
Abstract
Objectives
The aim of this study was to compare four inflation techniques on endotracheal tube cuff (ETC) pressure using a feline airway simulator.
Methods
Ten participants used four different endotracheal cuff inflation techniques to inflate the cuff of a low-pressure, high-volume endotracheal tube within a feline airway simulator. The simulator replicated an average-sized feline trachea, intubated with a 4.5 mm endotracheal tube, connected to a circle breathing system and pressure-controlled ventilation with oxygen and medical air. Participants inflated the ETC: by pilot balloon palpation (P); by instilling the minimum occlusive volume (MOV) required for loss of airway leaks during mechanical ventilation; until a passive release of pressure with use of a loss-of-resistance syringe (LOR); and with use of a syringe with a digital pressure reader (D) specifically designed for endotracheal cuff inflation. Intracuff pressure was measured by a manometer obscured to participants. The ideal pressure was considered to be between 20 and 30 cmH2O. Data were analysed by Shapiro–Wilk, Kruskal–Wallis and χ2 tests, as appropriate.
Results
Participants were eight veterinarians and two veterinary nurses with additional training in anaesthesia. Measured median intracuff pressures for P, MOV, LOR and D, respectively, were 25 cmH2O (range 4–74 cmH2O), 41 cmH2O (range 4–70 cmH2O), 31 cmH2O (range 18–64 cmH2O) and 22 cmH2O (range 20–30 cmH2O). D performed significantly better (P <0.001) than all other techniques, with no difference between the other techniques.
Conclusions and relevance
Use of D for cuff inflation achieved optimal cuff pressures. There may be high operator-dependent variability in the cuff pressures achieved with the use of P, MOV or LOR inflation techniques. As such, a cuff manometer is recommended when using any of these techniques.
Introduction
General anaesthesia of small animals is routinely performed with the use of an endotracheal tube (ETT). The tube provides patency of the patient’s airway enabling the delivery of anaesthetic gases and the provision of ventilation. Inflation of the endotracheal tube cuff (ETC) is performed to provide a seal between the tube and the trachea, preventing air or fluid leakage around the tube (underinflation). Cuff inflation must be of an appropriate pressure to provide this seal without any damage to the tracheal mucosa (overinflation). Inflation itself is therefore a secondary skill of endotracheal intubation. Currently, there are no standardised guidelines for appropriate ETC pressures in veterinary, or human, anaesthesia practice. Most of the relevant literature refers to human practice, recommending an intracuff pressure range between 20 and 30 cmH2O.1–7 However, the normal values range from as low as 14 cmH2O to as high as 40 cmH2O.8,9 To date, there are no feline-specific recommendations.
Endotracheal intubation has been reported to increase the risk of death in cats.10,11 Further to this, cats are overrepresented for cases of tracheal rupture following ETC hyperinflation.12–14 Tracheal rupture carries significant morbidity, and potential mortality, requiring intensive therapy to achieve recovery. 13 Therefore, appropriate ETC inflation in this species is essential.
Multiple ETC inflation techniques have been described in the veterinary literature.15–17 However, there is no information about the popularity of each technique. Palpation and minimum occlusive volume are two commonly performed techniques. When using the palpation technique (P), the operator palpates the pilot balloon to estimate the pressure within it, using this as an approximation of the pressure within the cuff, as both are connected and inflate concurrently by design. 18 The minimum occlusive volume technique (MOV) requires the operator to inflate the ETC until the point of loss of audible air leakage around the cuff, during the inspiratory phase of ventilation. If ventilation is performed manually then there is a recommendation to maintain an airway pressure of 20–30 cmH2O. 16 Lately, the loss-of-resistance technique (LOR) has been tested in human anaesthesia.19–21 In this case, the operator uses a plastic loss-of-resistance syringe to temporarily overinflate the cuff and then allow the passive release of excess pressure. More recently, a novel syringe device with digital pressure indicator has become available (AG Cuffill; Provet). Use of the digital syringe technique (D) has not been reported in veterinary species; however, good correlation between the syringe and the gold standard of a manometer has been shown in human practice. 22 The operator attaches the syringe to the pilot balloon and instils air to the desired pressure, as read on the digital screen of the syringe plunger.
