
Abstract
Objectives
Changes in bowel movements (BMs) are an important clinical sign in many diseases, including chronic kidney disease (CKD), and the purpose of this study was to collect information on BMs and fecal scores in both apparently healthy and CKD cats. A secondary aim was to assess owner awareness of BM frequency.
Methods
Owners were asked to complete an initial online questionnaire about their cat’s health and litter box habits (including predicted BM frequency and fecal scores) and were then asked to clean the box daily for 7 days and report results (observed frequency of BMs and fecal scores) daily. Differences in BM frequency and fecal scores between apparently normal and CKD cats were compared using the Mann–Whitney test, and predicted vs observed data were compared using the Wilcoxon signed rank test. Difference in percentage of cats defecating more or less than once daily were assessed with Fisher’s exact test.
Results
Survey data from 124 owners of apparently healthy cats and 43 owners of CKD cats who submitted two or more days of daily observations (in addition to the initial questionnaire) were analyzed. Eighty-five percent of apparently healthy cats were observed to defecate one or more times per day and 15% defecated less than once per day. Fifty-eight percent of CKD cats defecated one or more times per day and 42% defecated less than once per day. A significantly higher percentage of CKD cats defecated less than once per day in comparison with apparently healthy cats (P <0.0001). Observed BM frequency was significantly less in CKD cats compared with healthy cats (P = 0.02). Observed fecal scores were not significantly different between healthy and CKD cats.
Conclusions and relevance
The observed BM frequency of cats with CKD was less than apparently healthy cats and represents a clinically important variation from normal.
Introduction
Cats with chronic kidney disease (CKD) have been identified to be at an increased risk of severe constipation requiring emergency treatment. 1 However, little is known about the prevalence of subclinical constipation in stable CKD cats in the home environment. As CKD has been shown to be a highly prevalent disease in feline practice, understanding this potential aspect of the disease has the possibility to impact a large number of cats. 2 The reason for the association between constipation and CKD is likely multifactorial and potentially stems from changes in hydration status, electrolyte disturbances (specifically hypokalemia), gastrointestinal physiologic alterations and pharmacologic management of the condition.1,3,4 Similar associations between constipation and CKD have been demonstrated in human medicine, as well as an association between the severity of constipation and risk of incident CKD, end-stage renal disease and progressive decreases in glomerular filtration rate. 5
Changes in bowel movements (BMs) are a commonly reported clinical sign in feline practice. 6 The specific clinical sign of diarrhea is identified at a relatively high 2.6% general population prevalence during primary care visits for cats. 2 However, other gastrointestinal clinical signs, such as constipation, are likely under-reported or unnoticed until they are severe in nature. 1 Despite being a less common reason for evaluation in primary care practice, constipation is a common and challenging presenting complaint in emergency feline medicine. 1 This may result from under-recognition of subclinical constipation and BM changes in cats. Collectively, this information underscores the importance of recognizing changes in a cat’s gastrointestinal clinical signs and specific defecation habits for health monitoring of presumed healthy cats and early intervention for cats beginning to show signs of disease.
The aim of this study was to use a daily survey to establish frequency of defecation and associated defecation behaviors in apparently healthy cats and CKD cats. A secondary aim of the study was to assess how aware owners are of the normal behaviors of their apparently healthy cat’s or CKD cat’s litter box and defecation habits. The hypothesis of the study was that CKD cats would have lower defecation frequencies and lower fecal scores compared with apparently healthy cats.
