
Abstract
Purpose:
To highlight the burden of surgical site complications (SSCs) across inpatients who have recently undergone orthopedic surgery by undertaking surgical site infection (SSI) prevalence days.
Patients and Methods:
Sites from the United Kingdom and Ireland enrolled in a single day’s data collection (either March or September 2022) to capture inpatient prevalence of SSIs and other SSCs. Data were collected from patients recovering from primary and revision hip or knee surgery and neck of femur (NOF) fracture surgery.
Results:
Data were collected on 851 inpatients across the two days, with NOF fracture surgery representing 50% of overall procedures, followed by primary hip (25.4%) and primary knee (12.8%) procedures, with 11.9% of patients in the hospital following revision procedures. The majority of patients documented across both days had at least one risk factor (76% overall). The overall prevalence of SSCs was 8% (n = 68). Revision surgical procedures had significantly higher complication rates than primary surgical procedures in both hips and knees (p < 0.01). The highest observed odds ratios (ORs) for SSCs were in patients who listed immunosuppression (OR = 2.47), previous SSI (OR = 4.59), and smoking (OR = 2.34) among their risk factors. Higher overall lengths of stay were observed in patients with complications.
Conclusion:
These prevalence days were a successful initiative to help hospital sites understand their own burden, benchmark against national averages, and contribute to a better national understanding of the burden of SSC, both to healthcare systems and, most importantly, patients.
Keywords
Introduction
Surgical site infection (SSI) is an important complication of surgery that can have a significant impact on patient mortality and morbidity.1,2 Orthopedic surgery encompasses high-risk procedures that carry an increased incidence of SSI and other surgical site complications (SSCs).1,3,4
Although the incidence of SSCs varies depending on the type of procedure and the patient population, it can demonstrate a complication rate of up to 10%. 5 Factors, such as variations in adherence to infection control practice, inadequate resources, patient comorbidities, and smoking, have been documented to contribute to the burden of SSCs. 6
The consequences of developing an SSC are often far-reaching, affecting not only patient factors such as length of stay and quality of life 3 but also causing a detrimental impact on the healthcare system, specifically the economic burden caused by factors such as the need for further intervention or reoperation. 7 The projected economic burden of prosthetic joint infection for hip and knee in the United States (US) is estimated to be within the region of 1.85 billion US dollars by 2030. 8 This can cause compounded negative outcomes on metrics such as elective waiting lists, bed capacity, and antimicrobial stewardship.3,9–12 Studies have shown that the cost of treating SSCs can be several times higher compared with the cost of the original surgical procedure. 13
SSC surveillance is the systematic collection, analysis, and interpretation of data on the rate of SSCs to help identify rates of occurrence and understand additional patient and procedural risk factors with an aim to raise awareness and identify opportunities to prevent their incidence.9,14,15 The surveillance of SSCs across all surgical specialties is vital in assessing the effectiveness of SSC prevention interventions and to facilitate the improvement in patient outcomes,16,17 with orthopedics being one of the most progressive areas for surveillance tools and strategies.16,18 The initiatives available include the National Nosocomial Infections Surveillance system, the Surgical Site Infection Surveillance system, and the Global Surgical Site Infection Prevention program.1,5,19 Patient registries can also be utilized to track the incidence and risk factors of SSCs.16,20,21
Even with these initiatives, however, the difference between reported and actual rates of SSCs is understood to have a high degree of variance. This may consequently lead to a detrimental effect on patient outcomes, healthcare workers’ morale, and infection control efforts.8,22,23 A number of factors may be involved in the inconsistency between reported and actual rates of SSCs.8,24 The key factors contributing to this variance include inconsistencies in SSC definitions and surveillance methods, variability in detection and documentation, reporting culture irregularities, lack of complete patient follow-up processes, and data collection bias.25,26
Despite the practice of SSC surveillance being a recognized method in improving clinical outcomes and reducing complication rates, the resources available to clinicians to aid with data collection vary considerably between hospitals. 27 The slow uptake of Electronic Patient Record systems and other indicators of digital maturity across the United Kingdom’s (UK) National Health Service (NHS) also provides challenges in the accuracy and ease of data collection despite their inclusion in the NHS long-term plan. 24
Choosing the correct mode of surveillance of SSC is paramount in ensuring data collected is both useful and applicable to clinical practice. The prevalence of an SSC can be defined as the number of SSCs within a population at a given period of time.
This article aims to highlight the burden of SSCs across populations of patients who have recently undergone orthopedic procedures utilizing the point prevalence methodology.
