
Abstract
Objectives
This study has compared clinical and imaging features in 52 cats naturally infected by respiratory nematodes Aelurostrongylus abstrusus, Troglostrongylus brevior and Capillaria aerophila, and in both monospecific and mixed infections.
Methods
Medical records of cats with a lungworm disease were retrospectively reviewed. Cats with clinical examination findings, haematobiochemical analysis and thoracic radiography were included in the study and clinical and radiographic scores were assigned. For eight cats CT of the thorax was also available and analysed. A statistical analysis was performed to investigate the potential correlation between clinical and radiographic score, and to evaluate the effect of age, sex and infection on clinical and radiographic severity.
Results
Monospecific infections by A abstrusus (32/52), T brevior (6/52) and C aerophila (5/52) and coinfections by T brevior/A abstrusus (7/52), T brevior/C aerophila (1/52) and A abstrusus/C aerophila (1/52) were diagnosed. Cats with mixed infections showed higher clinical scores compared with cats with monospecific parasitoses (P <0.05), while no differences were observed for radiographic scores. No correlation between clinical and radiographic scores was found (rs = 0.50), and these scores were not affected by patient age or sex. CT, performed on cats infected with A abstrusus, T brevior or A abstrusus/T brevior, provided additional information in cats with mild radiographic signs.
Conclusions and relevance
This study indicates that clinical parameters may be more severe in mixed infections than in monospecific parasitoses. A significant correlation between clinical and radiographic score was not detected, while several subclinically infected cats showed radiographic changes. In cats with mild-to-moderate lung patterns, the ventrodorsal/dorsoventral projection showed lesions that are not visible in the lateral projections, especially in the caudal lobes.
Keywords
Introduction
Different parasitic nematodes affect the respiratory system of domestic cats and, in recent years, mixed infections are increasingly being reported, especially in Mediterranean countries.1–4 Aelurostrongylus abstrusus (Metastrongyloidea, Angiostrongylidae) is the most important species for its worldwide distribution and clinical importance.5–8 Nonetheless, in the past few years a rise in the number of infections by zoonotic Capillaria aerophila (Trichocephalida, Capillariidae) 8 has been recorded in cats.3,4,6,9 Also, Troglostrongylus brevior (Metastrongyloidea, Crenosomatidae), historically affiliated to wildlife, has been recently described in domestic cats from some European countries.2–4,10–12 Feline lungworm infections may be subclinical, or cause mild-to-severe respiratory signs, depending upon the parasite species and burden, 7 and clinical signs are non-specific.1,3,11 The most common radiographic abnormalities in naturally3,13–15 or experimentally 16 infected cats are bronchial, nodular and unstructured interstitial patterns with multifocal distribution, which may evolve into a generalised alveolar pattern in severe cases.
CT provides higher-resolution images of lung fields and this examination recently proved useful for a thorough characterisation of pulmonary lesions in feline aelurostrongylosis.15–17 However, there is no information on the use of CT in cats with mixed infection or infection with T brevior and/or C aerophila.
The aim of the study was to describe clinical, radiographic and CT features of feline lungworms, along with a comparison of clinical and radiographic characteristics in 52 cats with single and mixed lungworm infection.
Materials and methods
Records from the Teaching Veterinary Hospital, University of Teramo (Italy), of cats with feline lungworm infections, diagnosed by microscopic and molecular methods,1,7,18–20 were retrospectively reviewed.
Dorsoventral (DV) or ventrodorsal (VD) and left-to-right lateral radiographs of the thorax (ALFA 90 PLUS; CAT Medical System) were obtained in non-sedated cats, and presence, degree and distribution of radiographic patterns were evaluated as previously described.3,21 The clinical and radiographic findings were assessed with a score (Table 1) aimed at measuring the degree of clinical and radiographic severity.
