
Abstract
Background:
Traumatic amputations are morbid complications of blunt traumatic injury. Given the contaminated nature of these wounds, surgical site infections (SSIs) are frequent in this population. The natural history of these wounds following guillotine amputation is not well described. This study seeks to define the relation between operative technique, timing, and SSI.
Patients and Methods:
Using our institutional trauma registry, we obtained data for all patients with an admitting ICD-10 code for an amputation. Those that underwent amputation for non-traumatic indications were excluded.
Results:
Between 2013 and 2023, 100 patients with traumatic extremity wounds presented to our Level 1 Trauma Center and subsequently underwent completion amputation. Most patients were males (70%), and the mean age was 42.7. Of the 100 patients, 65 underwent guillotine amputation, 39 of which occurred within six hours of arrival. Of the studied population, SSI developed in 24% of them. The patients in the SSI group compared with the non-SSI group had a mean hospital length of stay (LOS) of 30.2 days (vs. 16.5, p = 0.007). Patients who did not undergo an attempt at salvage had a mean mangled extremity score of 8.25 (vs. 6.14, p < 0.001), a mean injury severity score of 19.4 (vs. 14.5, p = 0.014), mean lactate at presentation of 5.37 (vs. 3.18, p = 0.004), and mean ICU LOS of 8.4 days (vs. 4.2, p = 0.021). Patients who underwent guillotine within six hours had a lower risk of SSI (12.8% vs. 31.1%, p = 0.036).
Conclusions:
Understanding the impact of surgical timing and operative technique on SSI will inform surgeons about the best course of action when these difficult cases present to the trauma center. On the basis of these findings, early guillotine amputation in patients likely to undergo amputation was associated with a decrease in the rate of SSI.
Keywords
Traumatic amputations are an uncommon but morbid complication of traumatic injury. 1 These injuries can involve substantial soft tissue loss, blunt vascular and nerve injury, and open long bone fractures. Approximately 185,000 patients undergo amputation of an upper or lower extremity each year, and of these patients, trauma accounts for an estimated 16% of amputation-related hospital discharges. 2 A study utilizing the National Trauma Database demonstrated that nearly 83% of traumatic injuries resulting in amputation are because of blunt mechanism. 3 The most common mechanism of injury is auto versus pedestrian (AVP), followed by motorcycle collision (MCC). Lower extremity amputation is more common in AVP and MCC, and those involved in motor vehicle collisions are more likely to undergo upper extremity amputation. 3
Initial management of these injuries is commonly by guillotine amputation: a through-bone or through-joint amputation at or above the level of injury with control of hemorrhage and typically without formalization. The amputation site can then be serially debrided and formalized later when the patient is resuscitated and physiologically stable. At the time of the initial injury, if the limb appears viable and functional outcome can be preserved, attempts at limb salvage can be performed.
Many scoring systems exist to aid in decision-making for management of these injuries. The Mangled Extremity Severity Score (MESS) was proposed in 1990 by Johansen et al. 4 as a means of predicting which traumatic extremity injuries would ultimately require amputation. The MESS utilizes a scoring system on the basis of skeletal and soft tissue injury, limb ischemia, shock, and age. This, along with other scoring systems, 5 is an adjunct in the operating surgeon’s decision-making between an amputation at the index operation versus an attempt at limb salvage.
Given the frequently contaminated nature of severely injured extremities, surgical site infections (SSIs) are frequent in this population. Guillotine amputation as a damage-control tactic before formalization has been shown to reduce infectious complications in other patient cohorts, 6 but this has not yet been demonstrated in traumatic extremity injuries. Delayed closure of traumatic amputations has likewise been shown to decrease the likelihood of SSI, 7 but the natural history of these wounds following guillotine amputation versus those that undergo an attempt at limb salvage is not well described. Although preserving as much extremity function as possible is a noble goal, there is a paucity of literature concerning complications related to failed attempts at limb salvage. The authors of this study have concerns that this practice may result in worsened infectious complications compared with the early amputation groups. The objective of our study is to seek comparison between operative technique, timing, and SSI in patients who undergo early amputation versus those who fail limb salvage.
