
Abstract
The stigmatization of stay-at-home fathers (SAHFs) has been widely studied, but little research has examined how these experiences vary between rural and urban areas. In this qualitative study, 20 SAHFs in Islamabad, Pakistan were recruited through purposive sampling and interviewed using interview guide. Results show that most men did not choose to become SAHFs, and were involuntarily thrust into the role due to unemployment, lack of appropriate employment opportunities, or disability. These men faced stigmatization, social isolation, and labeling from their friends, family, and community, resulting in their increasing stress and anxiety. Additionally, the study found that rural and urban residential backgrounds played a significant role in the experiences of SAHFs. Examining the concept of caring masculinities, the study discovered that cultural differences, adherence to gendered norms, and severe stigmatization made it difficult for SAHFs in a non-Western culture context to depart from traditional masculine roles and embrace caring masculinities.
Introduction
Over the past few decades, the number of stay-at-home fathers (SAHFs) has grown globally (Connolly et al. 2014; Latshaw 2015; Hoewe et al. 2017). SAHFs, also known as at-home fathers, househusbands, male primary caregivers, and primary caregiver fathers (Boyer et al. 2017), are defined as individuals who are not working or out of the labor force for at least a year, stay at home, and engage in family caregiving and domestic responsibilities while their female partner works outside the home in the labor force (Rushing and Powell 2015). Despite this increase in the number of SAHFs, research on the stigmatization and experiences of SAHFs, particularly in non-Western sociocultural contexts, is limited (Latshaw 2015; Hoewe et al. 2017; Rushing and Sparks 2017).
In Pakistan, the female labor force participation rate is 24%, a significant increase over the past decade (Pakistan Bureau of Statistics 2021). This increase in women joining the labor force has also increased male unemployment in the country (Pakistan labor force survey 2021). As more women enter the services sector with increasing levels of education, the labor force in Pakistan, traditionally dominated by men, is seeing a shift in work-family arrangements. However, there is a lack of available data on the actual percentage of SAHFs in Pakistan, making it difficult to reflect on the change in trends over time accurately (Islam 2019).
Despite the small number of SAHFs, they hold both practical and theoretical importance (Kramer and Kramer 2016). While much of the existing literature focuses on the experiences of female breadwinners (e.g., Medved 2016a; Chesley 2017; Blom and Hewitt 2020), there is less attention given to caregiving fathers with part-time work responsibilities (Doucet 2004; Medved 2016b; Lee and Lee 2018). Furthermore, research on the stigmatization of SAHFs across different social categories is scarce. Deutsch and Gaunt (2020) argue that it is important to document societal responses to nontraditional gender roles in order to understand their larger societal impact.
This study aims to fill this gap by examining the experiences of SAHFs in Pakistan and how they face stigmatization and differential treatment across their residential backgrounds in a traditional patriarchal society that expects gendered roles. The research question at the center of this study is: How do SAHFs experience stigmatization and differential treatment across their residential backgrounds in a traditional patriarchal society that expects gendered roles? By taking a qualitative approach and using a semi-structured interview guide for data collection, this study will recruit 20 SAHFs in Islamabad, Pakistan through purposive sampling. By critically evaluating the concept of caring masculinities, this study aims to identify the cultural differences, emphasis on gendered norms, and severe stigmatization that make it difficult for SAHFs in non-Western cultural contexts to depart from traditional masculine roles and embrace caring masculinities. This research will contribute to a deeper understanding of the stigmatization and challenges faced by SAHFs, highlighting the importance of considering cultural and societal factors in this area of study.
Literature Review
Caring Masculinities
Elliott, (2016) concept of “Caring masculinities” is an alternative viewpoint toward traditional gender practices and roles. Elliott’s work is substantially based on
Elliott (2016) identified three characteristics that form caring masculinities. First is the rejection of domination due to its role in creating relationships' inequalities. Rejection or absence of domination makes equality between the partners, and therefore men adopting caring masculinities are expected to show disloyalty to traditional norms of violence, domination, and masculinity. The second characteristic of caring masculinities is to emphasize interdependent, emotional, relational, and effective qualities of care and positive emotions. In this way, a difference is created between traditional and caring masculinities. Traditional masculinities emphasize emotional stoicism, where men are expected to suppress feelings of hurt and pain (Hooks 2004). The third characteristic is to reshape traditional masculine values where men are considered breadwinners, protectors, and head of the household to interdependent, care-oriented, and relational values. For instance, a male partner can take the responsibility of caregiving instead of or in addition to being a breadwinner for his household. Caring masculinities generally introduce caregiving and relational qualities to traditional masculine identities, establishing new meanings and understandings for men who exhibit caring masculinities.
