
Abstract
Objectives
The aim of this study was to describe the use of an external landmark that defines the attachment of the tentorium ossium for planning a craniectomy to access the cerebellar fossa. The external landmark was defined by a line where the caudal aspect of the convexity of the cranium transitions to a flat surface in the caudal aspect of the temporal fossa. We also aimed to determine if this external landmark was present and readily visualized, and to establish its relationship to the nuchal crest using three-dimensional (3D) volume-rendered CT reconstructions created from cats with normal cranial morphology.
Methods
First, a case is presented for the description of an approach in a cat with a meningioma located dorsolateral to the cerebellum. Second, CT studies of five cats with normal cranial morphology were selected. Regions of interest (ROIs) were drawn at the attachment of the tentorium ossium to the cranium and nuchal crest. Three-dimensional reconstructions were developed with colored ROI overlays. The external landmark defined the tentorial attachment on all 3D reconstructions. Additionally, using the postoperative CT of the clinical case described herein, ROIs of the tentorial attachment and nuchal crest along with a third ROI, the craniectomy, were drawn and overlaid on the 3D reconstruction to illustrate the position of the craniectomy in relation to the tentorium ossium attachment and nuchal crest.
Results
The use of the external landmark provided for a craniectomy that enabled adequate visualization for excision of a meningioma. On all 3D reconstructions, the external landmark was present and readily visualized.
Conclusions and relevance
Between the attachment of the tentorium ossium and nuchal crest exists an area adequately sized for a craniectomy in cats. Clinicians can use an identifiable external landmark on the lateral aspect of the cranium to plan the rostral boundary for a craniectomy to access the cerebellar fossa in cats.
Introduction
The choice of a surgical approach for intracranial lesions is based on lesion size and location, along with the intended goals of surgery (ie, biopsy vs gross cytoreductive excision) balanced against inherent anatomic barriers, such as extracranial anatomy (ie, emergence of cranial nerves, nasal cavity or eye) and extra- and intracranial vasculature. Another consideration is to choose an approach that maximizes visualization of intracranial contents and thereby minimizes the potential for iatrogenic injury to nervous tissue or vascular structures.
The three main approaches to the brain in dogs include the modified transfrontal, rostrotentorial and occipital approach. 1 Each approach allows access to a specific region of the brain. No one approach in dogs enables access to the dorsolateral aspect of the cerebellum. To access the dorsolateral aspect of the cerebellum in the dog, a combined rostrotentorial and occipital approach must be used. 2 The necessity for a combined approach in the dog is likely a reflection of the location of the attachment of the tentorium ossium to the inner surface of the cranium. 3
In the dog, the attachment of the tentorium ossium to the inner surface of the cranium is formed from bony extensions of the parietal, interparietal and occipital bones.3,4 The external feature of the cranium that likely marks the attachment of the tentorium ossium in the dog is the nuchal crest. 3 In comparison, the tentorium ossium in the cat is attached further rostrally, which likely contributes to a more rostral position of the caudal fossa within the cranial cavity. 5 We hypothesize that a more rostral attachment of the tentorium ossium to the cranium in the cat provides for an area rostral to the nuchal crest on the lateral side of the cranium, which allows access to the cerebellar fossa via a craniectomy. Furthermore, we hypothesize that the rostral extent of the craniectomy is bounded by an externally visible landmark. The external landmark is defined by a line where the bone caudal to the convexity of the cranium (the widest aspect of the cranium) abruptly transitions to a flat surface in the caudal aspect of the temporal fossa.
To support the feasibility of using this external landmark to define the rostral extent of a craniectomy to access the cerebellar fossa, a descriptive report is presented of a 17-year-old domestic shorthair cat in which a lateral approach was used for gross cytoreductive surgery for an intracranial meningioma. To determine if this external landmark is present and readily identifiable in other cats, three-dimensional (3D) volume-rendered CT reconstructions from five cats with normal cranial morphology were qualitatively assessed.
