
Abstract
Objectives
Lymphoma is the most common feline hematopoietic malignancy. Incidence of renal lymphoma has not been reported as a subset of a large population of feline lymphoma cases. Previous studies have reported renal lymphoma as both a singular entity as well as a component of multicentric disease. The clinical presentation, diagnostic evaluation, therapy and outcomes related to renal lymphoma have not been reported since Mooney et al in 1987. This retrospective study aimed to describe the incidence of renal lymphoma, clinical signs, treatment and survival.
Methods
Using a database of cats diagnosed with lymphoma between January 2008 and October 2017, cats with renal lymphoma were selected for further analysis. Cases were retrospectively staged according to Mooney et al (1987) and Gabor et al (1998). Data collected included age, clinical signs, clinicopathologic data, diagnostic imaging findings, lymphoma diagnostic method(s), treatment protocol(s) and survival time. Analyses comparing median survival based on therapy administered, renal lymphoma vs multicentric lymphoma, central nervous system involvement, presence of azotemia, anemia and International Renal Interest Society (IRIS) stage at diagnosis were performed.
Results
From a population of 740 cats with lymphoma, 27 cats had renal lymphoma (incidence, 3.6%), and 14 of those cats had multicentric lymphoma. Fewer stage IV and V cases were identified in this data set compared with Mooney et al; however, not all cats were completely staged. Median survival (range) for cats receiving corticosteroids alone compared with those receiving an L-CHOP (L-asparaginase, vincristine, cyclophosphamide, doxorubicin, prednisolone)-based protocol was 50 days (20–1027 days) in the corticosteroid group and 203 days (44–2364 days) for the L-CHOP group (P = 0.753) for cats that died secondary to lymphoma.
Conclusions and relevance
Neither clinical stage nor other factors were predictive of survival. Prospective studies are required to determine the optimal chemotherapy protocol.
Introduction
Lymphoma is the most common hematopoietic malignancy in cats and is the most common neoplasm reported in the kidney of cats. 1 The incidence of renal lymphoma has been reported to range from 7–30% in studies of approximately 100 cats each.2–5 The clinical presentation, results of a diagnostic work-up, therapy and outcomes related specifically to renal lymphoma have not been reported since Mooney et al in 1987. 1 Since that time, advances in diagnostics, such as the widespread use of abdominal ultrasound, have improved the ability to detect changes concerning for neoplastic infiltration and may have resulted in stage migration in feline lymphoma, as has been reported in canine multicentric lymphoma. 6
The goals of this study were to retrospectively apply two staging systems for renal lymphoma in cats to this population of cats and to describe the incidence, clinical signs, treatment and outcomes in cats with renal lymphoma. The secondary aim was to evaluate prognostic factors in renal lymphoma including International Renal Interest Society (IRIS) stage, presence of azotemia and anemia at diagnosis and evidence of multicentric disease at diagnosis.
Our primary hypothesis was that renal lymphoma occurs both as a singular entity within the kidneys and also as a component of multicentric disease. Our secondary hypothesis was that the presence of azotemia or anemia, diagnosis of multicentric disease, stage of disease and type of treatment pursued would significantly impact survival. The authors also hypothesized that the decrease in the prevalence of feline leukemia virus (FeLV)-positive cats since 1987 would have an impact on response to therapy and survival.
Materials and methods
The pathology database of the Animal Medical Center (AMC) was searched from January 2008 to October 2017 for cats with a lymphoma diagnosis obtained via cytology or histopathology. Renal lymphoma was defined as large cell lymphoma in the kidney(s) diagnosed via cytology by a board-certified pathologist. Multicentric disease was defined as large cell lymphoma in the kidney(s) and other organs diagnosed via cytology by a board-certified pathologist. Cats diagnosed with large granular lymphocyte lymphoma were included in the large cell lymphoma group. Medical records of cats diagnosed with renal lymphoma were reviewed. Data collected included age, clinical signs, clinicopathologic abnormalities, diagnostic imaging abnormalities, diagnostic method(s), treatment protocol(s) and survival time.
