
Abstract
Endotracheal intubation was carried out in 11 common marmosets (Callithrix jacchus). A commercially available tilting stand and a Miller laryngoscope blade were used to visualize the larynx. Anaesthesia was induced with alphaxalone (10.6 ± 1.6 mg/kg intramuscularly, followed by 3.2 ± 1.2 mg/kg intravenously). The diameter of the proximal trachea easily fitted an endotracheal tube made from readily available material (a 12 G ‘over the needle’ catheter). Once the tip of the endotracheal tube was at the level of the vocal folds, the tube had to be gently rotated through a 180° angle in order to pass through the larynx into the trachea. Assessment of the dimensions of the larynx and trachea, and comparison with external anatomical features of the animals (n = 10) showed that the length of the trachea could be predicted by multiplying the craniosacral length of the marmoset by a factor of 0.42.
Indications for endotracheal intubation include: maintaining a patent airway access, efficiently delivering oxygen or inhalant anesthetics to the lungs, and applying positive pressure ventilation. 1 As a result, endotracheal intubation should be part of standard anaesthetic care. If the endotracheal tube is of appropriate length and positioned correctly, it will also minimize the anatomical deadspace. This is especially important when anaesthetizing smaller animals, since their tidal volumes are relatively low. To minimize dead space the length of the endotracheal tube should be estimated prior to intubation. Aside from adding dead space, an excessively long tube may lead to endobronchial intubation and ventilation of only one lung. 2 This can result in atelectasis and collapse of the contralateral lung and hypoxaemia. However, if the tube is too short, this increases the risk of accidental extubation.
When the endotracheal tube is used to deliver inhalant anaesthesia it is important to ensure a reasonably tight seal between the tube and the tracheal wall in order to decrease anaesthetic gas leakage and room pollution. A potential disadvantage of intubation is that inevitably this will result in a narrowing of the airway diameter. In smaller animals, this can have a significant effect on the resistance to the gas flow, since for a laminar gas flow the resistance is inversely proportional to the fourth power of the radius of the tube. Hence an ideal endotracheal tube has its length determined by the anatomical characteristics of the animal, and with the maximal internal diameter possible.
Marmosets may require anaesthesia for a variety of reasons, and there is no purpose-made commercially available endotracheal tube suitable for use in this species. Oral endotracheal intubation for marmosets has been described using a 5 French urinary catheter. 3 The authors reported that intubation could be easily performed if an assistant accurately positioned the head. Here we describe an alternative method of endotracheal intubation for marmosets using a commercially available tilting workstand. This workstand facilitates accurate positioning of the head of the animal and allows intubation to be performed by a single operator. In order to assist research workers in determining the appropriate diameter and length of the endotracheal tube, we also describe the dimensions and anatomical features of the larynx and trachea of the common marmoset.
Materials and methods
Endotracheal tube
A 14 and 12 G ‘over the needle intravenous catheter’ (Becton and Dickinson, Madrid, Spain) were customized and used as endotracheal tubes (Figure 1). A small length of silastic tubing was positioned around the proximal end of the catheter, extending to 3 cm from the tip. The tracheal end of the tube was bevelled at an approximately 40° angle and on the 14 G-based tubes a Murphy eye was created on the opposite side of the bevel.