The use of simulators is becoming increasingly common in many disciplines of human and veterinary medical training. The use of simulators for ETC inflation testing and training has been reported previously in human23,24 and veterinary 25 literature. Basic tracheal simulators can be easy to construct, allowing clinicians to develop the skills required for appropriate cuff inflation, without the use of live animals. Given the previously mentioned complications that may occur in cats, the use of a feline airway simulator (FAS) might play an important role in the training of veterinarians and veterinary nurses.
The aim of this study was to compare four different ETC inflation techniques through use of an FAS. We hypothesised that inflation with the use of D would provide an accurate method of cuff inflation. P, MOV and LOR were hypothesised to be less reliable at achieving intracuff pressures in the recommended range owing to the subjective nature of each technique.
Materials and methods
This prospective study was conducted at the University Veterinary Teaching Hospital of the University of Sydney. Ten members of the anaesthesia service were recruited (eight veterinarians and two veterinary nurses). Participation in the study was voluntary, with all participants giving oral consent prior to enrollment.
The FAS was built as previously described. 25 The FAS was intubated with a 4.5 mm ETT (Microcuff Paediatric Endotracheal Tube 4.5 mm; Halyard), connected to a paediatric circle breathing system (SW Low Volume Breathing Circuit; Darvall) with a 1 l reservoir bag connected to an anaesthetic machine with internal ventilator (GE Datex-Ohmeda Aespire 7900; GE Healthcare). The ETT pilot balloon was directly connected to a manometer (Cuff Pressure Monitor, NS 60-TBS-CP; Instrumentation Industries), allowing the measurement of intracuff pressure after its inflation. The accuracy of the manometer was confirmed prior to the beginning of the study, via calibration with a water manometer.
Each participant performed each cuff inflation technique once. The anaesthetic machine flowmeter was set to deliver 1 l of oxygen, and 1 l of medical air, per min. Rates were chosen so as to prevent leakage from the ventilator bellow during the periods of cuff deflation. Pressure-controlled mechanical ventilation was performed with a peak inspiratory pressure of 20 cmH2O, a respiratory rate of 15, an inspiratory to expiratory ratio of 1:3 and no positive end-expiratory pressure. The ETC was deflated prior to the beginning of each cuff inflation, as confirmed by a manometer reading of 0 cmH2O. The manometer’s gauge was turned away from participants so they could not read the pressure values at any time, thus simulating a clinical setting where an ETC pilot balloon pressure gauge is not available. A new 3 ml syringe (3 ml BD slip tip syringe; BD) was provided for cuff inflation. This size of syringe is routinely used for feline ETC inflation in our clinic and previously tested to be optimal for use with the FAS.
The participants were instructed to perform ETC inflation, first with the use of MOV, listening for loss of audible airflow around the cuff during mechanical ventilation. The participant was instructed to inflate the cuff slowly (at an approximate rate of no more than 0.3 ml/s), with the end point occurring at loss of an audible air leak without the use of a hearing aid (eg, stethoscope). When the participant was satisfied they had achieved loss of audible inspiratory cuff leak, the technique was considered complete. The participant was instructed to not touch the pilot balloon during this first task. The cuff manometer was then turned and the intracuff pressure recorded. The manometer was reset by disconnecting it from the ETT and confirmed by a 0 cmH2O intracuff pressure reading.
For the second part, participants were instructed to inflate the ETC using P, palpating the pilot balloon while inflating the ETC. The experiment was considered complete when the participant was satisfied with the palpation pressure of the pilot balloon. At this point, the intracuff pressure was recorded.
Participants were then instructed to use LOR with use of a low-resistance syringe (Perifix LOR 10 ml; B-Braun) by temporarily overinflating the cuff and then allowing the passive release of all excess air (plunger stops moving). Once the inflator was satisfied they had reached this point they were instructed to disconnect the syringe, and the cuff manometer was read and the value recorded.
For the final technique, participants were asked to use D (AG Cuffill; Provet) to inflate the cuff. Participants were instructed to aim for a pressure anywhere between the recommended range of 20–30 cmH2O. Once participants were satisfied with the digital syringe reading they were instructed to once again disconnect the syringe from the manometer valve so the instructors could record the intracuff pressure reading.
Participants remained blinded to manometer readings at all times. Intracuff pressures were manually recorded at the completion of each technique, for each participant.
