
Abstract
Practical relevance:
Abdominal ultrasound plays a vital role in the diagnostic work-up of many cats presenting to general and specialist practitioners. Ultrasound examination of the urinary tract provides important information useful in the investigation of several conditions including ureteral obstruction and cystitis.
Clinical challenges:
Despite ultrasonography being a commonly used modality, many practitioners are not comfortable performing an ultrasound examination or interpreting the resulting images. Even for the experienced ultrasonographer, differentiating between incidental findings, such as lipid droplets in the bladder, and pathological changes can be challenging.
Aim:
This review, part of an occasional series on feline abdominal ultrasonography, discusses the ultrasonographic examination of the normal and diseased renal pelvis, ureters and urinary bladder. Aimed at general practitioners who wish to improve their knowledge of and confidence in feline abdominal ultrasound, this review is accompanied by high-resolution images and videos available online as supplementary material. Ultrasound examination of the kidneys and perinephric space was discussed in an article published in May 2020.
Equipment:
Ultrasound facilities are readily available to most practitioners, although the use of ultrasonography as a diagnostic tool is highly dependent on operator experience.
Evidence base:
Information provided in this article is drawn from the published literature and the author’s own clinical experience.
Keywords
Abnormalities of the renal pelvis
Dilation of the renal pelvis
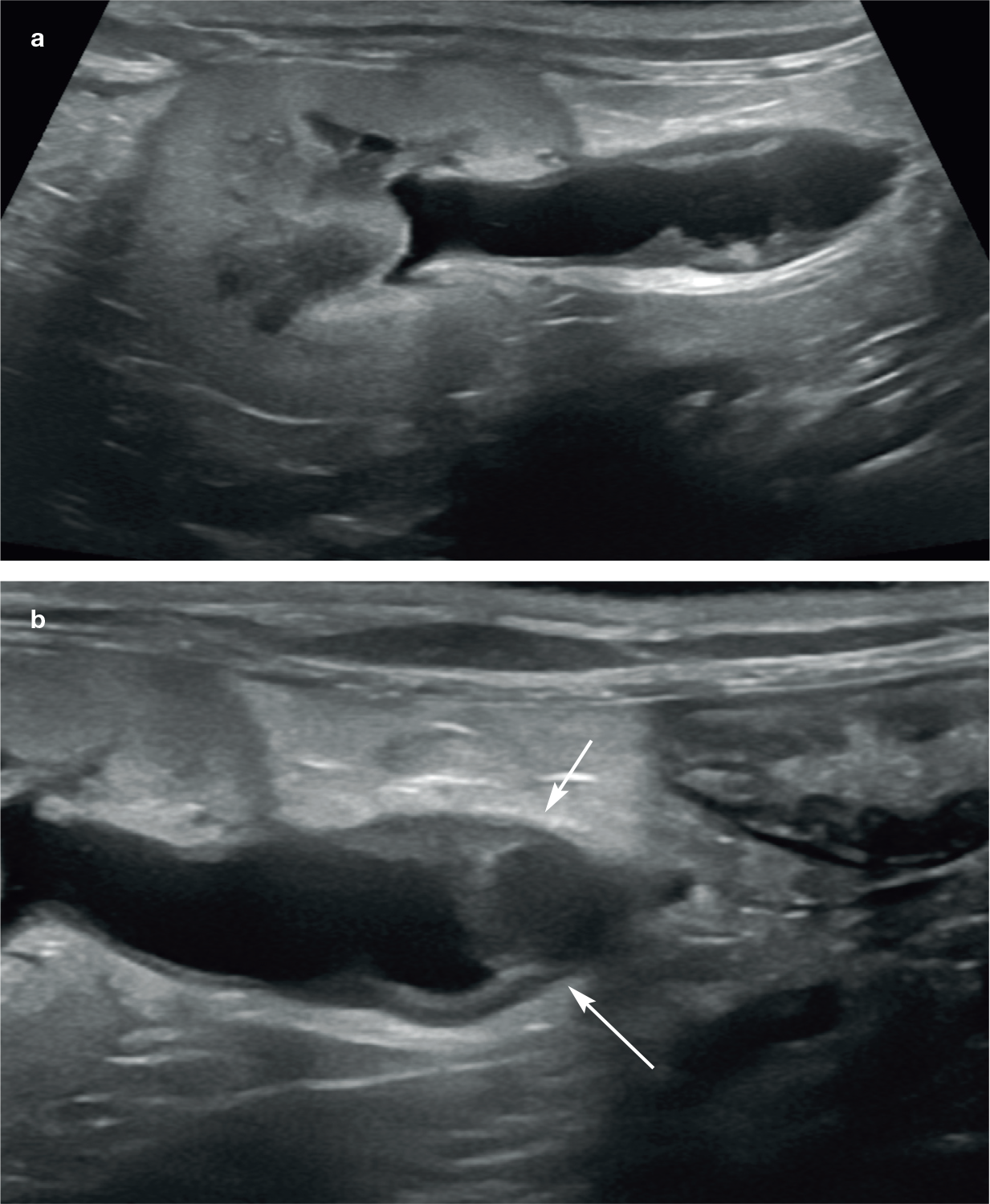
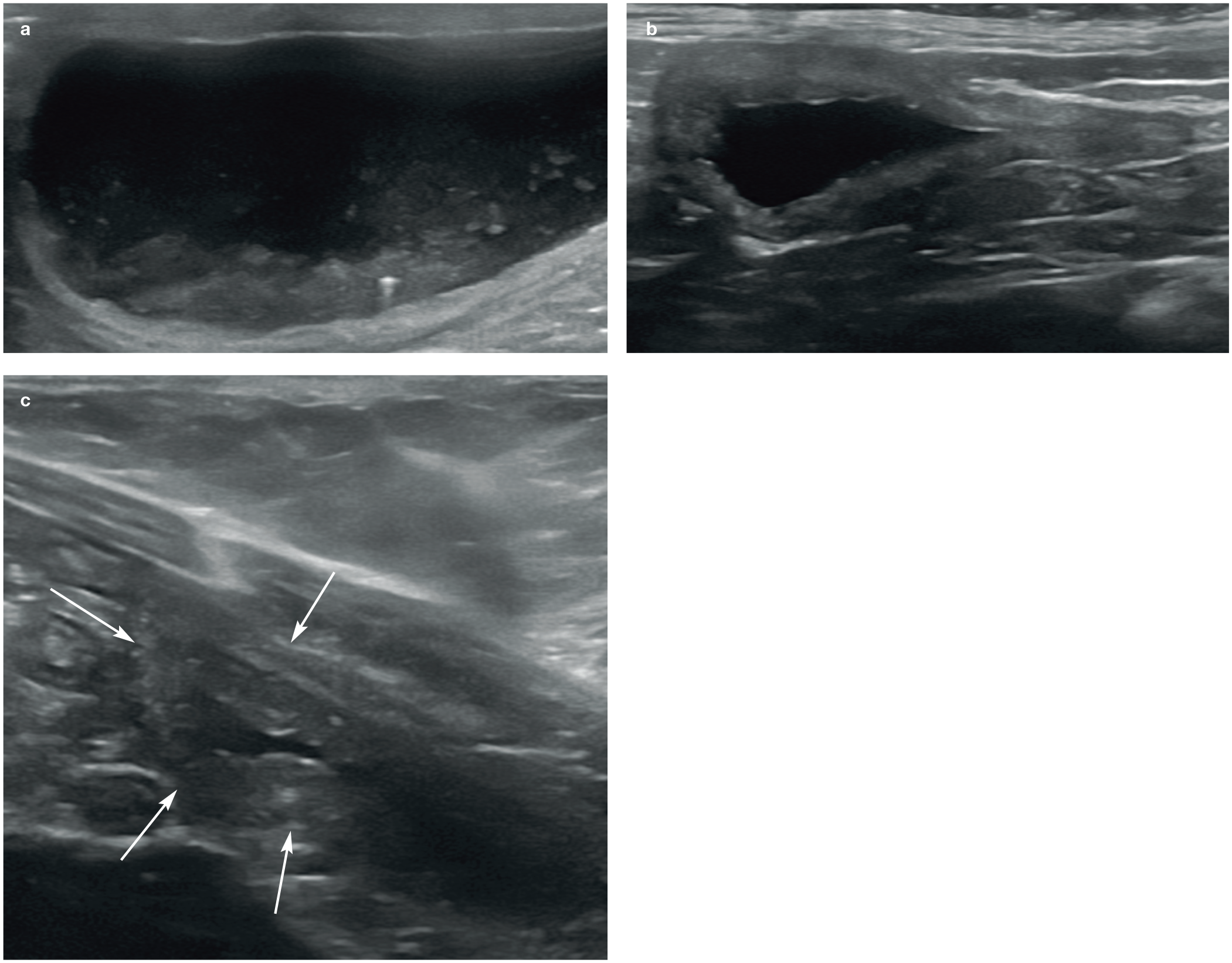
The term pyelectasia is used to describe mild or moderate, non-obstructive dilation of the renal pelvis, 1 whereas the term hydronephrosis is typically reserved for pelvic dilation secondary to obstruction, which is often much more severe. 2 It is important not to confuse the hypo- to anechoic medulla with a dilated renal pelvis. Pyelectasia is usually easier to recognise in the transverse plane on ultrasound. 1 The fluid within the pelvis forms a heart- or crescent- shaped anechoic region that wraps around the renal crest (Figure 1). 1 When viewed with the kidney in the dorsal plane, pelvic dilation becomes linear to oval-shaped. 1 As pelvic distension becomes progressively more marked, the pelvis develops a rounded appearance (Figure 2). In severe cases of hydronephrosis, pressure necrosis of the renal parenchyma can result in substantial loss of tissue. In extreme cases, the only remaining tissue may be that forming a thin border surrounding a markedly dilated pelvis (Figure 3). Multiple echogenic linear bands of tissue representing interdiverticular septa are often evident extending from the hilum towards the renal capsule (Figure 3c). 3
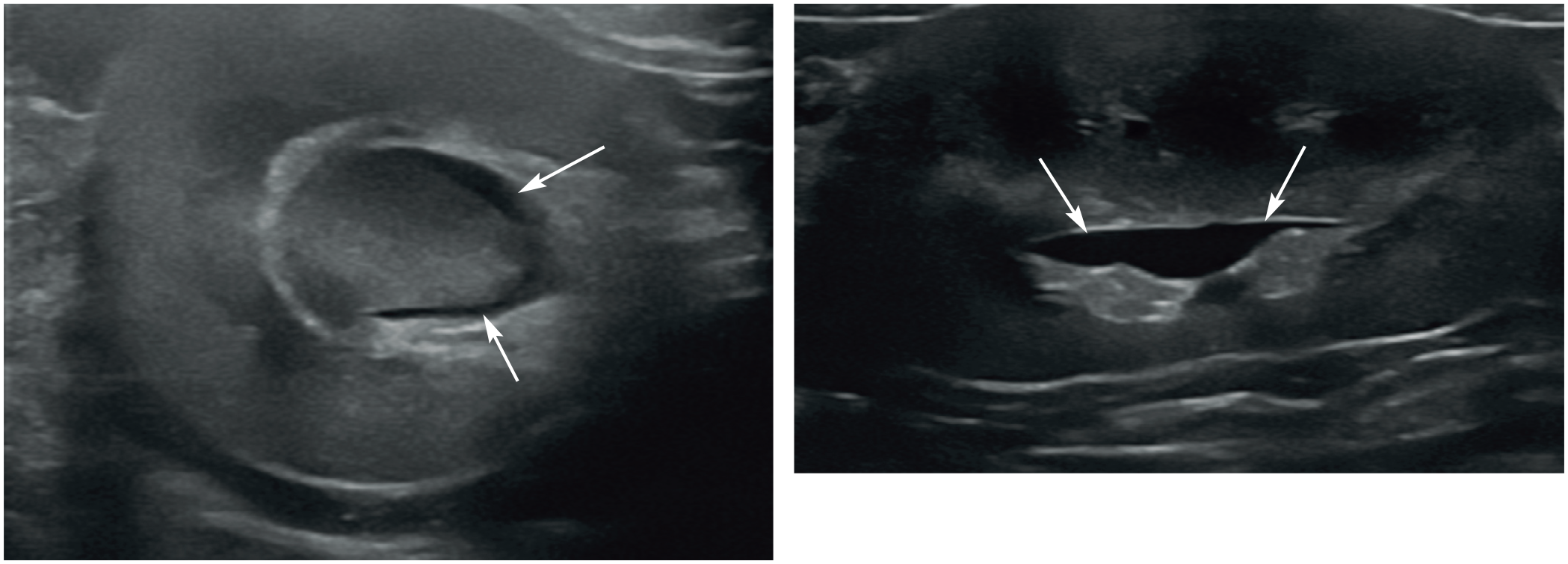
Mild distension of the renal pelvis (arrows) in transverse (a) and longitudinal (b) planes. A video showing mild pyelectasia is available as supplementary material