Prognostic factors for survival (when available), including IRIS stage, presence of azotemia or anemia at diagnosis and evidence of multicentric disease, were evaluated. Anemia was defined as a hematocrit below 28.2% at diagnosis. Azotemia was defined as a blood urea nitrogen (BUN) greater than 27 mg/dl or a creatinine greater than 1.6 mg/dl. The designated value for anemia was selected due to this being the lower end of the reference interval for IDEXX reference laboratories, which provided laboratory testing in these patients. The high end of the reference interval for BUN and creatinine are 27 mg/dl and 1.6 mg/dl, respectively. IRIS guidelines for creatinine were used to categorize cats by IRIS stage.
Cases were retrospectively staged according to Mooney et al 1 and Gabor et al. 2 The AMC staging system is outlined in Table 1. The Gabor staging system is outlined in Table 2.
Animal Medical Center staging system 1

Gabor staging system 2

GI = gastrointestinal; CNS = central nervous system
Screening for comorbidities was based on availability of clinical pathologic data, thoracic radiographs and abdominal ultrasound. Chemotherapy toxicity was retrospectively graded according to the Veterinary Co-operative Oncology Group’s Common Terminology Criteria for Adverse Events (VCOG-CTCAE). 7
Statistical methods
Baseline descriptive statistics are reported as mean and standard deviation for normally distributed variables and median and interquartile range for non-normally distributed variables. The distribution of error residuals derived from general linear models were assessed by visual inspection followed by the Kolmogorov–Smirnoff test. Between-groups analyses of baseline variables were performed using analysis of variance, as error residuals were normally distributed. Analyses for proportions of categorical variables were evaluated with a χ2 test or Fisher’s exact analysis as appropriate. Date of study entry was the time from date of diagnosis with renal lymphoma while end date was date of death. Time-to-event analyses were carried out in univariate by way of Kaplan–Meier product limit estimates. Statistical differences between Kaplan–Meier product limit estimates strata were determined by a log-rank test. Time-to-event survival time analyses represented time from study entry to end date. Cases lost to follow-up, dead from causes other than lymphoma or remaining alive were right censored. Analyses were performed with statistical software (SAS 9.3, Cary NC 2016) where P <0.05 was deemed significant.
Event-free survival was defined as the time interval from the date of diagnosis with renal lymphoma to the date of death. Patients with an unavailable date of death were considered lost to follow-up at date of last contact and censored.
Results
Review of the AMC pathology databases identified 740 cats with a diagnosis of lymphoma based on histology or cytology interpreted by a board-certified pathologist. Of these cases, 121 cats had a diagnosis of large cell lymphoma confirmed by cytology. Twenty-seven of 121 cats diagnosed with large cell lymphoma were found to have renal lymphoma based on renal aspiration cytology, making the incidence of renal lymphoma in this population 3.6% of all cats with lymphoma and 22.3% of cats with large cell lymphoma. Thirteen cats were found to have renal lymphoma only and 14 cats were found to have multicentric lymphoma. One cat had evidence of central nervous system (CNS) involvement, which was confirmed with MRI and cytology of the cerebrospinal fluid. One cat with renal lymphoma and sternal lymphadenopathy and a diagnosis of large granular lymphocyte lymphoma was included in the large cell lymphoma group because of similar outcomes between large cell lymphoma and large granular lymphoma.8–10 Figure 1 is a photomicrograph of a fine-needle aspiration cytology sample from a feline patient with renal lymphoma. Figure 2 illustrates case selection.

Fine-needle aspiration cytology of renal lymphoma in a cat. In addition to the monomorphic population of large lymphocytes, a renal tubule can be seen on the lower left of the image and a glomerulus in the upper right. Magnification × 20. Wright-Giemsa. Courtesy of Dr Michael Wiseman, IDEXX Laboratories

Feline lymphoma diagnoses from the Animal Medical Center between January 2008 and October 2017
The mean age of the cats included was 7.67 years (range, 1–18 years; median 11 years). Seventeen were castrated males and 10 were spayed females. There were 24 domestic shorthair cats, two domestic longhair cats and two Maine Coon cats. The most commonly reported clinical sign at presentation was anorexia (9/27 cats). Other clinical signs included weight loss, polyuria, polydipsia, pollakiuria, lethargy, hyporexia, dyspnea and hematuria.