Patients and Methods
Following approval from the institutional review board, the trauma registry from our Level 1 trauma center was queried over a period from January 2013 to December 2023 for cases in which adult patients (18 y or older) underwent amputation following traumatic extremity injury. Data were obtained for all patients with an admitting ICD-10 code for an amputation. Those that underwent amputation for non-traumatic indications were excluded.
A standard set of registry parameters were gathered pertaining to patient demographics, initial clinical condition, details of injury, emergency department (ED) details, and inpatient details. SSI was recorded in the trauma registry based on standard American College of Surgeons criteria. Data regarding the operative timing and surgical technique were gathered by chart review of operative reports. These parameters include time from arrival to guillotine amputation, arrival to first debridement, and arrival to closure. They also include number of operations on the extremity that was amputated and whether the amputation was converted to a higher level. During chart review, the MESS at the time of arrival was also calculated for each case. The time from admission to initiation of antibiotic agents and the total duration of antibiotic therapy were also gathered by chart review.
Patients were compared with on the basis of whether they experienced an SSI at the amputation site. They were also compared with on the basis of timing of their operation. Those that received a guillotine amputation before six hours were compared with those that did not. The 6 hour cutoff to define the “early” guillotine was on the basis of Western Trauma Association guidelines by Scalea et al., 8 which list ischemia greater than six hours as a predictor of need for amputation. Patients were also grouped on the basis of whether they underwent guillotine at index operation or an attempt at limb salvage, which was defined as an operative procedure before a guillotine amputation.
All categoric variables are expressed as a percentage of the total and were compared with using the Chi Square test. Continuous variables are expressed as the mean ± SD and were compared with using the Student’s t-test. All statistical analyses were performed using SPSS version 28.0 (IBM Corp., Armonk, NY).
Results
From January 1, 2013, to December 31, 2023, 110 cases were identified through the trauma registry that underwent amputation for traumatic extremity injury. Of these, 2 had amputations but died before guillotine amputation, 4 had partial amputations of hands or feet and underwent successful limb salvage, and 4 had amputations as the result of limb ischemia not due to the original injury. These 10 cases were excluded from the analysis, resulting in a study group of 100.
Of these 100 patients, 85 underwent lower extremity amputation, 14 underwent upper extremity amputation, and one patient underwent both an upper and lower extremity amputation. Demographics, injury severity measures, and surgical management characteristics are shown in Table 1. The overall SSI rate was 24%. There was no significant association between SSI and patient demographics (age, race, gender), BMI, injury severity (MESS, injury severity score [ISS]), or ED vitals. There was also no significant association between SSI and time to initiation of antibiotic agents (4.42 h ± 9.86 vs. 3.77 ± 9.93, p = 0.391) or duration of antibiotic agents (106.75 h ± 97.52 vs. 88.66 ± 109.21, p = 0.236). Patients in whom an SSI developed had a greater likelihood of requiring a conversion to a higher amputation compared with those in whom it did not (25.0% vs. 7.9%, p = 0.025) and had a greater number of operations on the affected limb (7.25 ± 5.59 vs. 4.05 ± 3.51, p = 0.013). Patients in whom an SSI developed also had longer hospital length of stay (LOS, 30.17 d ± 21.56 vs. 16.51 ± 13.19, p = 0.007), but no difference in ICU LOS (9.67 d ± 12.02 vs. 5.62 ± 8.80, p = 0.137).
