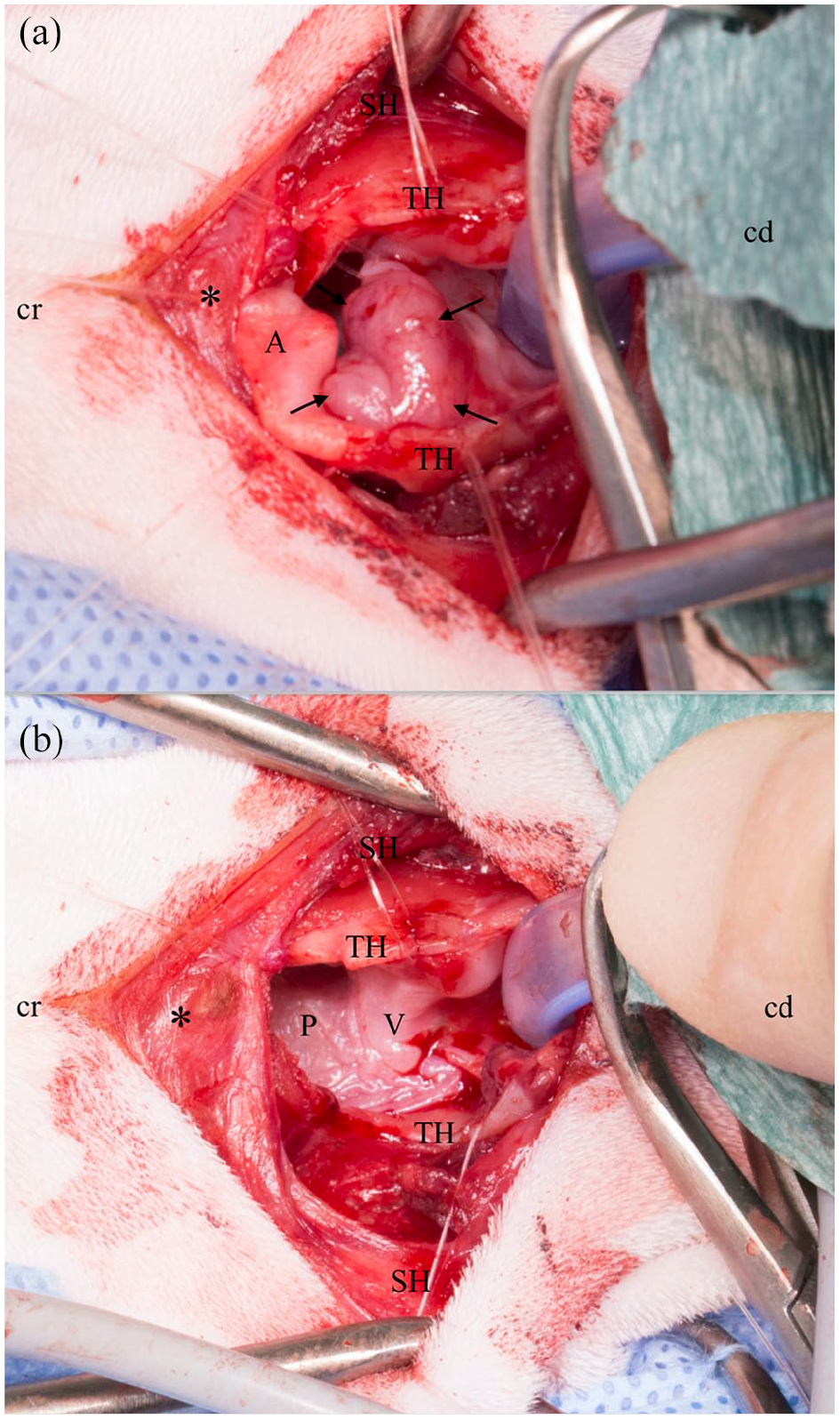
(a) The laryngeal mass (arrows) was exposed and elevated with additional stay sutures; (b) aspect of the larynx after resection of the mass. Portions of the thyroid and arytenoid cartilage were resected. *Basihyoid bone; cr = cranial; cd = caudal; SH = sternohyoid muscle; TH = thyroid cartilage; A = arytenoid cartilage; P = dorsal pharyngeal wall; V = vocal cord
Where possible, the remaining laryngeal mucosa was sutured to the remaining laryngeal cartilage (cat 5). In cat 3, pharyngeal mucosa was used to close the laryngeal defect and the laterodorsal defect in the pharyngeal mucosa was left to heal by second intention. In cases where primary closure would have led to a narrowing of the laryngeal diameter, a muscle patch using the sternohyoid muscle was used to cover the cartilage defect (cats 1, 2, 4 and 6) (Figure 4). Attention was paid to place the suture knots outside the laryngeal lumen as often as possible. The wounds were otherwise closed routinely.