Materials and methods
A series of online surveys were designed for cat owners, aged 18 or older, evaluating elimination behaviors. The study was reviewed by the Institutional Animal Care and Use Committee (IACUC) and Institutional Review Board at The Ohio State University and was determined to not require IACUC approval as the study did not involve the use of animals. The survey was propagated to cat owners on a number of social media platforms (Reddit, Twitter, Facebook, Instagram and Snapchat). The survey was also propagated directly and indirectly to owners through their veterinarian via emails to cat owners, feline only veterinary practices, feline specific interest groups, the ACVIM listserv and the Vet Professionals website and database of cat owners and veterinary professionals (www.vetprofessionals.com). The surveys were open online between the dates of 13 May 2019 and 20 December 2019. In order to participate, respondents were required to have an alive, indoor cat that lived with them and was either apparently healthy or diagnosed with CKD and could be evaluated for 7 days consecutively. Each owner could only participate one time and for one cat only.
On the first day of the study, respondents were asked to complete an initial survey consisting of 35 background questions about the cat to help confirm the cat’s health status, its elimination behavior, the owner’s awareness of their cat’s elimination habits, estimated frequency of BMs, urinations and estimated fecal score (see files 1 and 2 in the supplementary material). When asked about specific habits, owners were asked to compare current habits to what is considered historically normal or typical for the cats (ie, prior to CKD diagnosis). Respondents were then asked to scoop their cat’s litter box daily for the next 6 days and fill out a corresponding survey each day. Surveys for days 2 through 6 consisted of eight questions specifically about the cat’s elimination behavior (eg, observed number of BMs in the previous 24 h) on those days (see questions in files 1 and 2 in the supplementary material). The final day 7 survey consisted of 16 exit questions including those asked on the day 2–6 surveys as well as questions pertaining to the owner’s knowledge of their cat’s elimination behaviors (see files 1 and 2 in the supplementary material). Observed number of BMs refers to the total number of BMs identified by the owner in the litter box. This includes those that were witnessed and those that were not witnessed directly by the owner. Questions pertaining to fecal scores and body condition scores throughout the study were reported by the owner using a provided color copy of the Purina Fecal Score Chart and Purina Body Condition Chart, respectively. Follow-up emails were sent to owners on a daily basis to encourage completion of all 7 days.
Cats were classified as apparently healthy, CKD or other based on the results of the screening survey. In order to be considered apparently healthy, the cats must have been seen by a veterinarian within 12 months of starting the study and deemed clinically healthy. These cats were additionally screened based on reported body condition, reported clinical signs and diet/medication history provided by the questionnaire. Cats were considered diagnosed with CKD if they had been seen by a veterinarian within 12 months of starting the study and diagnosed with CKD based on veterinary evaluation. Creatinine data were collected when available. Cats were considered unhealthy based on their reported medications, clinical signs, lack of recent veterinary evaluation and diagnosed conditions reported in the day 1 survey. Owners of cats with known abnormal clinical signs (eg, cough), diagnosed illnesses identified on screening questions or those that had not been evaluated by a veterinarian in the past 12 months were excluded. Information from cats receiving medications that are known to causes changes in BMs, urinations or indicative of being prescribed for a disease process, were excluded from the study. Allowed concomitant treatments included anti-parasiticides and non-specific nutritional supplements. A complete list of excluded medications is available online (see file 3 in the supplementary material). Indoor cats were defined as cats that spent less than 5% of their time outside unless that time was spent in an enclosed ‘catio’ or similar indoor/outdoor enclosure. Cats that spent greater than 5% of their time outdoors were excluded from final results.
The majority of questions were multiple choice with some short answers to explain and provide additional details. Short answers were evaluated and grouped based on similarity during the data analysis. Completion of the entire day 1 survey as well as two or more consecutive follow-up surveys were required for inclusion in the data set reported here. Predicted data was based on owner responses from the day 1 survey, prior to daily evaluation of elimination behaviors. Observed data was based on averaged recorded variables obtained from the multiple, consecutive follow-up surveys. Individual median observed responses was used to calculate BM frequency and fecal scores by age in both apparently healthy cats and CKD cats.