A sample size calculation was performed using the results obtained in a previous study. 25 A sample of 40 observations was considered adequate to detect a difference of 30% in the proportion of participants successfully reaching 20–30 cmH2O with one of the techniques, using a power of 80% and 95% level of significance. The data were analysed for normality with the Shapiro–Wilk test. Intracuff pressures between techniques were analysed with the Kruskal–Wallis test. The data were then classified into three categories: underinflation (<20 cmH2O); optimal inflation (between 20 and 30 cmH2O); and/or overinflation (>30 cmH2O). The categories were compared between techniques using the χ2 test. Finally, the results were also classified into overinflation (>30 cmH2O) or not (⩽30 cmH2O), and the groups were compared using these categories. In all cases, differences were considered significant at the P <0.05 level. All data are presented as median (range). All the statistical analyses, including the sample size calculation, were carried out using R V3.3.2 Mac OS (The R Foundation for Statistical Computing, http://www.r-project.org).
Results
All participants completed all experiments in full. Two experiments had to be repeated, both owing to operator failure (participant 3 [MOV], participant 5 [P]) when using the equipment. All repeats immediately followed the initial attempt. No data were recorded from the failed attempts.
The intracuff pressure values were not normally distributed (Figure 1). There was no difference in intracuff pressure achieved between techniques. Table 1 shows median intracuff inflation pressures for each inflation technique, and the percentage of users in each category (underinflation, optimal inflation and overinflation). There was a significant difference between D and other methods, with D performing best (P = 0.001). All users inflated the cuff within the optimal pressure range when using D. When this technique was excluded from the analysis, there was no difference between the other three techniques. Table 2 shows the percentage of users over-inflating, or not, for each technique. Again, there was a significant difference between D and the other three techniques (P = 0.016). When D was removed from the analysis, there was again no difference between the remaining techniques. D always produced inflation pressures within the optimal range. P group had the greatest percentage of users not overinflating, while MOV had a tendency towards overinflation, with no users achieving optimal pressures with this technique. Half of the users overinflated with LOR.

Pressure ranges, interquartile difference and median pressure (shadowed line) for each technique are shown (cmH2O).
Median intracuff inflation pressures for each inflation technique, and the percentage of users in each category*
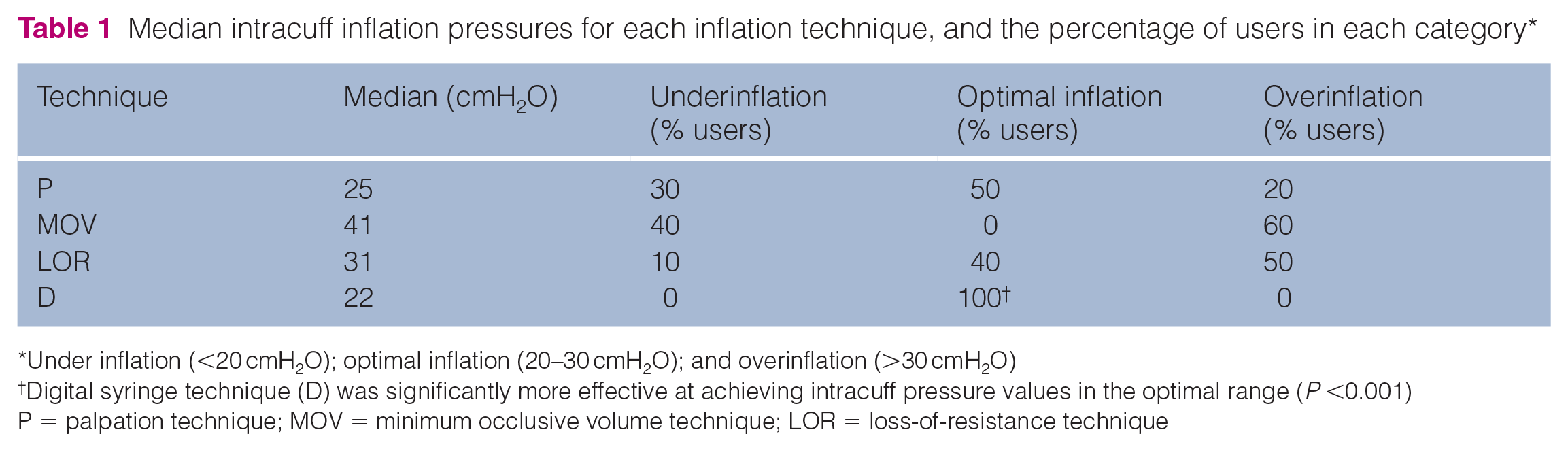
Under inflation (<20 cmH2O); optimal inflation (20–30 cmH2O); and overinflation (>30 cmH2O)
Digital syringe technique (D) was significantly more effective at achieving intracuff pressure values in the optimal range (P <0.001)
P = palpation technique; MOV = minimum occlusive volume technique; LOR = loss-of-resistance technique
Percentage of users, for each technique, overinflating (>30 cmH2O) or not overinflating (⩽30 cmH2O) the endotracheal cuff

Percentage of user not overinflating was significant for the digital syringe technique (D) compared with other methods (P <0.016)