The defect in the thyroid cartilage was reconstructed with a muscular patch (right sternohyoid muscle). *Basihyoid bone; cr = cranial; cd = caudal; SH = sternohyoid muscle; rSH = right sternohyoid muscle
A temporary tracheostomy was performed in one case (cat 3), and two oesophagostomy feeding tubes were placed in two cases (cats 1 and 3), at the surgeons’ discretion.
Postoperative medical treatment
Analgesia was provided with methadone (0.1 mg/kg IV), buprenorphine (0.02 mg/kg IV), or a combination of methadone (0.1 mg/kg IV) and meloxicam (0.05 mg/kg IV). The duration of administration of analgesics was determined by scoring pain according to the Glasgow Composite Measure Pain Scale. 11
Three cats received adjuvant chemotherapy after histopathology confirmed lymphoma. Cats 2 and 4 were treated with cyclophosphamide, vincristine and prednisolone, and cat 1 with prednisolone (1 mg/kg q24h) as a sole treatment. Cat 6 was diagnosed with ILD and received a course of prednisolone (0.5 mg/kg q12h) and amoxicillin clavulanate (12.5 mg/kg q12h).
Postoperative complications
Breathing difficulties were noticed in four cats in the short-term period. Two complications were classified as major (cats 2 and 3) and two as minor (cats 1 and 4).
Two days after surgery, cat 2 developed upper airway oedema. It received glucocorticoids and supplemental oxygen, but respiratory dyspnoea was still present. A temporary tracheostomy was therefore performed, which remained in place for 9 days.
Cat 3 was dependent on its tracheostomy and developed respiratory distress as soon as a membrane was forming over the stoma. Additionally, it required intensive care with the tracheal stoma because of recurrent partial occlusion. This cat was euthanased 7 days after surgery owing to continuing partial occlusion of the tracheal stoma.
Cats 1 and 4 showed signs of respiratory distress in the immediate postoperative period but could be managed with a course of glucocorticoids.
No complications were observed in cats 5 and 6. In the four cats that were still alive at the time of writing, no long-term complications have been noted.
Histopathology
The most common histopathological diagnosis was lymphoma (n = 3). The remaining three cats had a laryngeal carcinoma, a cyst and ILD (n = 1 each).
In cat 4, cytology was discordant with histopathology. A benign epithelial mass was identified preoperatively, and lymphoma was diagnosed on postoperative histopathology.
Margins were considered as complete (cats 1, 5 and 6) or incomplete (cats 2, 3 and 4) in three cats each.
Clinical outcome
The median length of hospitalisation was 4 days (range 1–22 days; mean 6.6).
Five cats survived to discharge. Four cats were alive at the time of data collection, which was >1 year after surgery for three of them.
Cat 1 was still alive 1339 days postoperatively but was then lost to follow-up. Cat 2 was euthanased 85 days after surgery due to recurrence of lymphoma. Cat 3 developed severe respiratory distress and was euthanased 7 days postoperatively. Cats 4, 5 and 6 were still alive at the time of writing, 654, 618 and 252 days after surgery, respectively.