Patient Characteristics and Surgical Timing and Therapy
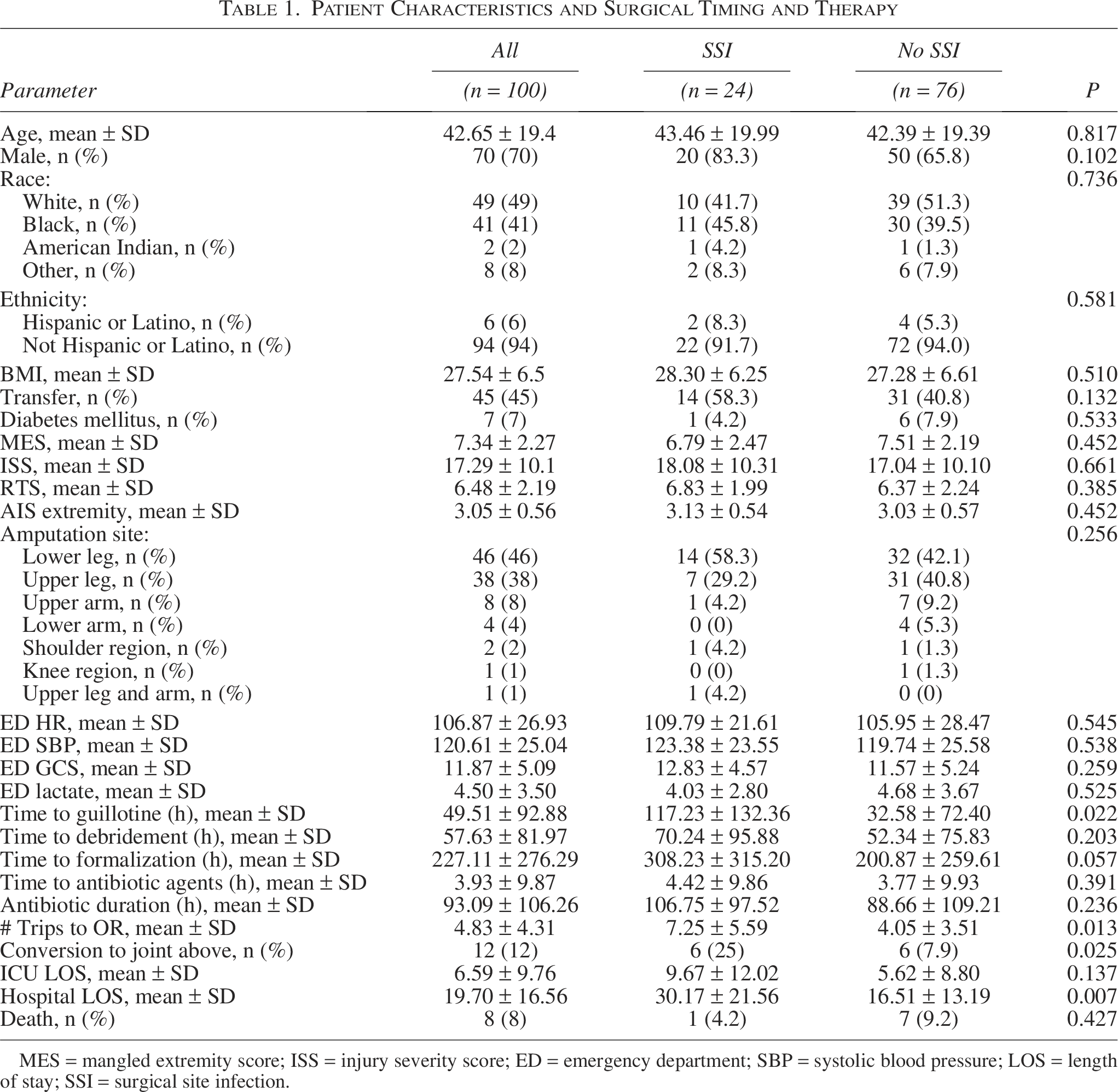
MES = mangled extremity score; ISS = injury severity score; ED = emergency department; SBP = systolic blood pressure; LOS = length of stay; SSI = surgical site infection.
