
Abstract
To better understand the needs of fathers who experience health inequities, we individually interviewed fathers, mothers, and service providers about their perspectives of supports for men in Vancouver’s Downtown Eastside, one of the most disadvantaged groups in Canada. Using a gender lens, thematic analysis of transcribed interviews with three cohorts revealed the following themes: “we need a He-way”: Fathers arguing for men-friendly services; “I had to do all the hard work”: Mothers identifying relational impacts of fathers’ barriers to services; “there is nothing out there for them”: Service providers acknowledging the lack of father-focused programs. Findings highlight the need for, and challenges to creating accessible, gender specific, father focused programs and services to best support men and families within the complex contexts of experiencing significant health inequities. This work illustrates how gender-based analyses can guide strategies for health promotion programs that will ultimately support fathers, mothers, and their families.
Introduction
Shifts in expectations of contemporary fathering and parenting practices are well documented. Research consistently shows that involved fathers can positively influence children’s behaviour, social, and psychological outcomes (Flouri and Buchannan 2003; McBride, Schoppe-Sullivan, and Ho 2005; Sarkadi et al. 2008). Despite these known benefits, a lack of tailored social services, as well as barriers to existing resources supporting the development of such fathering skills remain (Bayley, Wallace, and Choudhry 2009; Sicouri et al. 2018). At play here are normative gendered frames wherein mothers’ alignment to primary care roles attracts services while dominant discourse around men’s reticence for help-seeking has likely impeded the development and availability of fathering tailored services (Oliffe et al. 2019). In addition, structural factors such as staff attitudes toward fathers and the predominance of mother-centered program content are significant service barriers for men (Panter-Brick et al. 2014). While father focused programs exist in small numbers, fathers are often unaware that such services exist or where to find them (Darroch et al. 2021; Summers et al. 2004) and advertisements for such services are found in areas less frequented by men, and are geared towards female clientele (Bayley, Wallace, and Choudhry 2009). Further, some fathers anticipate that programs will not appropriately address or meet their needs or fear that engaging in these types of programs will criticize and/or dictate how they should parent (Bayley, Wallace, and Choudhry 2009; Summers, Boller, and Raikes 2004).
While some empirical work has linked the gendered dimensions of men’s risk-taking
In light of these strength-based approaches to men’s health promotion and the significant gap in services for fathers facing marginalization, the current study presents a needs analysis of supports for fathers living in highly marginalizing conditions in Vancouver’s Downtown Eastside (DTES).
Masculinities, Fathering, and Tailored Social Services
The integration of masculinities (Connell and Messerschmidt 2005) and fathering (Dolan 2011; Dolan 2014) has afforded important empirical insights to contemporary parenting. Among these, Dolan’s (2014) research with working class fathers unpacked gender and relational parenting practices. Revealed were a plurality of fathering roles, relations, and identities (Dolan 2014) wherein marginalized men were understood as both challenging and sustaining hegemonic masculinities, while they made efforts to preserve their own masculine status within their subordinate sub-groups. Specifically, some men in Dolan’s (2014) study alluded to the tact necessary to balance the desire to express their emotions in ways in which such expressions would be deemed appropriate by other men rather than pose a threat to their masculine identities. Some characteristics of masculinities—such as protector and provider roles - were embodied by working class fathers as value-adding to their fathering projects (Dolan and Coe 2011). Contrasting these benefits were the limits invoked by masculine ideals of stoicism and emotional detachment—characteristics inhibiting contemporary discourses about involved fathering (Dolan 2011; Dolan and Coe 2011).
Taken together these contexts and factors shed some light on the tendency for fathers to be significantly less involved with and connected to child welfare services compared to mothers and, as a function of this, caseworkers focus their attention and work with mothers (O’Donnell et al. 2005). Dolan (2014) noted UK government policies have urged support services to engage fathers; however, men remain notably absent from such provisions. Policies and practices that focus solely on mothers rely on and likely reinforce dated understandings of mothering and absent provider discourses associated with fathering aligned to traditional masculinity (Oliffe et al. 2012). In essence, “strong gendering biases in parenting policies tend to reproduce a mothering rather than fathering cultural model of childrearing” (Panter-Brick et al. 2014, 1190). These critiques and calls for changes to services have been underpinned by contemporary fathering discourses encouraging dads to be involved, present and skilled in co-raising their children. The leap of logic is that beyond wanting to be meaningfully involved, men will know how to embody these contemporary fathering ideals. The tensions for those ‘new’ fathers who don’t have role models to draw on, and/or feel and fear being seen as ill equipped for the job, can be profound—and perhaps go some way to explaining the rise in male postpartum depression (Eddy et al. 2019). In this respect, it is not just the need for services targeting fathers; strategies for signalling men that there is strength in attaining those skills is also critical (Jenkinson 2016; Rossiter et al. 2017). For dads who have low income and/or education levels, being involved fathers can be especially challenging because of a lack of masculine capital to fully protect let alone provide for their family. Within this text accessing services—and by extension being unable to independently fulfil breadwinner roles—may amplify the marginalization of resource poor fathers.
