
Abstract
Practical relevance:
Feline triaditis describes concurrent pancreatitis, cholangitis and inflammatory bowel disease (IBD). The reported prevalence is 17–39% in ill referral patients. While the aetiology is poorly understood, it is known to include infectious, autoimmune and physical components. What is not known is whether different organs are affected by different diseases, or the same process; indeed, triaditis may be part of a multiorgan inflammatory disease. Feline gastrointestinal tract anatomy plays its role too. Specifically, the short small intestine, high bacterial load and anatomic feature whereby the pancreatic duct joins the common bile duct before entering the duodenal papilla all increase the risk of bacterial reflux and parenchymal inflammation. Inflammation may also be a sequela of bowel bacterial translocation and systemic bacteraemia.
Diagnostic challenges:
Cholangitis, pancreatitis and IBD manifest with overlapping, vague and non-specific clinical signs. Cholangitis may be accompanied by increased serum liver enzymes, total bilirubin and bile acid concentrations, and variable ultrasonographic changes. A presumptive diagnosis of pancreatitis is based on increased serum pancreatic lipase immunoreactivity or feline pancreas-specific lipase, and/or abnormal pancreatic changes on ultrasonography, though these tests have low sensitivity. Diagnosis of IBD is challenging without histopathology; ultrasound findings vary from normal to mucosal thickening or loss of layering. Triaditis may cause decreased serum folate or cobalamin (B12) concentrations due to intestinal disease and/or pancreatitis. Triaditis can only be confirmed with histopathology; hence, it remains a presumptive diagnosis in most cases.
Evidence base:
The literature on feline triaditis, pancreatitis, cholangitis and IBD is reviewed, focusing on histopathology, clinical significance and diagnostic challenges. Current management recommendations are provided. Further studies are needed to understand the complex pathophysiology, and in turn improve diagnosis and treatment.
Introduction
In human medicine, triaditis refers to inflammation of the portal triads within the liver. In contrast, triaditis in cats has widespread acceptance in the veterinary field as referring to concurrent pancreatitis, cholangitis and inflammatory bowel disease (IBD). Despite being reported relatively fre-quently,1–3robust literature regarding the true prevalence of triaditis and its aetiopathogenesis is still lacking. Case reports investigating this condition started to emerge in the mid-1990s 1 and, to date, it has been reported in 17–39% of cats in ill referral populations.1–3While no sex, age or breed predisposition has been convincingly documented, cats with concurrent acute neutrophilic cholangitis (NC) tend to be younger than those with chronic lymphocytic cholangitis (LC), 4 and Siamese cats are over-represented in some studies of pancreatitis.5,6
This article reviews the literature on feline triaditis, focusing initially on pancreatitis, cholangitis and IBD. Histopathological descriptions, relative clinical significance and difficulties inherent in making these diagnoses are discussed, and recommendations given on how best to manage these conditions individually and collectively.
Component inflammatory disorders
Pancreatitis
In most cases, pancreatitis is considered idiopathic; however, some underlying causes such as viral infection, toxoplasmosis, fluke infection, trauma and organophosphate poisoning have been reported.6–8In humans, autoimmune and genetic components have been associated with pancreatitis;9–11and the role of the microbiome is currently gaining more interest as a study area. However, none of these have been recognised in feline pancreatitis as yet.
Pancreatitis can be divided into acute and chronic inflammation on the basis of histological findings.12,13The published scoring system is based on histopathological characteristics in humans, and recognises two main forms of feline pancreatitis. 14 Acute pancreatitis (AP) is characterised by neutrophilic inflammation, with associated interstitial oedema and necrosis of mesenteric fat, while chronic pancreatitis (CP) is characterised by lymphocytic inflammation, fibrosis and acinar atrophy. 14 However, a consensus scoring system for feline pancreatitis is still lacking. Since cats with CP are more likely to have concurrent diseases (eg, hepatobiliary disease) than cats with AP, 15 CP may be more common in triadi-tis. Pancreatic inflammation can extend to the pancreatic duct and even the sphincter of Oddi (see later), going on to cause cholangitis and, potentially, extrahepatic biliary obstruction (EHBO). Cholangitis occurring as a primary disease can cause inflammation extending to the sphincter of Oddi and pancreatic duct, and so, in turn, is a risk factor for pancreatitis. 16

Cholangitis
Cholangitis describes inflammation of the biliary duct; when the inflammation extends into the hepatic parenchyma, a diagnosis of cholangiohepatitis is made. 17 Cholangitis is a common form of feline hepatic disease: in a UK study of almost 1500 feline liver biopsy samples, 18 the most common histopathological diagnoses were NC and reactive hepatitis, while LC was ranked fourth (after reversible hepatocellular injury). Hepatic lipidosis is the most common form of liver disease in the USA. 19 It is important to remember that this can occur as a primary condition or secondarily to other diseases, particularly cholangitis and pancreatitis; as such, it is often associated with triaditis. 20
The World Small Animal Veterinary Association (WSAVA) Liver Standardization Group has revised its histopathological classification of feline liver disease, and recognises three distinct forms of cholangitis in cats (Table 1): neutrophilic, lympho-cytic and chronic cholangitis associated with liver fluke infection. 17 Acute and chronic forms of NC are no longer considered as separate diseases, as is now generally accepted.