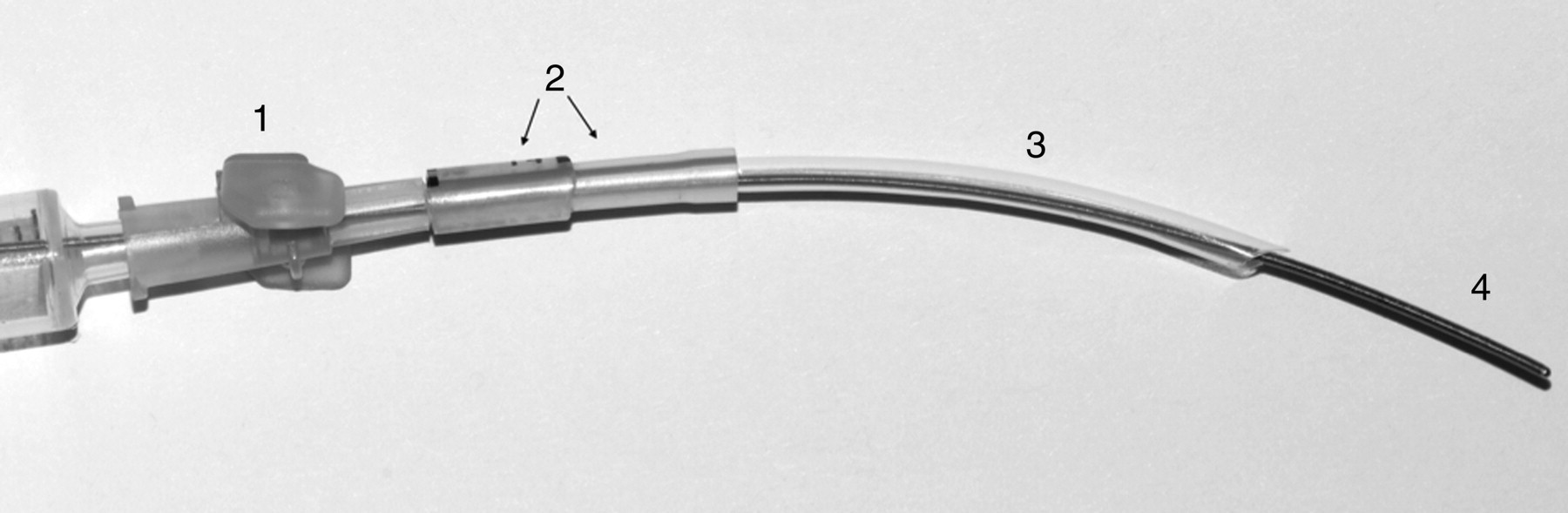
Twelve gauge over the needle catheter customized for use as endotracheal tube: (1) head of the catheter, (2) silastic tubing, (3) body of the catheter and (4) syringe mounted blunt metal introducer
Eleven common marmosets (Callithrix jacchus) were obtained from a non-commercial breeder (Medical Research Council, Edinburgh, UK) and used for an unrelated project ethically reviewed at Newcastle University and compliant with the UK legislation for the protection of animals used for experimental or other scientific purposes (Animal Scientific Procedure Act 1986).
The marmosets were housed in groups in purpose-built caging (2 × 1.22 × 1.10 m). Stocking densities complied with UK Home Office Codes of Practice. Animals were fed a commercial diet (SDS expanded diet, Essex, UK), with supplements of fruits, seeds and muesli to provide additional environmental enrichment. Room temperatures were maintained at 25 ± 2°C, relative humidity 55 ± 10% and the rooms had 12–15 air changes per hour. All animals appeared clinically normal, but no health screening for potential pathogens was undertaken. When anaesthetized (2–8 weeks after arrival in the unit), animals weighed 374 ± 47 g. Their ages ranged from 18 months to seven years old.
Six of the marmosets were anaesthetized in the morning, five in the afternoon.
Alphaxalone (Alfaxan®, Vetoquinol, Buckingham, UK) at 10 mg/kg was administered intramuscularly to provide initial sedation. The quality of the sedation was subjectively assessed based on the degree of muscle relaxation and level of arousal of the animal 5 min after the injection (poor, good or profound sedation). A 22 G ‘over the needle’ intravenous catheter was placed in one of the lateral tail veins. Additional alphaxalone was administered intravenously, to effect, to induce a medium plane of surgical anaesthesia, assessed by loss of the pedal withdrawal reflex and relaxation of the jaw. The marmosets were then positioned in dorsal recumbency on the tilting workstand (Tilting WorkStand, Hallowell EMC, Pittsfield, MA, USA) and held in this position with an elastic band positioned on the lingual side of the canines. The workstand was then tilted to position the animal at a 45° angle. The change in workstand position resulted in extension of the head and neck (Figure 2). A laryngoscope with a Miller 0 blade was used to visualize the epiglottis and the entry of the larynx. Two milligrams of lidocaine were sprayed on the entry of the larynx before any intubation attempt. Oxygen was administered for 1–2 min and the depth of anaesthesia assessed by the operator based on the jaw tone, absence of gag reflex and general muscle relaxation. When the depth of anaesthesia was assessed as adequate, the endotracheal tube was guided into the larynx using a blunt, flexible metal introducer (a modified Seldinger catheter wire). The tube was advanced so that the end of the outer silastic tubing was positioned immediately in front of the larynx. The tube positioning and respiratory gas movement were checked by observation of condensation on a mirror.

Positioning of the marmoset on the table for intubation
The total dose of alfaxalone received by the animal, the number of coughs during intubation, the number of attempt before successful intubation and the size of the catheter used were recorded.