Longitudinal (a) and transverse (b) ultrasound images showing moderate dilation of the renal pelvis (asterisk in [a] and measuring calipers in [b]) in a 10-year-old male neutered domestic shorthair cat with hydronephrosis due to obstructive ureterolithiasis. The diverticula are mildly dilated in (a). A video showing the moderate hydronephrosis in this cat is available as supplementary material. The kidney is also enlarged (4.8 cm in length) and there is reduced corticomedullary definition. (c) Moderate dilation of the left renal pelvis in a 5-year-old female neutered domestic shorthair cat referred for further investigation of acute renal failure. There is marked dilation of the pelvic diverticula (asterisk). Ultrasonographic findings were consistent with previous obstruction of the right kidney resulting in a non-functional, end-stage kidney and concurrent obstruction of the left ureter due to a ureterolith and secondary hydronephrosis. A video showing these findings is available as supplementary material

(a,b) Severe hydronephrosis in two cats following ureteral ligation during ovariohysterectomy surgery. In both cats, the renal parenchyma has been reduced to a thin mantle of tissue surrounding a severely dilated urine-filled pelvis. Reverberation artefact in the near field of the dilated pelvis is due to gas introduced iatrogenically during pyelocentesis. A video showing severe hydronephrosis is available as supplementary material. (c) Same cat as in (b). Hyperechoic bands of tissue located within the periphery of the kidney represent interdiverticular septa (arrows)
Urinary stasis and subsequent infection can lead to pyonephrosis. The term literally means pus in the renal pelvis and this has been reported in cats with ureterolithiasis and in a single cat with a circumcaval ureter.4,5 Ultrasonographic findings include echogenic debris within the renal pelvis, hydronephrosis and loss of renal architecture (Figure 4). 5
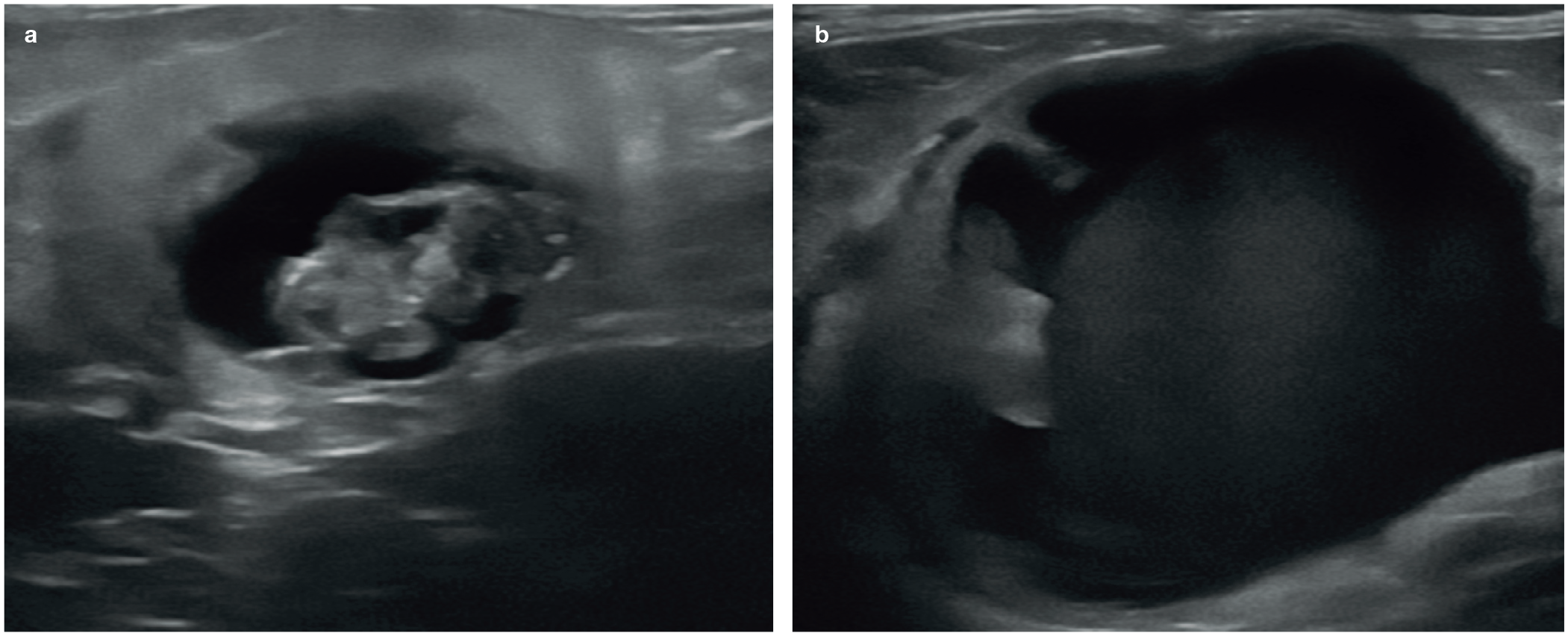
Pyonephrosis. (a) A conglomerate of non-vascularised echogenic material is visible within the dilated renal pelvis of a 12-year-old male neutered domestic longhair cat with chronic pyelonephritis. The kidney is small and the renal cortex is abnormally hyperechoic. (b) Severely hydronephrotic kidney in a 12-year-old female neutered Burmese cat. Three ureteroliths were present within the ureter (not shown), causing complete outflow tract obstruction. The pelvis contains a large amount of echogenic fluid consistent with pus. A video showing these findings is available as supplementary material. Urinalysis revealed a concurrent urinary tract infection. Fat surrounding the kidney is moderately hyperechoic, consistent with inflammation of the retroperitoneum
Two studies have specifically evaluated renal pelvic diameter in healthy cats and in those with renal disease.6,7 Although the pelvis is a potential space in many cats, mild pyelectasia up to around 3.0–3.5 mm in diameter may be recognised in cats with clinically normal renal function and in cats with clinically normal renal function undergoing diuresis. 6,7 Pelvic dilation greater than this should be regarded as potentially abnormal.
A significant proportion of cats with stable chronic renal insufficiency will also have evidence of pelvic dilation, a feature that is likely to be attributable to the diuresis naturally accompanying this condition. In a group of 66 cats with chronic kidney disease (CKD), two-thirds had evidence of pyelectasia on ultrasound, with pelvic diameters ranging from 1.2 mm up to 11.5 mm. 7 Interestingly, the degree of pelvic dilation does not appear to correlate with serum creatinine levels or CKD stage according to International Renal Interest Society (IRIS) guidelines. 7 Since pelvic dilation can occur with CKD, it is recommended that baseline pelvic measurements are determined at the time of initial diagnosis. 7 This is to avoid mistaking pelvic dilation in cats undergoing a uraemic crisis as evidence of pyelonephritis or urinary obstruction when the dilation may have been present for some time. 7 A total of 20 cats with a diagnosis of pyelonephritis across both this study and an earlier study have also been evaluated.6,7 Recorded pelvic dilation among these cats varied from 0 mm to 12.4 mm.6,7 However, as expected, the most severe cases of pelvic dilation occurred in cats with urinary outflow obstruction, with diameters up to 39.1 mm reported. 6
Both of the aforementioned studies showed clear evidence of substantial variation in pelvic width between animals with the same condition (such as CKD) and a significant overlap of pelvic diameters in cats with different conditions.6,7 For example, cats with clinically stable CKD can have renal pelvic dilation of similar magnitude to that observed in cats with pyelonephritis. 7 Similarly, not all cases of outflow obstruction are associated with marked pelvic dilation. Ureteral calculi in the presence of minimal pelvic dilation (1–2 mm) were reported in some cats. 6 In other studies, absence of pelvic dilation was even reported in a small proportion of cats with confirmed ureteral calculi,6,8 suggesting that obstruction may have been incomplete.
Therefore, while pelvic diameter can be used as a guide, it should not be relied upon as the sole criterion by which different conditions are differentiated. Notwithstanding this, a few rules of thumb can be deduced from the results of these studies (see box on right).
Pyelonephritis
Pyelonephritis refers to inflammation of the renal pelvis and parenchyma that typically results from an ascending bacterial urinary tract infection. 2 Although pyelonephritis has been described in the cat,7,10–19 reports detailing the specific ultrasonographic appearance of the condition in this species are scarce, with findings limited to renal enlargement and irregular margination, hyperechoic cortices, decreased corticomedullary definition 11 and obliteration of normal medullary architecture. 17 Further abnormalities include mild to marked pelvic dilation,11,17,18 the presence of echogenic gravity-dependent sediment within the renal pelvis 18 and dilation of the proximal ureter. 1 Gas within the kidney consistent with emphysematous pyelonephritis has been diagnosed in two cats (one diabetic).11,18 While both gas and uroliths produce hyperechoic interfaces on ultrasound, gas results in a ‘dirty’ acoustic shadow due to the presence of reverberation artefact within the shadow, whereas uroliths produce a ‘clean’ shadow, thus allowing the two to be distinguished. 3

