
Abstract
Objectives
The objective of this study was to quantify the effects of owner separation and physical examination location on fear, anxiety and stress (FAS) behavioral indicators in cats.
Methods
The study was a prospective, non-blinded, randomized, two-period, two-treatment crossover trial. Healthy adult cats presenting for wellness or dental evaluations at a single veterinary teaching hospital received three physical examinations: a baseline assessment (owner present) followed by physical examinations in both a treatment area (owner absent [TAOA]) and an examination room (owner present [EROP]). The physical examination sequence order was randomized. Low-stress handling techniques were used for all examinations. The primary endpoints were heart rate (HR; beats per min [bpm]) and total FAS scores. HR was measured by auscultation, and FAS by five specific behaviors scored as 0/1 and summed for each assessment period.
Results
Twenty-one healthy cats were enrolled. HR measured at entry (baseline) was a significant determinant of subsequent HR readings. HR measured during examinations conducted in both EROP and TAOA were elevated to levels indicative of stress (>180 bpm). HR was significantly higher for TAOA relative to EROP (30 bpm, 95% confidence interval 18–43; P <0.001). Behavioral FAS scores showed no statistically significant effects of sequence or room. FAS scores for TAOA assessments were clinically elevated relative to baseline (1.5 FAS, SE 0.7; P = 0.05); EROP FAS scores relative to baseline did not differ statistically (0.5 units, SE = 0.5; P = 0.43).
Conclusions and relevance
Owner separation coupled with physical examination location can result in clinically significant increases in perceived stress in cats, and compromise vital sign assessments. Whenever possible, physical examinations and procedures should take place with the owner present with separation from unfamiliar dogs and cats.
Introduction
Less than one-half of all cat owners in the USA seek routine preventive veterinary care and wellness examinations for their pets.1,2 Two common reasons cat owners cite for not taking their animals for routine care relate to anxiety and stress experienced by their cat during transport to the clinic, and prior stressful experiences at the veterinary clinic.2–4 Ideally, stress associated with clinic visits could be minimized or eliminated by conducting physical examinations in the cat’s home environment. 5 However, although in-home veterinary care services are increasing, many practices cannot make house calls on a regular basis, and certain procedures will require clinic facilities.
Even healthy cats can experience considerable anxiety and stress in the clinic environment because of unaccustomed surroundings, people and methods of handling.6–9 Anxiety and stress affect many clinical measurements used to evaluate animal health, such as temperature, respiratory rate, blood pressure and heart rate (HR).3,10 Anxiety and stress can also adversely influence the results of diagnostic tests, such as those for blood glucose, lactate and cortisol.4,7,11,12 Furthermore, the effects of stress on cat behavior and health may persist far beyond the actual clinic visit. Surveys of cat owners suggest that cats were remote and unfriendly for several days after the clinic visit.2,9 Routine but stressful veterinary visits may contribute to long-term patient behavioral issues,9,13 and prolonged stress can induce or exacerbate abnormal behaviors7,14,15 and comorbid conditions.15,16 As a result, best practice evidence-based guidelines now recommend cat-friendly low-stress handling procedures to minimize stress to cats during clinic visits.4,17,18 Whenever possible, it is suggested that cats be kept separate from unfamiliar conspecifics and dogs, and that procedures are performed in the examination room with the owner present. However, anxious owners can make their pet’s experience more stressful and impede examination.2,19
The purpose of this study was to compare and quantify simple indicators of stress experienced by healthy cats when examined in different clinical examination locations, with and without the owner present. We hypothesized that perceived stress would be greatly enhanced for healthy cats examined in an unfamiliar setting without the owner, but alleviated in part by owner presence.