Anatomical data
A total of 10 marmosets were euthanized as part of research projects that were unrelated to the present report. At postmortem examination, a thoracotomy was performed and the heart removed in order to expose the trachea and its bifurcation. The ventral neck was dissected to expose the cervical trachea and the ventral side of the larynx. The distances from the tracheal bifurcation to the thyroid cartilage of the larynx; from the thyroid cartilage of the larynx to the external nostril; from the sacrum (base of the tail) to the occiput; and from the sacrum to the cranium (top of the parietal bone) were recorded. The ratio of nose to tracheal bifurcation with craniosacral distance (NTB/CS) and nose to tracheal bifurcation with occipitosacral (NTB/OS) length were also calculated. The shape and diameter of the trachea were also measured based on photographs taken in situ.
Sagittal sections of the larynx were performed and photographed in four animals. The diameter of the proximal trachea at the level of the third cartilage ring and the angle formed by the larynx over the trachea were measured using Photoshop (Photoshop CS3, Adobe System Inc, San Jose, CA, USA).
Data analysis
All statistical analyses were carried out using SPSS software (Version 18, SPSS Inc, Chicago, IL, USA). All data are presented as means ±1 standard deviation, except the NTB/CS and NTB/OS ratios that were means ±95% confidence intervals (CIs) are presented. Bland–Altman plots 4 were produced in order to assess the level of agreement between estimated (using ratio of NTB/CS or NTB/OS) and actual measurement of the nose to tracheal bifurcation. Following this plot, a one-sample t-test was carried out to test whether there was a significant difference between the estimated and actual distance between the nose and tracheal bifurvation.
Results
Endotracheal intubation
The animals received a mean dose of 10.6 ± 1.6 mg/kg of alphaxalone intramuscularly for premedication and an induction dose of 3.2 ± 1.2 mg/kg intravenously. The degree of sedation was judged as good for nine of the marmosets and profound for the remaining two. One marmoset had an episode of apnoea a few minutes after intramuscular administration of alphaxalone but spontaneous respiration recommenced within 2 min, during which time manual chest compression was undertaken. A total of three marmosets required an additional 1.1–2.9 mg/kg of alphaxalone intramuscularly to provide sufficient depth and duration of sedation to enable tail vein catheter placement.
The head and neck extension of the marmosets positioned on the tilting workstand enabled a clear view of the larynx, and there was no need for position adjustment or for an assistant to hold the animal (Figure 2). The jaw tone was decreased sufficiently to allow good access to the buccal cavity and clear visualization of the entrance to the larynx. With the marmoset in dorsal recumbency on the workstand, the tip of the blade was positioned under the prominent epiglottis and gentle pressure applied to displace the tongue upwards. This manipulation, in combination with the head and neck extension resulting from the animal's position on the workstand, allowed the creation of a new (non-anatomical) visual axis and direct visualization from the operator's eye to the larynx (Figure 3). Intubation was successful at the first attempt in seven marmosets, with a second attempt required in the remaining four. Nine marmosets were intubated with a 14 G tube and two marmosets with a 12 G tube.

View of the entry of the larynx (prominent epiglottis and arytenoids) obtained by gentle depression of the tongue with a Miller blade size 0
Anatomical data
A total of 10 marmosets underwent thoracotomy postmortem and upper airway dissection. Data for the various anatomical features are summarized in Table 1. The epiglottis was prominent and overlapped the ventral insertion of two thick arytenoid cartilages (Figure 4). A sagittal section of the larynx was performed in four marmosets. On the sagittal view, all the usual anatomical structures of the mammalian larynx were identified (Figure 5). The sagittal view also illustrated the laryngotracheal angle made by the successive anatomical structures. This angle on an isolated larynx, freely positioned on the dissection board, was 137 ± 10°. The internal diameter of the trachea, measured at the third tracheal ring, was 4.8 ± 0.2 mm.