WSAVA histopathological classification of feline cholangitis

Adapted from WSAVA standards for clinical and histological diagnosis of canine and feline liver diseases 17
The most common type of cholangitis in cats is NC, which is characterised by infiltration of large numbers of neutrophils into portal areas of the liver and bile ducts. 17 It is believed to result from bacterial infection ascending from the intestine,19,21,22an assumption that is supported by the involvement of common enteric species, including Escherichia coli, Streptococcusspecies, Clostridiumspecies and Salmonella typhimurium. 23 NC can be further divided into acute and chronic forms, which are distinguished by their histopatho-logical appearance. Acute neutrophilic cholangitis (ANC) is characterised by neu-trophilic inflammation alone, while chronic neutrophilic cholangitis (CNC) is thought to be a progression of ANC, and is characterised by variable infiltrates of neutrophils, lymphocytes and plasma cells (Table 1). Fibrosis and bile duct proliferation depend on the chronic-ity of disease. 17
EHBO is often associated with NC. One study identified EHBO in 64% of cats with cholangitis, 24 with another study reporting EHBO in 76% of cats with CNC and 40% of cats with ANC. 25 Separately, in an investigation where EHBO was confirmed at surgery or necropsy in 22 cats, 15 (68%) had at least one inflammatory disease, including pancreatitis, cholangiohepatitis, cholelithiasis and chole-cystitis. 26 These inflammatory conditions, together with biliary or pancreatic neoplasia, were the most common causes of EHBO in that study. 26
LC is characterised by infiltration of lymphocytes and plasma cells confined around portal areas, with variable degrees of fibrosis and biliary hyperplasia. 27 The nature of the inflammatory infiltrate suggests an immune-mediated pathogenesis.28,29A study of 51 cases of feline LC found no strong evidence to implicate in situ bacterial colonisation as an aetiopathogenesis using standardised histo-pathology, immunophenotyping (B and T cells), PCR for T-cell receptor gene rearrangement, and fluorescence in situ hybridisation (FISH) for eubacteria. 29 LC typically has a chronic progressive clinical course, extending over months or years.28,30Affected cats may be young or old, and Persian cats have been reported to be over-represented, suggesting a possible genetic predisposition. 31
Chronic cholangitis associated with infection by liver flukes (family Opisihorchiidae) - the third distinct type of feline cholangitis - can be seen in cats from tropical environments. Cats, as the definitive host for liver flukes, acquire infection by ingestion of raw fish, and the young flukes migrate from the intestine to the liver via the bile ducts, causing thickening and cystic dilatation of the bile ducts.32,33In cats (and dogs), chronic cholangitis due to liver fluke infection has been associated with intra-hepatic and extrahepatic cholangiocellular car-cinomas. 32 Slight to moderate inflammation may be seen both within the ducts (neutrophils and macrophages) as well as in the portal areas (neutrophils, lymphocytes and plasma cells). 17 There is little to implicate chronic cholangitis as having a role to play in triaditis.
IBD
The exact cause of IBD remains unknown. However, it is believed that (as in people and dogs) the pathogenesis of IBD in cats involves the intestinal microbiome, dietary antigens, genetics and dysregulation of the intestinal immune system.34,35Both quantitative and qualitative alterations in intestinal microbiota are closely linked to the aetiopathogenesis of feline intestinal diseases, and a balanced intestinal microbiota ecosystem is crucial to ensure feline intestinal health. 36
In a study by Janeczko et al, 35 the number of mucosa-associated Enterobacteriaceae was higher in cats with signs of gastrointestinal (GI) disease than in healthy cats. The number of Enterobacteriaceae and Clostridiumspecies has been correlated with abnormalities in mucosal architecture (principally atrophy and fusion), upregulation of cytokine mRNA (particularly interleukin [IL]-1, IL-8 and IL-12), the density of cellular infiltrates, particularly macrophages and CD3+ lymphocytes, and the number of clinical signs exhibited by affected cats.30,35The composition and number of mucosa-associated bacteria correlate with the presence and severity of IBD in cats, raising the possibility that abnormal mucosal flora are involved in the pathogenesis of feline IBD and, in turn, that therapeutic intervention directed at the mucosal flora may abrogate the mucosal inflammatory response. 35
Another study found that cats with IBD had lower FISH counts on faecal samples for total bacteria, Bacteroidesspecies and Bifidobacteriumspecies, but higher counts of Desulfovibriospecies, compared with healthy cats. 29 Desulfovibriospecies are able to produce hydrogen sulphide, which may be associated with the pathogenesis of feline IBD. 36 However, in contrast, another study failed to identify significant differences in FISH counts between cats with IBD and controls, despite targeting the same bacterial groups. 37 Since cats with IBD have lower numbers of faecal Bifidobacteriumspecies compared with healthy cats, 34 bifidobacteria may be helpful in promoting an anti-inflammatory environment and decreased numbers of bifidobacteria might be harmful to cats at risk for primary GI disease. 38 While this area of research is expanding rapidly, there is still much to learn about the role of the microbiome in the patho-genesis and treatment of IBD.
Feline IBD predominantly affects middle-aged animals, although it is also seen in cats of 2 years of age or less. 39 Compared with cats with IBD or alimentary lymphoma, cats with food-responsive enteropathy tend to be younger and present with diarrhoea, while muscle wasting is infrequent. 40 Certain breeds are predisposed to IBD (eg, Siamese), but all breeds may be affected. 41
The WSAVA Gastrointestinal Standardization Group developed ‘Histopathological standards for the diagnosis of gastrointestinal inflammation in endoscopic biopsy samples from the dog and cat’ and established a grading system for the severity of GI inflammation with a simple four-point scale: normal (0), mild (1), moderate (2) or marked (3). 42 However, it is important to note that the number of intraepithelial lymphocytes (IELs) is much greater in healthy cats compared with dogs.43,44In addition, feline IELs are more frequently seen within the villus than crypt epithelium, and within the villus the number of IELs increases from the duodenum (where they number ~50% of epithelial cells) to the ileum (~80%).43,44This can lead to the over-diagnosis of IBD, as seen in a study where 42% of cats diagnosed with inflammatory lesions in their small intestine had no clinical signs suggestive of enteropa-thy. 3 More studies are needed to explore how this grading system for feline GI inflammation helps in the understanding and management of our feline patients.

Triaditis: insights on prevalence, aetiology and manifestations
Prevalence
Several studies have looked at the prevalence of triaditis (Table 2). In an early investigation, Weiss et al 1 evaluated sections of liver, intestine and pancreas from 78 cats at necropsy; 46% had lymphocytic portal hepatitis, 23% had cholangitis and 31% had no inflammatory cholangiohepatic disease. This study revealed that the prevalence of IBD (28%) and pancreatitis (14%) in cats with lymphocytic portal hepatitis was not significantly different from that of cats with no inflammatory cholangiohepatic disease. However, the researchers found that 39% of cats with cholangitis also had IBD and pancreatitis (ie, triaditis), and the prevalence of IBD and pancreatitis was greater in cats with cholangitis (83% and 50%, respectively) compared with cats with non-inflammatory hepatic disease. 1 Evidence of IBD in association with cholangitis was characterised by cholangio-hepatic infiltration of lymphocytes and plasma cells; however, neutrophilic infiltrates were also found in more than 40% of cats with concurrent IBD. Pancreatitis was histopathologi-cally mild in all cats. 1
Studies investigating the association between gastrointestinal, hepatic and pancreatic inflammatory disorders in cats