Sixty-five patients underwent guillotine amputation of which 39 occurred within six hours of arrival. Patients who underwent guillotine amputation at index operation had a greater MESS (8.25 ± 1.85 vs. 6.14 ± 2.23, p < 0.001) and ISS (19.42 ± 10.30 vs. 14.47 ± 9.22, p = 0.014) compared with those who did not. The guillotine cohort had a greater heart rate (113 ± 28 vs. 99 ± 23, p = 0.014) and lactic acid at presentation (5.37 ± 3.88 vs. 3.176 ± 2.29, p = 0.004) and were more likely to receive a blood transfusion (71.9% vs. 39.5%, p = 0.001). There was no significant difference in the total number of operations for those who underwent guillotine at index operation versus those that did not (4.95 ± 5.18 vs. 4.67 ± 2.77, p = 0.75). Patients who underwent guillotine at index operation also had longer ICU stay (8.42 d ± 11.14 vs. 4.16 ± 6.96, p = 0.021). There was no significant difference in SSI between those that underwent guillotine at index operation versus those that did not (17.5% vs. 32.6%, p = 0.082). Demographics, injury severity measures, and surgical management characteristics for these groups are shown in Table 2.
Comparison On the Basis of Index Operation
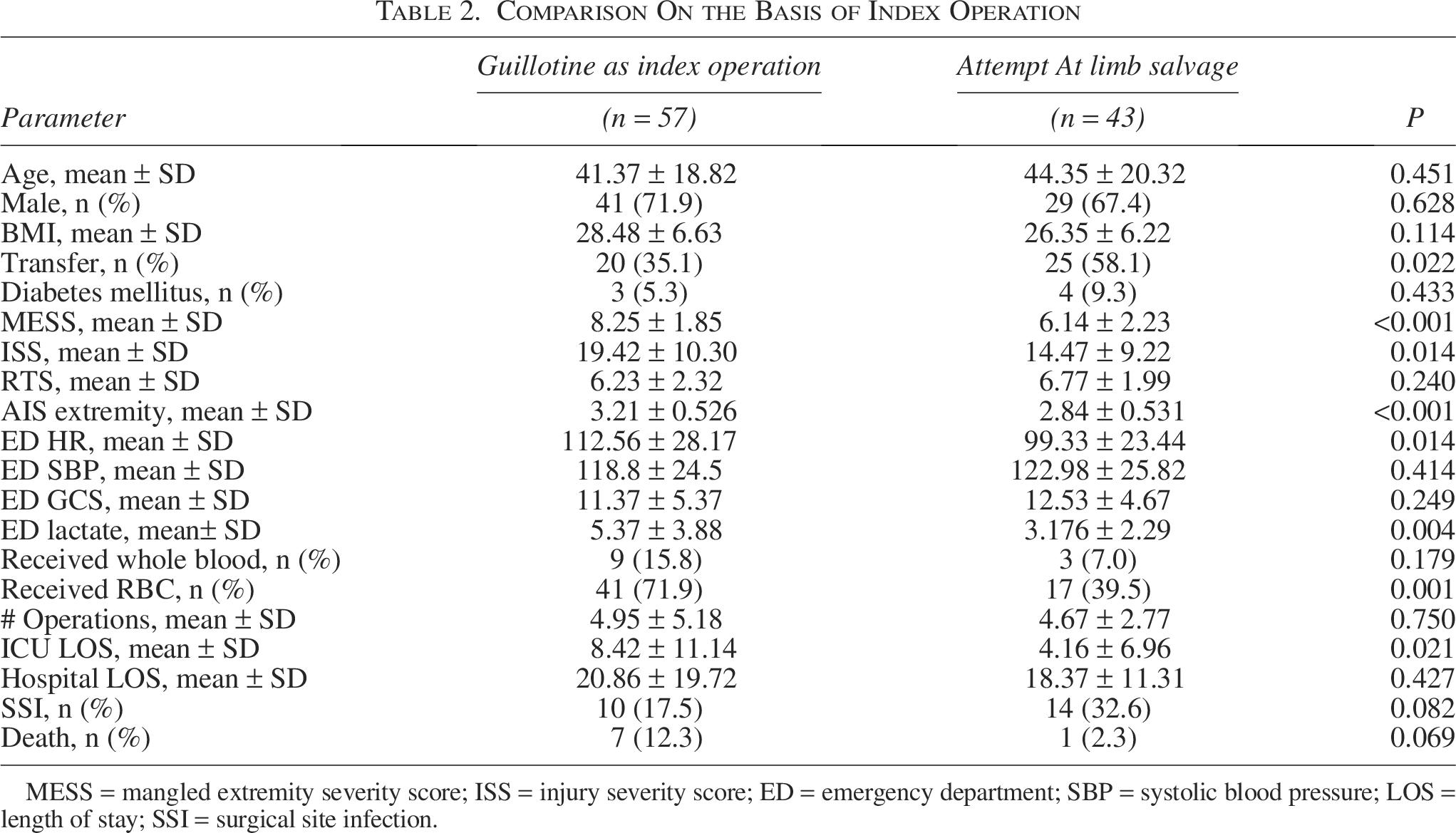
MESS = mangled extremity severity score; ISS = injury severity score; ED = emergency department; SBP = systolic blood pressure; LOS = length of stay; SSI = surgical site infection.