Pelvic calculi
As mentioned, calculi are occasionally identified within the renal pelvis. Depending on their location and the frequency of the transducer, small calculi may be difficult to differentiate from renal parenchymal mineralisation or bright echoes from the walls of arcuate vessels. The appearance of calculi within the urinary tract is described in the ‘ureteral dilation’ section.
Abnormalities of the ureters
Ureteral dilation
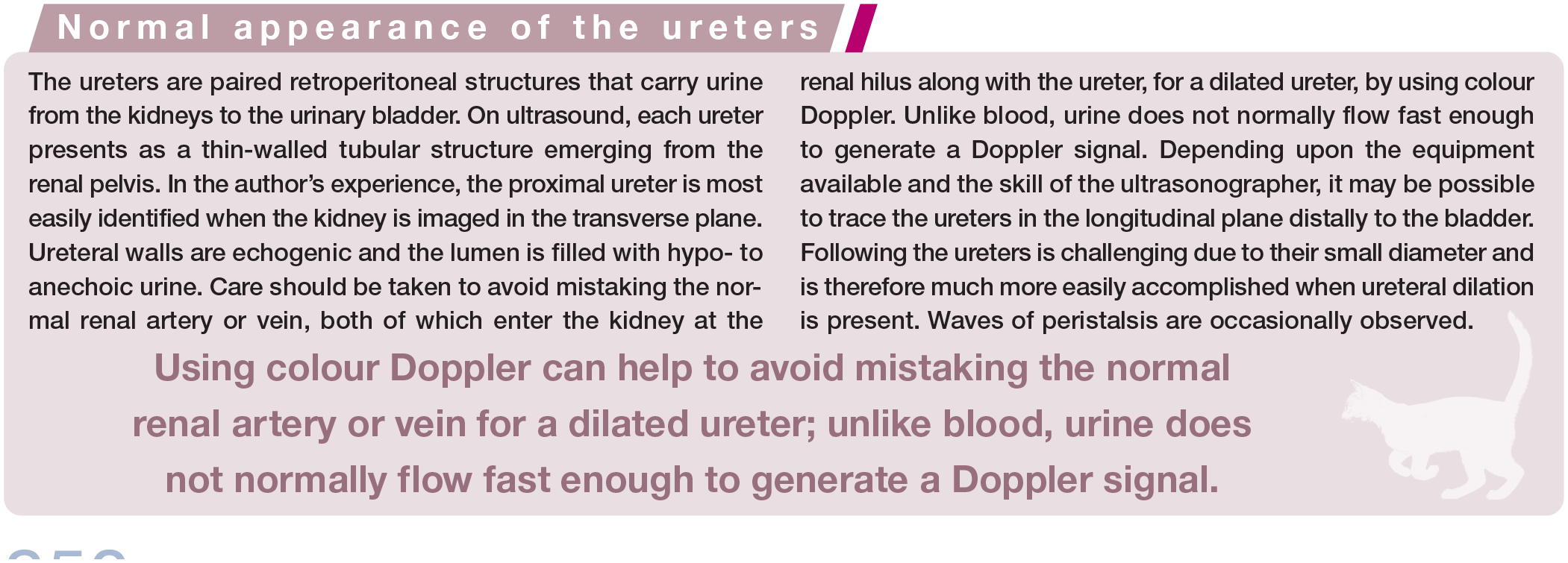
Ureteral dilation (hydroureter) is defined as the persistence of fluid within the ureteral lumen. 20 A dilated ureter may be recognised on ultrasound as a tortuous tubular structure running from the renal pelvis to the urinary bladder. Underlying causes of dilation include an ectopic ureter (rare in the cat compared with the dog),21–23 pyelonephritis, ascending infection and obstruction. 1 Cats are predisposed to ureteral obstruction on account of their small ureteral lumen, which is around 0.4 mm in diameter. 24
The most common cause of obstruction in this species is ureterolithiasis.6,25,26 The vast majority of ureteral calculi in cats are composed of calcium oxalate and present on ultra-sound as intensely hyperechoic structures within the ureter associated with strong distal acoustic shadowing (Figure 5). 8 The size of the acoustic shadow is related in part to the size of the urolith and very small uroliths may not produce an appreciable shadow. Acoustic shadowing can be maximised by increasing the insonation frequency and adjusting the focal zone to the level of the calculus. 1 Where there is doubt, the ‘twinkling artefact’ can be used to confirm the presence of a urolith.

(a) Ultrasound image from a 10-year-old female neutered British Blue cat presenting with inappetence and weight loss. The ureteral wall is slightly thickened and the lumen is mildly dilated. Towards the termination at the vesicoureteral junction, a hyperechoic ureterolith is identified obstructing the ureter. Note the mild acoustic shadowing distal to the ureterolith (arrows). (b) Same cat as in (a). The renal pelvis is mildly dilated and measures 4.1 mm in maximal diameter. Multiple echogenic calculi (arrows) associated with distal acoustic shadowing are present within the renal pelvic recesses. (c) Hydroureter due to obstructive ureterolithiasis in a 12-year-old female neutered Burmese cat. The ureterolith is large, has a convex echogenic interface and is associated with strong clean distal acoustic shadowing (arrows). Note the reduction in ureteral luminal diameter distal to (to the right of) the ureterolith. A video showing hyperechoic ureteroliths associated with distal acoustic shadowing in the left ureter, which is tortuous and mildly dilated as a result, is available as supplementary material. (d) Severe hydroureter (arrow) and hydronephrosis (arrowhead) in a 6-year-old male neutered Ragdoll presenting with inappetence and abdominal pain due to complete obstruction of the proximal ureter by a ureterolith. A video showing these abnormalities is available as supplementary material. (e) Same cat as in (d). The contralateral ureter (between the arrows and measuring calipers) is very mildly and uniformly dilated, presumably due to compensatory diuresis of the unaffected kidney
This is a phenomenon pertaining to colour Doppler that occurs distal to strongly reflective interfaces such as those due to uroliths and manifests as a mixture of rapidly fluctuating red and blue Doppler signals. 27 Around one-third of cats will have bilateral ureteroliths and many will have additional calculi within the kidney, which have the potential to pass into the ureter. 8 When obstruction is complete, ureteral dilation will end abruptly at the level of the ureterolith. Since it is not uncommon to find more than one ureterolith, the entire ureter should be examined if possible.
The sensitivity of ultrasound for the detection of ureteral calculi in the cat has been reported to be 77%, although a higher sensitivity of around 90% may be achieved if ultrasound is combined with radiography. 8 In a further, much more recent study, ultra-sound was determined to be 98% sensitive for the detection of ureteroliths. 28 In this study, ultrasound examinations were performed by a board-certified veterinary radiologist or a radiology resident under direct supervision, using one of three machines with up to 18 MHz scanning capabilities. 28 Although such details are not given in the earlier study, it is likely that improvements in ultrasound equipment and ultra-sonographer experience in general account for the much higher sensitivity reported in the later study.
Other, less commonly reported causes of ureteral obstruction in the cat have included luminal occlusion owing to blood clots or inflammatory debris,29,30 a congenital ureteral stricture,31,32 acquired ureteral stenosis secondary to ureteral fibrosis, 33 retroperitoneal fibrosis following renal transplantation,34,35 circumcaval ureter or previous ureteral surgery,25,36,37 retroperitoneal infarction 38 and ureteral or retroperitoneal neoplasia (Figure 6).39,40 Despite having a high sensitivity for the detection of ureterolithiasis, ultrasound was found to be poorly sensitive (44%) for the detection of ureteral strictures in one study. 28 More than half of ureteral strictures identified at surgery were misdiagnosed as ureteroliths during pre-operative ultrasound and 5/7 solidified ureteral blood clots detected at surgery were misdiagnosed as either ureteroliths or strictures on ultrasound. Possible reasons suggested for these errors included difficulty differentiating between a small ureterolith lacking an acoustic shadow and a blood clot or stricture, and failure to differentiate an accumulation of debris proximal to a stricture from a ureterolith. The varying echogenicity of blood clots was also suggested as a potential contributing factor, making them easy to miss on ultrasound. 28
Suspected ureteral lymphoma in an 8-year-old male neutered domestic shorthair cat with confirmed lymphoma of the right kidney. (a) The wall of the left ureter is circumferentially and irregularly thickened. (b) Approximately 2 cm distal to the kidney, the thickening progresses to a mass (arrows) that obstructs the ureteral lumen, causing hydroureter and hydronephrosis. Fat surrounding the ureter is moderately hyperechoic
The author has scanned a number of young cats in which a ureter had been inadvertently ligated during ovariohysterectomy, a surgical complication that has been reported in the veterinary literature (Figure 7). 41 Interestingly, bladder neoplasia, which is a relatively common cause of ureteral obstruction in the dog, is rare by comparison in the cat. Although not a direct cause of ureteral obstruction, long-standing urethral outflow obstruction can also result in bilateral ureteral dilation due to a build up of pressure.

