
Abstract
Case series summary
This case series describes the neuromuscular blockade (NMB) following 0.15 mg/kg intravenous (IV) cisatracurium administration in 11 cats undergoing ophthalmological surgery and anaesthetised with isoflurane. Anaesthetic records were analysed retrospectively. Neuromuscular function was assessed by a calibrated train-of-four (TOF) monitor. Cats were 73 ± 53 months old, weighed 4 ± 1 kg and were of American Society of Anesthesiologists’ physical classification 2. Duration of anaesthesia and surgery were 144 ± 27 and 94 ± 24 mins, respectively. The lowest TOF count was zero in four cats, four in six cats and for one cat the TOF ratio never decreased below 31%. The time of onset was between 1 and 6 mins after the administration of cisatracurium and the mean duration of action was 20.4 ± 10.1 mins.
Relevance and novel information
Cisatracurium at a dose of 0.15 mg/kg IV did not consistently induce a TOF count of zero in all cats. The dose used in these cats did not produce any remarkable cardiovascular side effects. Although the NMB was not complete, the dose given was sufficient to produce central eyeball position, which was the goal of the ophthalmic surgeries.
Introduction
Although cats have been used as an experimental model to investigate the pharmacology of neuromuscular blocking agents, 1 there is still limited information on the clinical use and duration of action of these drugs in cats. 2 Cisatracurium is one of the non-depolarising neuromuscular blockers that belongs to the benzylisoquinoline group; it is a competitive antagonist of acetylcholine at post-synaptic nicotinic receptors. It causes the inactivation of these receptors, leading to muscular paralysis. 3 Cisatracurium is the purified form of one of 10 stereoisomers of atracurium and, according to the human and veterinary literature, it has fewer adverse effects such as histamine release and undesirable cardiovascular effects than seen with atracurium.1,3 This case series describes the neuromuscular blockade (NMB) produced by a single or repeated dose of cisatracurium in 11 cats during isoflurane anaesthesia for ophthalmic surgery.
Case series description
The anaesthetic records of cats undergoing ophthalmic surgeries and anaesthetised with isoflurane from July 2017 to August 2019 were selected retrospectively from our institutional database.
The inclusion criteria consisted of cats that received 0.15 mg/kg cisatracurium intravenously (IV) as the first dose, and cats were monitored using a train-of-four (TOF) monitor (TOF-Watch SX; Organon). The cats were classified were of American Society of Anesthesiologists’ physical status 2. With the help of hypodermic needles (23 G Agani; Terumo), electrodes were placed 1 cm apart in the lateral tibial area in regard to the peroneal nerve: proximally for the positive electrode and distally for the negative one. The piezoelectric crystal sensor was fixed on the dorsal aspect of the ipsilateral paw.
Before administering cisatracurium the free movement height was configured to establish a control height value of 100%. Every 13 s, the nerve was stimulated by the TOF watch and values were recorded on a separate sheet.
Data from the medical records were collected in Microsoft Excel and included age, breed, sex, body weight, duration of anaesthesia, and type and duration of the procedure. Clinical parameters, recorded every 5 mins, included the following: body temperature; heart rate; systolic arterial pressure (SAP [Ultrasonic Doppler Flow Detector Model 811-B; Parks]); haemoglobin saturation (Nellcor; Datex Capnomac Ultima); end-tidal carbon dioxide pressure, end-tidal isoflurane concentration and respiratory rate (RR) (VT9000 multimonitor [Veterinary Technics] or EKG Hewlett Packard 78353A Monitor)); and peak inspiratory pressure (Drager Cicero anaesthesia machine or Penlon, Prima 320; [Veterinary Technics]). The peak onset of NMB was established to be the time of cisatracurium administration until the lowest TOF ratio (%) or TOF count (1–4) was observed. The time and dose of the first cisatracurium administration, the NMB onset time, and the time and number of additional cisatracurium boluses were recorded. Finally, the time to recovery (from the last dose administered and TOF ratio ⩾95%) and the use of neostigmine were also registered.
Drug doses and administration routes used for premedication, induction and maintenance of anaesthesia were recorded (Table 1). The time between the end of anaesthesia and extubation, adverse effects and the anaesthetist’s experience (diplomate, resident, intern) were noted. Data were assessed using MedCalc 19.2. A Shapiro–Wilk test was used to evaluate normal distribution. Data with a normal distribution are presented as mean ± SD, and data with a non-normal distribution are presented as median (range).