Caring masculinities focus on determining caring roles as neither inherently female nor male. Therefore, SAHFs are a relevant group with whom how changes in masculinities take place can be considered. SAHFs may adopt caring masculinities due to various reasons, including unemployment, job loss, challenges in balancing work-family issues, and underemployment (Chesley 2011). Some men may opt for caregiving due to their desire to become primary caregivers or personal preferences (Fischer and Anderson 2012). However, irrespective of the motives and reasons for adopting caregiving roles among men, it has the potential to contribute new viewpoints and perspectives that emphasize the interconnectedness of masculinity and caring (Doucet 2004). SAHFs are aware of the stereotypes of traditional masculinities, and they differ from employed fathers' traditional masculine characteristics (Fischer and Anderson 2012). Simultaneously, SAHFs report lower adherence to traditional male gender norms than employed fathers (Rochlen et al. 2008). Caring masculinities do not suppose that the behaviour of men is in accordance with traditional masculine standards. Instead, it assumes that through integrating rationality, interdependence, and positive emotions, men rework their traditional masculinities into caring ones. There are also differences in the implications of caring masculinity and other theories for men. The main emphasis in caring masculinities is on adopting the values of care, which will enrich men’s lives psychologically, physically, and emotionally. Instead of shaming and blaming men, caring masculinities focus on supporting and encouraging men’s participation in care work to help promote gender equality and develop nurturing attitudes.
My study, employing caring masculinities as a framework, focuses on how SAHFs in a patriarchal cultural context experience masculine norms and identities and how these experiences with non-traditional gendered roles vary across rural and urban residential backgrounds. More importantly, how do they interpret these challenges of stigmatization and gendered expectations in a patriarchal cultural context?
Stay-at-Home Fathers and Masculinities
As more men adopt caregiving roles, traditional gender norms continue to influence parental decisions and roles (Rushing and Sparks 2017). Several studies find that men in the SAHF role feel a sense of loss for the breadwinning role, a traditional work-family arrangement for men (Chesley 2011; Solomon 2014; Tinsley et al. 2015). Loss of the breadwinning role is associated with isolation and anxiety for most SAHFs in almost all parts of the world (Burkstrand-Reid 2012; Latshaw and Hale 2016). Negative stereotyping and societal responses negatively affect the development of the masculine self and its maintenance (Medved 2009; Rushing and Powell 2015; Liong 2017). Connell (2001) asserts that masculinity is socially acquired and not biologically determined, so masculinities are likely to change over time. However, social pressures often undermine the changing nature of masculinity and require men to abide by the socio-cultural ideals attached to hegemonic masculinity (Gilbertson 2020).
Earlier studies on the experiences of SAHFs and whether these men are inclined to engage in more masculine or more feminine behaviors had inconsistent findings regarding the gender characteristics of these stay-at-home men (McGinnity and Russel 2008). Studies conducted more recently on the experiences of SAHFs also consider their gender behaviors (e.g., Lee and Lee 2018; Liong 2017). For instance, Doucet (2018), in her qualitative study with 64 Canadian fathers and 14 heterosexual couples, attempted to explore whether men do mother when they take on the caring role. She found that mothers and fathers acknowledged sticking with traditional notions of different gendered parenting roles. The study further found that although SAHFs were responsible for childcare, typically reserved for mothers, they still spoke of the fundamental differences between fathering and mothering. She concluded that fathers though capable of parenting like mothers, are not actually mothering, and men still identify themselves more with masculine roles. One of the reasons for sticking to masculine identities for men is that they experience severe flexibility stigma compared to women if their responsibilities as caregivers impinge on their jobs in any way possible (Berdahl and Moon 2013; Rudman and Mescher 2013).
Other studies demonstrate that stay-at-home fathers experience Stigmatization, social isolation, and discomfort when they attend parent-child groups and meetings mainly run by women in stay-at-home roles (Ammari and Schoenebeck 2016; Boyer et al. 2017; Zimmerman 2000). The perception of playgrounds as non-appropriate spaces for SAHFs, who confront most of the stigmatization and responses from stay-at-home mothers, is also elaborated in other research studies (e.g., Rochlen et al. 2008; Haberlin and Davis 2019). SAHFs also experience discomfort and isolation in different social spaces, such as shopping centers and parks, mainly because of the responses of mothers with children. Rochlen et al. (2008) reported that fathers perceive negative judgment for their parenting abilities by stay-at-home mothers, who advise them on how to take care of their children when they face each other in spaces like parks and shopping centers. Similarly, Haberlin and Davis (2019), who used the method of poetic inquiry to evaluate interviews of SAHFs, reveal that most schools prefer that mothers attend parental meetings instead of fathers and that fathers who participate in these meetings are stigmatized by most of the stay-at-home mothers.