IBD = inflammatory bowel disease; AP = acute pancreatitis; CP = chronic pancreatitis; ANC = acute neutrophilic cholangitis; CNC = chronic neutrophilic cholangitis
In a study of 44 cats diagnosed with moderate to severe cholangitis at necropsy, the majority had CNC (n = 33) or ANC (n = 7); 60% also had pancreatitis, 50% also had IBD and 32% had both (ie, triaditis). 2 However, necropsy studies may overestimate the prevalence of chronic disease as, unless patients die during the acute stage of the disease, the histopathology may only show signs of chronic changes due to the ongoing disease. Also, cats are notoriously good at hiding pain and illness, so some diseases, such as pancreatitis, can be apparently subclinical. In a study of 115 cats, 45% of apparently healthy cats had evidence of pancreatic lesions on post-mortem examination, 14 which underlines the challenges of diagnosing acute disease.
A later prospective study set out to investigate the frequency of IBD, cholangitis, pancreatitis, or a combination of these conditions, in symptomatic and asymptomatic cats by comparing clinicopathological features with histopathological and laboratory findings. 3 Inflammatory changes were detected in 47 cats (27 symptomatic, 20 asymptomatic); 28% of the cats had histopathology consistent with IBD alone, 13% with cholangitis alone and 2% with pancreatitis alone. 3 However, 57% of the cats had inflammation involving more than one organ: 34% had concurrent IBD and cholangitis; 17% were diagnosed with triaditis; and 6% had IBD and pancreatitis. 3 Importantly, triaditis was identified only in symptomatic cats (20%), and a mild, positive correlation was detected between the severity (score) of IBD lesions and the number of comorbidities. 3
Aetiology
The aetiology of feline triaditis is poorly understood. The disease may occur because of an infectious or an autoimmune process, or a physical problem such as duct obstruction. It is also not certain if cats suffer from different diseases in each organ or if the disease process in each organ has the same aetiology. The anatomy of the feline GI tract may play a role: the small intestine is comparatively shorter than in the dog; 46 there is a higher concentration of bacteria in the duodenum;47–49and the pancreatic duct joins the common bile duct before entering the duodenum at the papilla (Figure 1). 46 These adaptations increase the risk of bacteria ascending from the duodenum into the liver and pancreas, resulting in parenchymal inflam mation. 50 In support of this, the bacteria isolated from the pancreas and liver of cats with pancreatitis and hepatic diseases are common enteric species, such as E coli. 51 Vomiting can cause reflux of duodenal juice into the pancreatic and/or bile duct, spreading enteric bacteria into the pancreas and biliary tree. 52
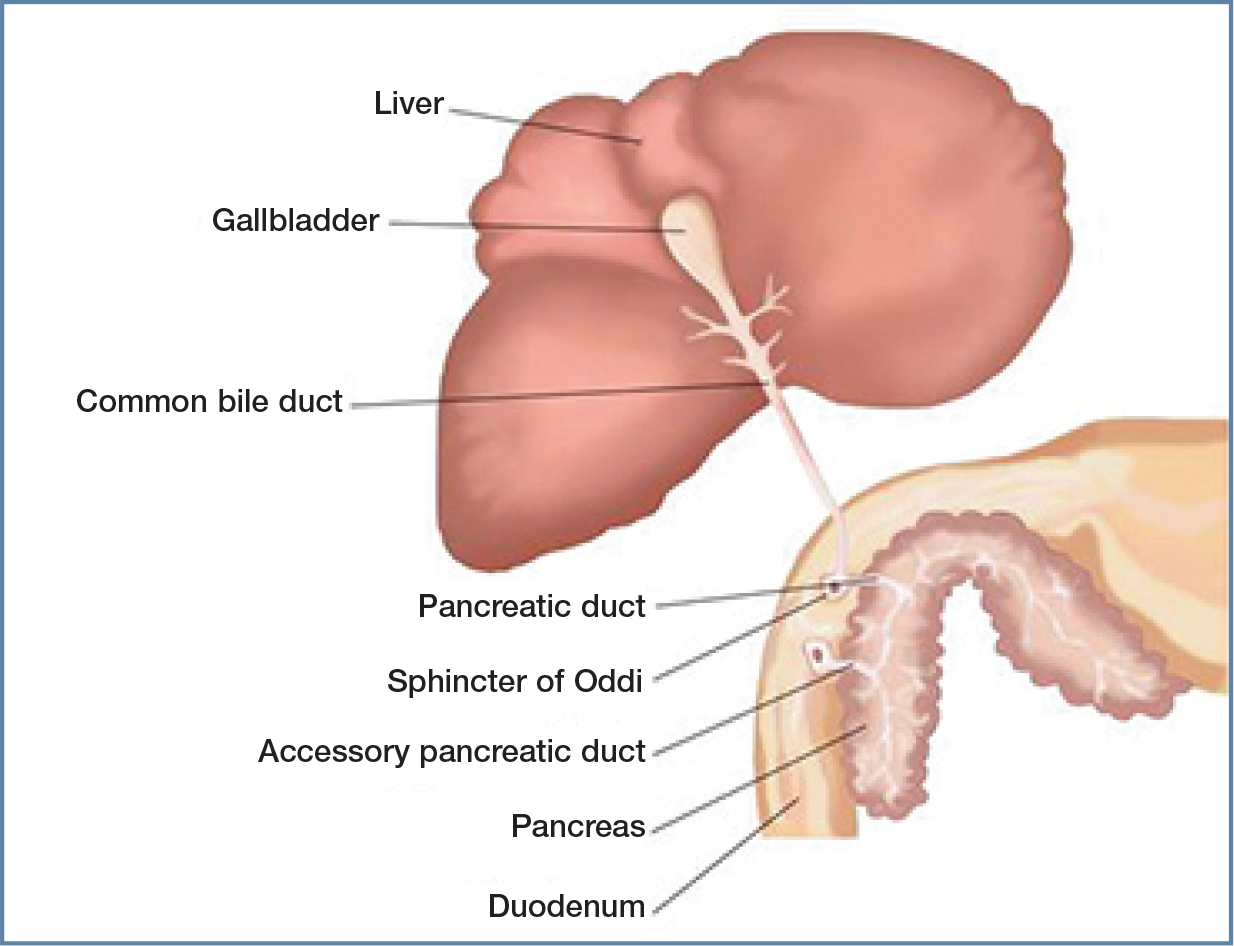
Illustration showing the close proximity and anatomical relationship between the liver, pancreas and duodenum of the cat. The pancreatic duct joins the bile duct before entering the duodenum at the papilla, which may predispose to ascending infections of both the liver and pancreas, and potentially multiorgan inflammation. Of note, the accessory pancreatic duct is present in only around 20% of cats. Courtesy of Ceva
A study of cats with AP demonstrated that bacterial colonisation of the pancreas can occur by reflux from the intestinal tract into the pancreatic duct, and also by haematoge-nous spread. 53 Additionally, bacteria may pass, by translocation, across the mucosal barrier into the portal blood circulation and then enter the liver, rather than ascending via the bile duct. A FISH study has provided supporting evidence, showing intrahepatic bacterial colonisation of venous sinuses, portal vessels and the hepatic parenchyma, rather than colonisation within the bile ducts. 54 Inflammation or infection could also spread as a local effect due to the close proximity of the pancreas, bile duct and small intestine in cats. Intestinal inflammation may promote the translocation of enteric bacteria into the liver and pancreas. 51
Obstruction to the flow of bile or pancreatic juices may also play a role in triaditis. The sphincter of Oddi is a muscular valve that controls the flow of bile and pancreatic juices and is located within the wall of the duodenum at the terminal end of the common bile duct. 55 Blockage or dysfunction of the sphincter can predispose cats to pancreatitis and cholangitis. 55 In humans, gallstones can cause a blockage of the duct near the sphincter of Oddi, but this is very rare in cats.55–57Dysfunction or spasm of the sphincter has been described in humans and cats, causing blockage of both pancreatic and bile ducts and, in turn, obstruction.55–57In humans, this is often diagnosed in association with IBD -with inflammation in the intestinal wall around the sphincter predisposing it to spasm. 58 A case series study reported six cats with obstructive processes within their sphincter of Oddi, and three of these cats had concurrent IBD. 55 Also of note, only around 20% of cats have an accessory pancreatic duct; and, when present, it is most commonly rudi-mentary. 59 Hence, when pancreatitis does occur, digestive enzymes are unable to leave the inflamed pancreas, exacerbating the activation of digestive enzymes within the acinar cells, leading to pancreatic autodigestion. 60
The pathophysiology of triaditis may also have an immune component. 51 Memory T lymphocytes that arise as a consequence of IBD have been shown to express homing receptors that lead them to migrate to the liver and pancreas. These memory lymphocytes can then be activated within these organs, producing inflammation and tissue damage. This, in turn, stimulates the recruitment of more lymphocytes and causes a persistent inflammatory state. 51 Moreover, it has been suggested that altered mucosal integrity, secondary to IBD, may lead to inflammatory mediators, endo-toxins and microbes accessing the portal circulation. This can lead to immune complex deposition within the liver, complement activation and hepatocellular necrosis.50,61Changes to intestinal permeability that can occur with IBD also allow passage of bacterial and colonic epithelial cell antigens, promoting production of autoreactive antibodies. 50
It is possible that the three organs involved in triaditis are all affected by the same process concurrently. For example, humans with primary sclerosing cholangitis commonly have concurrent IBD, which is thought to be part of the same disease process as they have the same unique disease phenotype. The pathogenesis of this comorbidity in humans is still unclear, but the disease phenotype is different when these conditions occur separately and an immune-mediated component has been suggested. 62
Clinical signs
The clinical signs associated with feline pancreatitis are vague and non-specific (Table 3). Anorexia has been reported in 63-97% of cases and lethargy in 28–100%, while weight loss, dehydration, pallor and icterus are frequently noted on physical examination.2,5,8,15In contrast to dogs, fever is less common with feline pancreatitis. In one study, only 25% of feline patients with pancreatitis presented with pyrex-ia, whereas hypothermia was noted in almost 50% of cases. 8 A study evaluating systolic blood pressure in feline patients in an intensive care unit found that pancreatitis and/or hep-atopathy were associated with systemic hypotension, and reported that a Doppler systolic blood pressure lower than 124 mmHg was a negative prognostic indicator for survival. 70
Clinical signs that can be seen in cats with triaditis