Pre-treatment hematology results were available for 26 cats and biochemical profile results were available for 27 cats. The most common hematologic abnormality was anemia (17/26 cats). Other hematologic abnormalities included thrombocytopenia, leukocytosis, neutrophilia, monocytosis and lymphopenia. Serum biochemical abnormalities included azotemia (17/26 cats), hypoalbuminemia (5/26 cats), hypercalcemia (1/26 cats) and elevated alkaline phosphatase (1/26 cats). Pre-treatment BUN was available in all 27 cats and creatinine was available in 16 cats. Thirteen cats had elevated BUN and/or creatinine. Pre-treatment urine specific gravity was available in 11 cats. All 11 cats were diagnosed with renal azotemia. Two cats were categorized as stage 1, three cats as stage 2, two cats as stage 3 and four cats as stage 4 according to IRIS. Retroviral testing results were available for five cats. One cat was feline immunodeficiency virus (FIV) positive and FeLV negative. The remaining four cats were FIV and FeLV negative.
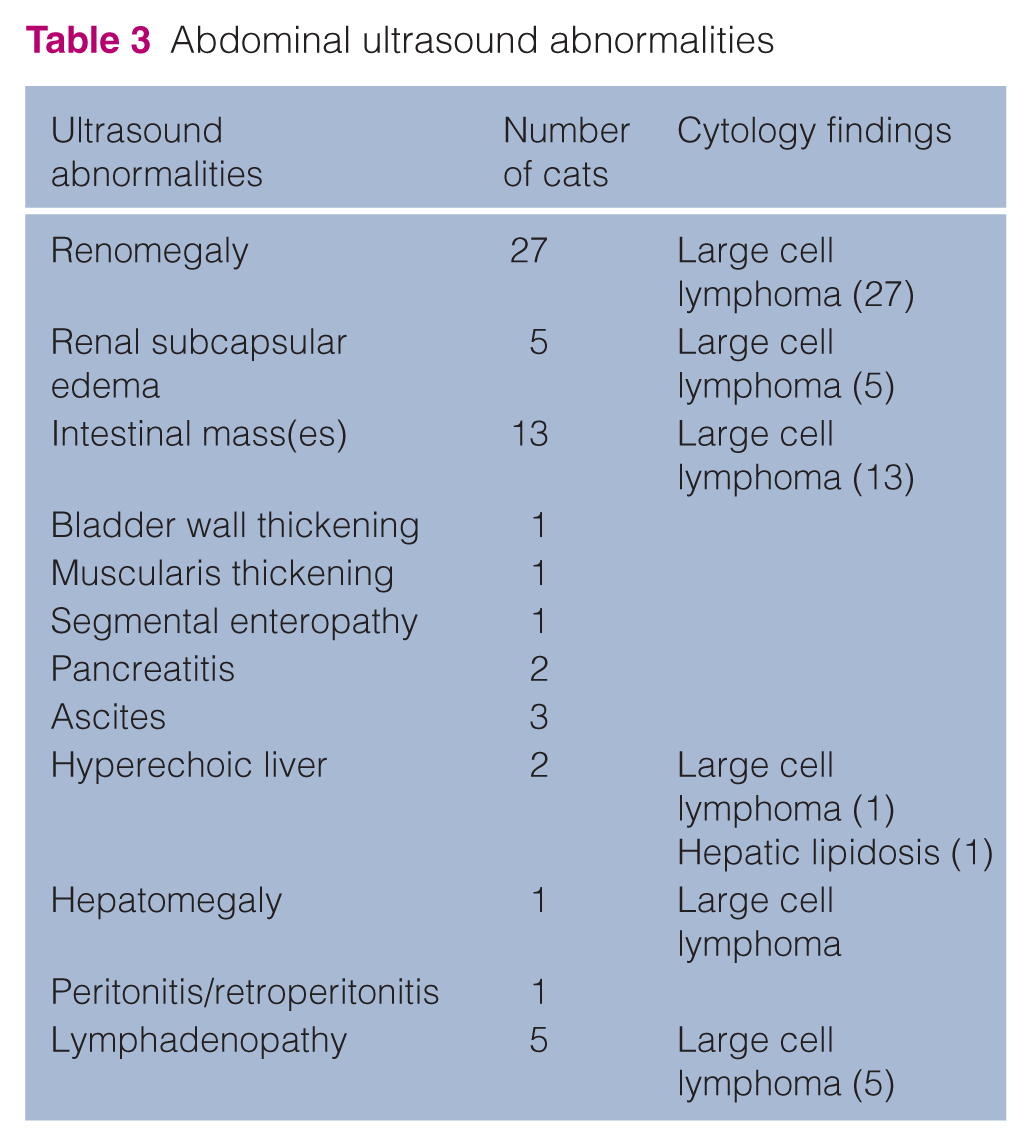
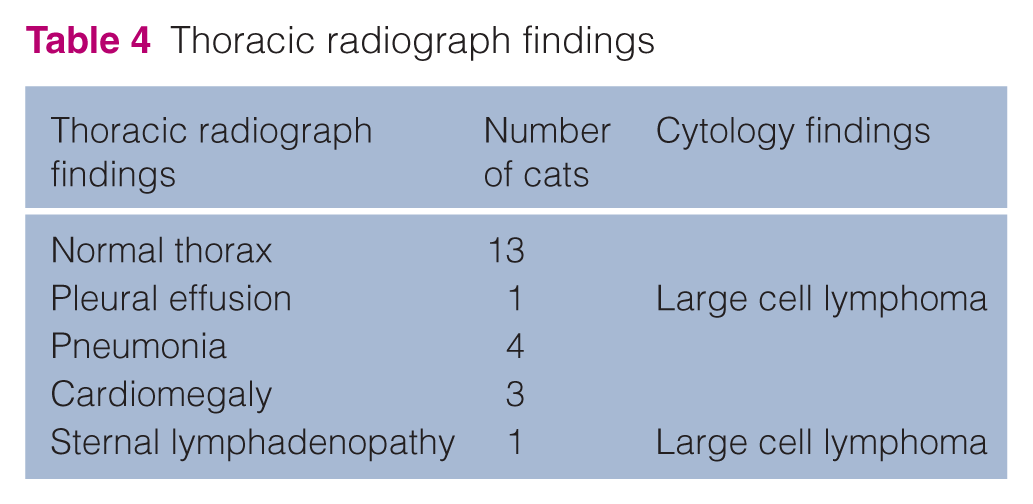
Diagnostic imaging results were available for all 27 cats. Abdominal ultrasound was performed in all cats, with the most common ultrasonographic abnormality being renomegaly (27/27 cats). Other abnormal ultrasound findings are included in Table 3. Fine-needle aspiration was performed on the liver and spleen in all cats with ultrasonographic abnormalities of these organs but not in cats with a normal appearance of these organs on ultrasound. Results of fine-needle aspiration cytology performed in abdominal organs are outlined below in Table 3. Thoracic radiographs were available in 19 