Materials and Methods
Sites from the UK and Ireland were invited to enroll in a single day’s data collection to capture inpatient prevalence of SSIs and SSCs. Participation of all sites was entirely voluntary and initiated through the completion of a registration form. This day was officially titled the “SSI prevalence day.”
Data on the day itself were collected using a custom-built form, delivered using the Snap Survey XMP platform (Bristol, UK). The Snap platform was chosen because of its comprehensive data collection capabilities and security credentials.
Although no patient-sensitive data were collected, data protection was a key consideration of the platform’s selection as these data measured key healthcare outcomes of participating sites that would not naturally be observed in the public domain. As no interventions were made and no patient-sensitive data collected, ethics approval was not required, although sites were encouraged to seek local approval where considered necessary.
Data were collected across all patients currently in each unit recovering from primary and revision hip or knee surgery and neck of femur (NOF) fracture surgery.
Variables collected as part of the prevalence day initiative comprised the procedure type, patient gender, body mass index (BMI) and comorbidities, complication presence and type, readmission details, and the patients’ current length of stay in the hospital.
The prevalence day was conducted twice in 2022, once in the spring (March 9) and once in the autumn (September 7). There is some evidence to suggest seasonal variation in the rates of SSI by time of year, with higher rates being recorded in those months with higher recorded average temperatures, 13 which is why two prevalence points were chosen.
Once data were collected, each registered site received a report of their individual burden of SSC, facilitating greater awareness of their hospital’s inpatient prevalence of complications and their impact. Each site also had access to an anonymized national aggregate to enable them to make comparisons to a national average and understand their relative performance and the true societal and system burden of SSC. The data provided in these national aggregates were subsequently analyzed for this article.
Data were analyzed using SAS 9.4 (Marlow, UK). Frequency counts were conducted for descriptive statistics to summarize the data collected. Statistical testing, such as Fisher exact tests, was performed to explore relationships and associations between different variables and their impact on complication prevalence. Odds ratios (OR) were calculated to understand if complications, when they occurred, were predictable based on the characteristics of the patient.
Results
Demographics
On the first prevalence day in March 2022, 284 patients’ data were recorded. An increase in participating sites led to this growing to 567 on the day in September 2022, providing a total patient sample of 851 patients (although 15 had no procedure reported). On both days, the largest proportion of patients documented were NOF fracture repairs. Primary hip and primary knee surgical procedures represented 25.4% and 12.8% of the overall sample, respectively; 11.9% of patients were in the hospital following revision procedures (Fig. 1).
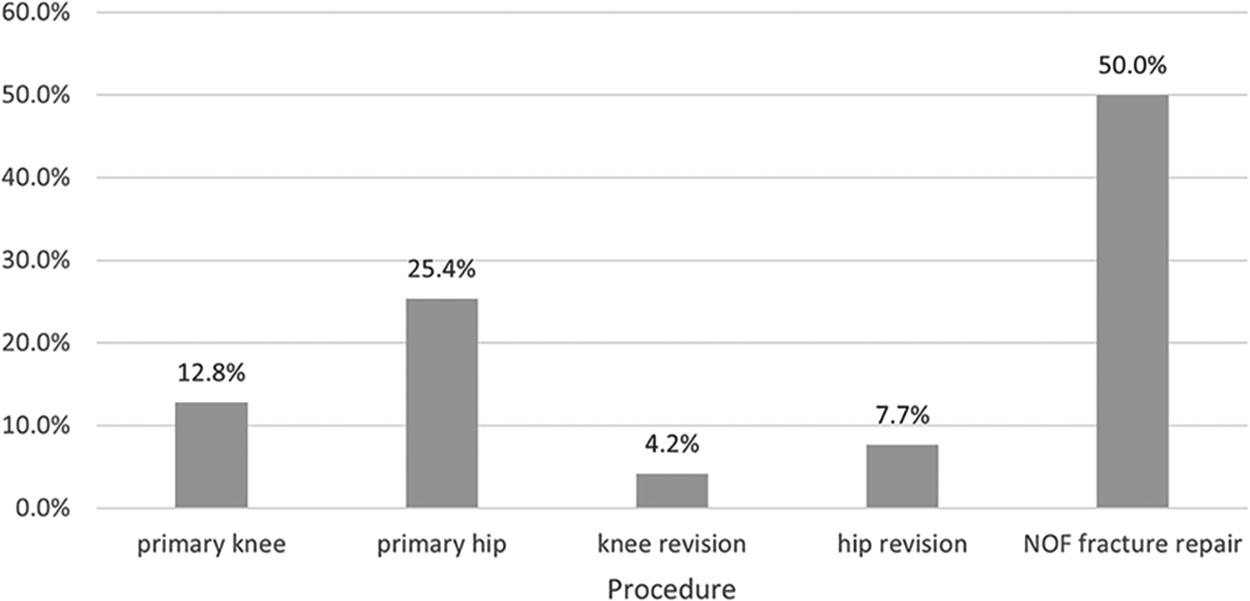
Overall proportion of patients undergoing each surgical procedure. NOF, neck of femur.