Patients who underwent guillotine amputation within six hours of arrival were younger on average (37.46 ± 16.37 vs. 45.97 ± 20.61, p = 0.016), but otherwise there were no significant differences in demographic characteristics. These patients had elevated MESS (8.62 ± 1.41 vs. 6.52 ± 2.35, p < 0.001) and ISS (20.00 ± 10.28 vs. 15.56 ± 9.78, p = 0.016) compared with patients who did not undergo guillotine amputation within six hours. These patients had a lower systolic blood pressure at admission (114.90 ± 23.99 vs. 124.26 ± 25.21, p = 0.034) and were more likely to receive a blood transfusion (71.8% vs. 49.2%, p = 0.025). There was no significant difference in number of operations (4.67 ± 4.86 vs. 4.93 ± 3.95, p = 0.383), ICU LOS (7.72 d ± 10.19 vs. 5.87 ± 9.48, p = 0.179), or hospital LOS (19.00 d ± 16.91 vs. 20.30 ± 16.45, p = 0.352) between those that underwent guillotine within six hours and those that did not. Patients undergoing guillotine amputation within six hours (n = 39) had a significantly lower rate of SSI compared with the patients (n = 61) who did not (12.8% vs. 31.1%, p = 0.036). Demographics, injury severity measures, and surgical management characteristics for these groups are shown in Table 3.