P = palpation technique; MOV = minimum occlusive volume technique; LOR = loss-of-resistance technique
Discussion
The primary aim of this study was to compare four ETC inflation techniques, through the use of a simulator. Inflation with D, specifically designed for cuff inflation, provided the most effective method of cuff inflation to achieve intracuff pressures within the recommended pressure range of 20–30 cmH2O. D has been reported to achieve good correlation with a manometer when used in people. 22 These syringes are more expensive to purchase than the other techniques tested here, with either single-patient use and/or a maximum of 100 inflations being recommended by the manufacturer. This expense may be a significant contributing factor for the syringes not being currently routinely used. The other three techniques all performed poorly at achieving intracuff pressures in the ideal range, with no significant difference found between these techniques.
A pressure range is recommended for intracuff pressure to prevent underinflation of the cuff, as well as overinflation. Underinflation carries the risk of aspiration; for example, if the patient experiences gastro-oesophageal reflux, or from the oral flushing that occurs during a dental procedure. Overinflation is cautioned against to prevent tracheal mucosal damage and, more extremely, tracheal rupture. In humans, the incidence of sore throat is commonly cited as a consequence of tracheal mucosal injury secondary to an overinflated cuff.2,26,27 It is likely that veterinary patients also experience a sore throat after being intubated with an overinflated cuff, but it is very difficult to ascertain. Cats have been reported to have very low incidences of both gastro-oesophageal reflux and even lower, or no, incidence of regurgitation.28,29 Conversely, cats appear over-represented for incidences of tracheal rupture.12–14 When considering endotracheal cuff inflation in cats, an upper pressure limit, rather than pressure range, may be more appropriate.
The results of this study show that when the intracuff pressures achieved are classified as either ‘overinflation’ or ‘not overinflation’, D performed best with no users overinflating the cuff. Only two operators overinflated with the use of P vs six when using MOV and five with LOR.
White et al also reported a tendency to underinflate for P, with the use of the same simulator. 25 P is consistently reported to be an inaccurate cuff inflation technique, with overinflation frequently reported in both simulator-based and in vivo human and veterinary models.15,17,21,30,31 Pisano et al postulated that P is frequently reported to be an inaccurate technique because the smaller radius of the pilot balloon creates a lower wall tension (Law of Laplace) when compared with the larger endotracheal cuff; therefore, predisposing to overinflation. 32 This theory may, in fact, also explain the tendency for underinflation seen in the current study as the ETT used (Microcuff Paediatric Endotracheal Tube 4.5 mm; Halyard) has a cuff that is smaller than the pilot balloon. A recent study reported that use of P for cuff inflation in 40 cats, intubated with two different types of ETT, resulted in overinflation with mean ± SD pressures of 36 ± 14 cmH2O and 46 ± 13 cmH2O. 17 The ETTs used in that study (different from the type used here) appear to have the cuffs larger than the pilot balloons.