Class and regional differences in stigma for Stay-at-Home Fathers
Class and regional differences also play a role in the stigmatization of fathers. Poor men may be more vulnerable to the “flexibility stigma,” or the negative association with taking time off from work for family reasons, compared to professional men (Williams, Blair-Loy, and Berdahl 2013). Poor men may struggle to live up to societal expectations of ideal workers and may feel their masculine identities are threatened as they are seen as subordinate to those with economic power and as weak breadwinners with little control over their own lives. Professional men, on the other hand, can more easily meet societal expectations and are therefore trusted to internalize norms of work devotion. Elite men may also be vulnerable to the flexibility stigma, but if it is triggered, they may fall further as they leave the high status of ideal men and ideal workers and plummet into the family caregiver category
Coltrane et al. (2013) used a U.S. national longitudinal dataset to examine the impact of taking time off from work for family reasons on men’s future earnings. After controlling for various characteristics, they found that unemployed men who took a break from work or reduced their working hours for family reasons experienced a sharp decrease in their future earnings. These findings were not in line with experimental studies, which predict a strong flexibility stigma for men compared to women (Allen and Russell 1999; Butler and Skattebo 2004). Instead, their data showed that the flexibility stigma is gender-neutral, and men who choose caring responsibilities at home or adopt the “daddy track” suffer long-term earning penalties similar to those experienced by women who reduce their working hours.
Methods
The study participants were recruited from Islamabad, which is the capital city of Pakistan. Islamabad is the abode of people from various sociocultural and ethnic backgrounds. Islamabad’s total population is 2.3 million (Pakistan Bureau of Statistics 2019), comprising urban and rural areas. The urban population represents 66% of the total population, and the rural population represents the rest. The literacy ratio in the urban areas is higher than that of the rural areas (ibid). The nuclear family system is the central family organization in urban areas, while the joint family system is predominant in rural areas. The number of couples with female breadwinners is increasing, along with the possibility of getting comparative data from rural-urban and joint-nuclear family contexts.
Respondents' Demographic Information.
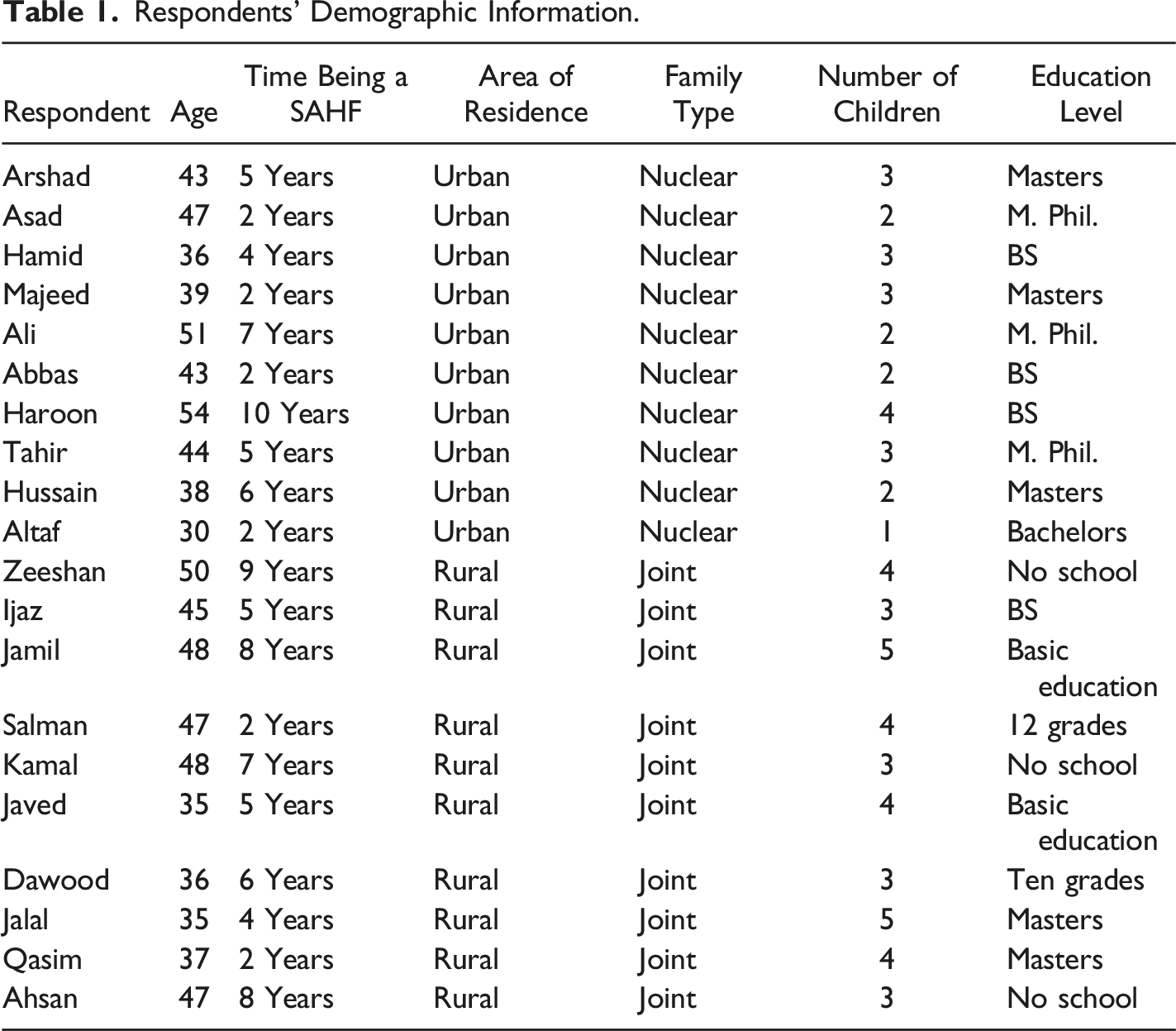
Recruiting the study participants from rural areas was particularly difficult due to their role being more stigmatized, and therefore, it took me more time to find and persuade them. I assured them of their anonymity and confidentiality of the data provided. I also assured them of not employing their real names in the study. For this reason, the names mentioned in Table 1 are not the real names of the study participants; instead, pseudonyms are created.