Criteria for assessment of clinical and radiographic severity indices

A volumetric pre- and post-iodinated contrast (Optiray 320 mg/ml; Mallinckrodt Pharmaceuticals) total body CT, followed by high-resolution CT (HRCT) of the thorax, were performed with an eight-slice scanner (GE Brightspeed) while under general anaesthesia. Intramuscular dexmedetomidine (Dexdomitor; Elanco Animal Health) and methadone (Semfortan; Dechra Veterinary Products), intravenous propofol (Proposure; Boehringer Ingelheim Animal Health Italia) and a mixture of oxygen and isoflurane (Vetflurane; Virbac Animal Health) were administered through an endotracheal tube to all cats, which were hyperventilated before the scan to allow for a few seconds of apnoea. The cats were placed in sternal recumbency and scans were acquired in the craniocaudal direction with soft tissue (volumetric CT) and lung (HRCT) algorithms. Scanning parameters for the volumetric study were 1.25 mm slice thickness, 200 mA, 120 kVp and pitch 1.3; for the HRCT, the parameters were 0.6 mm slice thickness, 280 mA, 120 kVp and axial.
Statistical analyses were performed with MedCalc Statistical Software version 17.9.2. The effect of age (younger vs older than 12 months), sex and infection (single vs mixed infection) on clinical and radiographic severity was evaluated. The degree of association between clinical and radiographic scores was calculated using Spearman’s coefficient. Pearson’s χ2 or Fisher’s exact tests were used to compare categorical variables, and Mann–Whitney U-tests or Kruskal–Wallis tests were used to compare continuous variables between two or more groups, respectively. A P value <0.05 was considered significant.
Results
Clinical cases of 26 cats (of the 52 analysed) have been described in a previous study with different aims, 3 and only the severity of clinical signs were again analysed in the present study.
There were 22 males and 30 females (age 2 months to 11 years [median 10 months]), which had regular outdoor access. Forty-three cats had single infections, whereas nine were infected by more than one parasite (Table 2). Twenty cats showed mild clinical signs with clinical scores of 1–3, moderate-to-severe signs (clinical score ⩾4) were observed in 11 animals, whereas in 21 cats no abnormalities were detected during the physical examination (Tables 2 and 3). Cats with a mixed infection showed higher clinical scores than cats with monospecific parasitoses (P <0.05) (Figure 1).
Distribution of cats with no, mild or moderate-to-severe clinical signs based on studied variables (age, sex and aetiology)

Data are n (%)F = female; M = male; Aa = Aelurostrongylus abstrusus; Tb = Troglostrongylus brevior; Ca = Capillaria aerophila; ns = not significant
Clinical and radiographic scores of 52 cats with single and mixed lungworm infections

Aa = Aelurostrongylus abstrusus; M = male; Tb = Troglostrongylus brevior; F = female; Fs = spayed female; Ca = Capillaria aerophila; Mc = castrated male

Box plot of the clinical scores in cats with Aelurostrongylus abstrusus (Aa), Troglostrongylus brevior (Tb), Capillaria aerophila (Ca) and mixed lungworm (MIX) infections. The MIX group statistically differs to other groups (P = 0.007211).
Radiographic abnormalities were observed in all patients, with an interstitial pulmonary pattern the most common, being found in 45 cats (39 generalised unstructured, six nodular pattern); a bronchial pattern was found in 43 cats. An alveolar pattern was present in 14 animals, and three cats showed caudal pulmonary artery dilatation (vascular pattern). Thirty-seven were mixed patterns, whereas 15 presented single patterns (Table 3). Pulmonary infiltrates had a multifocal distribution (Figure 2) in all cats but one with capillariosis, where a single large nodule in the caudodorsal field of the left lung was visible in three projections (Figure 3). The most severe nodular patterns with multifocal distribution were found in four cats infected by A abstrusus/T brevior. In cats with mild-to-moderate lung patterns, the VD or DV radiographic projection showed lesions that were not visible in the lateral projections, especially in the caudal lung lobes (Figure 4). No significant differences were recorded in radiographic scores between monospecific or polyspecific infections (Figure 5).