ETT model and cuff characteristics have been shown to affect intracuff pressures and this must be considered when comparing the same technique with use of varying ETTs. 33 Low-pressure, high-volume (LPHV) cuffs provide an airway seal at a lower pressure than cuffs that are high pressure, low volume. 34 Intuitively, a LPHV cuff is therefore safer with regard to cuff hyperinflation; however, Mitchell et al found no difference in the number of cats with tracheal rupture secondary to each cuff type. 13 Pilot balloon shape also differs between ETT models, with pilot balloon shape reported to significantly affect the ability of experienced human anaesthetists to predict intracuff pressure using P. 35
The current study used a single ETT type, eliminating any bias due to varying tube characteristics. A clinical study of 174 children intubated with ETT sizes 3.0–6.0 mm showed similar results to the current study; P was used for initial cuff inflation, with a tendency to not overinflate the cuff reported for all tube sizes, with overinflation considered to be >25 cmH2O. 36 The use of a small-size inflation syringe (3 ml) in the current study is likely to also lend itself towards not overinflating. Khan et al tested P in intubated humans with use of 10 ml and 20 ml syringes, and showed that both resulted in overinflation; however, the 20 ml syringe resulted in the highest cuff pressures. 31
LOR is a recently reported technique for ETC inflation in humans, with no reports in the veterinary literature.19–21 The loss-of-resistance syringes are commonly used in medical anaesthesia, as LOR is one of the most commonly used techniques for identification of the epidural space. 37 Bulamba et al reported that LOR performed significantly better than P when inflating ETCs in humans, with 66% of inflations within the recommended range vs only 23% when using P. 21 Jin et al reported 56–63% cuff inflation pressures in the ideal pressure range with use of LOR. 38 In the current study, LOR performed poorly. This type of syringe is more rarely used in veterinary anaesthesia and this lack of familiarity may have contributed to the poor results obtained with this method. The large size of these syringes (10 ml) is also likely to have contributed to the tendency for overinflation, as previously described.
MOV also performed poorly in this study, with no operators providing cuff pressures in the optimal range with its use. This technique is commonly used at our institution and, as such, these results are concerning, with more operators overinflating than not. Previous reports of MOV with the use of an FAS showed experienced clinicians had a tendency towards overinflation while students had a tendency towards underinflation. 25 Only experienced clinicians were included in the current study and this might explain the result obtained. Bird et al also used MOV for cuff inflation in their feline clinical study and reported significant cuff overinflation with pressures of 56 ± 28 cmH2O and 66 ± 25 cmH2O. 17 Prasse et al found that a cuff pressure of 20 cmH2O did not prevent air leakage around the ETT when cats were being mechanically ventilated. 39 In the current study this leakage was not measured, so it is possible that a pressure >20 cmH2O was needed to prevent the leakage. In that case, maybe those operators inflating more than the recommended range may have truly achieved the ultimate purpose of the technique (the prevention of air leakage). MOV also tends to lead to overinflation in dogs and people.15,40 However, underinflation has also been reported in humans and in inexperienced operators with the FAS, as previously mentioned.25,30
The use of a simulator, compared with a live animal, is a limitation of this study, with a possible predisposition to cuff underinflation with P. The simulated trachea in the FAS was a larger ETT. This tube is likely to be less compliant than an in vivo trachea, and this difference may affect pressure palpated within the pilot balloon. The plastic casing and hollow nature of the simulator may have made auscultation of any leak around the ETT difficult to differentiate from the sound of air travelling through the ETT and artificial lung. Participants were advised to listen carefully prior to inflating the cuff for MOV to differentiate the two sounds, in an attempt to reduce any bias from this limitation. Furthermore, the use of a mechanical ventilator to provide breaths during this study provided additional background noise that may have affected the user’s ability to hear a leak.
Conclusions
Direct measurement of intracuff pressures with use of a manometer is the gold standard to consistently provide ETC inflation pressures within the recommended pressure range. In the current study, the use of D produced consistent pressures in the ideal range with use of an FAS. P, MOV and LOR did not consistently produce results in the ideal range and, as such, their use should only be supported with the use of a manometer. Cats are over-represented for tracheal rupture, but rarely reported to experience gastro-oesophageal reflux and regurgitation. Consequently, preventing the overinflation of a feline ETC may be more clinically relevant than preventing underinflation. P showed a tendency for underinflation and may present the best method of cuff inflation in a cat when a manometer or digital syringe are not available; however, studies using different types of ETTs and cuff shapes are required. The use of D for feline ETT cuff inflation appears to be promising; further investigations using them in live models are recommended.
Footnotes
Acknowledgements
The authors would like to thank the staff of the Department of Veterinary Anaesthesia at the University Veterinary Teaching Hospital (The University of Sydney) for their collaboration during the data collection.
Conflict of interest
The authors declare no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not required.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.