On both days, a larger proportion of patients were female (65.2% and 62.7%, respectively, 63.5% overall); BMI proportions were consistent between the two days, with one in five patients having a BMI more than 30 (20.2% overall). The most frequently observed risk indicator for SSC was an American Society of Anesthesiologists (ASA) score greater than or equal to 3 (56%), 22% of patients had poor renal function, and 19% of patients were classified as diabetic.
The majority of patients documented across both days had at least one risk factor (76% overall); mean numbers of risk factors per patient were consistent across both days (1.43 d one, 1.54 d two, 1.51 overall) (Table 1).
Demographics of Inpatients Having Orthopedic Surgery Across Both Prevalence Days
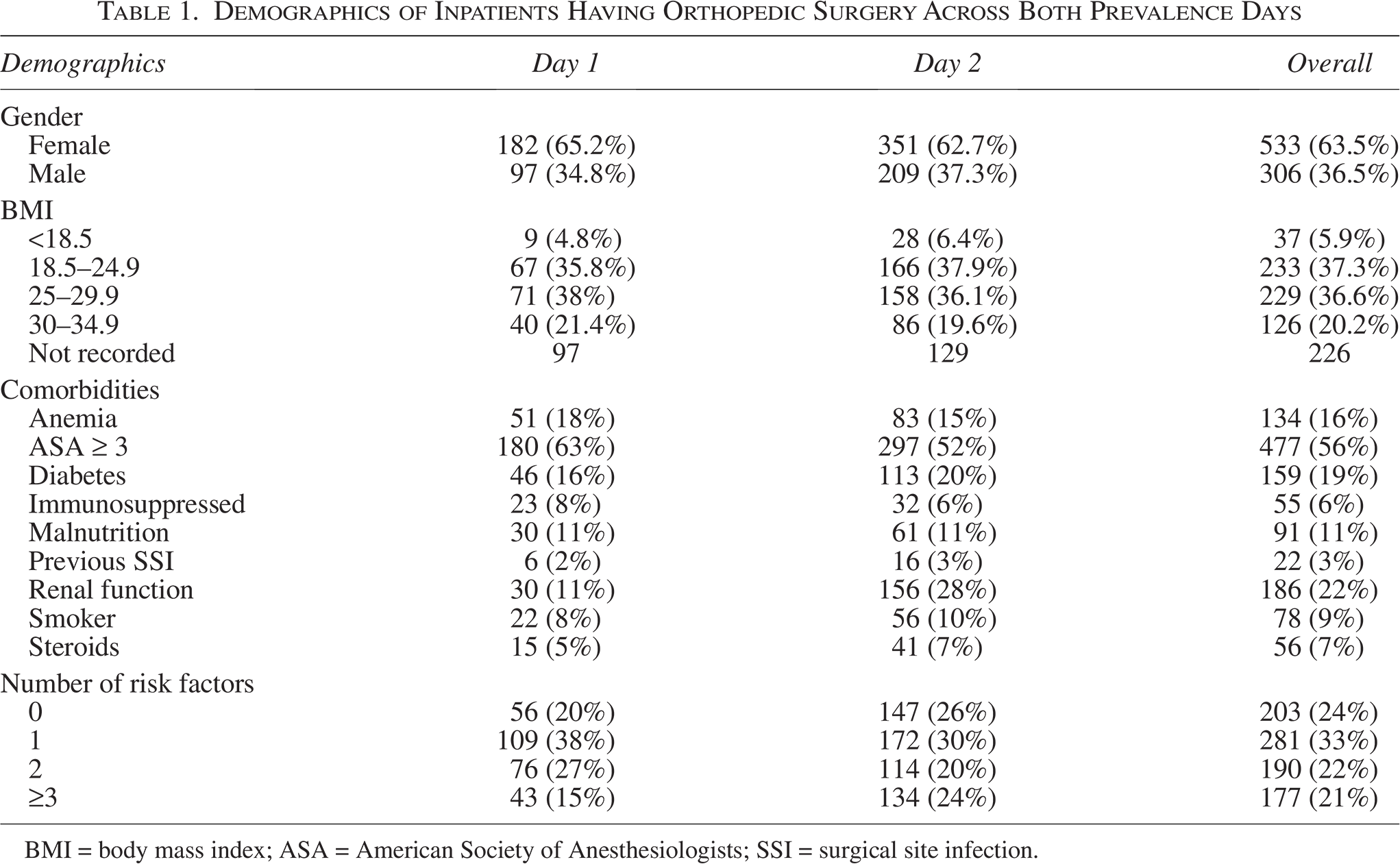
BMI = body mass index; ASA = American Society of Anesthesiologists; SSI = surgical site infection.