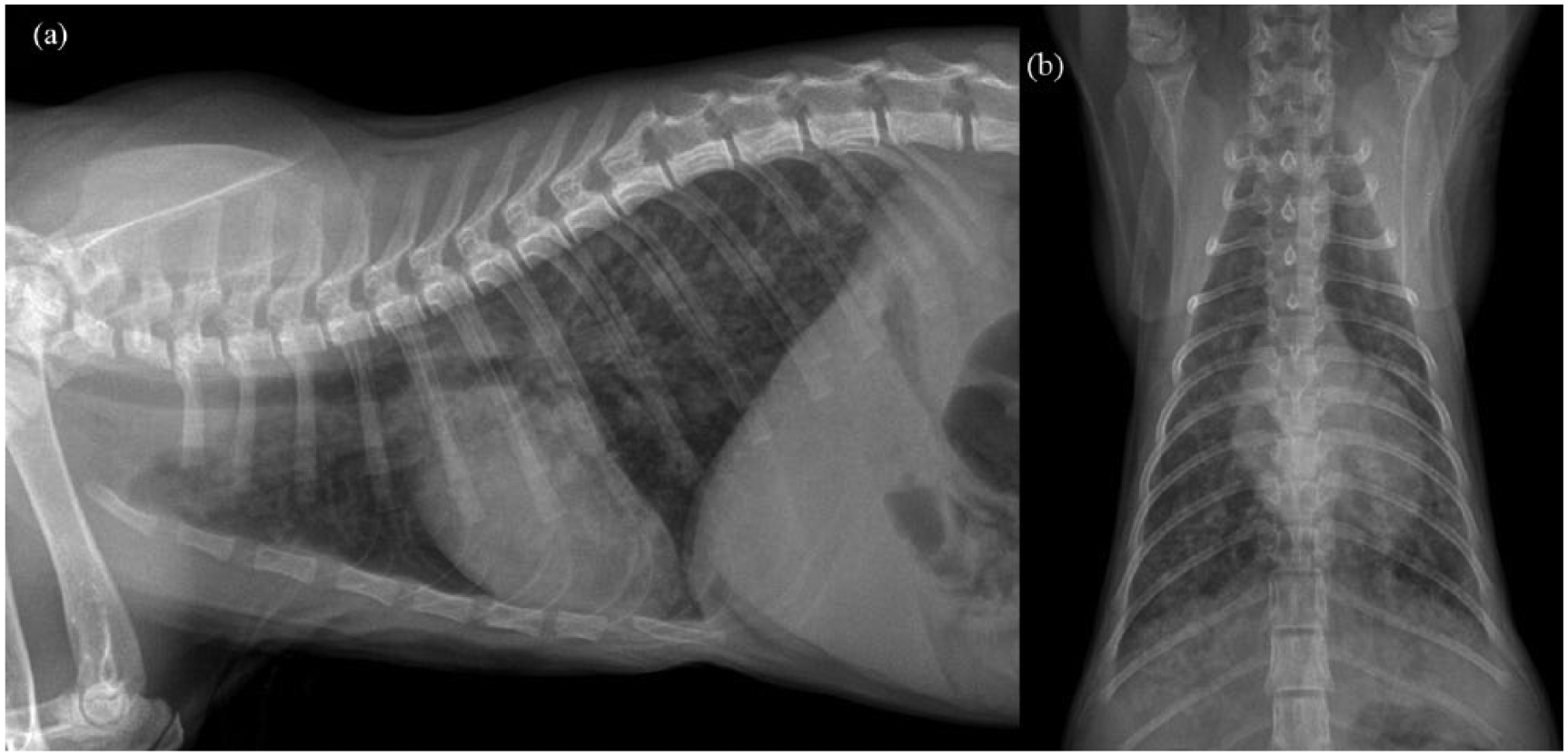
Right lateral (a) and ventrodorsal (b) radiographic projections of the thorax in a cat with mixed infection by Aelurostrongylus abstrusus/Capillaria aerophila; note the severe bronchointerstitial pattern with multifocal distribution
(a) Left lateral, (b) right lateral and (c) dorsoventral radiographic study of the thorax in a cat infected by Capillaria aerophila; note the mild bronchial pattern and single large nodular lesion (white arrow) in the caudodorsal field of the left lung visible in the three projections

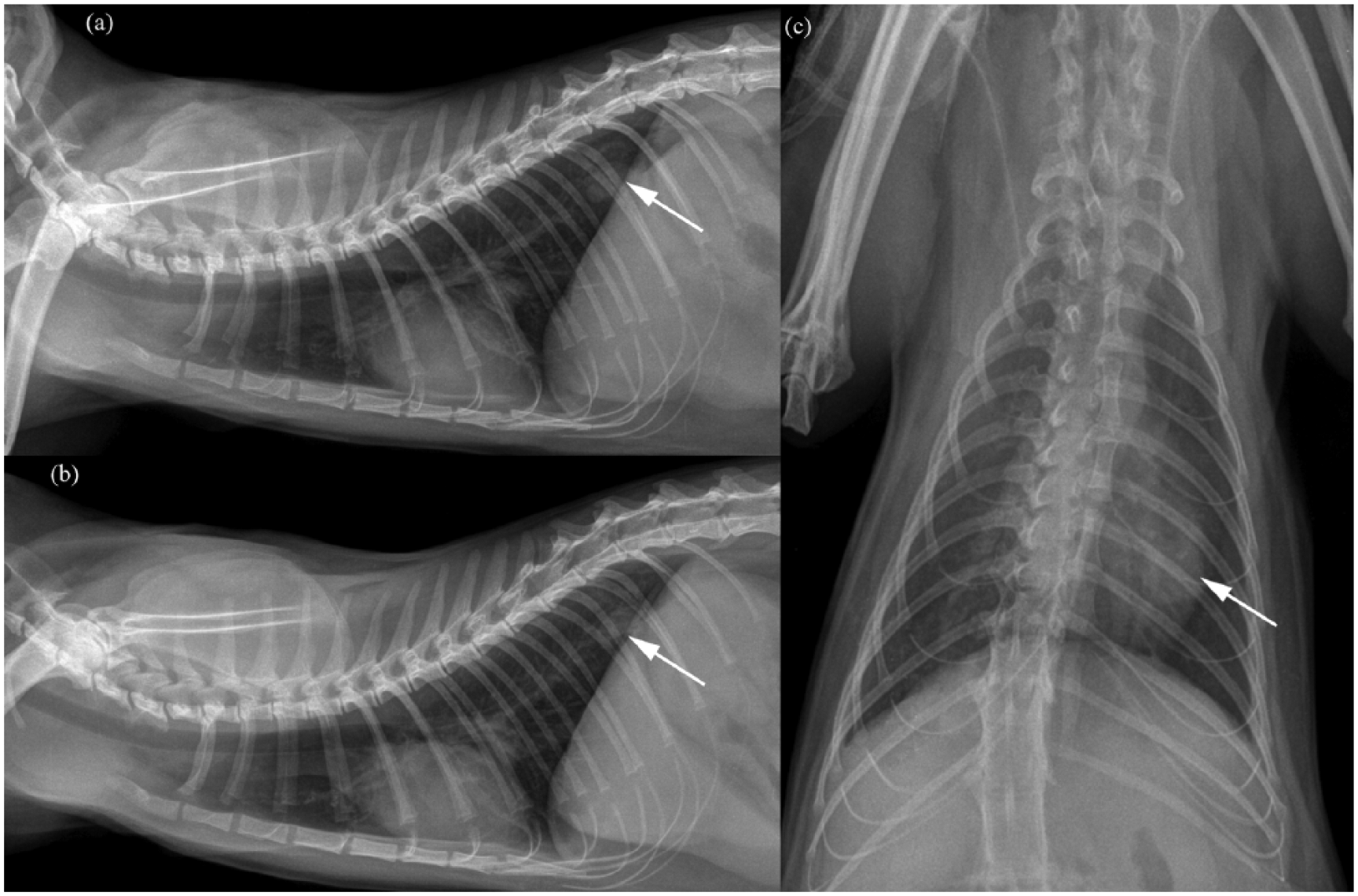
Radiographic study of the thorax in a cat infected by Aelurostrongylus abstrusus; a mild bronchial pattern in the (a) caudodorsal lung field