Descriptive statistical analyses were performed on all data then summarized and reported. Data were tested for normality using the D’Agostino Pearson test and reported as either median and range or mean and standard deviation based on results. For comparison data between predicted data from day 1 surveys and observed data on days 2–7 surveys, only individuals completing the baseline survey and at least two consecutive follow-up surveys were included in analyses. Associations between categorical variables was assessed with either the Fisher’s exact test or χ2 analyses. Differences between groups were compared with paired t-tests or the Wilcoxon signed rank test or one-way repeated measures ANOVA or Friedman test as appropriate based on normality testing. Data collected from the survey were collated and stored using FormSite (Vroman Systems) before downloading to Microsoft Excel for analysis. Statistical analyses were completed using GraphPad Prism.
Results
There were 435 respondents who completed the day 1 survey in its entirety for apparently healthy cats and 94 respondents who completed the day 1 survey in its entirety for CKD cats. These surveys were screened for completion, inclusion/exclusion criteria, as well as a number of follow-up surveys as described previously, which eliminated 311 submissions from the apparently healthy group and 51 of the submissions for the CKD group; thus 124 respondents from the apparently healthy group and 43 from the CKD group were included in the analysis. Creatinine values were available for 26 of the 43 CKD cats. The median creatinine was 221.05 µmol/l (range 141.67–291.79 µmol/l) [2.5 mg/dl (range 1.6–3.3 mg/dl)]. The number of follow-up surveys completed for apparently healthy cats were a median of 5 (range 2–6). In all, 34.7% of respondents of apparently healthy cats completed all requested surveys. The number of follow-up surveys completed for CKD cats were a median of 6 (range 2–6). The percentage of respondents of CKD cats completing all requested surveys was 76.7%. Responses to the surveys came from 19 countries; mainly the USA (59.5%) followed by the UK (19.3%), Australia (8.0%), and Canada (5.5%). The remaining responses came from Brazil, Netherlands, Hong Kong, Czech Republic, Ireland, Germany, Chile, Croatia, Bosnia and Herzegovina, Spain, Romania, Poland, Philippines, Italy and Mexico. Each of these had five or fewer individual responses per country.
Background information on respondents participating in the survey is outlined in Table 1. This table includes information on previous cat husbandry experience, how many years they have owned/lived with cats, whether respondents had previously had a cat that had a urinary blockage, constipation or chronic diarrhea, and whether respondents were from single cat or multi-cat households. The distributions of categorical background information variables were not significantly different between apparently healthy cats and CKD cats. When owners of multi-cat households were asked to describe how they were able to differentiate feces in the litter box, the most common responses were size (width, length), location, color, smell, shape and moisture levels.Signalment and environmental information on the cats included in the study is reported in Table 2. This table includes descriptive data on approximate age, sex, reproductive status, breed, as well as number, cleaning frequency and type of litter used in litter boxes. The distributions of cat signalment and environmental categorical variables were not significantly different between apparently healthy cats and CKD cats, with the exception of age distribution (P <0.0001). The distributions of cat signalment and environmental categorical variables were not significantly different between CKD cats with creatinine reported and CKD cats without creatinine reported.