Confirmed inadvertent ureteral ligation during ovariohysterectomy surgery in two cats (same cats as in Figure 3). (a) The left ureter of an 18-month-old female neutered domestic shorthair cat is mildly dilated and ends abruptly (arrows) several centimetres distal to the kidney. The ureter distal to this could not be identified. (b) Marked dilation (indicated between the measuring calipers) with an abrupt narrowing (arrows) in the mid-portion of the left ureter of a 7-month-old female neutered domestic shorthair cat. Mild hyperechogenicity of the periureteral fat and a small volume of anechoic retroperitoneal fluid (asterisk) are visible. A severely enlarged left kidney was discovered at a routine vaccination appointment and hydronephrosis was suspected. Inclusion of the mid-body of the left ureter within the previous uterine ligation was confirmed during surgery to remove the left kidney and ureter. (c) Normal right ureter (between the arrows) in the same cat as in (b) for comparison. The measuring calipers span the ureteral lumen
Following initial obstruction, the proximal ureter dilates first. If the obstruction is not relieved, the ureter becomes tortuous and progressively more dilated distally, although the dilation does not extend to the level of the obstruction in all cases. 8 The degree of hydro-ureter will depend upon the completeness and duration of the obstruction. Hyperechoic periureteral fat due to periureteral inflammation may be present at the site of obstruction and there may also be evidence of retroperitoneal effusion (Figure 8). 36
Hyperechoic fat indicative of periureteral inflammation surrounds the left ureter of a 10-year-old male neutered domestic shorthair cat presenting for further investigation of haematuria. Two ureteroliths are visible within the ureter (between the two sets of measuring calipers), causing mild hydroureter proximally. Distal to the ureteroliths, the ureter quickly regains a more normal diameter
Inducing diuresis through the administration of intravenous fluids may be sufficient to encourage ureteroliths to pass into the urinary bladder in some cats. Spontaneous retrograde movement of ureteroliths back into the renal pelvis has also been reported in cats and, therefore, it is always wise to confirm the position of a ureterolith prior to surgery. 42
Scanning the urinary bladder
Ultrasound is the diagnostic modality of choice for imaging the majority of disorders affecting the urinary bladder. 43 The bladder is superficially located and therefore easily accessible, and urine within the lumen provides an excellent acoustic window for imaging the bladder wall. 44 Ultrasound permits evaluation of bladder size, wall thickness and layering, while allowing direct visualisation of serosal and mucosal margins. 45 Additionally, the pericystic region and regional lymph nodes can be assessed and cystocentesis is facilitated under ultrasound guidance.
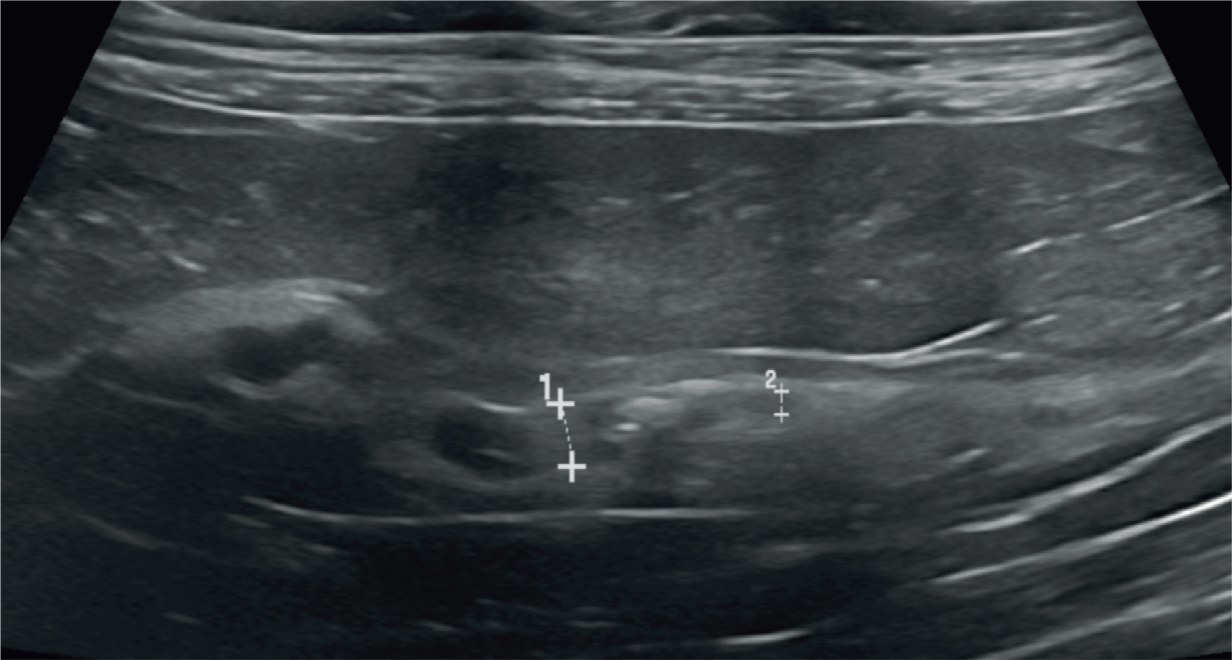
The urinary bladder is located within the caudoventral abdomen and is most easily imaged with the cat in dorsal or lateral recumbency (Figure 9). In dogs, the bladder neck is frequently intrapelvic, particularly when empty, and it can be difficult to access with ultrasound if obscured by the pubic bone. In contrast, the feline urinary bladder tends to remain entirely within the abdomen and, as such, is much easier to scan. As with other abdominal organs, the bladder is scanned in two orthogonal planes, usually sagittal or dorsal and transverse. Ideally, the bladder should be moderately distended to permit a complete and reliable evaluation of the mucosa and wall thickness (Figure 10). Mucosal folding in a minimally distended bladder can result in a nodular undulating mucosal surface, mimicking disease. 44
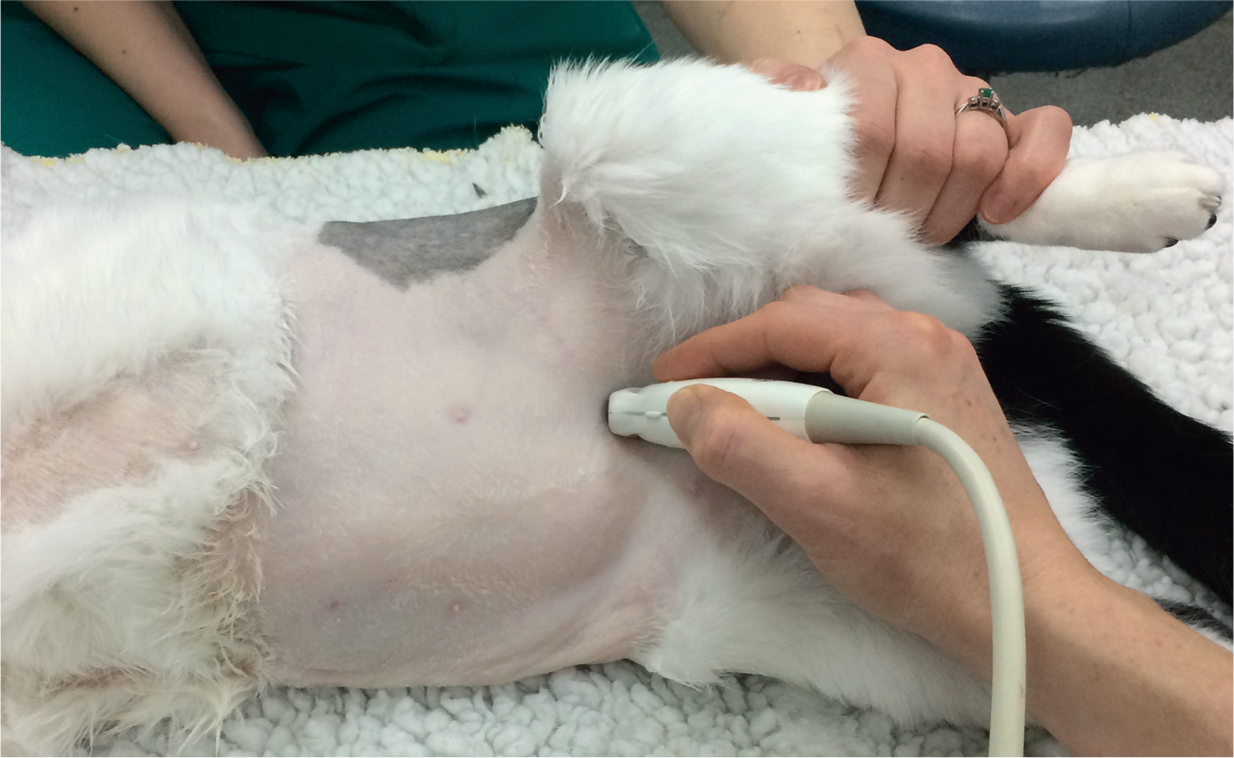
Typical transducer positioning for scanning the urinary bladder. The cat is in right lateral recumbency with the uppermost hindlimb elevated to improve access. An alternative method, which is preferred by some ultrasonographers, is to scan the bladder with the cat in dorsal recumbency