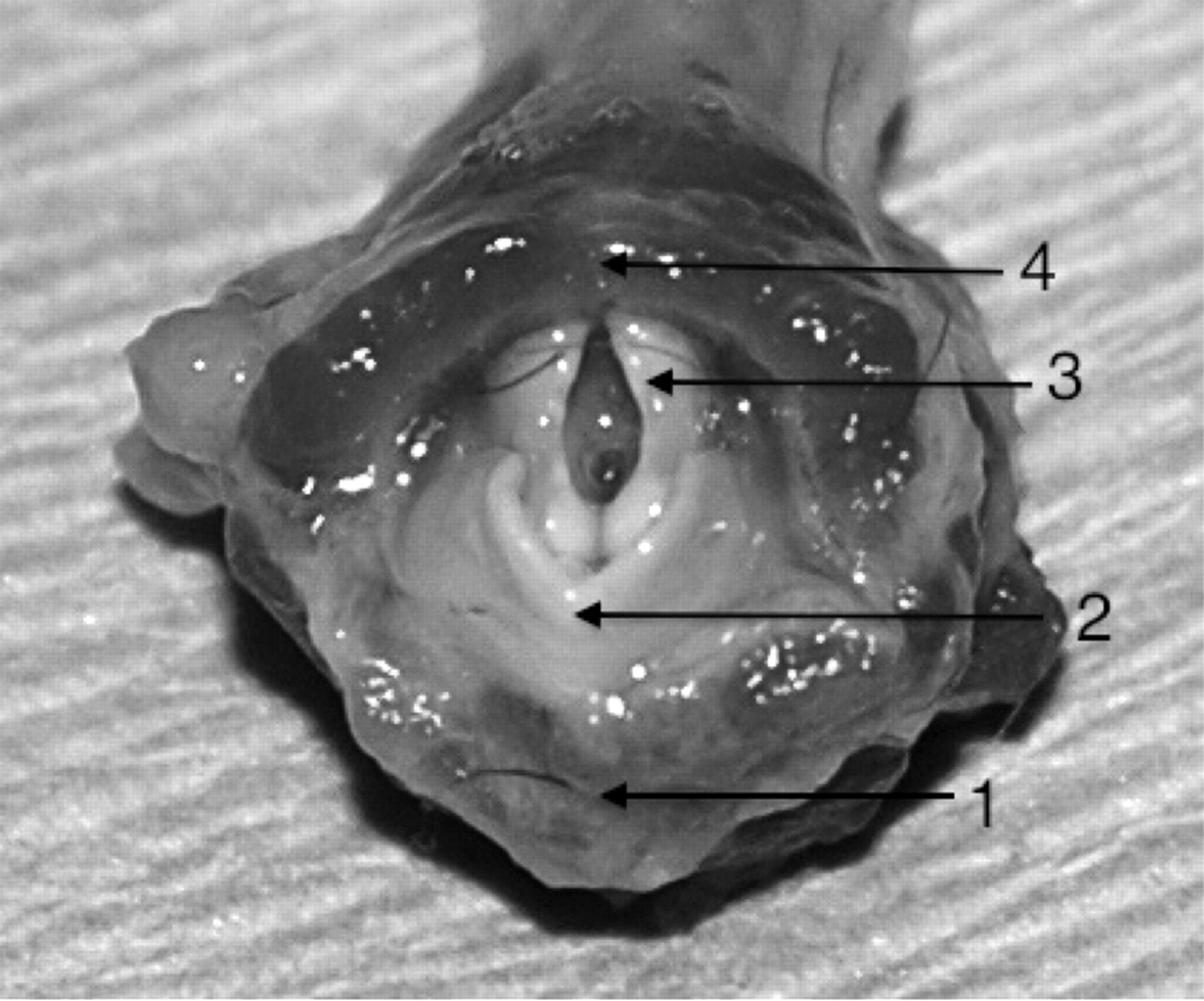
View of the entry of a marmoset larynx – isolated anatomical piece: (1) base of the tongue, (2) epiglottis, (3) arytenoid cartilage and (4) dorsal wall of the pharynx
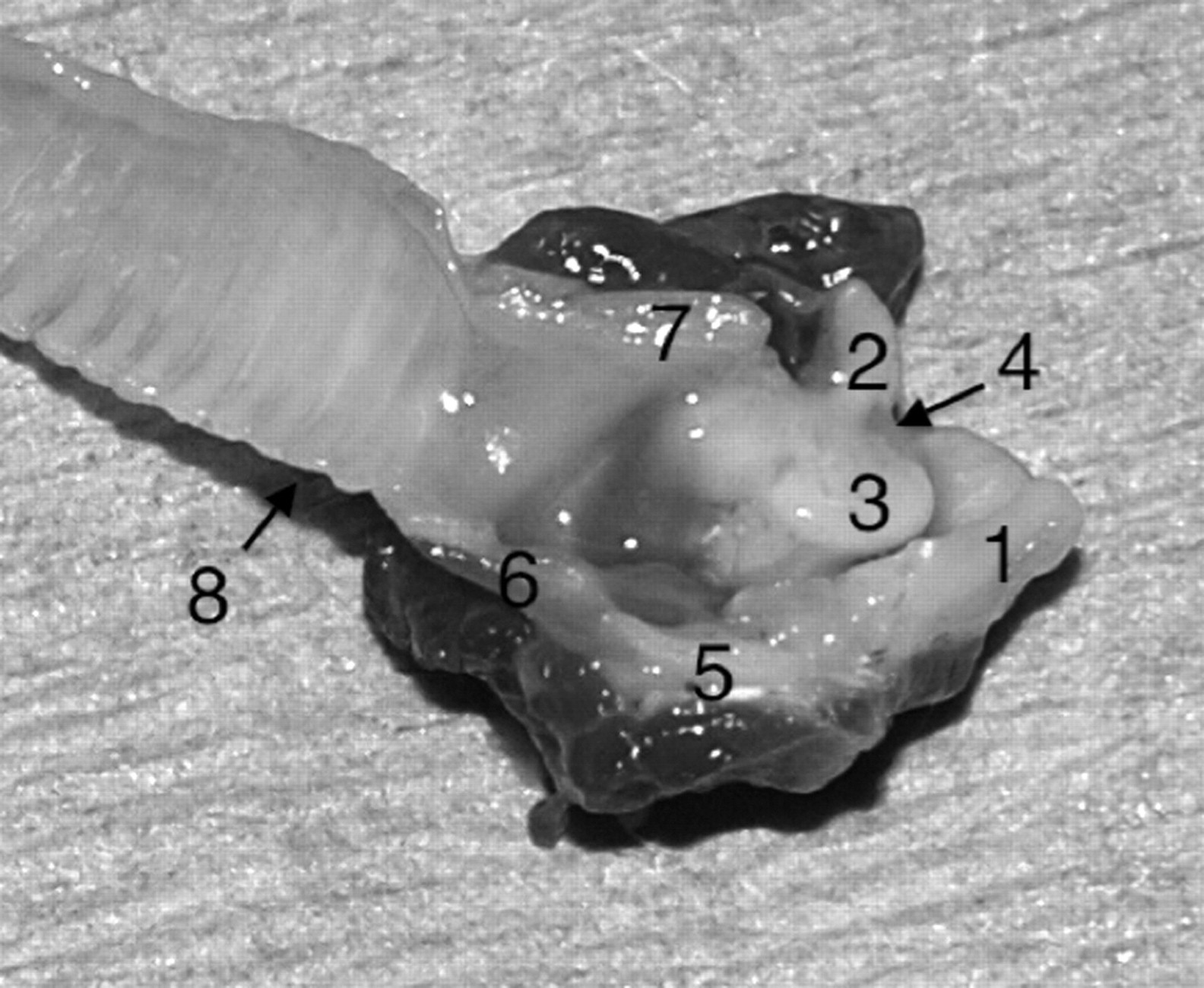
Sagittal section of a marmoset larynx: (1) epiglottis, (2) arytenoid cartilage, (3) vocal fold, (4) aryepiglottic fold, (5) thyroid cartilage, (6) crico-tracheal and cricothyroidic membrane, (7) cricoid cartilage and (8) trachea
Anatomical features measured and calculated (mean ± SD) based on 10 postmortem marmoset examinations
NTB: nose to tracheal bifurcation; CS: craniosacral length; OS: occipitosacral length
The trachea was constituted of a succession of C-shaped cartilage rings. They alternated with elastic annular ligaments that united the cartilages and allowed the trachea to stretch and bend without buckling. The dorsal part of the trachea was free of cartilage and was constituted of soft tissue, which was considered likely to be the tracheal mucosa, connective tissue and tracheal muscle (based on macroscopic examination). The external diameter of the trachea was greater at its proximal than its distal extremity, giving a clear tapered appearance. The tracheal bifurcation was located under the apex of the heart when the marmoset was positioned in dorsal recumbency.
The ratio of the nose to tracheal bifurcation with craniosacral (NTB/CS) and occipitosacral (NTB/OS) length can be seen in Table 1.