Respondent information: descriptive data pertaining to respondent background information
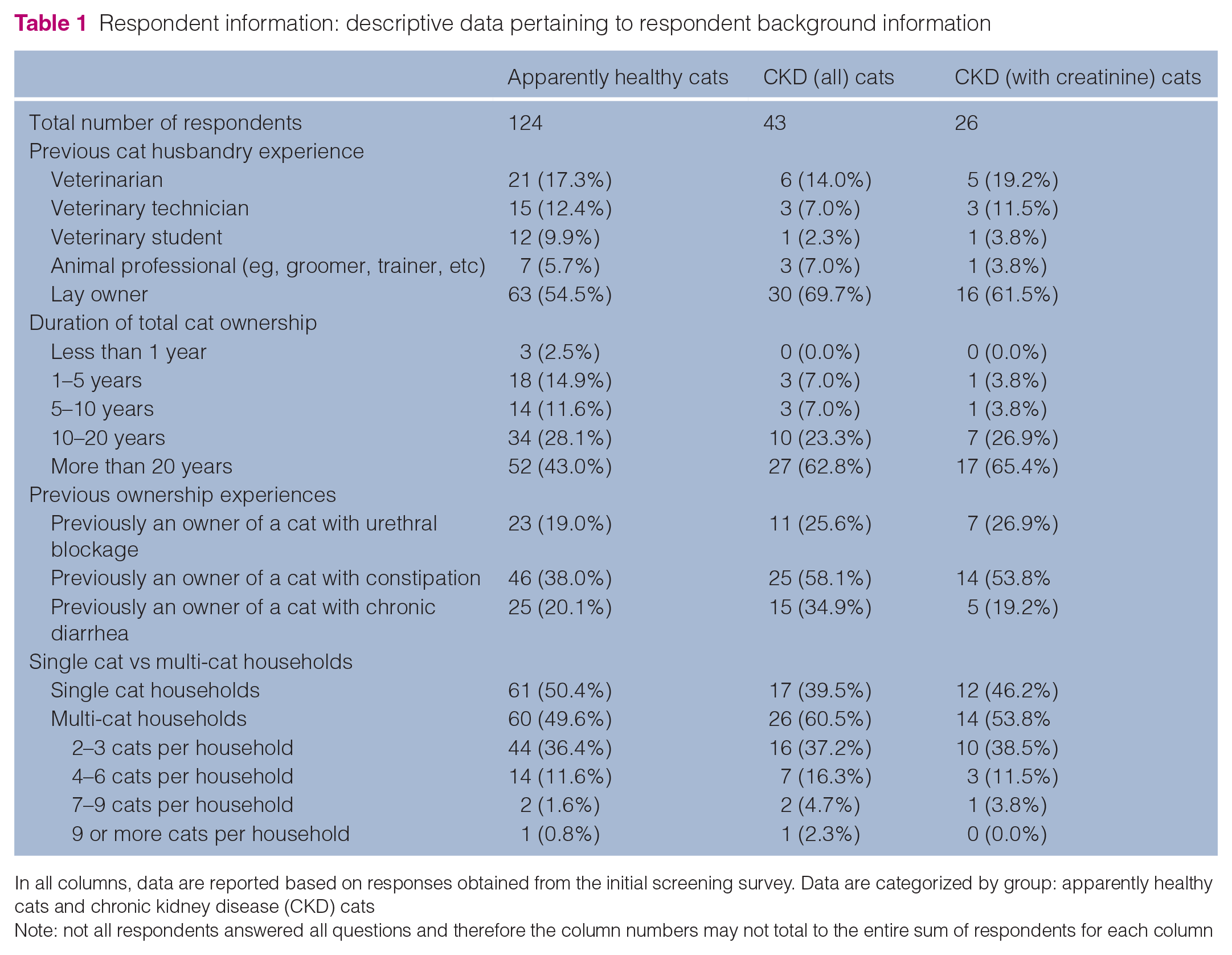
In all columns, data are reported based on responses obtained from the initial screening survey. Data are categorized by group: apparently healthy cats and chronic kidney disease (CKD) cats
Note: not all respondents answered all questions and therefore the column numbers may not total to the entire sum of respondents for each column
Cat and home environment information: descriptive data pertaining to the cat’s signalment, physical characteristics and home environment

In all columns, data are reported based on responses obtained from the initial screening survey. Data are categorized by group: apparently healthy cats and CKD cats. Statistically significant differences in the distribution of responses between healthy cats and CKD cats is denoted with an asterisk
Note: not all respondents answered all questions and therefore the column numbers may not total to the entire sum of respondents for each column
Ten (23.3%) of the cats in the CKD group had previously been evaluated for constipation by their veterinarian. In one case, a manual removal of feces under anesthesia was required for resolution and in four cases enema therapy was used for resolution of previous episodes of constipation. Eleven (25.6%) of cats in the CKD were receiving laxative medications including PEG 3350 (9, 20.9%), lactulose (2, 4.7%) and laxatone (1, 2.3%) at the time of study. Previously used constipation remedies reported by the owners of CKD cats included commercial laxatives, pumpkin, psyllium, yogurt, slippery elm, paraffin wax, prokinetics and olive oil.