(a–c) Variation in appearance of the normal feline urinary bladder. Mild lipiduria is noted in (c)


Normal appearance of the vesicoureteral junction (arrows)

A jet of urine from the right ureteral papilla is depicted by colour Doppler as a streak of red within the trigone of the bladder

Mild (a), moderate (b) and marked (c) lipiduria in three cats. Suspended echoes are visible in each urinary bladder. In (b) and (c), clumping of echoes is also observed. In each case, there was no evidence of distal acoustic shadowing, reverberation or twinkle artefact to suggest crystalluria

Normal appearance of the bladder trigone (asterisk in images a–c) and urethra (a–d); the latter shown between arrows or measuring calipers
Abnormalities of the urinary bladder
Cystitis
Cystitis is one of the more common indications for scanning the feline bladder. In some cats, there may be no changes visible, particularly when the disease is acute or mild. In chronic cases of cystitis, the bladder wall may be reduced in echogenicity reflecting oedema. Wall thickening due to cystitis is usually most pronounced at the cranioventral aspect of the bladder,1,50 but can become diffuse in severe cases (Figure 15). 44 Diffuse thickening and hyperechogenicity of the bladder wall associated with a loss of layering has been reported in a cat with granulomatous fungal cystitis due to Histoplasma capsulatum infection. 51 Urinary bladder wall thickness should always be assessed in the light of the degree of luminal filling and care should be taken to avoid interpreting the wall of a normal, but empty or partially filled bladder, as being thickened. Intraluminal material representing inflammatory debris may be present. 43 In severe cases of bacterial cystitis, the author has also observed evidence of localised inflammation surrounding the bladder. Emphysematous cystitis has been reported in the cat and describes the presence of gas within the lumen and/or bladder wall due to gas-producing bacteria such as Escherichia coli.11,18,52 On ultrasound, trapped intramural gas results in irregular hyperechoic interfaces associated with distal acoustic shadowing and reverberation. 44 It should be noted that gas is commonly introduced into the bladder lumen following cystocentesis and catheterisation and, therefore, a diagnosis of emphysematous cystitis should ideally be made prior to these procedures, where possible. Repositioning an animal can aid differentiation between luminal and intramural gas, since gas within the bladder lumen is free to move with gravity, whereas gas trapped within the bladder wall remains in situ.
(a) Cystitis in a 13-year-old male neutered domestic shorthair cat with chronic feline lower urinary tract disease including recurrent episodes of urethral obstruction. The bladder wall is thickened and there is a moderate amount of gravity-dependent sediment within the lumen. (b) Chronic cystitis in a 12-year-old male neutered Birman cat. The bladder wall is thickened and irregular. The cranioventral aspect of the wall is particularly severely affected. (c) Chronic cystitis has resulted in severe thickening of the cranial aspect of the urinary bladder (arrows) in this 15-year-old male neutered domestic shorthair cat
Pseudomembranous cystitis has been reported in four cats presenting with acute urine outflow obstruction and post-renal azotaemia. 53 In all cases, ultrasound revealed a thickened bladder wall and compartmentalisation of the lumen due to the presence of thick echogenic dividing septa (Figure 16). 53 Cystotomy was performed in 3/4 cats for diagnostic and therapeutic purposes and the remaining cat was euthanased. At exploratory cystotomy, the ultrasonographic changes corresponded to large pieces of fibrinohaemorrhagic tissue adherent to a severely thickened, haemorrhagic and ulcerated bladder mucosa. 53 It was thought that the septa observed on ultrasound represented sloughing of necrotic regions of the bladder wall into the lumen. All cats recovered uneventfully from surgery. One month after discharge and following a course of antibiotics, the urinary bladder appeared normal on ultrasound in all three cats. A definitive cause of the condition could not be identified and it was not possible to determine whether the cystitis was the cause or result of the obstruction.

Abnormal intraluminal membranes resembling pseudomembranous cystitis, although not confirmed histologically. (a) Ultrasound image of the urinary bladder of a 3-year-old male neutered domestic shorthair cat acquired following alleviation of urethral obstruction. There is marked thickening and irregularity of the cranial bladder wall. A thin, echogenic septum of tissue traverses the cranial bladder lumen, which was thought at the time of imaging to represent mucosal detachment. Fat surrounding the bladder was mildly hyperechoic. A video showing the suspected bladder mucosal separation in this cat is available as supplementary material. (b) Transverse image of the urinary bladder post-obstruction in a 7-year-old male neutered Maine Coon cat. A thick, highly echogenic ring of tissue, also thought to represent mucosal detachment, is present within the bladder lumen. Shadowing echogenic sediment was present within the bladder at the time of imaging. (c) Two days later, repeat ultrasound of the urinary bladder of the cat in (b) revealed resolution of the previously identified abnormalities
Polypoid cystitis is a rare disease of the urinary bladder, characterised by the presence of one or more polypoid or pedunculated masses projecting from the bladder mucosa.54,55 Although ultrasound appearance can be highly suggestive of the diagnosis, histopathology is required to rule out neoplasia. To the author’s knowledge, polypoid cystitis has only been reported in the dog to date. 55
Bladder calculi
As in the rest of the urinary tract, cystoliths have a characteristic strongly echogenic interface associated with clean distal acoustic shadowing on ultrasound (Figure 17). Both radiolucent and radiopaque calculi are visible on ultrasound. It is important to avoid misinterpreting the wall of the colon in transverse view as a calculus. Rotating the transducer by 90º will result in a longitudinal view of the colon, whereas a true calculus will remain unchanged in appearance (Figure 18).