cats. Radiographic findings are summarized in Table 4. Results of fine-needle aspiration cytology of pleural effusion and sternal lymphadenopathy are included in Table 4. Table 5 illustrates the AMC staging system from Mooney et al 1 compared with the current study.
Abdominal ultrasound abnormalities
Thoracic radiograph findings
Animal Medical Center staging system results from Mooney et al 1 compared with the current study

No abdominal ultrasounds performed
19/27 thoracic radiographs performed
8/28 cats underwent bone marrow aspiration
1/27 cats underwent MRI/cerebrospinal fluid tap; no cats underwent bone marrow aspiration
Each patient was staged according to clinical findings using the previously described staging systems.1,2 Twenty-four cats were placed in the abdominal stage and three in the mixed stage based on the Gabor staging system. Table 5 compares the staging of cats in the present study and the prior study using the AMC staging system.
Twenty-four cats underwent treatment for lymphoma. Fifteen cats were treated with chemotherapy. All cats treated with chemotherapy received steroids orally for the duration of their chemotherapy protocol. The most common chemotherapy protocol was a combination of L–CHOP, which was administered to nine cats. The L-CHOP protocol utilized is outlined below in Table 6. The cat with large granular lymphocyte lymphoma received cytosine arabinoside as a single agent. Five cats received chemotherapy but had an unknown treatment protocol owing to incomplete medical records. Nine cats were treated with corticosteroids alone. Radiation therapy was administered to the brain of the stage V cat with CNS involvement in addition to L-CHOP chemotherapy.