Materials and methods
First, a clinical case report is presented to illustrate the approach in a cat at Red Bank Veterinary Hospital. Second, CT studies of cats with normal cranial morphology and lacking central nervous system deficits were identified using the medical record system at the University of Georgia. Cases were selected in cats having undergone CT imaging of the head (from the nasal planum through to the C1 vertebra) from 2017 to 2018. Specific inclusion criteria included age >1 year at the time of CT imaging, access to the digital imaging and communications in medicine (DICOM) images of the CT study acquired using a bone reconstruction kernel, an etiological diagnosis in the medical record that did not involve the cranium or central nervous system, and a finalized radiology report by a board-certified radiologist in which there was no pathology described involving the cranium or central nervous system structures. CT (Sensation 64; Siemens) was performed with cats under general anesthesia and in sternal recumbency. Transverse images were acquired in helical mode at a slice thickness of 2.0 mm using 120 kVp and 190 mAs.
Regions of interest (ROIs) of the attachment of the tentorium ossium to the inner surface of the cranium and the nuchal crest were drawn and overlaid on a 3D reconstruction using free, open-source software (MRIcroGL; https://www.mccauslandcenter.sc.edu/mricrogl/home). Briefly, DICOM images were converted to a neuroimaging informatics technology initiative file format (NIfTI file). The nifti files were used to create multiplanar reconstruction images that were displayed with a window width and level considered appropriate for visualizing bone. On each transverse CT image, an ROI was drawn by hand (in red) where the tentorium ossium attached laterally to the inner surface of the cranium using a pen-tablet system (Intuos; Wacom). From the point of attachment of the tentorium ossium to the internal surface of the cranium, the ROI was extended to the external surface of the cranium to allow visualization of the ROI as an overlay on a 3D reconstruction. Likewise, another ROI was drawn by hand (in green) on the external surface of the nuchal crest. The ROI along the nuchal crest extended from approximately the external occipital protuberance to a level just dorsal to the external acoustic meatus. Finally, a 3D reconstruction was created and the two ROIs were applied as overlays. The resultant image was saved as a TIFF. The finalized TIFF images were qualitatively assessed for the presence and location of the attachment of the tentorium ossium to the cranium and its relationship to the nuchal crest.
Retrospectively, the same ROIs were drawn on both sides of the cranium on the postoperative CT of the cat in the case description. A third ROI was drawn (in yellow) at the site of the craniectomy. The 3D volume-rendered CT image had all three ROIs overlaid for assessment of the location of the craniectomy site in relationship to the external landmark that defines the attachment of the tentorium ossium to the cranium and the nuchal crest.
Results
Case report
A 17-year-old spayed female domestic shorthair cat (weighing 4.2 kg) was referred for intermittent falling to the left. One month before referral the cat developed a left head tilt and left-sided vestibular ataxia. A complete blood count and serum total thyroxine concentration were normal. Serum chemistry profile revealed azotemia (creatinine 2.3 mg/dl, reference interval [RI] 0.5–1.4 mg/dl; blood urea nitrogen 28 mg/dl, RI 7–27 mg/dl). The referring veterinarian initiated empiric therapy with enrofloxacin (Baytril; Bayer) at 22.7 mg orally once daily for a presumed otitis media/interna. When improvement was not observed, the cat was administered prednisone (1.25 mg/kg PO q12h). Despite therapy, the vestibular ataxia worsened and the cat was referred for further evaluation.
On presentation, general physical examination was normal. On neurological examination, the cat displayed a vestibular ataxia and left head tilt. Postural reactions were delayed in all four limbs, with the left limbs being more affected than the right limbs. Positional vertical nystagmus was elicited with the cat in dorsal recumbency. The remainder of the neurological examination was normal. The anatomical diagnosis was consistent with left central vestibular dysfunction. The differential diagnoses included neoplasia, encephalitis (infectious) or, less likely, a metabolic encephalopathy.