Parenting practices of mothers and fathers are also gendered, relational and co-constructed. Contrasting reports of egalitarian attitudes about shared parenting by young adults (Milkie et al. 2002; Negraia, Augustine, and Chambers-Prickett 2018), some persistent gender disparities in parenting realities prevail (Borgkvist et al. 2020; Monna and Gauthier 2008). The division of unpaid labour is such that many women remain the primary providers of childcare and housework amid needing to maintain paid employment (Borgkvist et al. 2020). Men tend to transition to active parenting through fatherhood, though paid work remains central to many men’s lives and breadwinner identities. Such practices are somewhat traditional and deeply engrained gendered practices reinforced and normed by in social, economic, and political policies. Clearly, there are many perspectives and important considerations to developing social services for fathers. The current study, by including the perspectives of fathers, mothers and service providers offers much needed inclusivity in presenting a needs analysis of supports for fathers living in highly marginalizing conditions in Vancouver’s Downtown Eastside (DTES).
Methods
Background
This work emerged from a larger, mixed methods participatory action research (PAR) project to conceptualize and implement physical activity and wellness programs and resources with/for individuals living in the DTES. The purpose of this aspect of the project was to conduct a needs assessment of fathering supports for men living in the DTES, where residents face disproportionate levels of social challenges (Campbell et al. 2009). The community is characterized by high rates of mental illness, substance use, and communicable disease (Linden et al. 2013) and 67% of the population are low income (Raynor and Johnson 2007). Specifically, we explored the connections between masculinity, fathering, and health inequities from the perspective of three distinct groups: fathers, mothers, and service providers.
Framework
A PAR approach was the guiding conceptual and methodological framework for this study. PAR requires a commitment to authentically engaging community members, activism, and social critique, leading to positive social change (Kemmis and McTaggart 2005). This project was pre-empted by 2 years of PAR focused on women living in marginalizing conditions
Data Collection
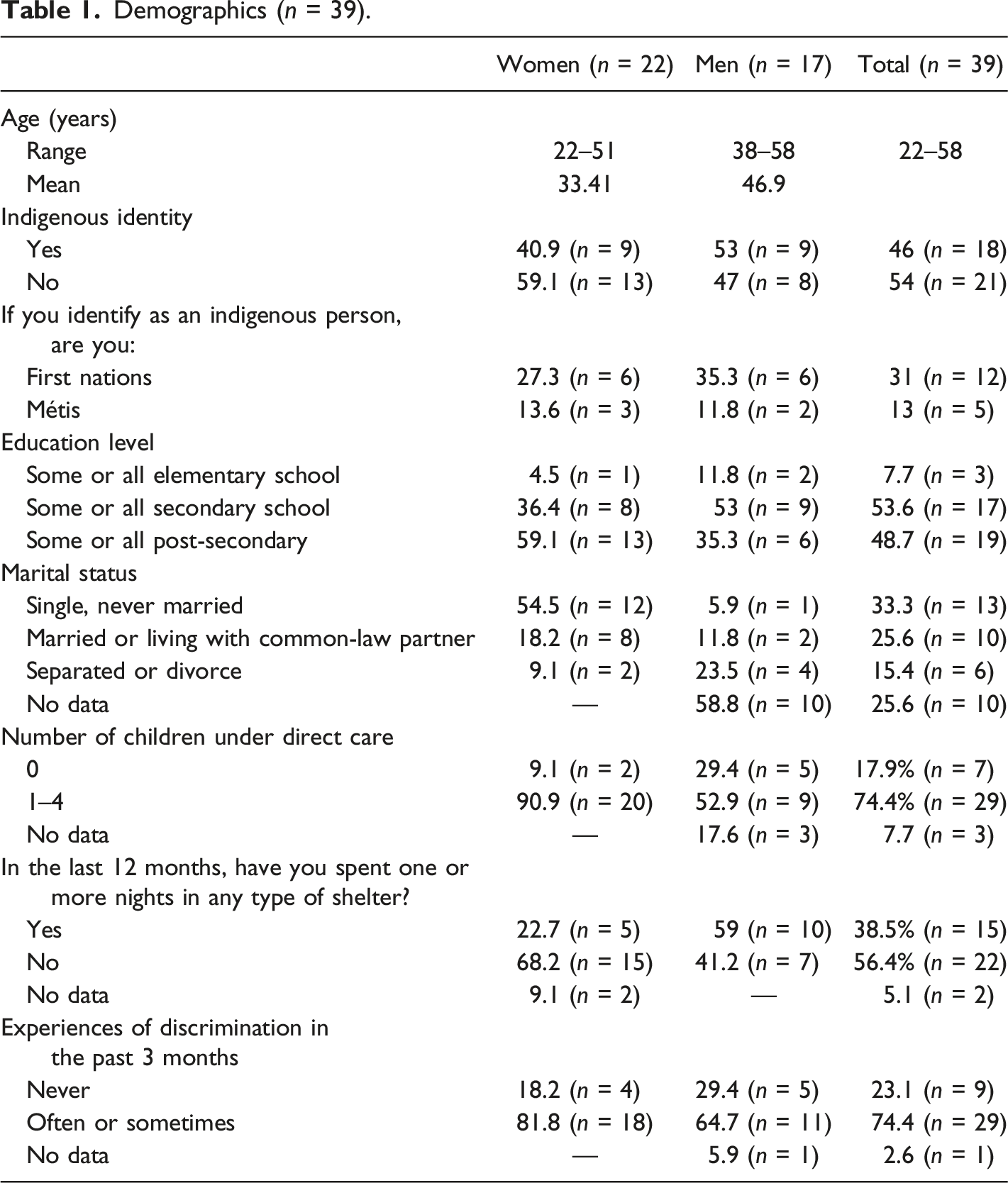
Data were collected between July 2018 and March 2019. There were three target populations for this research: (1) self-identified fathers who lived in and/or accessed services in the DTES; (2) self-identified mothers who lived in and/or accessed services in the DTES; and (3) key informant service providers in the DTES who provided support to parents. All participants were recruited through flyers posted at parent-serving organizations and through snowball sampling. Eligible participants were self-identified parents aged 19 years or older, or emancipated youth (or 16–18 years old, and no longer living with a parent or guardian). All participants understood and spoke English. The parent samples comprised 17 self-identified fathers and 22 mothers