Clinical signs marked with an asterisk are common. EPI = exocrine pancreatic insufficiency

Anecdotally, the authors have seen many cases of severe triaditis develop vasculitis (Figure 2). Vasculitis markers used in people (antineutrophil cytoplasmic antibodies) are variably increased in cats with pancreatitis, but have also been seen in healthy cats, so studies are needed to understand the importance of these antibodies in cats (K Rolph, unpublished data). Also, it is difficult to distinguish between vasculitis and bruising due to other causes. Ideally, platelet number and function should be evaluated by blood smear and buccal mucosal bleeding time and clotting times (prothrombin time [PT] and activated partial thromboplastin time [APTT]) measured; where available, thromboelastography can be used to diagnose possible platelet and clotting disorders or to detect disseminated intravascular coagulation. These are life-threatening conditions and require immediate treatment. More studies, possibly involving thromboelastography, are needed to investigate the exact cause of coagulation problems in these cases to inform treatment decision-making.

Siamese cat with triaditis that developed vasculitis. Courtesy of Kerry Rolph
Most cases of mild CP remain subclinical. 14 In one study, 45% of apparently healthy cats showed evidence of pancreatic lesions on post-mortem examination. 9 Ante-mortem diagnosis can be challenging, and the reported prevalence, based on histopathological findings, ranges between 0.6% and 67%.14,71,72Pancreatitis is often seen in cats with diabetes mellitus and can be a factor that contributes to deterioration of this disease and/or leads to the development of diabetic ketoacidosis.15,73–75
Cats with NC are often young (3–5 years old) and present with an acute illness that usually lasts for about a week. 76 The clinical signs are often nonspecific (Table 3), including anorexia, lethargy, vomiting and weight loss, with icterus, dehydration, fever, hepatomegaly and abdominal pain being observed in fewer than half of all cases. 71 Cats with LC may show clinical signs of anorexia, lethargy, vomiting and weight loss. The most common physical findings include icterus (Figure 3), 3 ascites and hepatomegaly. As with NC, severe cases may develop signs of hepatic encephalopathy 77 (Figure 4) or coagu-lopathy.78,79However, hepatic encephalopathy appears to be relatively uncommon in cats with acquired liver diseases and most commonly develops with severe chronic disease and/or secondary hepatic lipidosis. Its most frequent manifestations are ptyalism (excessive salivation) and altered mentation. Acquired hypocobalaminaemic encephalopathy has also been reported, and measurement of serum cobalamin concentration in patients with encephalopathy is recommended. 80

Burmese cat diagnosed with cholangitis. Jaundice is usually seen after a five- to-10-fold increase in serum bilirubin concentration

Same cat as in Figure 3, receiving a lactulose enema for treatment of hepatic encephalopathy that developed secondarily to neutrophilic cholangitis. Lactulose therapy is considered a first-line treatment and can be administered orally and/or rectally. Note, however, that there are high risks associated with oral administration in cats with decreased mentation (eg, aspiration pneumonia), so rectal administration is preferred in these cases
In cats, IBD is a diagnosis of exclusion, and clinical signs resemble those of other chronic GI diseases (eg, alimentary tract lymphoma), including diarrhoea, vomiting, hyporexia and/or weight loss (Table 3). 81 However, clinical signs can be subtle, and many cats found to have IBD show only hyporexia.
Diagnosing triaditis
Haematology and serum biochemistry abnormalities
Haematology, serum biochemistry (including serum total thyroxine), serum feline trypsin-like immunoreactivity (fTLI) and urine analysis are all useful in excluding common systemic and metabolic disorders such as renal disease, hepatopathy, hyperthyroidism (a frequent cause of increased liver enzymes and GI signs in elderly cats), 82 exocrine pancreatic insufficiency or other diseases causing chronic intestinal signs in cats. The most common haematological and serum biochemistry findings are listed in Table 4.
Haematology and serum biochemistry abnormalities in cats with triaditis