Materials and methods
Animals and study design
This study was a prospective, non-blinded, randomized, two-period, two-treatment crossover trial. Study animals consisted of healthy adult cats presenting for routine wellness and/or dentistry examinations through the Primary Care and Dentistry Service at the University of Florida Small Animal Hospital, between June and July 2018. The service provides care for approximately 1300 cats in Gainesville, FL and the surrounding area, and includes approximately 450 wellness visits per year. Cats eligible for this study included all adult cats whose owners consented to participate in the study and reported that their animals typically presented without requiring undue restraint, sedation or anxiolytics prior to examination. No restrictions were placed on breed, age, sex or reproductive status (spayed/castrated, entire). Animals excluded from the study were those with a history of fractious behavior (growling, hissing, swatting, biting), ill at time of presentation, if there was any reported use of sedatives (eg, acepromazine), anxiolytics (trazadone, benzodiazepines), opioids (tramadol, buprenorphine), phenobarbital or gabapentin, or if there was a diagnosis of chronic conditions that could alter normal cardiovascular physiology. The study was approved before subject enrolment by the University of Florida Institutional Animal Care and Use Committee (IACUC# 201810125).
Study workflow
Electronic records of potential subjects were screened before arrival to assess eligibility. Owners were contacted by telephone 3–5 days prior to a scheduled wellness or dental appointment to be given the opportunity to participate in the study, provide an explanation of the study protocol and obtain verbal consent. The owner was then asked to describe the typical behavior of the pet during clinic visits, and if sedatives or anxiolytic medications were usually required. Candidates were enrolled if the inclusion criteria were met. Owners were instructed to arrive at the time of their appointment to minimize the time spent in the waiting room. On arrival at the clinic, owners were provided with a formal written consent form and directed to a dedicated cat-only waiting room.
Examinations were conducted between 08:00 and 14:30 over 21 days in June and July 2018. Each subject was evaluated three times. With the owner present, baseline HR and behavioral measures were obtained by two primary care veterinary students trained in low-stress handling and assessment techniques. The attending veterinarian then conducted two complete and identical physical examinations in both an examination room and the treatment area. Each physical examination consisted of standard wellness procedures: body weight determination, auricular temperature, thoracic auscultation (for heart and respiratory rate and sounds), otoscopy and ophthalmoscopy. The subject was placed on a clean towel for each examination, and all surfaces were cleaned with hospital-grade disinfectant between patients. Five examination rooms were available, each consisting of a single enclosed space separated from the medical areas. The treatment area was a single large multipurpose space with two examination tables, two wet tables for dental procedures, a row of large dog runs and two banks of cages for small dogs and cats.
Eligible subjects were randomly assigned to one of two examination sequences before clinic arrival using Google’s random number generator function (www.random.org). Patients assigned to the first group went first to the examination room with the owner present (EROP; intervention A, period 1), followed by transfer to the treatment area, a common examination space with the owner absent (TAOA; intervention B, period 2). Subjects assigned to group 2 received interventions in reverse order (B: TAOA in period 1, followed by A: transfer to EROP in period 2). Patients were transported to each examination location in their owner-provided carrier. The three assessments were completed <10 mins apart, and the total time to conduct all three assessments for each animal was under 30 mins. During examinations conducted by the attending veterinarian, the animal was gently restrained by one student, while the second student observed and documented signs of fear, anxiety and stress (FAS) according to a standardized checklist. All raters remained the same over the duration of the study.
Prior to the study, all veterinary assessors completed the online eight-module Fear Free certification program (https://fearfreepets.com) to standardize training in low-stress handling and assessment. Low-stress handling methods involved patient placement in a sternal position, with minimal hands-on restraint (resting along dorsum or flanks, petting) without scruffing or head restraint. The patient was allowed to stand up and move around if it chose to, although it was not allowed to leave the examination table. As far as possible, the examining veterinarian maintained hands-on contact with the patient to minimize any startle response. No analgesics or sedatives were used for any animals in this study.
Outcome variables
The primary outcomes of this study were HR and cumulative FAS score measured at baseline and during each physical examination. HR was measured by auscultation for at least 30 s, and converted to beats per min (bpm). An HR of 120–150 bpm was considered to be within the normal range for a non-stressed cat, and an HR >180 bpm to be indicative of stress, based on comparisons of hospital vs home environment assessments. 3 FAS was scored by presence/absence (1/0) on each of five standardized behaviors (Table 1) and summed for each behavior for a total possible score of 0–5 for each individual cat during each assessment.