Owner and cat behaviors reported and observed are listed in Tables 3 and 4. These tables include descriptive information on owner awareness of litter box habits and habits associated with voiding. Distribution of defecation location around the house (P <0.01), defecation outside the litter box (P = 0.05), straining during defecation/urination (P <0.001), vocalization during defecation/urina-tion (P <0.001) and vomiting during/after defecation/urination (P <0.001) were significantly different between apparently healthy cats and CKD cats. When cats with a history of constipation were removed from the analysis, straining during defecation/urination (P <0.0001), vocalization during defecation/urination (P <0.01) and vomiting during/after defecation/urination (P <0.0001) remained significantly different between apparently healthy cats and CKD cats. There were no differences in frequencies of owner-witnessed defecation, owner-witnessed urinations, covering BMs by cats or peri-voiding behaviors between apparently healthy cats and CKD cats. There were no significant differences in owner awareness of urinations and defecations or cat behaviors between CKD cats with creatinine reported and CKD cats without creatinine reported.
Owner awareness information: descriptive data pertaining to the owner’s environmental awareness and observation of voiding behaviors

In all columns, data are reported based on responses obtained from the initial screening survey. Data are categorized by group: apparently healthy cats and chronic kidney disease (CKD) cats
Note: not all respondents answered all questions and therefore the column numbers may not total to the entire sum of respondents for each column
Voiding behavior information: descriptive data pertaining to the cat’s peri-voiding behaviors

In all columns, data are reported based on responses obtained from the initial screening survey. Data are categorized by group: apparently healthy cats and chronic kidney disease (CKD) cats. Statistically significant differences in the distribution of responses between healthy cats and CKD cats are denoted with an asterisk
Note: Not all respondents answered all questions and therefore the column numbers may not total to the entire sum of respondents for each column
Descriptive statistics on the predicted and observed defecation frequencies, fecal scores and urination frequencies are reported in Table 5. Eighty-five percent of apparently healthy cats were observed to defecate one or more times per day and 15% defecated less than once per day. Fifty-eight percent of CKD cats defecated one or more times per day and 42% defecated less than once per day (Figure 1). A significantly higher percentage of CKD cats defecated less than once per day in comparison with apparently healthy cats (P <0.0001). Observed BM frequency was significantl less in CKD cats compared with healthy cats (P = 0.02, Figure 2).
Voiding and fecal score statistics: descriptive data pertaining to the cat’s predicted and observed bowel movement (BM) frequency, fecal score (FS) and urination frequency

In all columns, predicted data are reported based on responses obtained from the initial screening survey. Observed data has been reported based on the multiple points of follow-up for the variable of interest. Data are categorized by group: apparently healthy cats and chronic kidney disease (CKD) cats. Data are reported as mean ± SD or median (range) based on the data distribution
Note: not all respondents answered all questions and therefore the column numbers may not total to the entire sum of respondents for each column

Eighty-five percent of apparently healthy cats were observed to defecate one or more times per day and 15% defecated less than once per day. Fifty-eight percent of cats wtih chronic kidney disease (CKD) defecated one or more times per day and 42% defecated less than once per day. A significantly higher percentage of CKD cats defecated less than once per day in comparison with apparently healthy cats (P <0.0001)

Observed bowel movement (BM) frequency per day was significantly less in cats with chronic kidney disease (CKD) compared with apparently healthy cats (P = 0.02). Data are shown as mean and standard deviation
CKD cats with a reported history of constipation had significantly lower BM frequency than CKD cats without a history of constipation (P = 0.03). When CKD cats with a history of constipation were removed from the analysis comparing CKD cats and healthy cats, there was no difference between BM frequency in apparently healthy cats and CKD cats. Seventy-five percent of CKD cats without a history of constipation defecated one or more times per day and 25% defecated less than once per day. There were no significantly differences in proportions of CKD cats that defecated less than once per day in comparison with apparently healthy cats.