Under general anesthesia, CT (Lightspeed 16; General Electric Medical Systems) of the head was performed. Transverse images were acquired in helical mode at a slice thickness of 0.6 mm using 120 kVp and 175 mAs. Images were acquired prior to and after intravenous (IV) administration 1.7 ml/kg of iodinated contrast medium (Omnipaque 350 mg/ml; GE Healthcare). CT imaging disclosed several hyperattenuating foci in the region of the left dorsolateral cerebellum. Following contrast administration, a 1.2 cm × 1.0 cm × 0.6 cm single, ovoid, extraparenchymal mass that displayed peripheral contrast enhancement dorsolateral to the cerebellum was observed (Figure 1). The mass compressed the cerebellum and the underlying medulla, as shown by ventral displacement of the choroid plexus in the fourth ventricle. Imaging findings were consistent with neoplasia or a granuloma.

(a) Preoperative, postcontrast CT image at the level of the cerebellum of a 17-year-old domestic shorthair cat with progressive left-sided vestibular dysfunction. There is an ill-defined mass that displays mild, peripheral contrast enhancement (black arrowheads outline the mass). The mass causes ventral displacement of the choroid plexus (black arrow) and compression of the medulla. (b) Prior to contrast administration, mineralization of the mass was visible (arrow). (c) Postoperative CT displayed in a bone window demonstrates the rostral margin of the craniectomy, which was identified by using the external landmark of the line where the caudal aspect of the convexity of the cranium transitioned to a flattened surface of the caudal aspect of the temporal fossa. This transition is where the tentorium attaches the cranium (black arrowhead). The ventrorostral aspect of the nuchal crest (white arrowhead) is identified. Intracranial and extracranial gas (white arrow) is seen, consistent with surgical intervention. (d) Caudal to the image in (c). The dorsoventral size of the craniectomy (between arrows; approximately 1.2 cm) was large enough to enable gross cytoreduction of the mass
The following day, the cat underwent a craniectomy for gross cytoreductive surgery of the intracranial mass. Prior to induction of general anesthesia, the cat was administered hydromorphone (West-Ward) at 0.1 mg/kg IV and methylprednisolone sodium succinate (Solu-Medrol; Pfizer) at 30 mg/kg IV. General anesthesia was induced with propofol (Rapanofal; Ivaoes) at 4 mg/kg IV, titrated to effect and maintained on isoflurane. During anesthesia, the cat received lactated Ringer’s solution (3 ml/kg/h IV) and was administered cefazolin (West-Ward) at 22 mg/kg IV every 90 mins until the end of surgery.
A curvilinear skin incision was made from approximately 2 cm caudal to the lateral canthus of the eye extending toward the midline and ending 1 cm caudal to the external occipital protuberance. The subcutaneous tissue and superficial muscles of the head were sharply incised along the external sagittal crest to expose the fascia of the temporalis muscle. The temporalis muscle fascia was sharply incised along the external sagittal crest and continued ventrally along the nuchal crest. The temporalis muscle was elevated from the temporal fossa, reflected rostrally and maintained in position with Gelpi retractors. Within the temporal fossa, there was a distinct line oriented in a dorsal–caudal to rostral–ventral direction, which was present immediately caudal to the convexity of the cranium owing to an abrupt transition to a flatter surface in the caudal aspect of the temporal fossa. A high-speed pneumatic drill was used to create an approximately 1.2 cm × 1.0 cm oval-shaped craniectomy, using this line as the rostral boundary of the craniectomy.
The craniectomy provided adequate visualization of not only the meninges overlying the dorsolateral region of the cerebellum, but also allowed for gross removal (following durectomy) of the mass. Following removal of the mass, standard closure of the fascia, subcutaneous tissues and skin were performed. The dural defect was not closed. Microscopically, the mass was consistent with a meningioma.
Postoperatively, a CT was performed using the same imaging parameters as the preoperative CT. The hyperattenuating material observed preoperatively was absent, consistent with gross cytoreductive removal of the mass. Focal gas accumulations were present within the cranial cavity, as well as extracranially, consistent with a surgical intervention. The cat recovered from anesthesia and surgery without complications. There was no decline in neurological function at evaluations 6 h and 24 h postoperatively. The cat was maintained on prednisolone (1.5 mg/kg PO q12h), gabapentin (6 mg/kg PO q12h) and amoxicillin–clavulanic acid (Clavamox [Zoetis]; 13.75 mg/kg PO q12h) for 2 weeks after surgery. The cat was discharged 2 days postoperatively and, at the time of discharge, had improved neurologically. At 8 weeks postoperatively, the cat was neurologically normal.