Behavioral indicators of fear, anxiety and stress (FAS) used to score cat behavior during three separate examinations at baseline and with and without the owner. Behaviors were scored as present (1) or absent (0)

Statistical analysis
Sample size calculations were performed for HR using the paired-means test for equivalence under a 2 × 2 crossover design 20 using SAS Procedure Power (SAS version 9.4) and for FAS (an ordered categorical variable) by power simulations for a proportional odds model (http://www.pmean.com/04/OrdinalLogistic.html). 21 Calculations estimated a sample size of approximately 37 to detect a clinically relevant difference of 30 bpm in HR (assuming an SD of 10 and correlation of r = 0.3), and 35–40 to detect a shift in FAS score by at least 1 unit from the expected proportion of 80% of subjects exhibiting mild-to-moderate stress (FAS 0–2) at baseline to 80% with heightened to severe stress (FAS 3–5) at examination (α = 0.05 and 1 – β = 0.8).
HR data were analyzed by a mixed-effects 2 × 2 crossover model in SAS Mixed Procedure (SAS version 9.4). 22 Fixed effects were intervention, sequence and period. ‘Intervention’ refers to the examination location (EROP vs TAOA), ‘sequence’ refers to the order of examination location presentation (AB vs BA) and ‘period’ refers to the timing of location presentation (first vs second). ‘Subject’ was modeled as a random effect, and within-subject correlation modeled by unstructured variance–covariance structure. Baseline HR for each subject was used as a covariate. Ordinal FAS data were analyzed by cumulative logit mixed-effects 2 × 2 crossover model in SAS Glimmix Procedure, with baseline FAS as the reference level, intervention, sequence and period as fixed effects, and subject as random effects. 23
Results
Of 50 cats screened, 24 cats met initial inclusion criteria with owner consent. Three cats were subsequently excluded because of illness, based on the physical examination (n = 1) or procedural errors (n = 2). The 21 cats included in the study were mostly domestic shorthairs (n = 17), ranging in age from 1 to 12 years (mean 6 [SD 3] years). Twelve were male and nine were female, and all were castrated or spayed. Twelve cats (six males, six females) were randomized to sequence AB, and nine (six males, three females) to sequence BA. Data collected for analyses are presented in the supplementary material.
HR
HR response during the three assessment periods is shown in Figure 1. Baseline HR averaged 176 (SD 35) bpm during the preliminary examination, with 6/21 cats exhibiting an HR of >180 bpm. Baseline HR was a statistically significant covariate (F = 8.41, P = 0.01). Sequence (t = 0.69, P = 0.41) and period (t = 1.60, P = 0.22) effects were not statistically significant. However, HR differed statistically as a result of examination location (F = 27.77, P <0.0001); HR was elevated by 30 bpm (adjusted 95% confidence interval 18–43; P <0.001) during TAOA examinations (mean 226, SD 7 bpm) relative to EROP examinations (mean 195, SD 7 bpm).