Doses and administration routes of drugs used for premedication, induction, maintenance of anaesthesia and adjunct drugs recorded

IM = intramuscularly; IV = intravenously; ETAg = end-tidal inhaled agent; ETT = endotracheal tube; CRI = constant rate infusion
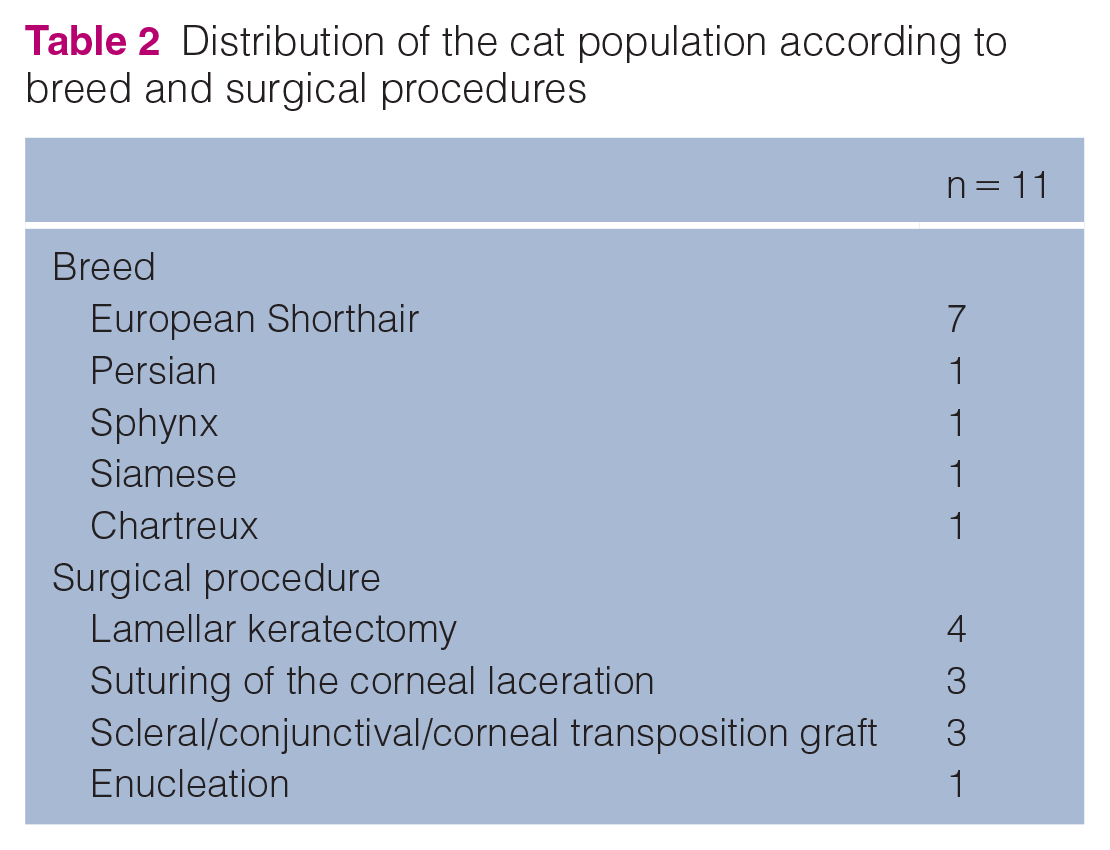
A group of 11 cats (five neutered males, two intact males, two spayed females, two intact females) with a mean ± SD age of 73 ± 53 months and a mean ± SD weight of 4 ± 1 kg fulfilled the inclusion criteria. All information regarding breed and surgical procedures is given in Table 2.
Distribution of the cat population according to breed and surgical procedures
All cats were administered lactated Ringer’s solution at 3–5 ml/kg/h IV using a fluid pump (VET-PRO VIP 2000 infusion pump). Some adverse events were seen before the administration of cisatracurium. Bradycardia (70–75 beats per min [bpm]) and severe hypotension (mean arterial pressure 35 mmHg) were observed in one cat before cisatracurium injection and treated with boluses of glycopyrrolate (0.005 mg/kg IV) and crystalloids (20 ml/kg/h for 15 mins IV). Moderate hypotension was seen in two other cats and resolved by modifying isoflurane concentration and boluses of crystalloids. These adverse events were resolved before the administration of cisatracurium.