Sample Characteristics
The sampling strategy for the study was purposive sampling for respondents who fulfilled the selection criteria. The sampling criteria required that participants be male, married, unemployed, or out of the labor force for the last year or more. Twenty SAHFs met the requirements, 10 of whom lived in urban areas of Islamabad and belonged to nuclear families. Ten of whom lived in the peripheral rural regions and lived in a joint family system. The level of education was higher for the respondents from urban areas than for those who lived in rural areas. All urban fathers had at least a bachelor’s or master’s degree. Whereas rural fathers had a range of qualifications (where three were having no school education, two each had primary and higher secondary school education, and the rest had bachelor’s and master’s degrees). As the purpose was to explore the experiences of SAHFs, all respondents were men and were of age 30 years and above. Comparisons across these social categories were possible because of the heterogeneous nature of the sample.
Interviews
Data was collected through semi-structured interviews using an interview guide. The guide included questions on the participants' experiences of stigmatization, as well as demographic information such as age, ethnicity, education level, family type, family monthly income, spouse’s occupation, duration of unemployment, and number of children. It also covered topics such as the participants' daily routines, reasons for becoming a stay-at-home father (SAHF), experiences and feelings about the role, responses from family and society, changes in their perspectives on masculinity and femininity, negative stereotyping and stigma they have faced, and coping strategies. Audio recordings of the interviews were transcribed verbatim, with the average interview lasting 45 min. Participants were given the opportunity to speak freely and add any additional information.
Analysis
Data was analyzed using thematic analysis, following the steps outlined by Braun and Clark (2006), which included familiarization with the data, generation of codes, development of initial themes from the codes, review and editing of the initial themes, naming and defining of the themes, familiarization with the themes, and production of a results report. The analysis began by identifying and listing codes that emerged from the initial reading of the interview transcripts, followed by evaluating the codes and highlighting those that were salient and reflected in the literature. Deductive and inductive codes were generated and refined through first-cycle coding, which described the data in relation to the research objectives and questions (Saldana 2021). Second-cycle coding identified conceptual and thematic similarities among the codes and resulted in the development of broader codes, which were later collapsed into themes. The final step involved refining the themes and comparing them with existing literature on the experiences of SAHFs.