N = normal; ↑ = increased; ↓ = decreased; ALT = alanine aminotransferase; ALP = alkaline phosphatase
Changes in haematology and serum biochemistry in feline pancreatitis are nonspecific. Regenerative or non-regenerative anaemia can be seen with AP; however, this is often masked by dehydration.8,15Leukopenia may be associated with a poorer prognosis. 8 Non-immune-mediated haemolytic anaemia may be seen, likely associated with oxidative damage. 83 Changes in serum biochemistry may reflect concurrent disease. Increased serum concentrations of alanine amino-transferase (ALT; 24–68%) and alkaline phosphatase (ALP; 50%) are commonly report-ed.5,8,15In one study, liver enzymes increased more in cats with CP than AP, possibly owing to concomitant hepatobiliary inflammation. 15 Other non-specific abnormalities include both hyperglycaemia and hypoglycaemia, as well as hypokalaemia.5,8,70Where available, ionised calcium should be measured in cats with pancreatitis, as ionised hypocalcaemia has been reported in many cats with AP (32–61% of cases) and, according to several studies, is associated with a poorer outcome.5,8,15,25
Haematology findings in cats with cholan-gitis may include neutrophilia (with or without a left shift) and serum biochemistry may reveal increased concentrations of ALT, aspar-tate aminotransferase (AST) and ALP, and mild to severe bilirubinaemia.84,85Serum bile acid concentrations may be increased if there is obstruction to bile flow. While increased liver enzymes may give information about liver damage, the bile acid stimulation test gives more information about liver function. 86 Note, however, that measuring bile acids in a jaundiced cat does not provide additional information on liver function in the case of cholestasis, as biliary stasis increases both bile acids and bilirubin. Clotting times may be extended and should be measured in cats with suspected liver disease prior to any sampling (eg, fine-needle aspiration).78,79
Additional tests
A number of assays have been assessed for their utility in the diagnosis of feline pancreatitis. Serum lipase and amylase activities are of limited value as they are insensitive and can be affected by liver, renal or GI dis-eases;5,72,87,88however, the DGGR-lipase assay has been shown to be useful, especially when compared with histology as the gold stan-dard. 25 Seroassays specifically measuring pancreatic lipase include feline pancreatic lipase immunoreactivity (fPLI), which is available as Spec fPL and SNAP fPL. Spec fPL is a quantitative test, for which concentrations >5.3 ug/l are consistent with pancreatitis and concentrations between 3.5 and 5.3 ug/l are in a grey zone. 89 Unlike Spec fPL, which is not available as an in-house assay, SNAP fPL is available as an in-house semiquantitative test. A positive SNAP fPL result indicates an fPLI value >3.5 Ug/l; it does not differentiate patients in the grey zone from patients with fPLI values considered consistent with pancreatitis. The DGGR-lipase test has similar sensitivity and specificity to the Spec fPL and, where available, may be a cost-effective alternative. 90 Serum fTLI is a species-specific immunoassay that has a relatively low sensitivity for the diagnosis of feline pancreatitis27,84,88and is more commonly used for diagnosing exocrine pancreatic insufficiency.
Evaluation of serum cobalamin and folate concentrations may aid in the diagnosis of IBD and chronic pancreatitis, and be important for guiding treatment in cats with both IBD and chronic pancreatitis. Low serum cobalamin concentration can indicate diffuse distal small intestinal (more specifically ileal) and/or pancreatic disease, while low serum folate concentration can be seen with diffuse proximal small intestinal disease. 77 Dietary cobalamin in cats is absorbed in the ileum and the uptake of the cobalamin-intrinsic factor complex is a receptor-mediated process.91,92
This can be affected by diseases of the intestinal mucosa as well as pancreatic disease, as the carrier protein, intrinsic factor, only comes from the pancreas in cats. Repeated bouts of pancreatitis can result in exocrine pancreatic insufficiency, with a concurrent deficiency in cobalamin, probably due to a lack of pancreatic intrinsic factor in these cats. Cats with GI disease may also have abnormalities in amino acid metabolism consistent with cobalamin deficiency. 93 Subnormal serum cobalamin concentrations may be found in 60% of cats with GI disease, and suggest that this test is a useful indirect indicator of feline enteric and pancreatic disease. 94
Other possible causes of chronic intestinal inflammation need to be ruled out through faecal examination for parasites (Giardia, Cryptosporidiumand Cystoisosporaspecies); culture for potential pathogenic bacteria; and/or a PCR panel including, for example, Tritrichomonas foetus, Giardiaspecies, Cryptosporidiumspecies, Toxoplasma gondii, Salmonellaspecies, Clostridium perfringensenterotoxin A gene, feline coronavirus and feline panleukopenia virus.
Diagnostic imaging
Imaging may be useful in the diagnosis of feline pancreatitis; however, abdominal ultrasound has been reported to have low sensitivity (11–35%).15,27,76,95Moreover, a study that evaluated ultrasonographic findings in cats with clinical, gross pathological and histo-pathological evidence of acute pancreatic necrosis found that the results of ultrasonog-raphy were consistent with a diagnosis of pancreatitis in only 7/20 (35%) cats. 96 Nonetheless, it has been suggested that a thick left limb of the pancreas, severely irregular pancreatic margins, and hyperechoic peripancreatic fat in cats with appropriate clinical signs and increased serum fPLI are highly supportive of pancreatitis. 96 The sensitivity of abdominal ultrasound is further influenced by difficulties in detecting the pancreas in some patients and is highly dependent on the skills of the imager and quality of the equipment.27,76
Abdominal radiography and/or abdominal ultrasound examination is used to confirm hepatomegaly and free abdominal fluid, if present. Ultrasonography may demonstrate diffuse heterogeneous (typically hyperechoic) liver parenchyma, sometimes with segmental dilatations in intrahepatic and extrahepatic bile ducts suggestive of repeated obstructions. There may also be hyperechoic contents. 45 However, in one retrospective study of cats with cholangitis, most of the cats had ultra-sonographically normal liver size, echogenici-ty and normal biliary systems. 45 In cases of EHBO, abdominal ultrasound may reveal diffuse heterogeneous change in the hepatic parenchyma, 97 plus distension of the common bile duct and gallbladder, with or without increased bile sediment. 25
Abdominal radiography is rarely useful in the diagnosis of IBD. Abdominal ultrasonog-raphy can be normal in many cases of IBD and low-grade alimentary lymphoma, but is important in ruling out other causes of chronic GI clinical signs. 98 Nonetheless, abdominal ultrasound is superior to radiology in defining focal vs diffuse mucosal disease, loss of intestinal layering, thickening of the muscu-laris layer, generalised intestinal thickening and mesenteric lymphadenopathy, which may be seen with IBD, as well as other infiltra-tive disorders (eg, lymphoma). 98 The significance of finding a thickened muscularis layer is debated. One study found this more commonly in cats with intestinal lymphoma or IBD compared with healthy cats; 99 in another study, a thickened muscularis layer in older cats was found more commonly in cats with lymphoma than those with IBD. 100 However, in a study of 56 cats - 22 with food-responsive enteropathy, 17 with IBD and 17 with alimentary lymphoma - there were no significant differences in the ultrasonographic findings between the three groups. 40
Ultrasonography can aid in the recognition of concurrent disease, providing useful information on the presence of multiorgan inflammatory disease, particularly involving the liver, pancreas and/or alimentary tract. A retrospective study by Marolf et al, looking at 26 cats with cholangitis, reported concurrent changes in the pancreas (enlarged in 39% of cats, hypoechoic in 26% and hyperechoic in 11%) as well as abnormal layering of the duodenum in 12% of cats. 45 In a necropsy study by Callahan Clark et al, looking at cats that had moderate to severe cholangitis diagnosed by abdominal ultrasound, liver abnormalities were described in 81% of cats (17/21), biliary tract abnormalities in 64% (14/22), pancreatic abnormalities in 52% (11/21) and GI tract abnormalities in 65% (13/20). 2 However, in another study, 58% (26/45) of cats with triaditis had no detectable abnormalities on abdominal ultrasound. 3
Practical guidance on performing abdominal ultrasonography in cats, and interpreting the resulting images, is provided in a virtual special issue series in JFMS, available at cpsi.jfms.com.
Biopsies
The gold standard for the ante-mortem diagnosis of inflammation in the pancreas, liver and GI tract in cats remains histopatho-logical analysis of biopsies. However, these patients are not always stable enough for surgical procedures.
Pancreatic biopsy (Figure 5) is invasive in nature and, because of the risk of further pancreatic inflammation, is not generally recommended in clinical practice for evaluating the presence of feline pancreatitis. 14 , 25 , 72 The biopsy procedure is often complicated by the sensitivity of the pancreas to hypoxaemia, whether induced by hypotension during anaesthesia or by pancreatic blood flow impairment following manipulation of other organs during surgery. Moreover, most cats with severe pancreatitis are poor candidates for anaesthesia. That said, pancreatic biopsy should be considered if laparotomy or laparoscopy are being performed for other reasons.89,101