is visible in lateral projection, compared with, in the (b) dorsoventral projection, a moderate (on the left hemithorax) and moderate/severe (on the rigth hemithorax) bronchointerstitial pattern
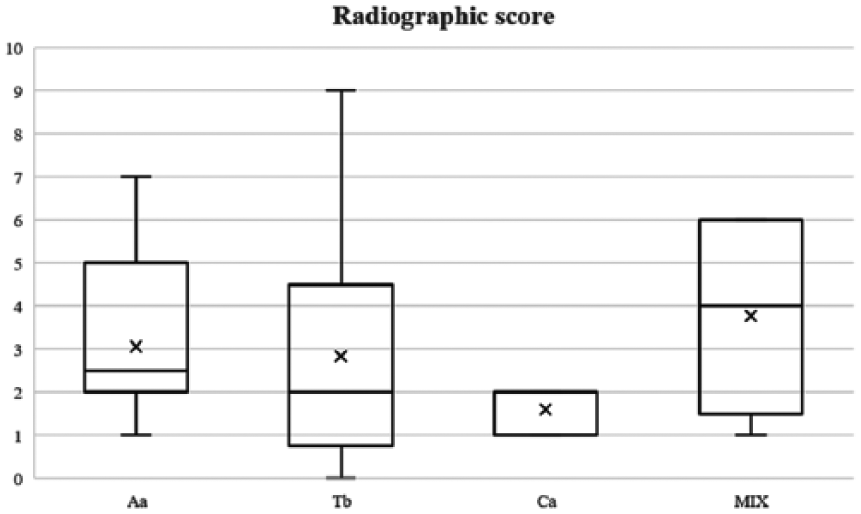
Box plot of the radiographic score in cats with Aelurostrongylus abstrusus (Aa), Troglostrongylus brevior (Tb), Capillaria aerophila (Ca) and mixed lungworm (MIX) infections. There was no significant difference among groups (P = 0.148187)
Clinical and radiographic severity (Table 3) did not differ statistically between males and females or between cats younger and older than 12 months. No correlation was observed between clinical and radiographic scores among cats with lungworm infection (rs = 0.50).
Eight cats underwent CT study (Table 4) and all of them showed multilobar involvement, with an interstitial ground-glass opacity. Furthermore, bronchial/peribronchial changes, together with an alveolar infiltrate not observed in the thoracic radiographs (Figure 6), were present in five cats with A abstrusus and in a cat coinfected by A abstrusus/T brevior. Moreover, in four cats with A abstrusus infection, multifocal ill-defined nodular lesions, which were not recorded during the radiographic examinations, were observed (Figure 7). CT of a cat with troglostrongylosis revealed only a ground-glass appearance. In examined cats, mean normal lung density was ‒730 HU vs ‒515 HU in ground-glass opacity areas vs −51 HU for an alveolar pattern.