L-CHOP chemotherapy protocol

Corticosteroids administered at 1–2 mg/kg daily according to clinician preference
Three cats received rescue protocols after treatment failure with an L-CHOP chemotherapy protocol. Rescue protocols included a MOPP (mechlorethamine, vincristine, procarbazine, prednisolone) protocol and single-agent lomustine. Radiation therapy was administered to the brain and spinal cord of one cat diagnosed with CNS lymphoma at relapse. Survival was known in nine cats treated with corticosteroids alone and nine cats treated with an L-CHOP chemotherapy protocol. The median survival in cats treated with an L-CHOP-based chemotherapy protocol was 203 days, which was not statistically significant when compared with cats treated with corticosteroids alone (median survival 42 days, P value = 0.0753). Figure 3 compares survival of cats treated with L-CHOP and cats treated with steroids.

Survival of cats treated with L-CHOP (blue line) compared with cats treated with corticosteroids alone (red line)
Weeks 1–4 were repeated four times, initially at a 7-day interval with a 1-week break after the first two cycles, then the treatment interval was extended to 14 days for the final two cycles.
Adequate medical records for grading chemotherapy toxicity were available in 10/27 patients. Chemotherapy toxicity was typically mild with the most common effect being loose stool. Vincristine administration was associated with the most adverse effects including grade 1 vomiting in one cat, grade 1 diarrhea in three cats and grade 2 lethargy in two cats. One cat developed grade 3 lethargy following mechlorethamine administration. No other grade 3 or 4 toxicities were reported. Gastrointestinal signs were commonly mild and managed at home with supportive medications (maropitant [Cerenia; Zoetis], ondansetron, metronidazole).
Cats with renal lymphoma as a singular entity within the kidneys had a median survival of 50 days. The difference between the two groups was not statistically significant (P = 0.8428). Azotemia at diagnosis was not found to have a significant impact on survival (median 75 days in azotemic cats, 47 days in non-azotemic cats, P = 0.4100). Anemia at diagnosis also had no significant impact on survival (median 44 days in anemic cats, 86 days in non-anemic cats, P = 0.1735). Cats with stage II disease had a median survival of 97 days and cats with stage III disease had a median survival of 45 days, which was not statistically different (P = 0.6595). A median survival could not be calculated for the cats in the remaining stages due to low case numbers. Cats within the abdominal stage had a median survival of 50 days and cats in the mixed stage had a median survival of 114.5 days, which was not statistically significant (P = 0.9586).
The primary cause of death in 22 of the 27 cats was lymphoma. Four cats died of causes other than lymphoma. The first cat died of a second malignancy, oral squamous cell carcinoma, 2639 days post diagnosis. This cat was treated with an L-CHOP chemotherapy protocol. The second cat was euthanized secondary to neurologic disease with no evidence of recurrent lymphoma based on complete blood count (CBC), biochemical profile, thoracic radiographs, abdominal ultrasound and MRI 2363 days post diagnosis. This cat was treated with an L-CHOP chemotherapy protocol. The third cat was euthanized for an unknown cause but had no evidence of lymphoma on physical examination, CBC, biochemical profile, thoracic radiographs, or abdominal ultrasound 1026 days post-diagnosis after treatment with steroids alone. The fourth cat had a complete necropsy performed by a board-certified pathologist, which revealed no evidence of recurrent lymphoma on histopathology examination 666 days post-diagnosis. This cat received an L-CHOP chemotherapy protocol as well as rescue protocols including radiation therapy to the brain and spinal cord, a MOPP chemotherapy protocol and single-agent cytarabine arabinoside. One cat was lost to follow-up and censored from survival data 1 day post-diagnosis.