Biliary bypass surgery in a 7-year-old cat with a biliary obstruction and acute pancreatitis. This image shows the right limb of the pancreas (black arrow) and the biliary bypass in situ (the gallbladder has been sutured to the duodenum [white arrow]). Pancreatic biopsies were also acquired. Courtesy of Donald Yool
In the literature, it was previously recommended that, in the absence of grossly identifiable abnormalities in the pancreas, a single biopsy at the distal aspect of the right limb of the pancreas should be taken because of its distance from the pancreatic duct system and comparatively reduced vascular supply to the other organs. 24 A later study reported that this may not be a reliable method of whole organ assessment; 102 however, taking multiple pancreatic biopsies increases the risks referred to above and is not recommended. A small study evaluating laparoscopic pancreatic punch biopsy of the left pancreatic limb in healthy cats reported this to be a safe technique. 103 Certainly, more studies are needed to evaluate the safety of pancreatic biopsies in cats with pancreatitis.
Intestinal biopsies should be considered in cats with normal intestinal layering on ultrasound or focal intestinal mass effects.98,100Intestinal biopsies can be performed via endoscopy, laparoscopy or laparotomy to confirm histopathological inflammation and to determine the extent of mucosal disease. 81 A study looking at techniques for taking intestinal biopsies in cats found endoscopic biopsies to be useful for the diagnosis of gastric lym-phoma, but inadequate for differentiating between IBD and lymphoma in the small intestine; this is because the common locations for lymphoma in cats are the jejunum and ileum, which can be challenging to reach by endoscopy in feline patients. 104 Full-thickness biopsies obtained via laparotomy or laparoscopy are better for more accurate evaluation of the jejunum and ileum, and for diagnosing inflammation in the pancreas and liver at the same time. However, these are invasive procedures, and laparos-copy may offer a minimally invasive alternative to laparoto-my for obtaining biopsy samples of all three organs, where available.
In cases of IBD, histology typically reveals lymphoplasma-cytic inflammation in the small and / or large intestine; 81 note that neutrophilic / suppurative, granulomatous and rarely eosinophilic scle-rosing fibroplasia can also be detected. 104 Full-thickness biopsies were useful in differentiating between intestinal lymphoma and chronic enteritis in one study, where ultrasonography or clinicopathological characteristics alone were not helpful for this differentiation. 105 Triaditis is most commonly associated with lymphoplasmacytic IBD; it can also occur as a suppurative syndrome, but this is much less common. 106
Treatment of triaditis
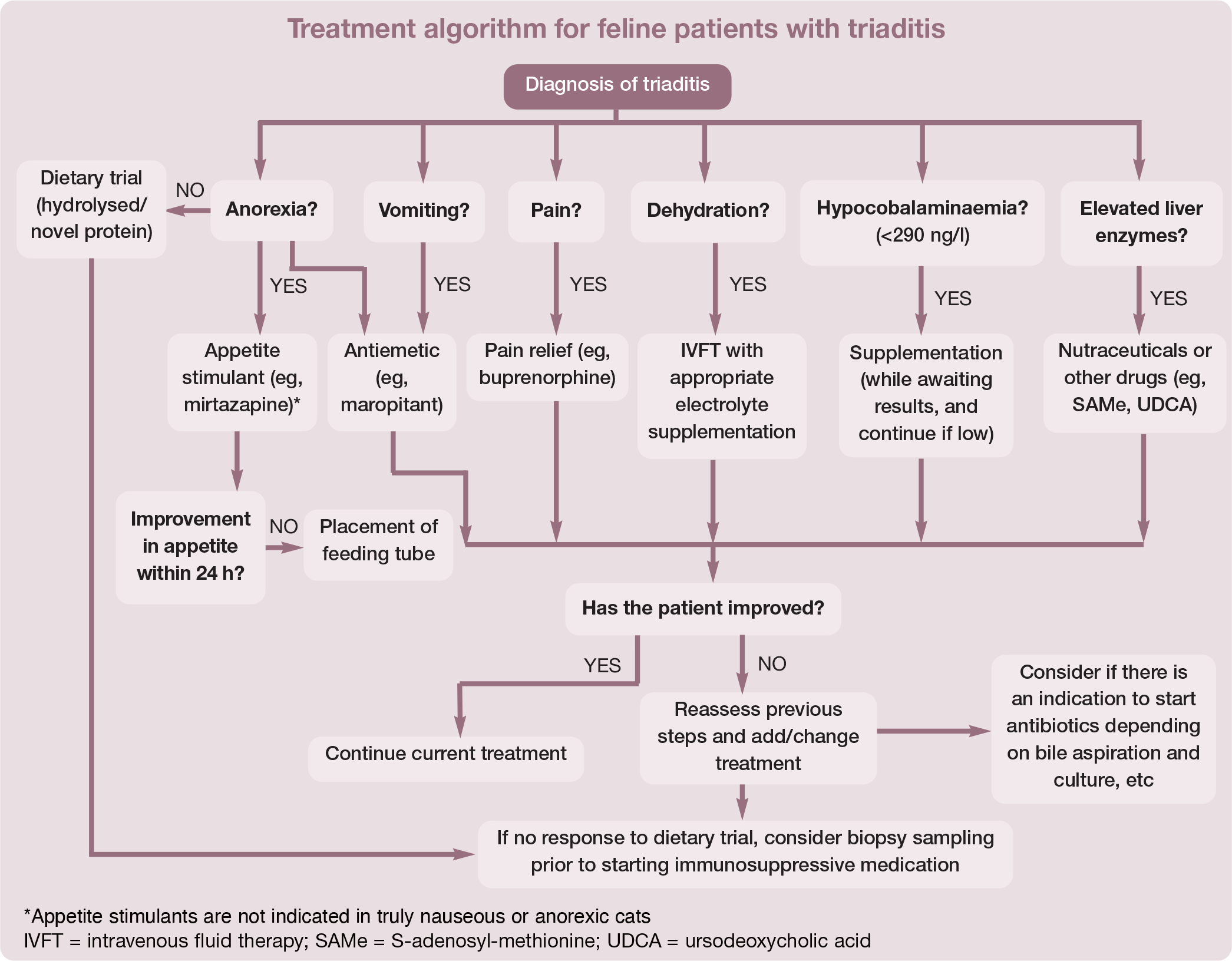
Since triaditis describes concurrent pancreatitis, cholangitis and IBD, and the aetiology of these comorbidities is unclear, treatment should be focused on the specific type and severity of the disease present in each of the organs involved in the individual cat (Table 5). 20 The authors recommend following a treatment algorithm for feline patients with triaditis, as shown on page 1058.
Recommended dosages of medications commonly used for the treatment of triaditis in cats