who attended one of four same-sex focus group interviews. The focus groups were co-facilitated by the first and fourth authors. All participants provided written informed consent prior to taking part and received a $25 honorarium, bus tickets, and a meal during the focus groups. The focus groups were semi-structured and addressed questions including: What challenges do you face as a parent in the DTES? In what ways are these challenges different for men and women? What programs are partner inclusive (for social services and physical activity)? The focus groups lasted between 60–95 min. Key informants were asked interview questions including: In what ways does your organization’s policies support moms, dads, and both parents? In what ways are these challenges different and diverse for men and women? The semi-structured interviews were 20–60 min, audio recorded and transcribed with participant written consent.
Participants
Demographics (n = 39).
Data Analysis
All focus group and interview data were transcribed, accuracy checked, and uploaded to NVivo10 a qualitative program used to house and code data segments. Each of the three cohort’s data were reviewed separately to inductively derive thematic findings from each sub-group. Drawing on Braun and Clarke’s (2006) six-step thematic analysis process we engaged in the following: first, all authors became familiar with the data in each cohort by listening to recordings and reading and re-reading transcripts; second, the authors generated preliminary codes to allocate data segments; third, we reviewed and adjusted the data in each code to develop preliminary themes; fourth, all of the authors met to discuss and revise the themes and sub-themes drawn from these analyses for each cohort; fifth, we further defined and differentiated the themes and their labels deciding on illustrative quotes to represent the findings; finally, in the writing up of the current article our analyses continued iteratively to ensure the rigor and representativeness of the findings. Upon authors review and discussion of the data, codes were continually adjusted and refined, collapsing or expanding to appropriately reflect findings. Field notes taken during focus groups and interviews were reviewed and consultation with the interviewers and Community Advisory Board members was conducted to ensure rigor. As we progressed through this six-step process, our results reflected what prevailed in each cohort of the sample. The essence of what the three sub-groups discussed was similar; however, the nuances of their arguments, experiences and perspectives were best illustrated by presenting thematic findings for each cohort. These results were drawn from explicitly addressing the research question: What are the connections between masculinity, fathering and health inequities?
Results
Through our analyses, we inductively derived the following themes: (a) “we need a he-way”: Fathers arguing for men-friendly services; (b) “I had to do all the hard work”: Mothers identifying relational impact of fathers’ barriers to services; and (c) “there is nothing out there for them”: Service providers acknowledging the lack of father-focused programs.