Tachycardia (170–200 bpm) was observed in two cats on two occasions. The tachycardia was unrelated to the administration of cisatracurium and responded to the administration of anaesthetic drugs. Therefore, it may be concluded that the tachycardia was a sign of insufficient depth of anaesthesia. All cats were mechanically ventilated (anaesthetic machines: Drager Cicero or Penlon Prima 320) with a median RR of 16 breaths per min (range 6–35); the median tidal volume was 40 ml (range 20–85) and the median peak inspiratory pressure was 8 cmH2O (range 5.8–20).
Before and after the administration of cisatracurium bolus(es), all cats were monitored with the TOF watch device and data were recorded manually every 15 s throughout the procedure.
The mean time between the induction of anaesthesia and the first administration of cisatracurium (Tfirst) was 40.7 ± 12.9 mins. The peak onset time of the NMB, measured as the time from Tfirst to its maximal effect, was a median of 2 mins (range 1–6). The mean time of duration of action (between Tfirst and the moment when NMB effects began to recover from the NMB) was 20.4 ± 10.1 mins.
During the surgical procedures, in order to maintain an appropriate central eye position, 7/11 cats were topped up with 0.05 mg/kg of cisatracurium: two cats had four top ups (TUs), four cats had two TUs and one cat had three TUs. In seven cats, cisatracurium 0.05 mg/kg (TU1) was administered 18.5 ± 12.6 mins after Tfirst. In these cats, the second dose of cisatracurium (0.05 mg/kg [TU2]) was administered 21.1 ± 10.3 mins after TU1. In three cats, the third dose of cisatracurium (0.05 mg/kg [TU3]) was administered 17.3 ± 6.8 mins after TU2. Fortwo cats, the fourth dose of cisatracurium (0.05 mg/kg [TU4]) was administered 25 and 12 mins after TU3, respectively. The time between two TUs ranged from 7 to 45 mins. The lowest TOF count was zero in four cats and four in six cats. In one cat, the maximal block was obtained at a TOF ratio of 31%. Neostigmine (0.01 mg/kg) was administered to eight cats at the end of surgery at 87.5 ± 26.0 mins after Tfirst. The decision was made with the agreement of each anaesthetist. Some decided to antagonise the patient according to the last administration of cisatracurium to prevent any residual NMB. The others preferred to antagonise even though the animal was recovered entirely from the NMB; finally, others did not antagonise the cats at all.
The mean time between the last administration of cisatracurium and a TOF ratio ⩾95% was 48.3 ± 23.2 mins. This included all cats, regardless of whether they received neostigmine or not, and regardless of the TOF ratio at the time of neostigmine administration. Not enough data were recorded in the anaesthetic sheets to analyse the time between the neostigmine dose and a TOF ⩾95%. No adverse events were seen in the recovery phase. Anaesthesia was performed by a resident in nine cats, a European College of Veterinary Anaesthesia and Analgesia diplomate in one cat and an intern in one cat.
Discussion
In this case series, cisatracurium was used at a dose of 0.15 mg/kg, which is within the dose range proposed for this species in textbooks, 4 and by a previous study, which used doses of 0.06–0.25 mg/kg. 1 In the latter study, the theoretical dose of 0.06 mg/kg was calculated as the effective dose where the twitch height was reduced by 95% (ED95).
The onset time in the present case series showed individual variation (1–6 mins), but it was similar to the onset time of 3.7 ± 0.1 mins reported previously. 1 For comparison, dogs receiving the same dose (0.15 mg/kg), had an onset time of 2.9 ± 0.8 mins. 5 Data from the latter study indicated that the onset time of the NMB induced by cis-atracurium can be shortened in isoflurane-anaesthetised dogs administered fentanyl and lidocaine. 5 It can also be influenced by others drugs that affect muscle contractility and/or cardiac output, such as benzodiazepines, 6 acepromazine, 7 alpha-2 adrenoceptor agonist drugs,7,8 propofol9,10 and inhalant agents.10,11 To date, there has been no study in cats comparing cisatracurium and different anaesthetic protocols. In the present case series, there was a huge variety of protocols (see Table 1), which could also have influenced the results.