Radiographic and CT findings of eight cats with single and mixed lungworm infections

Aa = Aelurostrongylus abstrusus; F = female; Tb = Troglostrongylus brevior; Mc = castrated male; Fs = spayed female; M = male

CT image of a cat infected with Aelurostrongylus abstrusus; note the note the bronchointerstitioalveolar infiltrate with a ground-glass appearance

CT image of a cat infected with Aelurostrongylus abstrusus; note the multifocal ill-defined nodular lesions
Discussion
Clinical signs in cats infected with respiratory nematodes are usually affected by different factors, 7 although in this study the clinical severity was not influenced by patient age or sex. Furthermore, although some species (eg, T brevior) are more pathogenic than others, in the patient cohort examined here, the nematode involved in monospecific infections did not influence the clinical severity, whereas the clinical parameters were more severe in multiparasitic infections. Indeed, cats infected with T brevior showed a clinical severity similar to those with a single infection caused by A abstrusus or C aerophila, probably due to the diagnosis being made at an early stage. This finding is relatively unexpected considering the high pathogenicity of T brevior,1,11,22 and this further emphasises the importance of a timely copromicroscopic diagnosis as a routine test. Cats with troglostrongylosis had severe lung changes, regardless of the severity of the clinical signs (Table 3); thus, it is plausible that they would have soon developed clinical signs if a prompt diagnosis was not achieved. Therefore, routine Baermann examinations are advisable in clinical practice, especially in young animals, regardless of the presence of clinical signs compatible with a respiratory parasitosis.
In agreement with previous studies,14,23,24 a significant correlation between clinical signs and severity of radiographic changes was not detected in the cats examined herein, whereas several of them showed radiographic changes without clinical signs.
No differences were seen in the severity of radiographic signs related to age, sex and lungworm involved, although the most severe nodular lesions were associated with mixed infections by A abstrusus/T brevior in four cats.
Interestingly, the large single nodule detected in the C aerophila-infected cat was similar to that described in a Serbian woman misdiagnosed with a bronchial carcinoma. 8 Felid pulmonary capillarosis is usually considered subclinical, although symptomatic cases are reported.3,25,26 In this study, 4/5 cats with capillariosis did not show clinical signs, and one showed an intermittent cough. However, all infected cats showed radiographic changes.
Although the scoring system used is not validated, and it might be flawed because the different signs are evaluated as if they all have an equal weight, the present study shows that the clinical severity of lungworm infections may only partially correspond to that of a radiographic study, and that radiographic changes may be evident before the onset of clinical signs.3,14 It is noteworthy that DV or VD radiographic projections showed lesions that were not visible in the lateral projections, especially in the caudal lung lobes.
The predominant lesion in feline aelurostrongylosis found on CT consists of multiple nodules of varying size, widely distributed throughout the lungs, 17 and the severity of the findings depends on the level of infection. 16 In a recent study, CT of cats with aelurostrongylosis revealed that a ground-glass appearance was associated with interstitial–alveolar infiltrate, multifocal nodular structures, generalised lymphadenopathy, and bronchial wall and subpleural thickening. 15
As expected, 15 CT allowed a very detailed characterisation of lung infiltrates compared with conventional radiology. Specifically, CT revealed a larger extension and more lesions than radiology. Although there was a lack of statistical analysis of the CT results, owing to the low number of cases, this approach appears to be promising for thorough analysis of respiratory lesions that are not detected by radiography, such as alveolar infiltrates and nodular lesions.
Potential limitations of the study could be the possible variance in practice between physicians (even though protocolled care is used for cats presenting with lungworm disease), and the lack of validation of the scores used herein.
Conclusions
Parasitic bronchopneumonia is now considered an important disease of domestic cats and should be considered as the main differential diagnosis for lower respiratory signs in cats living in endemic areas. Although non-specific, the presence of radiographic changes suggests a possible lungworm infection in cats exposed to risk factors, either with respiratory signs or that are apparently healthy.
CT seems to provides a more accurate evaluation of lung lesions compared with radiology and its importance in revealing the presence of pulmonary lesions is also confirmed for single and mixed lungworm infections.
Given that respiratory pathological changes occur in lungworm-infected cats regardless of the presence and severity of clinical signs, appropriate anthelmintic treatments are required in all cases when a lungworm infection is diagnosed.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.