Results
The results of the study are divided into three sections: SAHF is not a choice, stigmatization, and the cost of being a SAHF. The data revealed that patriarchal norms are deeply ingrained in Pakistani society, leading to severe criticism and stigmatization of SAHFs, making this role a non-choice for most study participants. The second section highlights the social stigmatization experienced by SAHFs, beginning with their family, friends, and the surrounding community. The third section demonstrates how these negative experiences of ridicule and stigmatization resulted in anxiety, stress, and social isolation for SAHFs. Throughout the themes, the study also shows how the experiences of SAHFs varied between rural and urban areas, with more severe stigmatization and ridicule faced by fathers living in rural areas compared to urban areas. In urban areas, actors engaged in stigmatization and ridicule of SAHFs included spouses, parents, and other family members, while in rural areas, both close relatives and neighbors and the community were actively involved in stigmatization. The level of stress and isolation was higher for SAHFs from rural areas, while it was comparatively lower in urban areas.
Stay-at-Home Father is Not a Choice
In Pakistan, gendered norms are deeply ingrained in society, with men expected to be the primary breadwinners and women responsible for domestic duties. As a result, men who take on the role of stay-at-home fathers (SAHFs) are often viewed as challenging these norms. Due to the societal pressure to conform to these gendered roles, the patriarchal structure of society, and the stigma associated with breaking gender roles, many couples in Pakistan find it difficult to choose non-normative roles. This study found that the majority of participants did not choose the role of SAHF willingly, but rather adopted it due to unemployment, lack of employment opportunities, disability, or underemployment. Despite this, they still faced negative judgment from society and were often considered responsible for their situation. One participant, Ijaz, who had been unemployed for the last five years while his partner, a schoolteacher, provided the only income for their family, shared his experiences of what led him to take the SAHF role: “I have an engineering degree but could not get an appropriate job, a position that fits my qualifications. I tried for two years to get a job in various government and private sectors, but I couldn't get one. Now I don't look for a job because there isn't any. I depend on my wife's earnings, and I feel terrible about this situation.
This account illustrates that the decision to adopt the SAHF role was not a voluntary one, but rather a consequence of Ijaz’s inability to find an appropriate job despite his higher education. The decision to adopt this role for most participants involved the consent of their partners, family members, and in some cases, people in the surrounding community.
Many men in the study stated that they discussed their decision to adopt the SAHF role with their partners and family members, and initially, everyone disapproved of it. Almost all participants stated that the SAHF role in society is not appreciated and that people in this role are subject to shaming and blaming. They are often questioned about their manhood and are assumed to be responsible for their situation.
Jalal, a participant with a master’s degree in political science from a rural area who had been unemployed for the last 4 years, shared his experience: Being a SAHF was not my decision. After losing my employment as a research analyst in a private company, I wanted to find an appropriate job, but I could not find work. I talked to my wife, and she suggested that she would help in this situation and look for a job. Luckily, she found a job, but it was then that my real problems started. People started questioning my employment status while mentioning my wife being employed. In the beginning, it was just questioning. Then it turned into taunts, labels, and blaming.
Jalal’s experiences highlight the challenges faced by SAHFs in a patriarchal society and demonstrate that the decision to adopt this role is not a choice, but rather a consequence of couples' earning and employment circumstances. In this study, similar accounts were not uncommon, and these negative societal responses were found to be instigating changes in participants' perceptions of themselves.
The transition to the Stay-at-Home Father (SAHF) role for men from urban areas who were living in nuclear family systems was found to be distinct from those of SAHFs in rural areas. Despite facing criticism for adopting the SAHF role, the decision was not resisted in the same manner as it was for their urban counterparts. As Tahir, an individual living in urban Islamabad and unemployed for the past 5 years, described his experiences of deciding to adopt the SAHF role: I am not in a situation that I could be proud of. I have to be earning for my family. However, I don't know many people in the surrounding community, and my wife is very supportive of me, so nobody interferes in our personal matters and the decision of adopted the SAHF role was not much resisted. But I am clear that sooner or later I will again take on the breadwinning role.
These interview extracts reflect the notion that the transition towards a gender atypical SAHF role for most men is not a matter of choice, but rather an involuntary decision compelled by their economic situation. It also highlights that these men intend to return to traditional male breadwinning roles if given the opportunity for appropriate employment. SAHFs must take into consideration the opinions of not only the immediate family but also the surrounding community, with disapproval of this role being more severe in rural areas in comparison to urban areas. SAHFs from urban areas, due to the prevalent nuclear family system, must take into consideration the partner’s opinion only, resulting in a higher level of ease in transitioning towards this gender atypical role. However, the integrated societal system in rural areas demands considering the opinions and perceptions not only of the family members, but also those of the community, making it difficult for SAHFs from these regions to adopt this role voluntarily.