In cats, the duration between injection(s) to recovery to 95% twitch height has been reported to range from 8 to 14 mins for most of the isomers of atracurium. 1 For a dose of 0.06 mg/kg of cisatracurium, a duration of action of 12.7 ± 0.9 mins was calculated. According to these authors, there are no cumulative effects of cisatracurium, even when four times the ED95 dose was given or when cisatracurium was given as a constant rate infusion. 1
Contrary to the article by Wastila et al, 1 we observed a longer duration of action (which ranged from 9.9 to 14 mins in their study) of 20.4 ± 10.09 mins for a single dose of 0.15 mg/kg, measured from injection to the moment when the fading response reduced. Moreover, the moment of reduction in fading is not equivalent to the 95% recovery of twitch height seen in the Wastila et al study. 1 The duration of action could even be longer. This longer duration of action could be influenced by the dosage or the concomitant use of other drugs. Another study showed that the NMB was significantly enhanced and prolonged by isoflurane vs propofol. 11 For the same dose of cisatracurium (0.15 mg/kg), dogs had a similar duration of action (34 ± 9 mins) to the present case series, with a significant difference seen for the fentanyl group (28 ± 7 mins). 5
One of the main events seen was an incomplete fading response. The TOF number never decreased below four twitches for seven cats, which meant that only between 70% and 74% of acetylcholine receptors were blocked.4,12 This may be due to various factors. Clinical paralysis may require more or less of the drug, depending on the dose used. The concurrent anaesthetic agents were chosen based on the speed of onset required, the duration of block desired and the body area where muscle relaxation was needed.3,4 Moreover, the various degrees of fade induced by non-depolarising NMB agents in repetitive muscular contractions may be due to the varying affinities or binding kinetics of pre- and post-synaptic nicotinic receptors. 13 It is also important to note the difficulty in placing the electrodes because of the size of patient and that unintended displacement of the patient or the electrodes may occur during the intervention.
Even if the TOF count did not reach zero, the paralysis was sufficient for all ophthalmic surgeries, according to the surgeons. One of the primary explanations proposed in the literature is that the intensity of the NMB will depend on the dosage and the anatomical position of the neuromuscular unit target. 3 The extraocular muscles are paralysed prior to the skeletal muscles, leading to globe centralisation. This sensibility of the extraocular muscles might be explained by their small size and their dense innervation.
No adverse cardiovascular effect related to cisatracurium administration was observed in this case series, confirming the safety of this drug.1,4,14 Some authors have reported its wide margin of safety.1,4,14 According to Wastila et al, ‘Cis-atracurium is about 1.5 times more potent than atracurium, less likely to release histamine, and has weaker cardiovascular or autonomic effects’. 1 Indeed, in another study of cats, plasma histamine concentrations were unchanged when up to 60 and 85 times the ED95 of cisatracurium was administered.1,4
There are some limitations to this case series. First, the literature concerning cats and cisatracurium is particularly old and includes only healthy cats, while we have described its use in a clinical setting including cats of various ages and with comorbidities. Secondly, the results are derived from only 11 cats. The number of patients in this report administered cisatracurium was too small to draw complete conclusions from. Thirdly, a wide range of anaesthetic protocols was used and it is well known that drugs such as inhaled anaesthetic agents or central myorelaxants can interfere with the effect of cis-atracurium as they do with other neuromusclar blocking agents. It would be interesting to carry out a prospective controlled study that allows better control of the intensity of the NMB and to determine an appropriate dosage for this species and ophthalmological surgery requirements.
Conclusions
Cisatracurium used at an initial dose of 0.15 mg/kg with TUs of 0.05 mg/kg appears to be safe in cats undergoing ophthalmic surgery. Although the fade was incomplete, the dose given was sufficient to produce a central eyeball position, which was the goal of the ophthalmic surgeries. The cisatracurium block lasted for approximately 20 mins and did not induce any adverse events.
Footnotes
Acknowledgements
We thank our entire ‘A-team’ for conscientiously collecting data during the latter years, and the ophthalmological team for performing the surgeries.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.