Bland–Altman plots generated from both the NTB/CS and NTB/OS ratios (Figure 6) show that the majority of the plotted points fall within two standard deviations (SD) either side of the mean of the difference between the pairs of measures (y-axis), indicating that the estimates using these ratios can be deemed interchangeable with that of actual measurement. Further the results of the one-sample t-test demonstrate that there was no significant difference between the estimated and actual distance from nose to tracheal bifurcation (P = 0.913). The 95% CIs for the NTB/CS ratio were smaller than those for the NTB/OS ratio (0.425 ± 0.02 and 0.534 ± 0.033, respectively).

Bland–Altman plot for the NTB/CS ratio. The y-axis shows the difference between each pair of values (i.e. actual measurement – estimated), and the x-axis shows the mean of each pair of values (estimated and actual measurement). The majority of points fall within the lines indicating two standard deviations either side of the mean (mean ± 2SD); therefore, the methods are considered interchangeable. 4 NTB: nose to tracheal bifurcation length, CS: craniosacral length
Discussion
Endotracheal intubation should be considered as a part of basic anaesthetic management of marmosets, just as it is in other animal species. However, the small size of marmosets as well as the absence of commercially available endotracheal tubes may discourage research workers from attempting this procedure. The approach described in this report allows endotracheal intubation to be performed rapidly and easily, using materials that are readily available in most laboratory animal units.
The tilting workstand was initially designed to aid intubation of rodents. However, it was appropriately sized and easy to use for marmosets. This allowed the intubation to be performed by a single operator since the head and neck of the marmoset were optimally positioned for visualization of the opening of the larynx. In the authors' experience, using a Miller blade size 0 to gently depress the base of the tongue provided a wider visualization of the arytenoid cartilages than the modified otoscope speculum provided by the manufacturers with the tilting workstand (although this speculum is ideal for use in rodents). Once the marmoset was positioned and the table tilted, the resulting extension of the head over the neck brought the axis of the oral cavity in alignment with the pharynx. In theory, aligning the oral, pharyngeal and laryngeal axis may seem ideal, as it would bring all structures concerned into a straight line, although the ‘3 axes rule’, introduced by Bannister and MacBeth has been recently challenged. 5–7 Given that the resting angle made by the larynx over the mouth seemed close to 90°, our experience with marmosets leads us to believe that it would be anatomically difficult or impossible to align oral, pharyngeal and laryngeal cavities on the same axis. In this study, intubation was made easier by a proper alignment of the buccal and pharyngeal cavity only, with the opening of the larynx as an endpoint of the pharyngeal axis.
Missing, broken or very worn canines are commonly observed in marmosets kept in captivity. 8 In this study two out of 10 marmosets had a canine missing. The canines are necessary to hold the marmoset in position on the workstand with an elastic band. As long as one of the canines was remaining, it was still possible to use the tilting workstand on these animals. The position of the strip holding the animal had to be slightly adjusted and the marmoset had to be manipulated with greater care during the intubation process to avoid the hanging strip to be dislodged from the canine.
Callitrichines are capable of a wide range of vocalization. This is made possible by a caudal descent of the larynx, increasing its resonance capacity. Compared with other non-primate animals, the descent of the larynx causes a large part of the tongue to be in the hypopharynx. In two of our 11 intubated marmosets, the large hypopharyngeal section of the tongue partially obstructed the view of the arytenoids and may have increased the number of attempts for successful intubation despite good positioning of the animal on the tilting workstand. The proportion of the tongue actually sitting in the hypopharynx is one of the predictors for difficult intubation via direct laryngoscopy in people. 9
The use of alphaxalone intramuscularly at the dose of 10.6 ± 1.6 mg/kg produced adequate sedation and muscle relaxation to allow an intravenous line to be placed in most animals, and the depth of anaesthesia could be increased easily with incremental doses of the agent. Alphaxalone is a synthetic neuroactive steroid, which produces anaesthesia and muscle relaxation mainly by interaction with the gamma-aminobutyric acid receptor. 10 Alphaxalone was previously available in the UK in combination with alphadolone, another steroid, in a polyoethylated castor oil-based formulation (‘Saffan’, Schering Plough Animal Health, Union, NJ, USA). Although widely used as an anaesthetic agent in dogs, cats and primates, 11–13 ‘Saffan’ had recognized adverse effects. Some hyperaemia or oedema of the pinnae or forepaws was observed in up to 69% of cats. 14 Some anaphylactoid reactions with histamine release were described in dogs and humans with subsequent fall in blood pressure, urticaria and skin oedema. 15 Most of these side-effects were associated with the polyoethylated castor oil. However, alphaxalone is now available in the UK with a new cyclodextrin-based formulation (‘Alfaxan’). Although ketamine is widely used for primate sedation, 16 it has been shown to have some local myotoxic effect 17 when administered intramuscularly to marmosets. Its use should therefore be avoided if the marmosets are to recover from anaesthesia. ‘Saffan’ was recommended as an alternative. 18 Based on the limited data in the present study, ‘Alfaxan’ would appear to be a suitable replacement, since none of the marmosets were found to have any abnormal muscular swelling or obvious pain at the injection site up to seven days postsurgery.