“We Need a He-way”: Fathers Arguing for Men-Friendly Services
We need a He-way emerged from the fathers’ evaluation that few tailored services existed for them, and the language in the aforementioned quote referenced Sheway (Coast Salish word for growth), and the name of a harm reduction pregnancy outreach program for women in the DTES. Within this context, a common way to articulate the lack of men’s services was to point to the services that were available to women. As a 38-years-old father affirmed that, based on his experiences, there were few supports available to men: There is no support. There is none for single, male fathers here in the DTES, there is nothing. There’s no programs. Literally […] one day I had one of those little step counters and just thought for fun let’s see how many clicks I’ll do in one day [to try and access services]. By the end of the day, I did 14 clicks [14,000 steps] in one day. Trying to find just anything that will kind of help me in my situation…that would help me be a better father, to me it just feels like there is nothing. […] I’m trying to stay with my kids, I’m trying to be there for my kids, I’m trying to take more responsibility for my kids, but it is hard, it is really, really hard.[…]. I’m getting tired, I’m angry…there is nothing.
In this man’s context, and in many fathers’ narratives, the lack of resources was detailed alongside their privation of capital—and reliance on multiple but distinctly sex-specific services. Again, the lack of masculine purchasing power and inability to be self-reliant were ever-present in the men’s testimonies about needing help. These frustrations often culminated aggravating and triggering a range of behaviours—many of which were potentially self-harming and harming of others.
Later in the conversations, this father summated, “we need a He-way,” a call for action underpinned by his masculine values in wanting to be in his children’s lives, as well as the challenges he had finding the resources to make good on that goal. Herein multiple layers of inequities emerged, amplifying his ‘situation’ and a subordinate status within masculine hierarchies (that he needed such services) and across gender relations (that he could not access female only services). Many men described themselves as committed to accessing services for their children; however, they noted the barriers were time consuming and physically and emotionally draining in that the frustrating outcomes often reinforced their inequities and subordinate status.
Fathers also reported feeling tired from having to continually advocate for themselves at women-focused organizations. A 49-years-old father, currently parenting one child, shared his experiences of trying to work with the Ministry of Child and Family Development (MCFD) shortly after receiving full custody of his child: I went there [MCFD office] three days in a row when I was trying to get everything transferred over […] and the receptionist […] was actually really rude to me and I was almost in tears. […] I’m going through all the stress of separation and social workers and I’ve got to just tell her [partner] to stay the hell away, otherwise I’m going to lose my son, and trying to get all the finances, and what am I allowed to get, and what do I have to do, and how long does it take, and she was just really rude to me.
Herein, this father detailed his experiences of discrimination as gendered in that he was accessing traditionally female services while feeling pressure to stoically handle emotional distress brought on by his mistreatment in addition to the fractured relationship that had brought him to need those resources in the first place. Within this context, beyond the need for services, it was also the etiquette required to access them. In essence, the men had to be complicit and perhaps apologetic in needing to access services that were not explicitly or typically for them. The complexities of inequities as relative and relational emerged in these examples—emphasizing the lack of capital some men experienced in advocating for tailored men’s resources in an effort to support their families.
Although most men reported feeling excluded by mother-focused programs, resources, and policies, a 58-years-old Indigenous father and grandfather was critical of the demands for ‘he way’ services—suggesting that the issues were not about services (or the lack thereof). Instead, he argued the ‘problems’ resided in men themselves: I don’t really think there are any obstacles [to accessing resources]. I dealt with my alcohol and drug problem. That’s the underlying problem with our people down here, they’re addicts or they’re alcoholics, that’s the problem, and as long as they have that problem, they’re going to rationalize it forever. Age is not a factor. You can be six years old and an alcoholic or you can be 70 years old and be an alcoholic. It is an individual thing. We can kind of rationalize it to death.
This participant’s view raised complex counter arguments meshing substance use, addictions, and neo-liberal notions of personal choice and responsibility. In essence, interrogated were the reasons for men needing services as the core issue, rather than the services themselves. The intricacies of fatherhood in the DTES were also shaped by the disproportionate levels of social challenges. Indeed, the barriers men faced in accessing services were rooted in social and cultural norms that placed women as the central caregivers for children. Pointed out here were assertions that men needed to take care of their own lives to effectively father their children—and/or legitimately qualify for services. Though talking to what some men didn’t or couldn’t do in this regard, the participant signaled his alignment to an idealized self-reliant masculinity in distancing himself from the group’s view that the lack of tailored services was the central issue.