Owner predicted BM frequency was significantly different than observed BM frequency in healthy cats (P = 0.04), but not in CKD cats. Owner predicted fecal scores were significantly different than observed fecal scores in healthy cats (P = 0.01), but not in CKD cats. Observed fecal scores were not significantly different between healthy and CKD cats. Owner predicted urination frequency was significantly different than observed urination frequency in healthy cats (P <0.001), but not in CKD cats. Observed urination frequency was significantly higher in CKD cats compared with healthy cats (P <0.0001). There were no differences in predicted BM frequency, observed BM frequency predicted fecal score, observed fecal score, predicted urination frequency, or observed urination frequency between CKD cats with creatinine reported and CKD cats without creatinine reported. When BM frequency and fecal score were analyzed across age groups in both apparently healthy cats and CKD cats (Table 6), there was no significant difference in either parameter by age group in either apparently healthy cats or CKD cats.
Voiding statistics based on age: descriptive data pertaining to the cat’s observed bowel movement frequency and fecal score separated within group by age

Data are reported as mean ± SD or median (range) based on the data distribution
Additional background information was obtained from respondents with CKD cats participating in the survey pertaining to appetite, drinking habits and vomiting. Owners of CKD cats reported their cats drank constantly (3, 7.0%), more than normal (20, 46.5%), about the same as normal (14, 32.5%) or less than normal (6, 14.0%). Defecation frequency in cats that were reported to drink less than normal was 0.89 ± 0.35 BM/day. There were no differences in average BM frequency between cats who were reported to drink less than normal, normal amounts, more than normal amounts or constantly by the owners. Owners of CKD cats reported that their cats vomited every other day (1, 2.3%), 1–2 times per week (9, 20.9%), 1–2 times per month (18, 41.9%), very infrequently (12, 27.9%), or never (3, 7.0%). There were no differences in average BM frequency based on frequency of vomiting. Owners of CKD cats reported their cats’ appetite was normal (6, 14.0%), decreased (32, 74.4%) or increased (5, 11.6%)). There were no differences in average BM frequency based on appetite.
Fifteen (34.9%) CKD cats were reported to have been hospitalized at some point previously, where they received intravenous fluids. Seventeen (39.5%) CKD cats regularly or intermittently received subcutaneous fluids at home. There was no difference in defecation frequency between CKD cats receiving subcutaneous fluids and those that did not. Additional medication reported in the CKD group included: amlodipine (9, 20.9%), cerenia (7, 16.3%), oral corticosteroids (6, 14.0%), cobalamin (5, 11.6%), phosphate binders (4, 9.3%), methimazole (4, 9.3%), telmisartan (4, 9.3%), oral potassium supplementation (4, 9.3%), gabapentin (3, 7.0%), famotidine (3, 7.0%), cyprohepatidine (3, 7.0%), mirtazapine (3, 7.0%) and cetirizine (2, 4.7%). The following medications were reported to be used in a single cat in the CKD group: non-steroidal anti-inflammatory drug, atopica, iron dextran, furosemide, pimobendan, benazepril and buprenorphine.