Comparison On the basis of Timing of Amputation
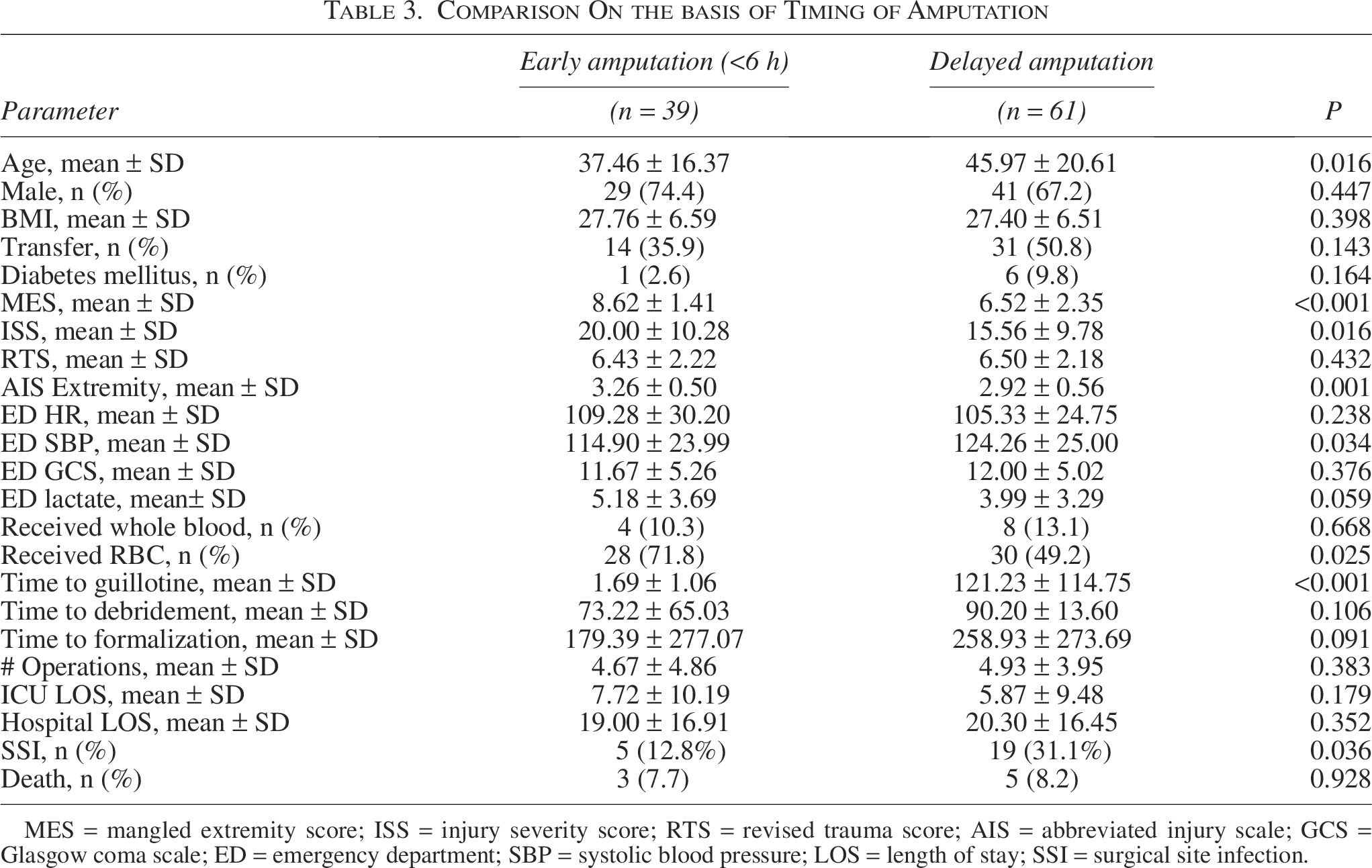
MES = mangled extremity score; ISS = injury severity score; RTS = revised trauma score; AIS = abbreviated injury scale; GCS = Glasgow coma scale; ED = emergency department; SBP = systolic blood pressure; LOS = length of stay; SSI = surgical site infection.
Discussion
This study represents one of the largest single-center experiences with mangled extremities ultimately requiring amputation. SSI will develop in nearly one quarter of these severely injured patients. We demonstrate the substantial impact of SSI in patients who undergo amputation for traumatic extremity wounds. These complications result in longer hospital LOS and more trips to the operating room, and ultimately, patients with SSI have a greater likelihood of requiring conversion to an amputation a joint above. We also demonstrate a significantly decreased rate of SSI in patients that underwent guillotine amputation within six hours of arrival to the hospital.
Previous studies regarding these injuries have demonstrated that delayed closure (>5 d from time of injury) is associated with decreased rate of SSI. 7 Delayed closure allows for more debridement and washouts of the wound before closure, which is important in these wounds which are often highly contaminated. Similarly, early guillotine allows for early debridement of devitalized tissue and washout of wound which should function to decrease wound complications. Management of these injuries also involves early initiation of antibiotic therapy, typically with narrow coverage for Gustilo grade I or II open fractures, and broader gram-negative coverage for grade III open fractures for a duration of 48 hours. 9 Notably, time to initiation of antibiotic therapy and total duration of antibiotic therapy were not associated with increased rate of SSI.