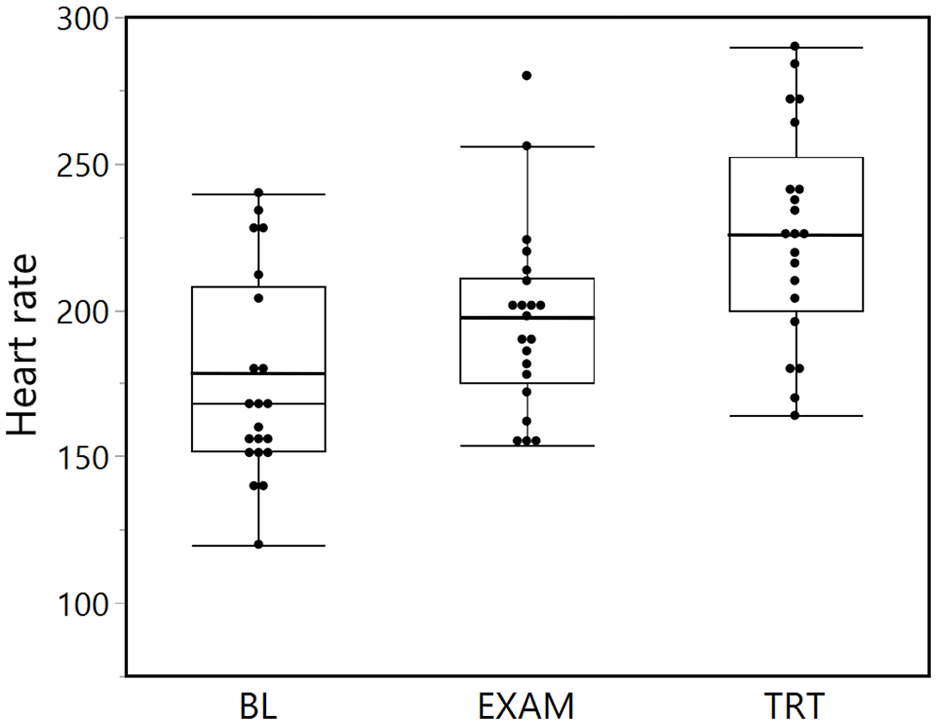
Box plots of heart rate (HR) response (beats per min) in 21 cats assessed at baseline (BL) and during two subsequent physical examinations, conducted in an examination room with the owner present (EXAM) and a common treatment area with the owner absent (TRT). HR measured in TRT was significantly elevated compared with BL
FAS scores
Distributions of FAS scores are shown in Figure 2. Modal FAS score at baseline was 3 (range 0–4) for all animals, with 15/21 cats with a FAS score of ⩾3. FAS scores changed by >±1 FAS unit dependent on sequence (AB vs BA, effect size +1.3 units, SE = 1.3; F1,19 = 1.05, P = 0.31) and period (EROP first, effect size –1.2, SE = 0.7; F = 3.47, P = 0.07). Overall location effects were not statistically significant. FAS for TAOA location relative to baseline increased by +1.4 units (SE 0.7, P = 0.051). FAS for EROP relative to baseline increased by +0.6 units (SE 0.7, P = 0.43). Nearly all cats showed tail curling (n = 16/21), back position changes (n = 17/21) and pupil dilation (n = 19/21) at baseline. For subsequent examinations, cats exhibited more frequent ear deviation (n = 10/21) and vocalization (n = 5/21) during TAOA examinations than EROP examinations (n = 7/21 and n = 2/21, respectively; Table 2; see also the data in the supplementary material).

Frequency of total fear, anxiety and stress (FAS) scores based on five behaviors assessed at baseline and during two subsequent physical examinations conducted in an examination room with the owner present (EROP) and common treatment area with the owner absent (TAOA). FAS was scored by presence/absence (1/0) for each of five standardized behaviors for each cat during each examination. Note the shift in FAS scores from a modal value of 3 at baseline (moderate stress) to FAS scores of 4 and 5 for both EROP and TAOA
Frequency of fear-, anxiety- and stress-related behaviors for 21 cats scored at baseline and during two subsequent examinations in an examination room with the owner present (EROP) and a common treatment area with the owner absent (TAOA)

Discussion
Cats may be subject to considerable stress from routine healthcare visits, both during carrier transport to the clinic2,24 and during the actual in-clinic physical assessments. During clinical examinations, cats will experience additional stress by transfer to a different room for treatment, separation from their owner and exposure to unfamiliar surroundings, personnel, and other cats and dogs. In this study, clinically significant elevations in both HR and FAS, coupled with more FAS-related behaviors (ears deviated, tail curling, back position, pupil dilation, vocalization) suggest that removal of the cat to the common treatment area away from the owner may exacerbate stress and anxiety induced by the clinic visit. Although this study was small, the clinical robustness of findings indicated that examinations in the segregated examination room in the presence of the owner may be of benefit in reducing some of the more overt signs of stress in cats. The strong influence of baseline levels of HR and behavioral stress indicators on subsequent responses further suggest that initial stress levels at clinic entry may contribute to overall stress associated with clinic visits.