To assess the presence and visibility of the external landmark that defines the attachment of the tentorium ossium, five CT studies of the skull that met the inclusion criteria were chosen. All cats were domestic shorthair cats ranging in age from 7 to 14 years. Two cats were castrated males and three cats were spayed females. Reasons for imaging were nasal lymphoma, rhinitis and otitis media. All CT images were sufficiently detailed to allow drawing of an ROI at the attachment of the tentorium ossium on the inner surface of the cranium and the nuchal crest. Given the oblique angle with which the tentorium ossium attached to the cranium, the resultant overlays had areas that were discontinuous. Despite this, a defined line of attachment of the tentorium ossium was discernable on all 3D reconstructions (Figures 2 and 3). In all five cats, the attachment of the tentorium ossium was present as a discernable line of attachment. This line of attachment was present at the caudal aspect of the convexity of the cranium as it abruptly transitioned to a flattened region in the caudal aspect of the temporal fossa.

Lateral view of three-dimensional (3D) volume-rendered reconstructions from five cats (a–e) with normal cranial morphology that underwent imaging for reasons other than central nervous system deficits. A region of interest (ROI) was drawn (in red) where the tentorium ossium attaches to the inner surface of the cranial cavity and was displayed as an overlay on the 3D reconstruction. The attachment of the tentorium is at the transition from the caudal aspect of the convexity of the cranium to a flat region of the caudal aspect of the temporal fossa. An ROI of the nuchal crest was also drawn (in green) and displayed as an overlay on the 3D reconstruction

Caudal–rostral view point of three-dimensional (3D) volume-rendered CT image of the five cats (a–e) from Figure 2. On the left side of each 3D reconstruction, the line (red) that demarks the tentorial attachment is more easily seen. The green line represents the nuchal crest