Discussion
Laryngeal masses are uncommon in cats,1–5 and, to the best of our knowledge, PL has not been previously reported in this species.
In this study, PL techniques varied with the extent and location of the mass. In all cats, a full-thickness portion of one or several laryngeal cartilages was resected. Primary closure of the mucosal defect was the preferred closing technique. In cases where apposition of laryngeal mucosa was not feasible, patches of pharyngeal mucosa or sternohyoid muscle were used. Laryngeal web formation is a reported complication in human and veterinary medicine if primary closure of laryngeal mucosa is not possible. It can lead to stenosis or require tracheostomy in severe cases.12,13 Even though the authors were aware of this possible complication, in four cases it was decided to leave the laryngeal mucosa to heal by secondary intention. The decision was based on the fact that primary closure would have not been feasible or would have led to severe narrowing of the laryngeal diameter. None of the cats in our study developed signs of laryngeal web formation.
Other major complications described in human literature after PL are wound infections, laryngocutaneous fistulae, voice impairment, aspiration pneumonia and swallowing disorders.14–17 In the present study, none of these complications arose. The most common complication was respiratory distress in the short-term period, which occurred in four cases. Cats 1 and 4 responded well to supplemental oxygen and administration of glucocorticoids, and did not require any additional surgical intervention. Cat 2 developed severe laryngeal oedema 2 days after surgery. It did not respond well to conservative treatment, thus necessitating a tracheostomy. The tracheostomy was left in place for nine days. In cat 3, a tracheostomy tube was placed during surgery at the surgeon’s discretion. This cat experienced recurring problems of tracheostomy tube obstruction, requiring it to remain in intensive care. As a result, its owners opted for euthanasia 7 days after surgery. The complication described in cat 3 was consistent with the study of Guenther-Yenke and Rozanski, 18 according to which the overall complication rate in cats undergoing temporary tracheostomy is 87%, with 40% of cats having life-threatening complications, including tube occlusion and tube dislodgement. Stepnik et al 19 pointed out that the mortality rate is 6.6 times higher in cats receiving a tracheostomy for ILD than for any other reason. Because of their high complication and mortality rates, tracheostomies are rarely performed in cats. 19 In the present study, none of the long-term survivors needed a temporary tracheostomy. The authors recommend monitoring PL patients carefully in the immediate postoperative period and only placing a tracheostomy tube if it becomes necessary, rather than as a preventive measure.
In previous studies, the mean survival time of cats with neoplastic laryngeal masses ranged from 15.5 days to 61 days.1,6 Two of the four long-term survivors in our study were diagnosed with lymphoma, which could be accurately diagnosed preoperatively in 2/3 cats. In the study by Taylor et al, 20 an excellent response of laryngeal lymphoma to chemotherapy was reported, with 100% showing response and 87.5% complete remission. Although a high response rate was observed, the median survival was only 112 days. Cat 4 also responded well to glucocorticoid administration prior to surgery. However, the laryngeal mass grew back as soon as glucocorticoids were discontinued. This cat might have gone into complete remission with chemotherapy alone, but its survival after PL and chemotherapy compared favourably with the previously reported survival times. Moreover, chemotherapy may be impractical if the laryngeal obstruction is severe, as response to treatment may take a few days. A temporary tracheostomy is a bridging option but, as mentioned above, it can be challenging to maintain in cats. 18 In this context, the authors deem it sensible to surgically resect lymphoma masses severely obstructing the larynx, as it can immediately relieve the airway obstruction, cytoreduce or remove the tumour, and allow precise definitive diagnosis and phenotyping, all in one procedure. In the present study, 2/3 cats with laryngeal lymphoma were still alive at the time of writing, 654 (cat 4) and 1339 (cat 1) days postoperatively. Cat 2 was euthanased 85 days postoperatively owing to tumour recurrence.