Guillotine amputations were more likely to be performed at our institution for those patients with more severe extremity injuries and those that are more physiologically unstable. The MESS and ISS were substantially greater for the group that underwent guillotine as the index operation, as were the heart rate and lactic acid recorded in the trauma bay. These patients were also more likely to receive a blood transfusion, again indicating more severe injury and physiologic derangement at initial presentation. These patients appropriately underwent a guillotine amputation and typically were transferred to the ICU for further resuscitation. Despite the patients having vital signs indicating more severe physiologic derangement and having more severely injured extremities, these patients had outcomes similar to or better than the group that did not undergo index guillotine. The up-front guillotine group had no difference in ICU LOS, hospital LOS, or mortality and had an improved SSI rate.
Traumatic amputations are only estimated to represent 16% of all amputations, but account for 45% of the total prevalence of limb loss. 1 This is because of the fact that traumatic amputations typically occur in patients that are younger compared with amputations for other reasons. 10 These patients will thus require high-quality prostheses over a longer period to maintain a normal functional status. Despite this, patients undergoing amputation following major lower extremity trauma have been shown to have improved functional status compared with those that underwent limb salvage. 11
This study has several limitations. Foremost, it is a single-center retrospective study. Decisions to amputate or attempt limb salvage were left entirely to the discretion of the operating surgeon, which leads to heterogeneity in management. Another limitation is that patients that successfully underwent limb salvage without eventual amputation were not included in the analysis. Comparison with this group may, in future studies, help define predictors of limb salvage failure. The justification for not performing a guillotine at index was also not well defined in the original data collection. Some initial debridement operations may be performed to control hemorrhage before a family discussion about possible limb loss. Thus, we cannot say with certainty that all those patients that did not undergo index guillotine were those in which a limb salvage was attempted.
Ultimately, the decision to amputate or attempt limb salvage is made at the discretion of the operating surgeon on the basis of the condition of the limb in question. Some of the factors that may influence this decision include the amount of soft tissue loss, nerve injury, prolonged warm ischemia time (>6 h), and degree of vascular segment loss. 8 When the likelihood of successful salvage is low, proceeding with amputation may lead to better functional outcomes than prolonged attempts at salvage in these injuries. 12 If amputation is to be performed, prompt decision-making may decrease infectious complications, as guillotine within six hours was associated with decreased rate of SSI.
Conclusion
This study findings show that early guillotine amputation in patients likely to undergo amputation was associated with a decrease in the rate of SSI. Understanding the impact of surgical timing and operative techniques to prevent SSI for these traumatic amputations will inform trauma surgeons about the best course of action.
Authors’ Contributions
S.E.G.: Conceptualization, methodology, formal analysis, writing—original draft, review and editing, and project administration; S.O.: Writing—review and editing; J.P.B.: Investigation, methodology, and writing—original draft; S.L.W.: Methodology, investigation, and writing—original draft; R.G.: Investigation; D.N.T.: Methodology, writing—original draft, and review and editing; S.A.C.: Writing—review and editing; N.M.G.: Methodology, writing—original draft, and review and editing; M.A.N.: Conceptualization, methodology, and writing—review and editing; W.I.: Methodology, formal analysis, writing—original draft, and review and editing; and E.A.T.: Conceptualization, methodology, writing—review and editing, and supervision.
Footnotes
Acknowledgment
The authors would like to thank the clinical and administrative staff who contributed to data collection and patient care.
Author Disclosure Statement
The authors declare no conflicts of interest relevant to this study. The authors have no conflicts of interest to disclose.
Funding Information
This research received no specific grant from any funding source.