The Stigma of Being Stay-at-Home Father
Stigmatization, negative societal judgments, and facing questions about their manhood was a common experience for most of the SAHFs in this study. Men who are dependent on their female partners for their livelihood are generally labeled to have feminine traits. They are blamed and publicly shamed for gender non-conformity. The stigmatization of SAHFs starts with their family members, as adult male family members who are married and unable to earn for themselves are subject to negative judgments. This stigmatization then spreads to the general community, as illustrated by the experiences of Salman, whose wife was employed in the police department: I am dependent on my wife’s earnings. I spent five years in Dubai, where I earned a good amount of money, but I lost my job and returned to Pakistan. My wife has a bachelor’s degree and is the only educated person in our family. She always wanted a job, but I never allowed her because, you know, our people don’t consider it appropriate for women to work outside the home. But as our economic situation angered, I had no choice but to allow her to work. My brothers and parents were against this decision and are still contesting our decision. I have to deal with their negative remarks on a daily basis because I don’t have enough money to arrange a separate living for my wife and my children. Life has become so terrible.
Another study participant, Ijaz, who had been in a SAHF role for the last 5 years, shared his experiences: I cannot go out in public. I cannot face my relatives or the people in my surroundings because they constantly question my manhood. They think I am not worthy of respect because I am not earning money for my family, and they think I am emasculated.
Varying experiences across urban and rural residential backgrounds.
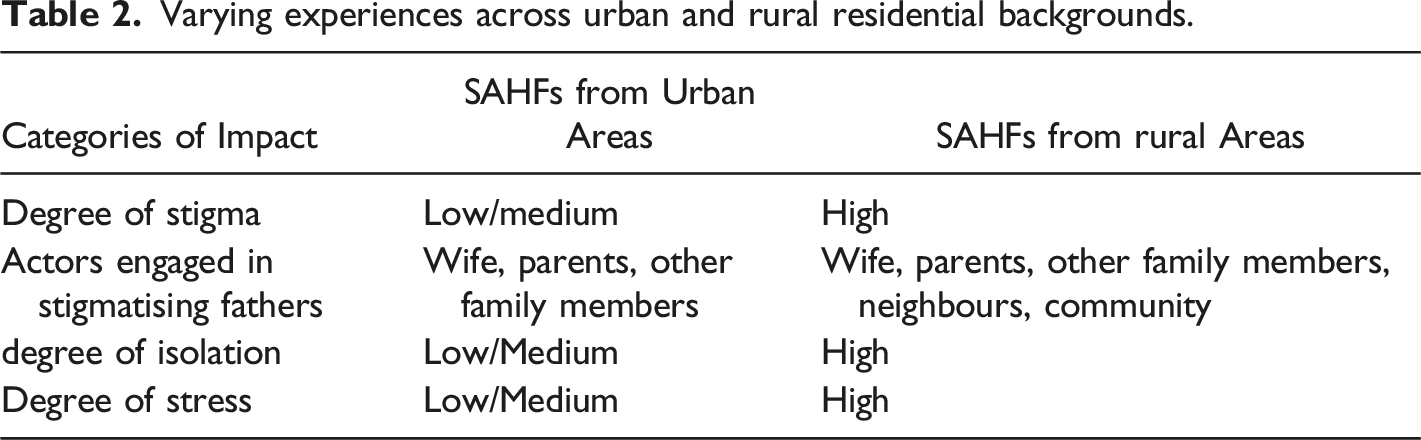
Data revealed that SAHFs living in rural areas and within a joint family system were the most affected by stigmatization. One participant, Kamal, a 48-year-old father of three who has been unemployed for the past 7 years and residing in a remote rural area, provided insight into his experiences: Look! I could not find a job for the last seven years. My wife is a nurse, and she is the only source of our family income. In principle, nobody in my extended family should be concerned about our situation, but this is not the case. My brothers, their wives, and even my parents label me as lazy and consider me responsible for not being in the job market. We are four brothers, all married, living under the same roof, and our parents have strictly forbidden us from living as a nuclear family. They won´t forgive us if I don’t comply with their wish. That is why we are compelled to live in a joint family, even when I am suffering psychologically.
This phenomenon can be attributed to the societal expectation of a gender-based division of labor, with a significant emphasis placed on men being the primary breadwinners and women being the primary caregivers (Brescoll et al. 2018; Chesley 2017). In rural areas and joint family systems, this expectation is reinforced through higher levels of social integration and the imposition of gender-specific norms, making it difficult for SAHFs to avoid socially imposed sanctions for non-conformity.