Not licensed for cats
See text for further discussion on when antimicrobial therapy is justified, and practical considerations
SC = subcutaneously; IV = intravenously; PO = orally; CRI = constant rate infusion; IM = intramuscularly; SAMe = S-adenosyl-methionine
Cats with mild clinical signs that are haemo-dynamically stable may be treated on an outpatient basis, but cats with severe clinical signs require hospitalisation and aggressive therapy including fluid therapy, analgesics, antiemetics and assisted feeding to prevent the development of hepatic lipidosis. Intravenous fluid therapy helps to ensure that the patient is well hydrated and the organs (eg, pancreas) are adequately perfused. At first, fluids should correct dehydration over the first 12–24 h, while also meeting maintenance needs and replacing ongoing losses from vomiting, diarrhoea and third-space losses such as peritoneal and/or pleural effusions secondary to pancreatitis. Acid-base and electrolyte abnormalities, such as hypo-kalaemia and hypocalcaemia, should be monitored closely and addressed if present.8,25Hypokalaemia can be corrected parenterally by adding potassium chloride to intravenous fluids for hospitalised patients or orally by supplementing with potassium gluconate (initial dose is 2.2 mmol/l per 4.5 kg q12h). The dose should be adjusted based on clinical improvement and serial measurements of serum potassium concentration.
Recommendations regarding the use of synthetic colloids, such as hydroxyethyl starch, have changed in recent years, with newer evidence questioning their efficacy and safety. 107 The use of fresh frozen plasma (FFP) in pancreatitis is questionable and one study reported higher mortality in dogs with pancreatitis that were receiving FFP compared with those that were not. 108 There is little specific information on the use of FFP in feline pancreatitis. However, the use of FFP may be beneficial in cats with severe liver disease and/or AP that have developed coagulopathy, 109 as active pancreatic enzymes can cause damage to cellular membranes, endothelium and adipose tissue, and interfere with the coagulation cascade; this can result in tissue damage, necrosis, disseminated intravascular coagulation, thrombosis, oedema and hypoxia.110,111
The fact that cats can hide pain and illness very well (a protective mechanism linked to predator avoidance in the wild 112 ) means they may appear healthy to their owners until their condition is very serious. Therefore, although cats do not always show abdominal pain, analgesia is important in the management of feline pancreatitis. Opioids such as buprenor-phine, methadone or fentanyl provide a good level of analgesia in cats.87,113Fentanyl trans-dermal patches have become popular as they provide a longer duration of analgesia; however, there is great individual variability in drug absorption and the risk of toxicity if the patient ingests the patch, so their reliability and safety have been questioned.114,115
Patients must be pain-scored frequently (eg, using the Glasgow Feline Composite Measure Pain Scale) to ensure they are receiving adequate pain relief.114–118Analgesia is also an important part of the management of cats with CP, and sublingual buprenorphine has been reported to provide a good level of analgesia in these cases.113,119Moreover, neuromodulatory analgesic drugs, such as gabapentin, have been reported to be useful for providing analgesia against neuropathic pain in humans and dogs,120,121and are a relatively well tolerated, easy-to-administer and potentially effective pain medication for cats, 122 especially the chicken-flavoured liquid version (where available).
Antiemetic therapy plays an important role in the treatment of triaditis. Although vomiting may only be intermittent in cats, patients may still be nauseous, which can contribute to the frequent anorexia seen in these patients. Maropitant citrate is a very effective antiemetic in cats and acts on the neurokinin (NK-1) receptors in the vomiting centre in the medulla oblongata. 123 Maropitant is also beneficial in reducing visceral pain in cats, which further supports its use in feline pancreatitis. 124 Ondansetron acts on the serotonin 5-HT3 receptors in the chemoreceptor trigger zone (CRTZ) 125 and is a very effective antiemetic in cats. 126 Metoclopramide is a dopamine antagonist and inhibits vomiting by blocking the central nervous system dopamine receptors in the CRTZ; however, cats are reported to have few dopamine receptors in the CRTZ, questioning the efficacy of this drug in this species.127,128In addition, as the effect of metoclopramide on splanchnic perfusion in cats is unclear, it should be avoided in patients with pancreatitis.
Nutritional support is crucial in the management of feline triaditis. The historical recommendation of nil per os for animals with pancreatitis is no longer accepted as this can cause intestinal mucosal atrophy and increased infectious complications due to bacterial translocation from the gut; in humans with severe acute pancreatitis, early initiation of feeding has resulted in reduced mortality.101,128–130This is especially important in cats as they often develop hepatic lipidosis with inadequate calorie intake.8,71,131Enteral nutrition stabilises the GI barrier, improves enterocyte health and immune function, improves GI motili-ty, prevents catabolism, and decreases morbidity and mortality.132–134
Appetite stimulants can help to support caloric intake, may reduce the need for feeding tube placement, decrease dependency on the feeding tube over time, and support the earlier removal of feeding tubes.
However, appetite stimulants are not indicated in truly nauseous and anorexic cats, and should not be used as an alternative to tube feeding. In cats that are not eating a significant amount of their daily requirements, feeding tube placement is preferred.
Mirtazapine is a commonly used appetite stimulant in cats and, although its mechanism of action is not fully understood, it most likely antagonises the 5HT2c and H1 receptors, which inhibit the appetite and regulate the appetite, respectively.135,136As mirtazapine undergoes hepatic metabolism, liver disease is reported to delay the clearance of the drug in humans and cats and, therefore, it is recommended that oral (or percutaneous) mirtazapine q24–72h only be given with caution to cats with significant liver disease. 137
Cats can be tempted with small portions of food, which can be warmed to enhance the smell. Note that syringe feeding should not be used as this can be stressful for cats and may create food aversion.
Assisted feeding may be provided through a naso-oesophageal, oesophagostomy (Figure 6) or gastrotomy tube. Typically, naso-oesophageal feeding is used on presentation, as cats with severe AP are often unstable, and have increased anaesthetic risk and severe hepatopathy (typically hepatic lipidosis), which can result in coagulopathy, thereby precluding surgical tube placement. 138 Once coagulation parameters (PT and APTT) have normalised (usually within 1-2 days of vitamin K treatment) and pancreatitis has stabilised, an oesophagostomy tube can be placed. Gradual introduction of food (see box) with continued monitoring for refeeding syndrome is recommended. 131

Assisted feeding through an oesophagostomy tube may be highly beneficial in the management of feline triaditis. Cats should always be offered food before tube feeding. This cat is eating warm chicken while also being fed through its oesophagostomy tube. There is an empty syringe beside the cat as the tube was also used to administer medications