Discussion
This study reports an incidence of renal lymphoma of 3.6% in a population of 740 cats diagnosed with lymphoma and a 22.3% incidence in a population of 121 cats with large cell lymphoma. Others reported a similar renal lymphoma incidence of 2.2–3.9%.11,12 However, renal large cell lymphoma was reported to have an incidence of 15%, which is lower than reported here. 5 The current data set appears to identify an increase in the incidence of renal lymphoma in the AMC feline population over the past three decades. 5
Stage has had variable impact on survival and response to therapy in the literature on feline lymphoma.1,4,13 Neither staging system evaluated predicted outcome in this group of cats, potentially owing to the small number of cases or lack of complete staging in the cats included in this and previous studies; however, the authors also believe there are likely inherent problems with the two staging systems. Tumor staging serves the purpose of identifying patients with increasing tumor burden and determining prognosis from that information. The Gabor staging system provides an anatomic description of tumor location, which would not be expected to correlate with tumor burden. 2 The AMC staging system attempts to define increasing tumor burden with increasing stage by having higher stages correlate with disease identified in an increasing number of anatomic sites. 1 Despite the cats included in this study not receiving full staging, the authors feel that the staging that was performed is reflective of the typical clinical staging performed in cats with lymphoma. The cats included in the Mooney et al 1 manuscript had no abdominal ultrasounds performed and only eight of 28 cats had bone marrow aspirates performed. The cats included in Gabor et al 2 only had thoracic radiographs performed if dyspneic or if the heart was in an abnormal location based on physical examination findings. Abdominal ultrasound was also not performed in all cats in Gabor et al. 2
Since the routine use of abdominal ultrasound became commonplace at the AMC after 1984, we hypothesized that the three decades between Mooney et al 1 and this data set would result in stage migration. Stage migration is defined as the addition of newer and more sensitive staging tests, which can identify previously undetectable lesions resulting in ‘migration’ into higher stages. 6 Stage migration has been documented in humans, dogs and cats.6,14–16 Our data showed that there were fewer stage IV and stage V cases, an increased number of stage III cases and similar numbers of stage I and II according to the AMC staging system, although no bone marrow aspiration cytology was performed in any cats in this study, which may have resulted in underestimation of stage. Our data suggests, but cannot confirm, the presence of reverse stage migration. Reverse stage migration has been previously documented in men with prostate cancer after the implementation of prostate-specific antigen testing. 17 Our hypothesis to explain the potential reverse stage migration observed in our patient population is that routine use of advanced diagnostics with greater sensitivity provides a more accurate assessment of internal organs than palpation and less sensitive imaging techniques such as radiography, which was used previously. 1 However, since neither the current data set nor the data sets in Mooney et al 1 or Gabor et al 2 had complete staging data on all cats, reverse stage migration in feline renal lymphoma remains speculative.
Clinical staging of feline cancer patients is inherently imprecise because samples are not typically collected from normal-appearing tissues that might harbor lymphoma. In many studies, costs associated with testing, risks of adverse outcomes from testing and the fact that complete staging is not required for successful treatment limit the number of cats undergoing an extensive staging evaluation. It is likely that nearly all reports of clinical staging of feline lymphoma patients over- or underestimate stage to some degree.
The authors acknowledge that this study may underestimate stage because 19/27 cats had thoracic radiographs and no cats underwent bone marrow aspiration. In the previous study, only 8/28 cats underwent bone marrow aspiration, and no abdominal ultrasounds or MRIs were performed. Stage may have been over- and underestimated in that group of cats. 1 However, given that similar limitations exist in all publications reporting feline lymphoma stage, there may still be value in comparing staging in different studies even though none of those studies are perfect.
The presence of azotemia and anemia at diagnosis is considered of potential prognostic significance in renal lymphoma. Based on Boyd et al, 18 we hypothesized severe azotemia would result in poorer responses to chemotherapy and shorter survival times. Previously, in cats with chronic kidney disease, IRIS stage at diagnosis has been shown to predict outcome. 18 Boyd et al 18 also reported a short median survival time in patients with chronic kidney disease and anemia requiring treatment. Our study did not identify azotemia or anemia as prognostic factors for survival, but anemia is one difference that might have influenced survival between the cats previously reported and these cats. In this study, a greater number of cats (17/27) were anemic compared with Mooney et al, 1 where 14/28 cats were anemic. In at least one study of canine lymphoma, anemia was a predictor of survival. 19 Dogs diagnosed with anemia and lymphoma had a median hematocrit 10% lower than dogs with lymphoma without anemia. Both remission duration and survival were shorter in dogs with anemia compared with dogs without anemia. This study may have been too small to identify anemia as a prognostic factor for survival but the subject warrants further investigation.
The decrease in FeLV infections and the decrease in its role in lymphomagenesis has made FeLV infection uncommon in cats with lymphoma. 20 FeLV infection is uncommon in our patient population and thus testing is no longer routine, as evidenced by the small number of cats tested. Because the cats in this study likely had a low prevalence of FeLV infection, we hypothesized the survival would be longer in these cats compared with Mooney et al 1 since FeLV infection has been shown to confer a shorter median survival time. 4 The median survival time of cats in Mooney et al 1 is difficult to determine but 17/28 cats had a complete response with a reported median survival of 169 days, which does not appear to differ from the median survival reported in this study. This finding was unexpected.