(a) Ammonium urate cystic calculi (arrow) in the bladder of a 4-month-old female domestic shorthair cat with a portosystemic shunt. A moderate amount of gravity-dependent sediment is also present. (b) Calcium oxalate cystic calculi in the bladder of a 16-year-old female neutered domestic shorthair cat. Hyperechoic structures associated with strong clean distal acoustic shadowing (arrows) are present within the dependent aspect of the urinary bladder. (c) Xanthine calculi in the bladder of an 8-year-old female neutered domestic shorthair cat

The distal portion of the descending colon is visible in the far field of the image (colon wall is indicated by the arrow), dorsal to the urinary bladder (arrowheads indicate the bladder wall). Care should be taken not to mistake the hyperechoic interface and distal shadowing of the colon for a stone (asterisks indicate shadowing due to colonic gas)
Urethral outflow obstruction
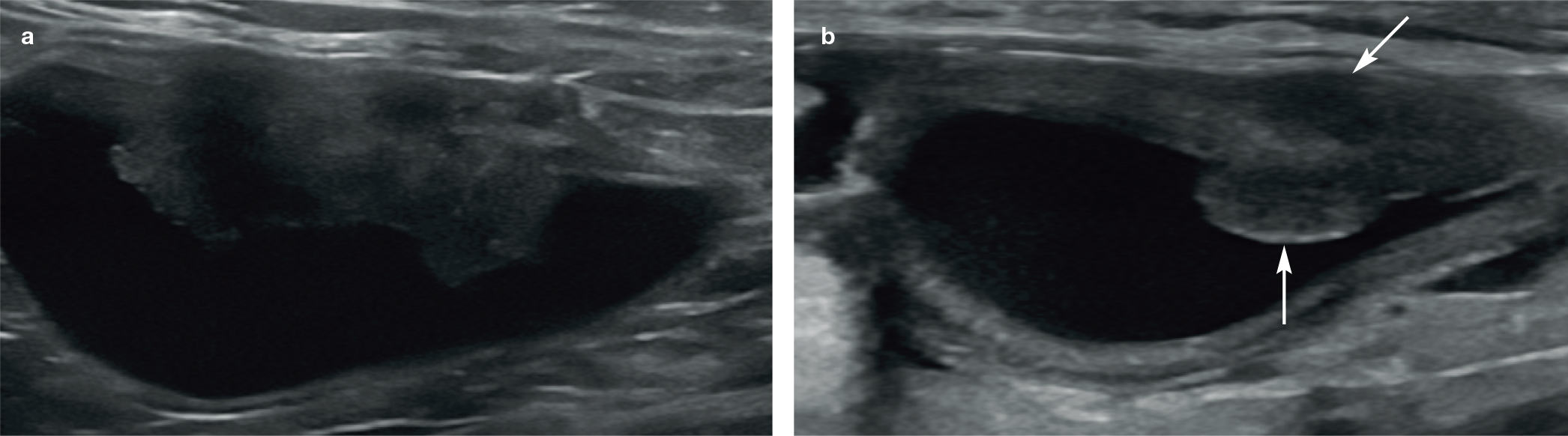
The ultrasonographic findings in 87 cats with confirmed urethral obstruction have been reported. 20 Common abnormalities included bladder wall thickening in almost all cats (89.4%), echogenic urine sediment, pericystic effusion and hyperechogenicity of pericystic fat. 20 It is unclear how the pericystic fluid develops but urine transudation across a severely compromised bladder wall 56 or the development of an aseptic inflammatory effusion 57 have both been suggested. Cystolithiasis was recognised in 41/87 cats (47.1%). 20 In 4/87 cats, large echogenic masses, some of which contained hyperechoic shadowing material, were identified within the bladder lumen and presumed to be blood clots (Figure 19). 20 Follow-up ultrasound was performed in one of these cats 2 weeks later and showed complete resolution of the previously identified mass, supporting the original presumption that this was a blood clot. Thick echogenic septa were present within the bladder lumen of a further four cats resembling the previously reported appearance of pseudomembranous cystitis, although this was not confirmed histologically. 20 Unlike the previous case series, 53 these cats were successfully managed medically. Changes in the appearance of the upper urinary tract were also noted and included renomegaly, pyelectasia, perirenal effusion, hyperechoic perirenal fat and ureteral dilation (Figure 20). 20

Blood clot within the bladder lumen. A non-shadowing echogenic structure is visible within the lumen of the urinary bladder. Note the absence of blood flow within the structure when interrogated with colour Doppler
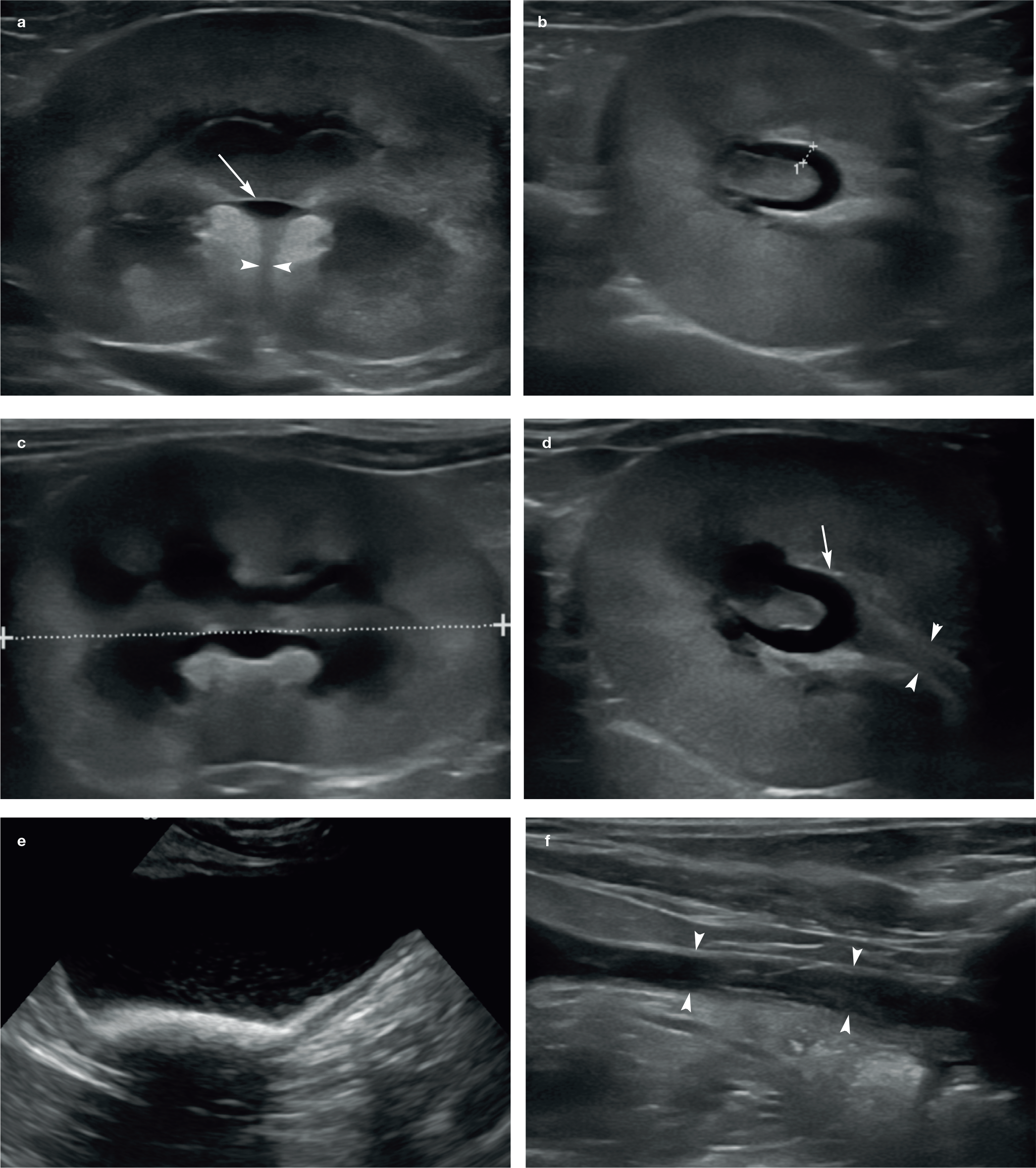
Ultrasonographic findings in a 5-year-old male neutered Persian cat presenting with urethral obstruction and marked hyperkalaemia. (a,b) Left kidney; (c,d) right kidney (indicated between the measuring calipers in [c]). Renomegaly (around 5 cm in length) and mild pyelectasia (arrow in [a] and [d] and measuring calipers in [b]) of both kidneys was observed in association with mild dilation of the ureters (arrowheads in [a] and [d]). (e) A moderate amount of echogenic shadowing sediment is present within the dependent portion of the urinary bladder. A video showing the echogenic bladder sediment in this cat is available as supplementary material. (f) Urethral dilation (arrowheads)
None of the abnormalities described above, in either the upper or lower urinary tract, could be used to predict the likelihood of obstruction recurring. However, the presence of a perirenal effusion was positively associated with severe hyperkalaemia. The authors suggested, therefore, that the identification of perirenal effusion on ultrasound may indicate a more longstanding obstruction and a seriously ill patient. 20
Bladder rupture
Positive contrast retrograde cystography is the preferred choice of imaging modality for the detection of bladder rupture, and is recommended over ultrasound. Refraction artefact (which causes edge shadowing) results in echo dropout and apparent discontinuity of a portion of the curved bladder wall (Figure 21). 3 This is particularly evident in the presence of free peritoneal fluid. Ultrasound-guided abdominocentesis of free peritoneal fluid can be performed to confirm suspected uroabdomen.