Discussion
This study identified significant differences in voiding habits between CKD cats and apparently healthy cats. Most notably, the observed BM frequency in the CKD cats with a history of constipation was less than in the apparently healthy cats and represents a clinically important variation from normal. Furthermore, the data documented an increased number of urinations in CKD cats compared with healthy counterparts, as would be expected based on the clinical signs commonly associated with CKD (polyuria/polydipsia). Recognizing abnormalities in these frequencies may assist in disease recognition, optimized patient management and improved outcomes as seen in human medicine. 7
There are many potential causes of the differences in defecation frequency observed between the CKD group and the apparently healthy group. Poor hydration status likely contributes to harder feces and hypokalemia contributes to decrease intestinal motility.1,4,8,9 Gut dysbiosis and the gut–kidney axis is an emerging area of focus in both human and veterinary medicine.7,10 Dysbiosis in kidney disease is noted early in the course of disease and has been implicated in altered metabolism of dietary components, altered metabolome, production of uremic toxins and precursors, oxidative stress, chronic inflammation, as well as changes in gut epithelium integrity.7,11 More recently, experimental models of CKD and clinical studies in uremic patients have started to link gut dysbiosis, uremic metabolites and motility to constipation.12–15 Exploration of dysbiosis in feline CKD and its functional changes is in its infancy and represents an important area for future study of disease mechanisms.
Lethargy is a commonly reported clinical sign in CKD cats. 9 Decreased physical activity in humans has been linked to constipation, and the same may be true in feline patients. 3 This study did not evaluate overall activity level, posturing ability, effects of potential osteoarthritis on mobility, or whether each cat was living a sedentary lifestyle. Human research has shown both renal disease patients as well as the elderly have decreased physical activity.16,17 As the CKD group was also significantly older in age distribution, both of these factors may have played a role in the difference in defecation frequency observed. In the sub-analyses in this study, there were no differences in defecation frequency in reference to age group in this population; however, previous studies have documented age-related changes in gastrointestinal function of older cats.18,19 The effect of these variables should be explored further in follow-up studies.
Another compounding factor in CKD cats that may result in constipation or lower defecation frequencies is the diet and medications that that animal is receiving. Many of the medications that are standard parts of geriatric patient management, including opioids, antihypertensives, phosphate binders, 5 HT3 antagonists and other medications may cause constipation.3,4,20 As nearly all cats in this study were receiving variable medications and management protocols, it was not possible to examine the impact of these factors on defecation frequency or other investigated variables. Diet, in particular dietary fiber content, and hydration also play an important role in defecation frequency and constipation. 3 Data acquired from this study were not sufficient to examine macronutrient and dietary fiber content impacts on voiding variables and no association was seen between animals receiving subcutaneous fluids and defecation frequency. Studies of CKD cats in the future should examine the effect of diet composition as well as hydration status on voiding outcomes.
The removal of cats with a history of constipation therapies or previous episodes of constipation from the analysis resulted in a lack of difference in BM frequency between apparently healthy and CKD cats. This study is unable to ascertain whether the constipation is secondary to CKD or secondary to an additional concurrent disease. Data in human medicine would support a link between constipation and CKD.4,5 However, as CKD cats often have comorbidities, it cannot be excluded that there are reasons unassociated with CKD status resulting in the BM frequency differences. Interestingly, in the cats reported to be on therapies for constipation or with a previous history of constipation, the owners did not report constipation as a clinical problem or diagnosis at the time of the survey.
There were significant differences between the predicted estimates of observed litter box habits (defecation frequency, urination frequency and fecal score) and observed litter box habits in apparently healthy cats. These differences were not identified in the CKD group. The exact cause of the lack of significant differences in the predicted estimates in the CKD group cannot be determined from this data set and represent an area for further research. However, it may be a result of the increased awareness of a cat’s general health that comes from managing a chronic illness, and owner bias. Presumably, the respondents in the CKD group were more observant of the litter box based on previously recognized changes in their cats’ behavior. In the CKD group, the majority of respondents had historical data that may have previously prompted closer observation of the litter box (constipation, diarrhea, polyuria, voiding behaviors). Regardless of the cause, considering potential daily variability in these variables and the level of accuracy that is clinically relevant, respondents in both groups were able to reasonably predict their cat’s litter box voiding habits including number of BM/day, average fecal score and number of urinations/day.