SAHFs in urban areas also experience stigma and negative responses, although to a lesser degree. Haroon, a SAHF residing in an urban area, narrated his experiences in this regard: It's a difficult situation for me where I cannot earn for my family. My wife thinks I am lazy and not earning for her and my kids. Whenever my family (parents and siblings) contacts me, they inquire about my employment status and are unhappy with my wife's employment. Although people in my neighborhood and community do not ask me directly about my employment status, I can still feel their inquisitive gazes when I go out. However, I am glad that I live in this area (Urban city center), where not many people know me. Otherwise, you know, people who are aware of your employment situation in our society make your life hell through their shaming attitude, questioning, and stigmatization.
The data highlighted a significant impact of the rural/urban dichotomy and family structure on the level and degree of stigmatization experienced by SAHFs. However, other factors such as education and social class also play a role, with SAHFs with higher education living in urban areas and within a nuclear family setup experiencing less severe stigmatization than those with lower education levels. Additionally, the impact of social class and education declines in the rural context within a joint family setup, where even relatively highly educated individuals from higher social classes experience more severe stigma than their counterparts in urban areas.
Cost of Negative Societal Responses
The negative societal responses to SAHFs undermine their mental and emotional wellbeing. Often, they have to deal with increased stress levels. Few of them were also diagnosed with depression and anxiety and were under treatment. To avoid facing stigmatization, they developed different strategies for different actors. They restrict themselves to their homes and reduce interactions with the outside world, avoiding public spaces, gatherings, and interactions with people as a strategy to avoid negative judgments and stigmatization. Coupled with guilt for not earning for their families, the social isolation further aggravates their stress, depression, and anxiety.
Jamil had been unemployed for the last 8 years and was married to a woman who was a teacher in a private school, shared his experience: Look, we live in an integrated society, where my matter is not only mine, but so many people can interfere in my private affairs. I have no problem with my wife's employment and being a SAHF because of unavoidable circumstances. Yet, my extended family, friends, and other community members are not happy about it. Their negative remarks and constant inquiry about my employment status and my wife's job are quite depressing for me. I am learning to avoid talking to people by restricting my mobility.
Similarly, another study participant, named Javed, who was unemployed for the last 5 years because of the termination of a contractual job, expresses: Please don't judge me, but I will tell you honestly that I am on medication due to mental health issues. I was never like this; I was a man of strong nerves. Blaming, shaming, and constant questioning from the people in my surroundings have caused me depression. People think I am enjoying my life on my wife's earnings; they think that I don't want to earn for myself and am happy being an at-home father.
Major and O'Brien (2005) also assert that stigmatized people’s physical, social, and psychological wellbeing is affected by negative judgments, stereotyping, and discrimination. My findings correspond to their conclusion with a slight variation of the differences due to the residential background of my respondents. Experiences of isolation, anxiety, and stress were more severe for rural SAHFs due to the integrated social system in the villages, where people know each other and have contact regularly. Therefore, SAHFs are more exposed to these negative experiences. Tahir, who is now an urbanite, used to live with his extended family in the peripheral area of Islamabad a couple of years ago, was in a better position to compare the experiences of both settings: Five years ago, I used to live in a joint family system with my wife, parents, and married siblings. Unfortunately, I lost my job and had to stay at home after being unable to find one. I spent my first three years being SAHF in that area, then shifted to this urban area (Islamabad city center) for the last two years. I experienced the worst scenario of anxiety and depression while living in the village, where everyone used to make fun of me and ridiculed me only because I was unemployed, and we were surviving on my wife´s earnings. Then we moved to the city center because my wife was fortunate enough to find a job here.
Repercussions of the negative societal response to SAHFs are disparately divided across rural and urban settings to affect their mental and psychological wellbeing. The intensity of these negative judgments is severe for SAHFs who live in rural areas. SAHFs from urban regions experienced less negative societal judgments, so they had less severe mental and emotional issues.