Edge shadowing occurs due to refraction of the ultrasound beam as it encounters a curved interface and is recognised on ultrasound as triangular hypoechoic zones (arrowheads). In the presence of free peritoneal fluid, it can create the impression of a defect within the bladder wall (long arrow). A video showing edge-shadowing artefact is available as supplementary material
Neoplasia
Neoplasms of the urinary bladder occur less commonly in cats than in dogs and the majority of those that do occur are malignant and epithelial in origin (Figure 22). 58 Transitional cell carcinoma (TCC), although rare in cats with an estimated prevalence of 0.18%, 59 is the most common malignancy of the bladder in both species and may be more prevalent in male cats. 60 In one study of 20 cats with TCC of the urinary bladder, approximately half of the tumours affected the trigone region with the remainder detected elsewhere in the bladder. 60 In two later studies, involving 20 and 118 cats with histologically or cytologically confirmed TCC, only five and 32, respectively, were trigonal, with the remainder more commonly in the mid-body or apex of the bladder.61,62 Urethral extension was only observed in 15 cats across both studies. This is in contrast to the situation in dogs where TCC has a strong predilection for the trigone region and urethral involvement is common. 63 In dogs, TCC typically appears as a broad-based sessile heterogeneous mass, which may be mineralised. 3 With the exception of location, the appearance of feline bladder TCC is similar to its canine counterpart. In the cats described above,61,62 the most common presentation was that of a solitary, broad-based mass associated with a loss of layering, with or without mineralisation. In a small number of cats, multiple bladder wall masses may be present. 62
(a) A large sessile, heterogeneous mass is visible along the left lateral bladder wall in a 12-year-old male neutered Egyptian Mau cat. There is complete loss of wall layering at the level of the mass. Sampling was declined by the owner. (b) Focal bladder mass (arrows) in a 10-year-old female neutered domestic longhair cat. Cytology from the left kidney was highly suspicious of carcinoma and, therefore, it was hypothesised that the bladder mass was also most likely a carcinoma in origin
Primary fibrosarcoma of the urinary blad‑ der has been described in two female spayed domestic shorthair cats.64,65 In both cases the ultrasonographic description was that of a vas‑ cularised mass of heterogeneous echogenicity arising from the dorsal bladder wall.
Several other tumours have also been reported in the feline urinary bladder including lymphoma, leiomyoma, leiomyosarcoma, adenocarcinoma, squamous cell carcinoma, haemangiosarcoma, rhabdomyosarcoma and malignant peripheral nerve sheath tumour (MPNST).58,66–69 The MPNST had a similar appearance to the fibrosarcomas and also arose from the dorsal bladder wall, emphasising the overlap in the ultrasonographic appearance of different tumours. Lymphoma can arise at any location in the bladder as a broad-based mural mass of mixed echogenicity 66 or as generalised mural thickening, 70 and thus also cannot be differentiated from other tumour types based on ultrasound appearance alone. Whenever neoplasia is suspected, it is important to assess the medial iliac lymph nodes which drain this region for any evidence of metastatic disease.
Uncommon conditions of the bladder
Vesicourachal diverticulum
Vesicourachal diverticula are seen occasionally in the cat and, while they may be asymptomatic, they can predispose to recurrent bacterial urinary tract infections. 71 They represent congenital anomalies that result from failure of closure of the urachus located at the bladder vertex. 72 On ultrasound, they present as a convex outpouching of the bladder lumen resulting in an abnormally pointed appearance, or as a focal depression within the bladder wall; they are most commonly identified in the cranioventral aspect (vertex) of the bladder.3,46
Foreign bodies
Intravesicular foreign bodies are rare but have been reported in cats.73,74 A grass awn has been described within the urinary bladder of a 10-year-old female neutered domestic longhair cat. 73 The cat was presented for investigation of a 2-day history of stranguria and had a small bladder on abdominal palpation. An ultrasound examination revealed the presence of a 1.3 cm linear V-shaped hyperechoic foreign body within the dependent portion of the bladder. 73 A grass awn was removed at cystotomy and was thought to have gained entry to the bladder via retrograde migration from the urethral opening.
Bladder inversion
Partial inversion of the urinary bladder has been described in a 6-month-old female domestic shorthair cat. 75 The cat was initially presented at 4 months of age with a history of haematuria, stranguria and inappropriate urination, and treated for a urinary tract infection. The cat was subsequently re-presented 2 months later with similar clinical signs. An abdominal ultrasound examination was performed and revealed the presence of a 2.2 x 2.2 x 1.4 cm multilayered mass within the cranial aspect of the urinary bladder. Unusually, the cranial apex of the bladder was blunted and indented centrally. The outer hyperechoic serosal layer could be followed caudally from the point of indentation into the centre of the mass. Colour Doppler ultrasonography was used to confirm the presence of blood flow within the mass. Anechoic urine was observed within the lumen immediately caudal to the mass. Based on the ultrasound appearance, a presumptive diagnosis of bladder inversion was made and later confirmed during cystotomy. Following a partial cystectomy to remove the inverted tissue and a course of antibiotics for a concurrent urinary tract infection, all clinical signs resolved.
While a definitive cause could not be determined, it was hypothesised that the stranguria resulting from the first urinary tract infection could have triggered the partial bladder inversion due to increased intraabdominal pressure. This hypothesis is based on the observation that bladder inversion is most commonly reported following parturition in other species, presumably due to the powerful abdominal contractions involved in this event. 75

Urinary bladder duplication
Urinary bladder duplication is a rare congenital condition that has been reported in humans, dogs and in a 4-month-old female American Curl cat.76–80 The cat was presented for further investigation of chronic, intermittent antibiotic-responsive urinary incontinence and chronic renal disease. 80 An abdominal ultrasound revealed dilation of both ureters and renal pelvises in addition to three cavitary structures within the caudal abdomen. All three structures were thin-walled and fluid-filled and contained smooth muscle and mucosa on histology, consistent with bladder duplication. 80


Key Points
Mild pelvic dilation up to around 3.5 mm may be present in cats with clinically normal renal function and in cats with clinically normal renal function undergoing diuresis.
Pelvic dilation ⩾3.5 mm should be regarded as potentially abnormal and further investigation considered.
Many cats with CKD will have evidence of pyelectasia which can be mild to moderate (renal pelvic diameter up to 11.5 mm recorded to date).
Pelvic dilation ⩾13 mm is suggestive of an outflow obstruction.
The most common cause of ureteral obstruction in the cat is ureterolithiasis.
Non-shadowing echoes suspended within the lumen of the urinary bladder may represent lipiduria.
Cystitis typically results in bladder wall thickening that is most marked cranioventrally.
Cats presenting with urethral obstruction may have ultrasonographic evidence of bladder wall thickening, echogenic urine sediment, pericystic effusion, hyperechogenicity of pericystic fat, cystolithiasis and mucosal separation.
Transitional cell carcinoma is the most common bladder tumour in the cat, though less common than in the dog, and does not appear to have as strong a predilection for the trigone region.
Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not necessarily required.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.