If vomiting cannot be controlled, parenteral nutrition (with total parenteral nutrition solutions) can be used to meet some or all of the patient’s caloric needs. However, although parenteral nutrition supports the patient’s caloric needs, it has significant side effect risks, and it does not nourish the enterocytes.131,141In human medicine, early initiation of enteral nutrition in the management of AP has been reported, with decreased mortality.101,128–130Feeding tubes can also be used to give extra fluids and facilitate drug administration.
Pancreatitis
Cats with pancreatitis should be monitored for the development of exocrine pancreatic insufficiency and hypocobalaminaemia 142 and, where necessary, cobalamin should be supplemented either parenterally or orally.94,143A recent study looking at the use of cortico-steroids in dogs with AP, reported an earlier reduction in C-reactive protein concentration and earlier improvement of clinical signs after initial treatment with prednisolone (1 mg/kg/day) compared with the non-prednisolone group; 144 however, more (longer term) studies are needed before this can be recommended in dogs. 144 Studies are also needed to see if an anti-inflammatory dose of cortico-steroids improves clinical signs in cats with AP. At present, there is not enough evidence to support the use of corticosteroids in this way.
Cholangitis
The management of cholangitis is ideally based on bile culture results and the histopathological diagnosis; however, symptomatic therapies can also help. As NC is often associated with bacterial infection, antibiotics are warranted. When possible, culture and sensitivity testing of a bile aspirate or liver biopsy/aspirate should be used to determine the most suitable antibiotics. In general, a 4-week course of antibiotics is indicated, with acute cases usually responding more quickly than chronic cases.
The use of antibiotics may also be supported by the finding of positive FISH staining for bacteria. 54 (The pathology laboratory can be requested to send the histopathology block to special laboratories in the University of Bristol, UK or Cornell University, USA, for FISH testing.) Gram-negative and Gram-positive bacteria can be involved in hepatobiliary infections: E coli, Enterococcusspecies and anaerobes (Bacteroidesspecies and Clostridiumspecies, among others) have all been reported, with a prevalence of 7–56%.145,146Empirical treatment is with amoxicillin-clavulanate; however, this is only appropriate while pending results of culture (both aerobic and anaerobic) and sensitivity testing of a bile aspirate or liver biopsy/aspirate, as resistance is an important concern, especially for E coli.146,147
The duration of antibiotic therapy should be adjusted according to the clinical signs and liver enzyme values, and treatments lasting several weeks are often necessary. Caution with antibiotics that are metabolised in the liver (eg, metronidazole) is required in animals with jaundice or significant hepatic damage, making an adjustment in dose or administration interval, as necessary. 148
Symptomatic adjunct therapies may include ursodeoxycholic acid (UDCA), S-adenosyl-methionine (SAMe), silybin (milk thistle)149,150or other antioxidants such as N-acetylcysteine (NAC) or vitamin E (tocopherol). Cats with liver disease or severe IBD have a high prevalence of vitamin K-responsive coagulopathies, so treatment with vitamin K is recommend-ed. 151 In one study, 98% of cats with liver disease had one or more abnormalities of the coagulation parameters (APTT, PT, thrombin time [TT]), most consistently prolonged APTT. 79 Measurement of coagulation factors is crucial in patients undergoing surgery (eg, surgical biopsies) or oesophagostomy tube placement.
LC is thought to be immune mediated and many cats will require immunosuppressive therapy with drugs such as prednisolone, ciclosporin or chlorambucil. 152 A retrospective study comparing UDCA alone vs cortico steroids alone in the treatment of LC found UDCA to be inferior based on improved survival time in the prednisolone group. 153 Prospective studies are needed to evaluate the benefit of using UDCA and corticosteroids together for these patients.
IBD
Lymphocytic-plasmacytic enteritis, the most prevalent form of IBD, frequently responds to dietary modification with an antigen-restricted (potentially novel protein) or a hydrolysed diet, as multiple dietary components are recognised as foreign antigens by the enteric immune system. 154 A novel protein is a protein source that the cat has never been exposed to before, such as rabbit or kangaroo, while the protein in hydrolysed protein diets has been broken down by enzymes into small peptides that are less allergenic than entire proteins. 155
One study of cats with chronic idiopathic enteric signs reported improvement in clinical signs in 50% of cases, usually within 4 days of eating only a commercially available chicken-or venison-based single protein diet (Whiskas Feline Selected Protein Diet [chicken and rice] or Waltham Veterinary Diet Feline Selected Protein Diet [venison and rice]). Clinical signs did not recur after challenge with the animal’s previous diet in 20% of these cases, indicating that this was not an allergic response in these cats, merely a temporary enteric imbalance. 156 In a study of eight cats with IBD, a hydrolysed protein diet (Royal Canin Hypoallergenic) resulted in resolution of clinical signs within 4–8 days in all cases; however, in these cats, a challenge with the previous diet did result in recurrence of clinical signs. 157
The importance of clients feeding only the single diet, and not letting the cat eat or drink anything other than that diet and water, must be emphasised and understood. In stable patients, if one dietary trial fails to reduce clinical signs in 14 days, the authors recommend instituting a trial with a different diet for another 2 weeks before considering drug therapy.
Immunosuppression plays an important role in the treatment of IBD, and prednisolone should be considered in patients that do not respond to at least one strict dietary trial. 81 In the event of clinical signs recurring when prednisolone is tapered, therapy with additional immunosuppressive drugs such as chloram-bucil or ciclosporin can be initiated.81,158Chlorambucil or ciclosporin should be used as a first-choice treatment over prednisolone in cats with concurrent diabetes, and pred-nisolone should be used with caution in Burmese cats, as they are predisposed to diabetes.159–163It is important to note that chlorambucil is a chemotherapeutic agent and owners need to take precautions when handling this drug, such as wearing gloves when administering the medication and when cleaning the litter tray; particular caution is required in homes with young children and pregnant women.
Other medications that may also be useful include probiotics or prebiotics, which have been shown to have a beneficial effect in some cases of IBD.164–166If a cobalamin deficiency is documented, it should be supplemented; initially by parenteral injection, and then either by parenteral injection or orally.143,167
Antimicrobial therapy using tylosin or metronidazole, among other antibiotic agents, can be justified in the presence of intestinal infiltration with macrophages or neutrophils, or when a suspected infectious process has been confirmed by culture, special stains and/or FISH.78,168As mentioned earlier, metronidazole should be given at a lower dose in patients with severe hepatic disease because it is metabolised by the liver. 41 Where culture and sensitivity testing for intestinal disease is available, antibiotic selection should be based on this.
Faecal microbiota transplantations are now being used in cases of intractable diarrhoea in people and dogs,169–173and the authors have had some success with using them in feline cases too.

Prognosis
The prognosis for cats with triaditis depends on the severity of their disease. Cats with only mild disease can be treated on an outpatient basis and have a good prognosis. However, cats with acute severe disease, especially with systemic complications (systemic hypotension, hepatic encephalopathy, coagulopathy, vasculitis, disseminated intravascular coagulation, etc), may have a poor prognosis and more aggressive therapy is warranted.
Several risk factors have been reported in patients with triaditis. Hypoalbuminaemia and hypoglycaemia are strong indicators of severe and life-threatening disease 15 and systemic hypotension has been reported as a negative prognostic indicator in feline patients within an intensive care setting. 69 The outcome for cats with triaditis will depend on the successful management of all concurrent conditions, which can be challenging. Many affected cats develop chronic signs of illness, with recurrent episodes of triaditis over time, and appropriate management is important for decreasing the risk of potentially severe consequences. Chronic pancreatitis can predispose to exocrine pancreatic insufficiency and/or diabetes;71,110,175chronic/severe cholangitis can predispose to cholangiohepatitis, gallstones, chronic biliary cirrhosis and possibly cholangiocarcino-ma;176,177and chronic lymphoplasmacytic IBD can predispose to enteric lymphoma.178,179
Summary
Undoubtedly there is still a lot to learn about the natural history and aetiology of triaditis. More studies are needed to impart better understanding of which organs can be affected by this inflammatory process, how best to diagnose all component parts, which treatments are most effective and what factors are important prognostically.

Key Points
Triaditis is the concurrent presence of pancreatitis, cholangitis and IBD; the exact aetiology and prevalence of triaditis in cats has yet to be determined.
Triaditis may occur as a result of an infectious or autoimmune process, or potentially a physical problem, such as duct obstruction.
The anatomy of the feline GI tract may play its role in the aetiology of triaditis, due to the increased risk of ascending bacterial infections of the liver and pancreas.
It is important to recognise that feline patients with cholangitis, pancreatitis and/or IBD can manifest with non-specific and overlapping clinical signs and the ante-mortem diagnosis of triaditis can be challenging. Definitive diagnosis involves assessing histopathology from each organ; hence triaditis remains a presumptive diagnosis in many cases.
Early and appropriate medical therapy and nutritional support are crucial in the management of feline triaditis.
The treatment of triaditis should be focused on the specific type and severity of disease in each of the affected organs; however, it is often symptomatic.
Footnotes
Acknowledgements
The authors thank Camilla Tørnqvist-Johnsen for help with developing the treatment algorithm that appears on page 1058.
Author note
At the time of writing, Petra Černá was based at the Royal (Dick) School of Veterinary Studies, Edinburgh, UK.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not necessarily required.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. For any animals or humans individually identifiable within this publication, informed consent (either verbal or written) for their use in the publication was obtained from the people involved.