“I Had to Do All the Hard Stuff”: Mothers Identifying Relational Impact of Fathers’ Barriers to Services
The second theme was drawn from the mothers’ data, wherein participants conceded their partners, or fathers they knew in the DTES, did not have adequate access to resources and services, in doing so they talked at length about the implications of this for their own well-being. One 32-years-old mother quipped, “I had to do all the hard stuff”, amid many mothers talking to the lack of support for fathers in highly marginalized communities. Mothers simultaneously affirmed and challenged traditional masculinities associated with fathering and recovery in making recommendations for services including increased access to services, acceptance of fathers, and the creation of some gender specific services for dads in the DTES. A 32-years-old mother providing direct care to two boys, explained from her experiences, The majority of programs […] do not cater to that male parent. […] And if they do […] they have to do it as a single person. Not as a single dad, but as a single person. Without the same support. Say if my husband wants to get clean with me, well we couldn't do it. We couldn't raise our kid at the beginning. I had to be taken away for 16 months, from my family in order to get to keep my family. I'll do whatever I need to do, but where was he? He was stuck at home not given the supports [… ] I had to do all the hard stuff.
This participant further discussed the supports she had in place to do the challenging work of recovery, contrasting the absence of those resources for her partner and father of her children. She elaborated, I had to change my life, like change everything of who I was. And like I was—I felt alone. We've been on the same page for eight years, and all of a sudden, we just get uprooted, and I've got all this work under me, and all this clean time, and stuff and he never got the chances that I got. So it sucks. It messes up our family unit.
The complexities of gender relations were ever present in the woman’s account, pointing to the long-standing co-dependency and the discordance that arose when she was not actively using drugs amid her partner’s continued substance use. The habitus of their relationship was, in essence disrupted by the uptake of services by the mother toward recovery and the father’s continued drug use. As this mother shared, the focus on her recovery and the supports to put her health first, were very important, and to some extent her efforts for being clean were driven by feminine ideals about nurturing and caring for her family. That said, she also had to forgo being with and caring for her partner in prioritizing their children’s well-being. Indeed, the lack of supports for her partner further marginalized and potentially replicated the harms her family had long endured. Unfortunately, many of the women shared similar experiences. A 23-years-old single mother of one shared the experiences of her child’s father: He's out there, and he's still struggling with his addiction and stuff right. And like he doesn't know where to go, so I don't feel angry because it's not his fault, that there is no support, right? It definitely is something that needs to get changed…men need that level of support too. The difference between genders doesn't mean that they don't need it too, right?
This participant excused her child’s father for his lack of parental involvement because she identified with his traumas and substance use struggles in reckoning that he did not have access to the services that she had. She then acknowledged these service barriers were directly related to sex differences. She further challenged the gender norms that perpetuated her situation to heighten and amplify the health inequities her partner (and by extension she) endured. Again, the relational aspects of gender emerged here to signal the complexities of well-intentioned (but potentially ostracising) gender-specific care for women. A 31-years-old woman currently caring for one child explained that she and her partner were separated amid succinctly arguing that that living arrangement should not disadvantage him (or other men): Men that aren't in a family union or together, if they have a child, they should have the same chance to be there for that child that we [women] do.
There was strong consensus among the women that fathers deserved the right to be in their child’s life. In sum, men’s lack of access to supports ultimately were situated by the women as creating greater stress for mothers and their families by virtue of the demands of raising children being placed entirely on the mothers. Herein feminine ideals weighed heavily on many mothers, both in respect to caring for their children and their explicit concerns for the health (and rights) of the father of their children. These normative femininities were also reinforced (albeit inadvertently) by health services and structures providing targeted care that implicitly (and sometimes explicitly) excluded men.
As grateful as the mothers were for the services they received, they also cited examples of fathers being excluded in lobbying for changes. The women discussed the need to accept fathers in sharing stories about witnessing the exclusion, both subtle and explicit, fathers experienced when trying to access or live in designated women-centered spaces. As a 33-years-old mother or two shared: Our building is a women-led building
This mother’s testimonial made a point about the limits of positive discrimination (protecting mothers from the harms their partners might invoke), a situation she elaborated on in chronicling how her partner and fathers in the community continued to face many challenges to parenting in the DTES context. The women suggested that some men experienced being ‘othered’ through these discriminatory practices and their lack of power to contest these situations and structures. The acceptance of men was deemed crucial and as a 39-years-old mother of two explained, the recognition of her partner extended to accept her choice to be with him: Some of us are fortunate to have the fathers and some aren't, right? But, I just feel supported when people accept my choices also, right. Like, here [women-centered organization] I get supported with my boys to raise my kids the way I want and have a partner.
This inclusivity was typically the exception rather than the rule, to the extent that some women were forced to choose between services and their partner. Women elaborated that their choice in partners was confined by structural and systemic issues. As a mother parenting two children succinctly stated, “cause sometimes when the ministry doesn’t like the person that you’re with, then there you go, well you have to choose.” She explained needing to decide between continuing to support her children through being housed or maintaining (and by extension relying on) a relationship with her partner. Many fathers were dealing with inaccessibility to resources, including housing, wherein their partnership with the women could nix their families’ entitlements.