A laryngeal cyst was detected in cat 5, which, to our knowledge, had only been reported once in a cat. 21 The diagnosis was already suspected from the CT studies, but a tumour could not be excluded. Owing to the sessile nature of the mass, PL was considered preferable in case of a malignant cystic mass. Should the mass turn out to be a benign cyst, recurrence was a significant risk, 22 especially as the mass was sessile, and PL was perceived to lower this risk. The cat therefore underwent PL, which led to long-term resolution of its clinical signs. The cat was still alive at the time of writing, 618 days after surgery.
Cat 6 was diagnosed with ILD. Reported MSTs for ILD in cats vary between 5 and 91 days, ranging from 1 to 2800 days.1,6,23,24 Treatment consists of administration of glucocorticoids and antibiotics, and temporary tracheostomy can be required in severe cases.19,24 Inflammatory and neoplastic lesions are indistinguishable on gross examination. Therefore, further investigations (preferably histopathology) are required.6,23,24 Cat 6 was presented with an acute onset of dyspnoea. Clinical signs had not improved with administration of glucocorticoids, and the cat was in life-threatening respiratory distress on presentation. This cat may have responded to prolonged conservative treatment, but such treatment would have taken some time to be effective; the cat would have required a temporary tracheostomy in the meantime, which would have carried the risks of complications previously discussed, and PL was considered a sensible alternative. The cat was still alive at the time of writing (252 days after surgery) and doing well without further treatment.
Diagnosis was made either with laryngoscopy, CT, or both. Radiography is of limited use in the staging of laryngeal masses, as not all laryngeal masses are visible on radiographs and the superimposition of the larynx with adjacent structures make images difficult to interpret.1,3 MRI is superior to CT in ruling out neoplastic invasion of the cartilage. 25 However, CT was preferred over MRI because it allows evaluation not only of the laryngeal mass, but also of possible metastatic disease in the neck and thorax. The authors recommend the use of both laryngoscopy and CT or MRI for preoperative planning. The laryngeal examination can determine aspect and location of the mass, as well as assess the laryngeal function. It may also be possible to distinguish between sessile and pedunculated masses, which impacts greatly on surgical planning. CT yields additional information about the exact extent and possible deep infiltration of the mass.
The authors found that the ventral approach to the larynx was swift and straightforward, and that it provided sufficient exposure to work comfortably in all cases, especially when the lumen of the larynx was freed by placing a new sterile tracheal tube through the laryngeal opening. During surgery, emphasis was put on gentle tissue handling given that the upper airways of cats are delicate. To avoid postoperative mucosal oedema, attention was paid to manipulate the mucosa as little as possible by working predominantly with stay sutures to avoid repetitive tissue microtrauma. Suture knots were placed outside the laryngeal lumen as much as possible, to minimise the postoperative laryngeal obstruction and irritation. PL may be viewed as a radical procedure, as portions of laryngeal cartilages are excised, but it is not highly invasive. In our study, it allowed rapid relief of the laryngeal obstruction in cats with severely obstructive laryngeal masses and did not appear to carry higher risks of complications compared to tracheostomy.
The limitations of the present study include the small number of cases and its retrospective nature. Larger studies are needed to determine a correlation between surgical procedure and outcome. Being retrospective, this study included procedures performed by multiple surgeons at different centres, with different routine postoperative care and hospitalisation times.
Conclusions
Our study demonstrates that successful outcomes after PL in cats are achievable. In cats with laryngeal masses, PL allowed rapid relief of the laryngeal obstruction and provided longer survival times and less severe complications than previously reported in the literature. Therefore, PL should be considered for the treatment of laryngeal masses in cats.
Footnotes
Acknowledgements
The authors thank Dr Jonathan Bray and Mag Christoph Leichtfried for the contribution of their cases.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.