Lymphoma of the CNS appears to be less common in this study than in Mooney et al. 1 We speculate the decrease in CNS lymphoma may be related to a decrease in FeLV infection. 1 The median survival in the present study is comparable to Mooney et al 1 , yet only one cat developed CNS lymphoma during treatment compared with eight cats in the previous report. The low number of cases with CNS involvement in this case series calls into question the recommendation to include cytosine arabinoside in the treatment protocol for renal lymphoma as previously described. 1 Cytosine arabinoside has been recommended as prophylaxis for CNS lymphoma due to its ability to cross the blood–brain barrier and cats treated with a protocol containing this chemotherapy agent were reported to have a lower rate of CNS lymphoma than cats not treated with cytosine arabinoside. 1 Prospective studies are indicated to determine the optimal chemotherapy protocol for renal lymphoma in cats and if CNS prophylaxis with cytosine arabinoside or any drug is indicated.
Another difference between this study and the prior one is the use of L-CHOP chemotherapy in nine cats. The chemotherapy protocol used previously to treat renal lymphoma did not include doxorubicin. 1 Doxorubicin was added to the chemotherapy protocol used in some cats in this study with the expectation that the addition of this drug would improve survival, though statistical analysis did not confirm this outcome. Prior reports of the efficacy of doxorubicin in feline lymphoma have been mixed. Some studies report long survival times using protocols without doxorubicin, some report no difference in survival times between protocols with and without doxorubicin and single-agent doxorubicin chemotherapy has not been as successful in the cat as in the dog.1,3,9,10,21–28 Three of the four long-term survivors (and cats potentially ‘cured’ of renal lymphoma) were initially treated with the L-CHOP protocol, suggesting the addition of doxorubicin to the treatment protocol of some cats with renal lymphoma is beneficial. The infrequent occurrence of renal lymphoma in this population of over 700 cats results in a small number of cases, causing a challenge in detecting differences between groups. Thus, we cannot conclusively say the addition of doxorubicin is not of benefit in at least some cats with renal lymphoma. Cats included within the current study treated with an L-CHOP protocol had a treatment duration of 25 weeks, unless there was evidence of progressive disease requiring a change in protocol prior to that time. Cats included in Mooney et al 1 were treated with chemotherapy for several years. Considering the median survival time in Mooney et al 1 was not longer when compared with the current data set, prolonged maintenance chemotherapy treatment may not have clinical benefit. The efficacy of prolonged maintenance chemotherapy has been questioned in canine lymphoma. 29 An interesting and unexplainable finding regarding survival time observed in both this study and Mooney et al 1 is the report of a few cats with very long survival times. In Mooney et al, 1 at least three cats survived >1 year and in the present study, four cats survived >1 year. The prolonged survival in the four cats ‘cured’ of renal lymphoma in the present study suggests prolonged maintenance chemotherapy is not required in at least a subset of cats with renal lymphoma.
In Australian 2 and Dutch cats, 28 a predilection for lymphoma in young, purebred cats, specifically Oriental breeds, has been reported. Young Siamese cats treated for lymphoma may have a prolonged disease-free interval. 10 The inclusion of two Abyssinian cats, a Siamese and a Burmese cat may have had an impact on survival in the prior study and explain in part why the cats in the present study, which included no young, Oriental cats, have a similar survival time to Mooney et al, despite there being fewer FeLV-positive cats in this study. 1 The two purebred cats in this study were both older, 13 and 17 years of age.
Conclusions
This study reports an incidence of 3.6% for renal lymphoma in a population of 740 cats diagnosed with lymphoma and a 22.3% incidence in 121 cats with large cell lymphoma. The survival time in this group of cats was unexpectedly and disappointingly short, although some cats appeared to be ‘cured’. The cause of the short survival time is elusive. The cats’ FeLV status, chemotherapy protocol and known prognostic factors do not appear to explain the outcome in this group of cats. This study suggests CNS prophylaxis may not be necessary in cats with renal lymphoma as has previously been suggested. Prospective studies are required to determine the optimal chemotherapy protocol for cats with renal lymphoma.
Footnotes
Acknowledgements
The authors thank Drs KZ Wright and AM Verrilli and Ms S Vaughan-Wasser for use of their feline lymphoma database.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.