From the postoperative CT of the cat having undergone a craniectomy, the ROI that defined the tentorial attachment appeared as the line observed in surgery. The rostral and caudal boundaries of the craniectomy were positioned between the line that demarked the tentorial attachment and the nuchal crest. Where the craniectomy was extended rostrally to the line of tentorial attachment, the caudal aspect of the cerebrum was exposed, which meant that the attachment of the tentorium ossium had been burred off (Figure 4).
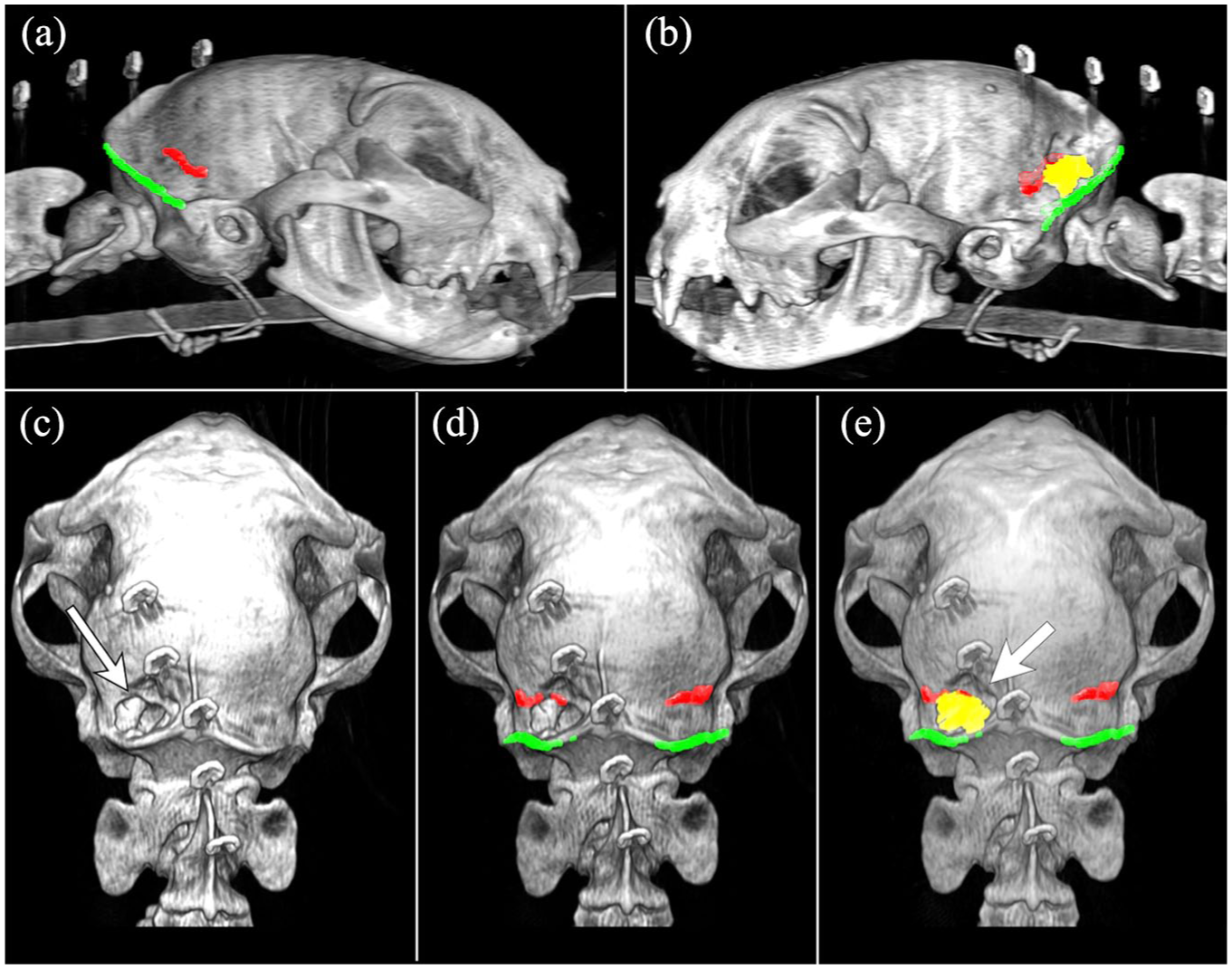
The same post-acquisition processing was applied to the postoperative CT images of a 17-year-old cat. (a) As in the other cats, the line that demarks the tentorial attachment (red) and nuchal crest (green) is seen on the right side. (b) On the left lateral view, the line that demarks the tentorial attachment (red) and nuchal crest (green) are overlaid. Additionally, the region of interest of the craniectomy is marked in yellow. (c–e) The same caudal–rostral view of the 3D reconstruction. The craniectomy is visible (white arrow). (d) The attachment of the tentorium (red) and nuchal crest (green) have been overlaid. (e) The craniectomy (yellow) is visible between the attachment of the tentorium (red) and nuchal crest (green). Note that a portion of the craniectomy is too rostral (white arrow)
Based on the 3D reconstructions and clinical case, a craniectomy bounded rostrally by the tentorial attachment was sufficiently large enough to access the cerebellar fossa. On the reconstructions of all five cats, the tentorial attachment was demarked by the line where the caudal aspect of the convexity of the cranium abruptly transitioning to a flat surface at the caudal aspect of the temporal fossa. This line was readily identifiable on the 3D reconstruction. The caudal boundary of a craniectomy would be just rostral to the nuchal crest. The dorsal and ventral boundaries are approximately at the level of the external sagittal crest and at the level of the zygomatic arch, respectively.