In terms of potential remedies many women argued for tailored and gender specific resources and programs aimed at fathers. The women simultaneously acknowledged and challenged masculine norms within their communities in arguing for these resources. A 29-years-old mother parenting one child described how she and other mothers were trying to actively support single parenting fathers and further engage them in programs. She stated: We want more of those dads to come too […] I know those dads; they talk to me. And I see how they struggle.
She explained that although some activities were open to all individuals who were parenting, the programs didn’t appeal to or affirm men as end-users of the service: “some activities are open to fathers, right? Because I know my dad and my partner can come. But the thing is the activities that we do that are more like, for women.” Another participant added to this explanation: For men it’s like they like to do stuff together, and they don’t want to sit down and gush over their issues and share their vulnerability, but in that different space where they’re doing an activity together, I think it can be more open for that kind of sharing.
This mother contrasted “typically” feminine conversations that embraced self-disclosures and the sharing of feelings with masculine forms of social engagement. She suggested that men connected with one another by “doing”—rather than talking or expressing their thoughts. Other women in the focus group confirmed that men don’t like to sit around and chat—they would rather “work with their hands,” “fix stuff” or “play cards.” Despite the overall argument to offer men services equal to those offered to mothers, many of the women agreed that men required “masculine” activity-based opportunities. Relied on in these examples were masculine norms wherein the women asserted the ill fit of their services and interactions based on their knowledge of the men in their lives. Indeed, while sharing their opinions on the fathers in their lives requiring masculine forms of engagement, the women ran the risk of further perpetuating masculine, and sometimes harmful, stereotypes.
Mothers reported their partners perceived barriers to accessing programs because men were seldom represented in the group or among the staff running programs. A 33-years-old noted the need to recast masculine norms to build alternative cultures that might permit and affirm men’s attendance: I know even if he goes to any family events […] it's just all women, he's the only guy. He feels kind of uncomfortable sometimes because he wishes there was more fathers that would go, because there is a lot of single dads.
Within this context women suggested that a force fit with existing services held little value for men (or women) and expressed that a critical mass of men might adapt and change to comfortably inhabit and meaningfully contribute to these feminine cultures. Indeed, there was considerable discussion about how men felt othered in mother-focused programs, and how this was a barrier to attending.
“There Is Nothing Out There for Them”: Service Providers Acknowledging the Lack of Father-Focused Programs
The thematic findings drawn from the service providers highlighted how female-focused programs knowingly and, at times, unknowingly excluded fathers. A female service provider who had worked with a women-focused organization for 3 years noted that fathers often felt left out of services. She stated, A lot of places work with mothers and children, by making that the primary focus it does prohibit the role of the father in the family, so I think that our organization is becoming more open to that idea and the gaps that we’re not addressing the family, or we’re not helping the mom in the context of the family because we’re not doing anything for fathers.
Herein the service provider conceded the imbalance and overall implications for reducing family care benefits by virtue of men being excluded. There was certainly awareness of the barriers for men to access services, as well as discussions about the complexities of the diverse situations in families living in the DTES. The services and resources were, first and foremost, designed in a way to offer women and children safety and protection, as per the explicit legislated priority of these finite resources. Service providers were bound by higher level policies and mandates to triage the women’s care ahead of the men. This service provider went on to explain that she hoped her organization mandate would shift in order to advance family care by including some men in their services. A service provider with 20 years of experience in the DTES community summated when organizations made it difficult for fathers “it takes the woman out the door, and she doesn’t want to participate.” This service provider recognized the relational impact and implications of excluding fathers. In this context, end-users and some providers had little agency in deciding to whom the existing services were delivered. In essence, deeply rooted and institutionalized gender norms invoked structural barriers which perpetuated women’s primary role as a caregiver. This service provider, who had worked in the DTES for 20 years, explained, Our program is mandated for women first, the way our funding comes in, that if we were to partner, our main focus would still be the women and we would pay more attention to them and making sure their needs are met. It is just the way we are set up and we’re trained to work. I don’t think maybe there’s enough services for these fathers. Some have come from … incarceration, some need to work on some issues of their own. Some really want to work on themselves but maybe can’t find the right supports.
Recognizing staff were trained to treat women ahead of their male partners demonstrated how well intended policies can inadvertently further marginalize women because their partners do not have the same service rights. Provided here was an example of institutionalized gender wherein the structures paying for the care governed and directed those finite health resources to women. Imbued with scarcity, the care was aimed at aiding women who experienced significant health inequities. This participant’s comment reiterated the context that drives gendered health policies and practices. As a female key informant who has worked in housing support for 10 years, shared, We have had applications, not a lot, but we’ve had applications from single fathers that we’ve rejected because our program agreement [housing contract] is signed by the women. We have fathers that live here, but the agreement is always in the women’s name. That could be prohibitive if a father couldn’t access housing, access supported housing, or if there was a reason that he couldn’t be a part of that family dynamic anymore.