In addition to implementation of low-stress handling procedures, 6 clinic-related stress mitigation measures have included pharmacological agent administration25–27 and environmental changes.6,28 However, choice of where to perform the physical examination is rarely considered. One practical application at this institution of the results of this study is that, whenever possible, procedures are restricted to examination rooms with the owner present, with more frequent use of feline-only examination rooms provided with catnip and hiding places. If invasive procedures are required, clinicians now more commonly request the owner to leave the examination room, rather than take the cat to the common treatment area. We have also incorporated use of Feliway ‘calming’ diffusers, towel restraint when indicated and food rewards. 9
The limitations of this study were lower-than-expected recruitment (resulting in underpowered estimates for effect sizes) and the inability to blind behavioral assessors to location. Low enrollment coupled with higher than expected baseline FAS scores meant that the study was underpowered to statistically detect certain behavioral changes resulting from examination location. Total assessment time and time between examinations were relatively short, so there may have been carry-over between exposures. Additional limitations include variations in daily caseloads and client arrival and wait times, resulting in patient exposures to different levels and duration of stimulation and activity in the waiting room. Effects of owner separation as a factor were unavoidably confounded by the use of a common treatment area and the presence of unfamiliar dogs and cats. There was no information available on the amount of preclinical habituation training provided by each owner. Entry stress levels may have been exacerbated by carrier transport2,24 and clinic wait times, and may account, in part, for the variability in baseline HR and FAS scores observed in this study. Finally, we were unable to measure serum cortisol levels as an independent and possibly more reliable measure of stress.5,10,11
Conclusions
To reduce stress associated with clinic visits, evidence-based guidelines have been implemented by the American Association of Feline Practitioners 4 and American Animal Hospital Association 17 to educate veterinarians in stress-mitigation handling strategies. Nevertheless, there is still considerable variation between practices in consistency and standardization.2,4,18,24 Results from this study indicate that minimizing transfer between examination areas and including the owner during wellness examinations can reduce some of the more overt signs of stress in cats during clinic visits. The data also suggest more proactive owner education measures may be of benefit, such as methods of owner habituation of their pet for transport and handling ahead of scheduled clinic visits.9,29 Future studies on feline stress mitigation measures should evaluate before and after practice changes on feline stress and owner satisfaction, and effects of standardized instructions to owners in pre-visit habituation methods.
Supplemental Material
Supplementary Material
Feline data
Footnotes
Acknowledgements
The authors thank Dr Amara Estrada for providing the initial impetus for this research project and useful feedback on the manuscript; Dr Rowan Milner for assistance with the initial analyses; and the faculty and staff of the University of Florida Primary Care and Dentistry Service for their support while performing this study.
Author note
Initial study findings were presented at the University of Florida, College of Veterinary Medicine, Florida Veterinary Scholars Program poster day, by student researcher, A Deriberprey (August 2018).
Supplementary material
The following file is available online: Feline data.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Financial support for the research for this article was provided by Fear Free (![]() ), PetSmart Charities grant, the Small Animal Clinical Sciences Department at the University of Florida, College of Veterinary Medicine (UF-CVM), and the Florida Veterinary Scholars Program at UF-CVM (recipients: A Deriberprey and A Blew). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
), PetSmart Charities grant, the Small Animal Clinical Sciences Department at the University of Florida, College of Veterinary Medicine (UF-CVM), and the Florida Veterinary Scholars Program at UF-CVM (recipients: A Deriberprey and A Blew). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee, while not necessarily required, was nonetheless obtained, as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.