Discussion
Surgical approaches to the brain have been defined in the dog and for many of the approaches, modifications and refinements have also been described.2,6–13 Of the surgical approaches described in dogs, the rostrotentorial approach has been used successfully in the cat to access neoplasms that involve the cerebrum.5,14 However, few modifications of the other surgical approaches have been studied in the cat.10,11 This likely relates to the preponderance of intracranial neoplasms being located rostral to the tentorium cerebelli in cats and therefore are easily accessible via a rostrotentorial approach. 15 Neoplasms also occur in a caudal tentorial location or in both rostral and caudal tentorial locations in approximately 3% and 9% of cats, respectively. 15 Limited reports describe surgical treatment of caudal tentorial lesions and likely involve the use of an occipital approach.16,17 Additionally, an approach for cytoreductive surgery for meningiomas involving the tentorium has been described in cats. 10 In that report, a lateral approach akin to that described here was used for access to the tentorium cerebelli. 10 In contrast, the focus of the report herein was to define an external surface landmark on the lateral surface of the cranium that would enable accurate localization of the tentorium ossium and therefore the cerebellar fossa. Unlike the approach described for tentorial meningioma excision, the approach defined here does not disturb the attachment of the tentorium ossium or exposure of the occipital lobe of the cerebrum. 10 Instead, the approach described here provides access solely to the cerebellar fossa.
Through analysis of CT images from cats with normal cranial morphology, the cerebellar fossa is accessible between the nuchal crest and where the convexity of the cranium abruptly transitions to a flattened region of the caudal aspect of the temporal fossa. The latter creates a readily seen line on 3D reconstructions. That line demarks the tentorial attachment. In the cat having undergone a craniectomy using this approach, the line demarking the tentorial attachment also was grossly appreciated at surgery.
This approach requires minimal tissue dissection and therefore is anticipated to reduce morbidity. 1 In the case described herein, an uncomplicated recovery from surgery occurred and no postoperative decline in neurological function was observed. Finally, the landmarks used to position the craniectomy also were present and were readily appreciated on the 3D reconstructions in all five cats.
The use of the line to demark the tentorial attachment is predicated on cats having a relatively similar cranial morphology. The veterinary literature contains few descriptions of the cranial morphology in cats, with none being focused on the attachment of the tentorium ossium.18–20 Although cats can be divided into three phenotypic skull shapes, round-shaped, triangular and cuneiform, the impact that parameters such as skull length, width and height have on the position of the tentorium ossium within the cranial cavity remains unknown. 19 In European cats, one external morphological feature that may be important is the squamous portion of the occipital bone, which approximates either the shape of an isosceles triangle or a semi-oval shape from a caudal viewpoint. 20 With the semi-oval morphology, the nuchal crest and external occipital protuberance may be less conspicuous. 20 The presence and impact that this difference has on defining the external landmark used herein in other cat breeds remains unknown. Based on the morphology of the squamous portion of the occipital bone on 3D reconstructions of the cats described here, all had triangular morphology, which likely aided in defining external surface landmarks. It is possible that in cats with a semi-oval morphology, it may be challenging to define not only the nuchal crest, but also at the caudal end the convexity of the cranium, which defines the attachment of the tentorium ossium.
Conclusions
Surgical access to the cerebellar fossa can be attained via a lateral approach to the cranium and craniectomy in the caudal aspect of the temporal fossa in cats. The rostral boundary of a craniectomy in the temporal fossa can be planned by an external landmark. This landmark is a line defined by the caudal aspect of the convexity of the cranium as it transitions to a flat surface of bone in the caudal aspect of the temporal fossa. Between this line and the nuchal crest, an area exists that is sufficient in size to create a craniectomy providing adequate access to the cerebellar fossa. It is anticipated that approaching the cerebellum via a lateral approach to the temporal fossa is technically less challenging and requires less soft tissue dissection than either an occipital approach or a combined rostrotentorial and occipital approach.
The positive outcome in the cat described herein and the results of the analyses of the 3D reconstructions suggest future investigation is warranted. Morphological analysis of more cats with differing cranial morphologies is necessary to ensure that the external landmarks used here can be used in other cat breeds. Until such morphological data are reported, clinicians can use multiplanar MRI or 3D CT reconstructions to help identify external landmarks to optimize the surgical approach to the dorsolateral cerebellum.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of client-owned animal(s) only, and followed established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal guardian of all animal(s) described in this work for the procedure(s) undertaken. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.