Complications
The key outcome of the SSI prevalence day was understanding the overall prevalence of SSCs across hospital inpatients following orthopedic surgery; this was found to be 8.0% (n = 851) (Table 2). There was a slight difference in reported rate between the two dates; complications were higher in the spring date (9.9%) than in the autumn date (7.1%).
Complication Rate by Orthopedic Surgery Performed
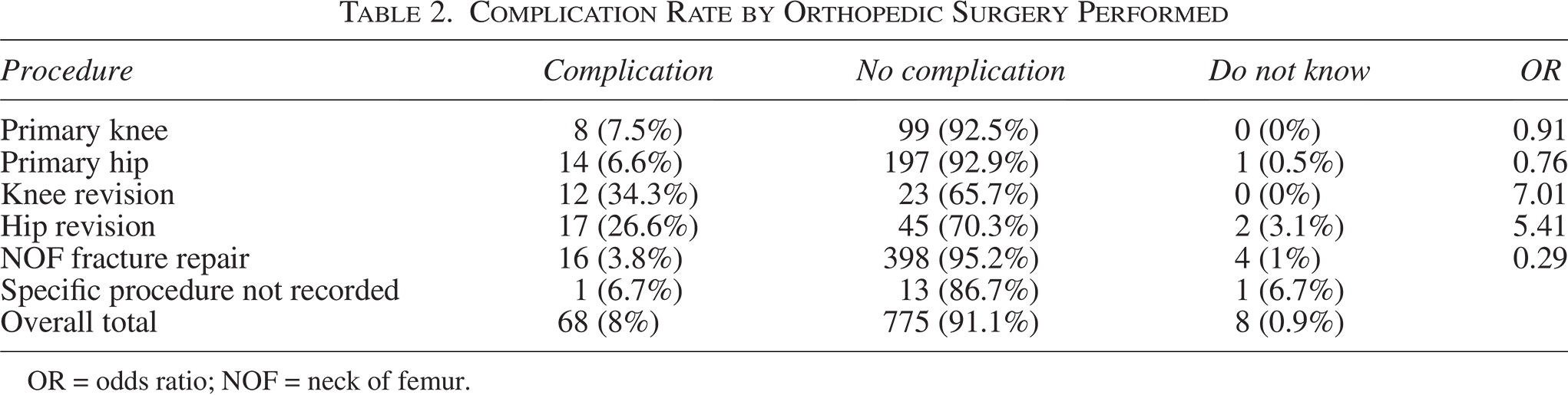
OR = odds ratio; NOF = neck of femur.
Revision surgical procedures were found to have a significantly higher prevalence of complication than their primary equivalents (OR = 7.01 knee, 5.41 hip); knee surgical procedures saw the rate increase from 7.5% to 34.3% once the surgery was revisional (p < 0.01, Fisher exact test), and hip surgery saw a similar increase of 6.6% to 26.6% (p < 0.01, Fisher exact test) (Table 2).
The majority of observed complications (n = 77) were deep SSIs (71.4%); 15.6% of surgical sites had dehisced; four of these dehisced wounds were considered to be suffering from a concurrent deep SSI.
In our analysis, males were more likely to suffer from complications than females, though this finding was not significant (p = 0.09, Fisher exact test). Similarly, a higher observed prevalence of complications was observed in patients with a BMI greater than 30 (p = 0.16, Fisher exact test).
Highest observed ORs for SSCs were observed in patients who listed immunosuppression (OR = 2.47, p = 0.03, Fisher exact test), previous SSI (OR = 4.59, p < 0.01, Fisher exact test), and smoking (OR = 2.34, p = 0.02, Fisher exact test) among their risk factors. Malnourished patients seemingly had an overall lower risk of complications (5.5%).
The presence of additional risk factors increased the likelihood of the patient having an SSC; once a patient had more than three identified risk factors, the likelihood of complication increased to 11.3% (OR = 1.65, p = 0.09) (Table 3).