In the social context and complexities of parenting in the DTES, women were prescribed the role of sole caretaker, even though they may have male partner supports. It can be reasonably argued that some reverse but inequitable patterns of exposure to risks were occurring by virtue of these gender biases (women are housed, and men are less prioritized). That said, protection seemed to be at the centre of these decisions, and such practices can be explained and justified as refusals to be complicit in sustaining dominant masculinities. Specifically, masculinities that rely on power differentials to wield patriarchy in subordinating women (and some men). Therefore, by equipping marginalized women with important family health resources most service providers rationalized their priority as directing care to those whose circumstances were most vulnerable
In addition to the institutionalized gender issues, a range of operational barriers were shared as reasons why men were less likely than women to access health resources. A service provider with 11 years of experience, explained fathers were often excluded simply based on the time programming is offered: Some of our dads work during the day or pick up labour work where they can, so it’s hard for them to access resources, daytime resources.
Indeed, programs and services were offered during weekdays to increase the ease of access for women and children. Again, within this context the structural challenges emerged to advantage the female clientele for whom the services were built in the first place.
There were some caveats and counterpoints shared by participants contesting the claims that men could not access services. A key informant, who had 20 years of experience, argued that the resources afforded to fathers by her organization were generous. She explained: With our specific housing program, it is for single mothers only, so only mothers and their children can live there, but fathers are welcome to visit as long as they are clean, sober and safe. So, we do have visitation hours, which I think is quite generous, because it’s from 8 in the morning until 11 at night, so that’s your whole day you can spend with your family if you wish.
Evident here were concessions that were intended to include men and protect women. Provisional and behaviour reliant visitation rights could be secured, but the underpinning potential that some fathers had to sleep in single room occupancies (SRO’s), shelters, or on the streets was ever present in these arrangements. Moreover, some mothers were left to care for children throughout the night without support from their partners, as a by-product of these rules. The same service provider noted, Different fathers are at different points in the path in terms of their own wellness, so we definitely in terms of the housing department will do what we can to help fathers access resources and support them, but our priority is mom and the children.
The service providers were trained and supported to work with women and children, in ways that perpetuated a range of gender norms (and the potential for challenges for some moms and dads). In sum, the service provider’s accounts confirmed the challenges for providing dyadic care with resources explicitly inclusive of moms and dads. Within this context, there were strong arguments for gender-specific services, and mothers as the predominant carer for family were rightly targeted. There was also a resistance to building the equivalent for men, and this likely flowed from the actuality of finite resources and concerns that the women’s care would be diluted through diversifying to men’s programs.
Discussion
Fathers who are parenting in highly marginalizing conditions found in the DTES are poorly served by the current programs, services, and organizational policies, and there is little discernment about where men reside on the continuum between being effective involved fathers and threats to their family’s well-being and safety. Our findings align with research by Brown et al. (2009), who discussed the invisibility of fathers in services. Moreover, we affirm and contextualize two broad barriers to services identified in the literature on fathers: (1) parenting services tend to be mother-oriented; and (2) parenting services often exclude fathers through program content, delivery, and/or scheduling (Bayley, Wallace, and Choudhry 2009). While all the participants reported services as mother-oriented, there were diverse reactions (and some potential remedies) offered for this long-standing trend. For example, the mothers reported that the programs available to all family members excluded their partners or their children’s father in arguing the additional pressures that resided with mothering roles by virtue of these arrangements. In agreement, but more cautionary and conservative in suggesting changes to current services or building tailored services for fathers were providers. Fathers critiqued being excluded from services in arguing for change. Clearly, the work of parenting is still deeply gendered, as is the provision of care, and this is perpetuated by structural factors that govern the care provided and influence the individual agency of parents and providers.
The intersections of masculinities and marginalization further challenged men’s ability and/or desire to access services. As Dolan (2014) noted, tensions between masculine and fathering identities can emerge especially when men are resource poor relative to other dads. The heterogeneity of working-class fathers wherein Dolan contrasted men’s participation in childcare as a part of contemporary masculinity with working class fathers who adhered to traditional working-class ideologies also resonated with the current study findings. Specifically, the fathering and mothering practices and men’s service needs reflected the diversity of masculinities and femininities operating within the unique institutionalized gendered frames operating in the DTES (Johnson and Repta 2012). A milieu characterized by marginality and scarcity the current study findings afford much needed insights from an array of viewpoints to the gendered dimensions (and challenges) of fathering in the DTES.