Although all animals could be intubated at the first or second attempt, some problems were encountered with the tube kinking despite the use of silastic tubing to support the junction between the catheter and its luer mount. Following examination of the laryngeal anatomy, it could be seen that there was an approximately 140° angle between the larynx and the cranial cervical part of the trachea. This angle was increased when animals were placed in a stereotaxic frame for neurosurgical procedures. In all cases the problem could be resolved by slight repositioning of the tube.
The cranial diameter of the trachea should allow intubation with a 12 G modified intravenous catheter. The final two animals in this series were successfully intubated using a modified 12 G over the needle catheter at the second attempt. This was made possible by gentle 180° rotation of the catheter once the tube had just passed the vocal fold. The use of a larger diameter endotracheal tube decreases the resistance to airflow and the relative strength of the tube makes it less susceptible to kinking and obstruction by mucosal secretions. The presence of the Murphy eye reduces the risk of significant tube occlusion if the end of the tube was positioned at the carina, and would also reduce the risk of occlusion with mucus.
None of the two marmosets intubated with a 12 G catheter had any tube occlusion by kinking during anaesthesia. The internal diameter of the proximal trachea was 4.8 ± 0.2 mm. The outer diameters of a 12 G catheter and a 5 F urinary catheter are 2.77 and 1.67 mm, respectively. Although the internal diameter of a 5 F catheter may vary with the type of catheter, it is very likely to be smaller than the internal diameter of a 12 G catheter (2.16 mm). We would therefore recommend the use of a 12 G modified intravenous catheter to intubate common marmosets in the body weight range used in this study. The tracheal and laryngeal dimensions suggest a significantly larger tube could be used, if a material that combined flexibility with sufficient wall strength to prevent kinking, luminal occlusion by secretions and collapse of the tube could be identified.
The use of an over the needle catheter required its length to be adjusted before intubation. The tracheal bifurcation was located 8.1 ± 0.5 cm away from the nose and was located under the base of the heart. This is consistent with a previous radiographic study. 19 The average length of the trachea itself was 4.9 ± 0.4 cm. Measuring the length of the marmoset once sedated could be used to estimate the distance from the nose to the carina. We assessed the pertinence of the use of external landmarks to predict the length of the trachea. The occiput, the top of the parietal bone and the base of the tail are easily palpated on a sedated marmoset. Both occipitosacral and craniosacral lengths could be used as a predictor for the tracheal length according to the Bland–Altman plots and one-sample t-test. However, the NTB/CS ratio had a smaller CI than the NTB/OS ratio. We therefore consider that the craniosacral length of the marmoset is a more reliable measurement than the occipitosacral length. Since the NTB/CS ratio is 0.42 ± 0.2 mm, we could express the length of the trachea as follow: NTB = 0.42 × CS, where NTB is the distance between the nose and the tracheal bifurcation and CS is the craniosacral length.
Our practical recommendations would be to position the silastic tubing around the proximal end of a 12 G catheter before sedating the marmoset. Once the marmoset is sedated and the intravenous line placed for induction, its craniosacral length (CS) would then be measured. The tube could then be bevelled at an appropriate length (=0.42 × CS), a Murphy eye cut if desired and intubation performed once the marmoset has reached an adequate plane of anaesthesia and has been positioned on the tilting workstand.
In conclusion, endotracheal intubation was easily performed in common marmosets and should be part of standard anaesthetic care. The view of the entry of the larynx was easily visualized when using the tilting workstand and gently depressing the base of the tongue with a Miller blade size 0. The length of the trachea could be predicted by multiplying the craniosacral length of the marmoset by a factor of 0.42. The diameter of the proximal trachea easily fitted an endotracheal tube made from readily available material (a 12 G ‘over the needle’ catheter).