Nearly half of respondents reported that they routinely observed the majority of their cat’s defecations and over half of respondent’s report observing the majority of their cat’s urinations. These percentages are higher than were expected during the design of this study. This might be additional evidence supporting the fact the many of the respondents participating in this study are both highly invested and attentive owners regarding their cat’s voiding habits. However, as less than a fifth of participants reported observing their cat defecate or urinate either ‘rarely’ or ‘never’, similar to a previous study, additional study of the accuracy of households where voiding is observed less frequently would be an interesting area of future study. 21
A small percentage of respondents reported atypical behaviors such as straining, vocalizing and vomiting around the time of voiding. A limitation was the inability to differentiate if these signs occurred during defecation or urination. The CKD cat group was shown to have higher frequencies of these abnormal behaviors associated with litter box use. Unfortunately, it is impossible to determine whether these are individual behaviors specific to the cat for unrelated reasons, associated with another disease process or associated with their CKD diagnosis. However, the relatively high prevalence of these abnormal voiding signs should be a focus when evaluating the comprehensive health of feline CKD patients. Further study with more intensive audiovisual monitoring should be performed on cats that have been more rigorously health screened to investigate these behaviors further.
There are limitations to this survey study. The largest concern pertains to the designation of health status in this population as the animals were not evaluated in person at enrollment. As described in the ‘Materials and methods’, healthy status was assessed by a series of survey screening questions and reported health status based on veterinarian evaluation within the past year. The specific medical records of each cat were not available and as such data relied on accurate owner reporting of information. Furthermore, many respondents were from multi-cat households and this may have affected the accuracy of some results based on the owners’ ability to accurately report data in a cat-specific manner. Surveys from multi-cat households were included in the analysis as they represent a real world scenario where many cat owners have multiple cats in their home. It is unknown what the potential magnitude or direction of effect that multi-cat households have on the variables assessed. However, this limitation may have not significantly affected this population as the percentage of respondents that were either from single cat households or reported that they always witnessed their cat’s defecations was 75.8% for the healthy cats and 81.4% for the CKD cats. The cats where this limitation would potentially affect the results are a minority from each group. In addition, when comparing the main outcome variables between single cat and multi-cat households there were no differences in defecation frequency, urination frequency or fecal score.
The online format also presented limitations to the study by requiring those participating to have a familiarity with the technological platform used and be exposed to marketing of the study, which was largely distributed in electronic formats potentially biasing subsets of the overall population who participated. The online format also allowed for owners to skip answers that they did not want to provide answers to, leaving data gaps throughout certain surveys. All data presented were sorted and sub-analyzed to ensure that for each variable the analysis were performed on surveys with complete data. Lastly, based on the way data were collected, there were limitations to how the data could be analyzed or summarized. Certain variables were collected as categorical variables (eg, age of cat) to increase accuracy. The disadvantage is that this prevented analyses of some variables as continuous variables (eg, correlation of fecal score and age).
Conclusions
CKD cats exhibited decreased defecation frequency as well as increased urination frequency when compared with a population of apparently healthy cats. A majority of owners were able to provide reliable information pertaining to the frequency of BMs, fecal scores and frequency of urinations for their cat.
Supplemental Material
File 1
Feline fecal survey study questionnaire
Supplemental Material
File 2
CKD feline fecal survey study questionnaire
Supplemental Material
File 3
Prohibited medications for healthy cat group
Footnotes
Acknowledgements
The authors wish to thank the owners and veterinarians who promoted this study online.
Authors note
The results of this study were presented in part, as a poster abstract, at the American College of Veterinary Internal Medicine Annual Forum 2020. The data used in this case study can be provided on demand from the corresponding author upon request.
Supplementary material
The following files are available online:
File 1: Feline fecal survey study questionnaire.
File 2: CKD feline fecal survey study questionnaire.
File 3: Prohibited medications for healthy cat group.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Buttons Fund For Chronic Kidney Disease Research.
Ethical approval
This study did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This study did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.