While gender is at the heart of the tensions permeating the current study findings, gender-specific considerations must also be central to the planning and delivery of services to parents in the DTES context. All the sub-cohorts agreed there could be important ‘family’ gains by better supporting fathers. The fathers argued for strength-based inclusivity in childcare and services; the mothers lobbied inclusiveness of fathers to reduce their sole-parenting burden; finally, the majority of service providers conceded the limits of current gendered approaches to care provision might encumber many mothers (and some fathers). As Connell and Messerschmidt (2005) explained, gender is relational and “women are central in many of the processes of constructing masculinities as mothers and partners…” (848). In the current study, mothers both challenged and perpetuated fathers’ alignments to masculine norms. For example, the men in this study transgressed some normative masculinities by needing and seeking out supports and services. Yet, it might also be reasonably argued that they were claiming patriarchal dividends in arguing they should be able to freely access family and fathering services (despite the backdrop of feminine ideals being deeply tied to family care).
Many of the parents who participated in the current study identified as Indigenous, and while we did not compare their experiences with non-Indigenous participants, it is likely that they face unique challenges. Related to this, a scoping review examining eight programs that focus on Aboriginal and Torres Strait Islander men and parenting confirmed a dearth of research to inform tailored fathering programs to support families and communities (Canuto et al. 2019). These findings underscore the need for change, in that many Indigenous fathers (and mothers) were interested and actively seeking supports to enhance their engagement with their child (ren) and families. Gender-specific programs and interventions, focused on fathers living in marginalizing conditions may benefit parents and the overall health of families. There is evidence that men are reticent to seek help and supports (Addis and Mahalik 2003); thus, gender-specific service provisions, as argued by the mothers in the current study, may secure men’s engagement (O’brien et al. 2005; Sicouri et al. 2018; Sierra Hernandez et al. 2014). Dolan (2014) argued a gender lens is a valuable analytic tool to understanding parenting expectations and practices, and clearly parenting and gender roles, relations, and identities in the DTES community are layered with complexities of poverty, substance use, lack of social status, income, and significant traumas and injury. Arguably, efforts to support fathers in the DTES context should respond to men’s health inequities. However, as with many marginalized groups, scarcity prevails in rationalizing and perhaps rationing the provision of services. In line with Randles’ (2018) assertion that marginalizing conditions undermine men’s abilities to live up to masculine norms as breadwinners, the fathers in the current study were receiving government social assistance and did not hold traditional jobs or primary provider roles for their families. Further, researchers have purported that minority men work to reaffirm their gender identity by embodying cultural and ethnic-specific aspects of manhood (Griffith 2015). Marginalized and subordinate within masculine hierarchies, “the layering, the potential internal contradiction, within all practices that construct masculinities” (Connell and Messerschmidt 2005, 852) were evident among the fathers in the current study.
The limitations identified in this study offer direction for future research. The small sample size of fathers in this research, and importantly the high mean age of the father’s (47-years-old), may not be representative of the experiences of younger fathers in the DTES, and elsewhere. Expanding the current research to gain (and compare) the insights of younger fathers who are experiencing inequities would be valuable.
A substantial number of the participants in this study identified as Indigenous and while our findings may not be generalizable to Indigenous fathers living in other contexts due to the unique social landscape of the DTES, they begin to shed light on the experiences of Indigenous fathers living in marginalizing circumstances, and echo calls for increased access to services for Indigenous fathers (Ball 2009). Finally,
The current research findings are novel as the fathers, data triangulation and the study setting operate outside of the work that has typically dominated masculinities and men’s health research. Our findings provide much needed insights to men’s (and women’s) health inequities in this regard—and the complexities that accompany those relational circumstances. There was consensus that the support systems in place need to be reconceptualised for fathers based on the recognition that parenting is deeply bound in social structures as mother led. However, the call to action for father-focused resources is easier lobbied than leveraged especially given the political and practice pressures for addressing health inequities. A helpful starting point might be to recognize that some traumas and triggers are shared across genders in catalyzing local, provincial, and federal level policies to be more inclusive in their social justice agendas. This includes revising and/or creating institutional polices and funding structures to engage under-resourced fathers with services. Such support for integration should maintain services for mothers but include gender-specific programming for fathers in the DTES. This might be argued a gender mainstreaming but afforded by these tailored services can be significant benefits (and protections) for family health. Pivotal to such programming is the need for formal evaluation of these tailored services to guide adjustments both in terms of sustainability and scaling potential. As the World Health Organization remind
Footnotes
Author Note
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in Banting Research Foundation Award # 393666.