Discussion
The experiences of SAHFs in relation to social stigma and the impact of this stigma on their lives have been largely unexplored in the literature. This study sought to address this gap by examining the experiences of SAHFs in rural and urban areas of Islamabad, Pakistan, using a qualitative approach. The data collected through interviews with 20 SAHFs, ten from each area, revealed that these individuals often experienced stigmatization and differential treatment from those around them, including name-calling and questioning their masculinity. In some cases, this resulted in mental health problems such as anxiety and depression. However, the severity of the stigma and the reasons for becoming a SAHF differed between the rural and urban participants. Those in rural areas were often involuntarily thrust into the role due to unemployment, lack of appropriate employment opportunities, underemployment, or disability. They also experienced higher levels of stigmatization due to the more traditional and integrated nature of their communities. On the other hand, SAHFs in urban areas, who tended to live in nuclear families, had more choice in their decision to become a SAHF and experienced less severe stigma.
The findings of this study align with the theoretical framework of caring masculinities, which includes the rejection of male dominance, an emphasis on emotional and relational qualities of care, and a reshaping of traditional masculine values to include care-oriented and relational values (Elliott 2016). However, the data suggests that the adoption of caring masculinities was less common among SAHFs in rural areas where traditional masculine norms were stronger. These individuals often felt pressure to conform to hegemonic masculinity but attempted to resist these expectations by redefining their gendered roles. Meanwhile, SAHFs in urban areas, where social pressures were weaker, were more likely to embrace caring masculinities, although this was often due to unemployment, job loss, disability, or underemployment rather than a conscious choice. Despite the trend towards greater adoption of caring masculinities in urban areas, traditional breadwinning and provider expectations of fathers remained strong due to the stigma attached to the role of SAHF and traditional gendered societal expectations.
The role of social class in shaping the experiences of SAHFs is also worth considering. Previous research has suggested that middle-class men are more likely to take on caregiving roles due to their greater economic and social resources (Ciabattari, 2021; McDonnell and Wasche 2016). The data from this study supports this, with SAHFs in urban areas, who were generally of a higher social class, experiencing less severe stigma and being more likely to adopt caring masculinities. However, the rural SAHFs in this study were also largely middle-class, suggesting that other factors, such as the traditional and integrated nature of the community, may also play a role in the stigmatization of these individuals.
Overall, this study highlights the need for a greater understanding of the experiences of SAHFs and the impact of social stigma on their lives. It also highlights the potential for the adoption of caring masculinities as a way to challenge traditional gender roles and reduce stigma. However, more research is needed to fully understand the complexity of these issues and to identify ways to support SAHFs and promote gender equality.
There are several limitations to this study that future research could address. One limitation is the lack of representation of the perspectives of female partners of SAHFs, as this study only included male respondents in SAHF roles. A study that includes the perspectives of female partners would provide a more comprehensive understanding of the impact of the spousal relationship on SAHFs. Another limitation is the focus on social isolation as a coping strategy for SAHFs to avoid negative societal judgments, without exploring other ways in which SAHFs may avoid stigmatization. Further research on these other coping strategies could add to our understanding of the experiences of SAHFs. Additionally, this study did not delve into the support mechanisms that may assist SAHFs in coping with their situations. Examining these mechanisms in different contexts could be valuable in understanding the support available to SAHFs.
Conclusion
This study sought to understand the experiences of stay-at-home fathers (SAHFs) in a patriarchal society and how these experiences vary in rural and urban contexts. The data revealed that becoming a SAHF was often not a choice for these men, but rather a result of unemployment, lack of appropriate employment opportunities, underemployment, or disability. SAHFs frequently faced stigmatization, labelling, and social isolation from their families, friends, neighbors, and communities, which caused stress and anxiety for many of them. These negative responses were more severe for SAHFs in rural areas, where there is a higher level of social integration and traditional gender roles are more entrenched. In contrast, SAHFs in urban areas experienced less severe stigmatization due to the lower levels of social integration and higher levels of anonymity in these areas. However, both rural and urban SAHFs struggled to adopt caring masculinities due to societal pressure to conform to traditional gender roles and cultural expectations. The study also highlights the challenges faced by SAHFs in non-Western cultural contexts and the importance of considering contextual factors in understanding their experiences.
This study has brought attention to the need for a greater understanding of the experiences of SAHFs and the impact of social stigma on their lives. It also highlights the potential for the adoption of caring masculinities as a way to challenge traditional gender roles and reduce stigma. However, more research is needed to fully understand the complexity of these issues and to identify ways to support SAHFs and promote gender equality.
Footnotes
Acknowledgements
I owe a debt of gratitude to my research participants of the study who helped me in carrying out this research study. Their time and availability for interviews and sharing their information made us able to complete this study in a smooth and steady way. I am also grateful to my Doctoral Supervisor, Prof. Dr. Sarah Speck for her valuable guidance, suggestions, and constant encouragement throughout my PhD project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.