Demographics of Inpatient Complication Rates Following Orthopedic Surgery
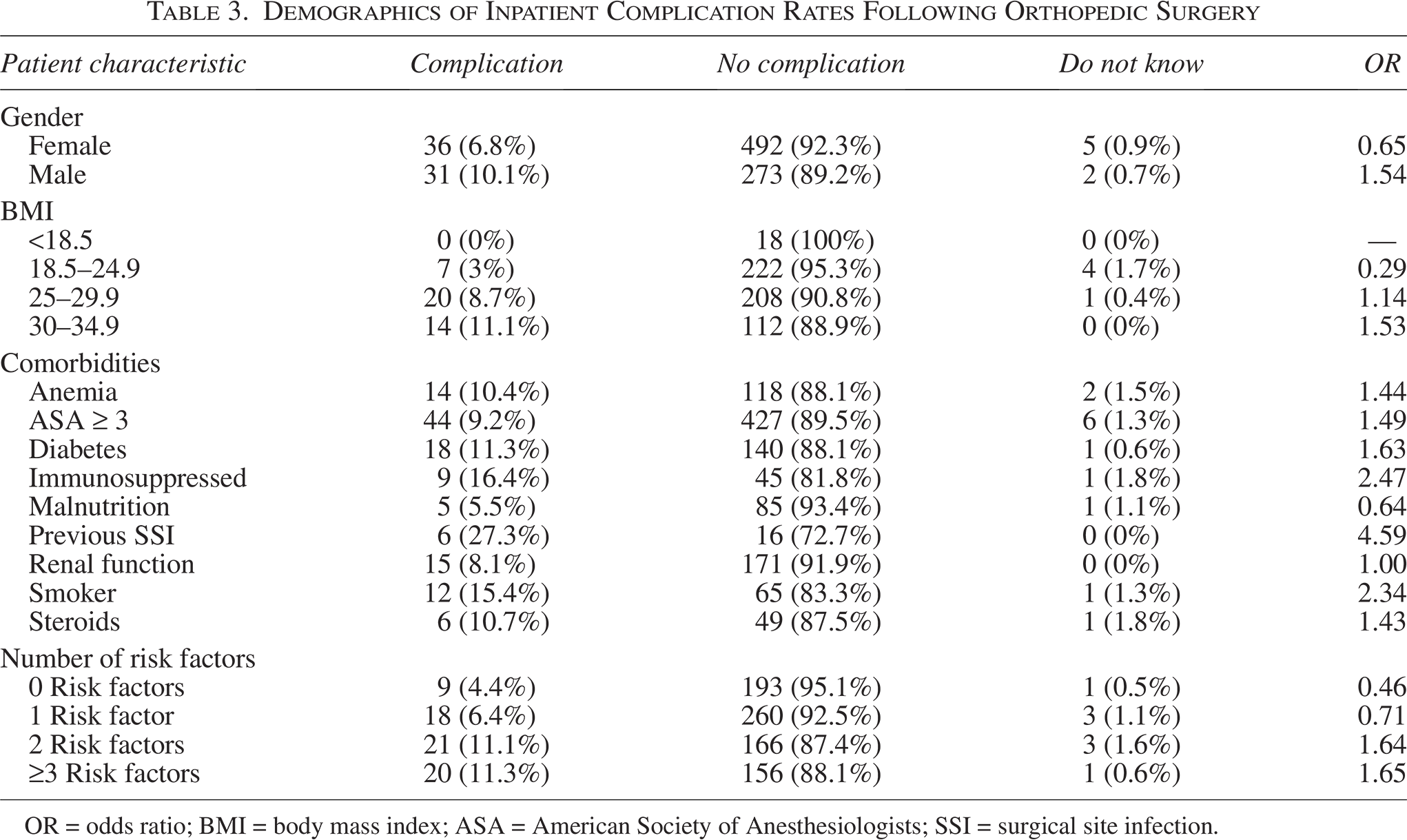
OR = odds ratio; BMI = body mass index; ASA = American Society of Anesthesiologists; SSI = surgical site infection.
Consequences of complications
Higher overall lengths of stay, inclusive of primary and any readmission episodes, were observed in patients with complications when compared with those patients who had no complications. Significantly, 65.7% (n = 67) of patients with complications had a current inpatient stay of more than 30 days, compared with just 14.6% of patients without a complication (p < 0.01, Fisher exact test) (Fig. 2). Seventy-five percent of patients with complications (n = 51) were in hospital following a readmission, and 25% (n = 17) were not.
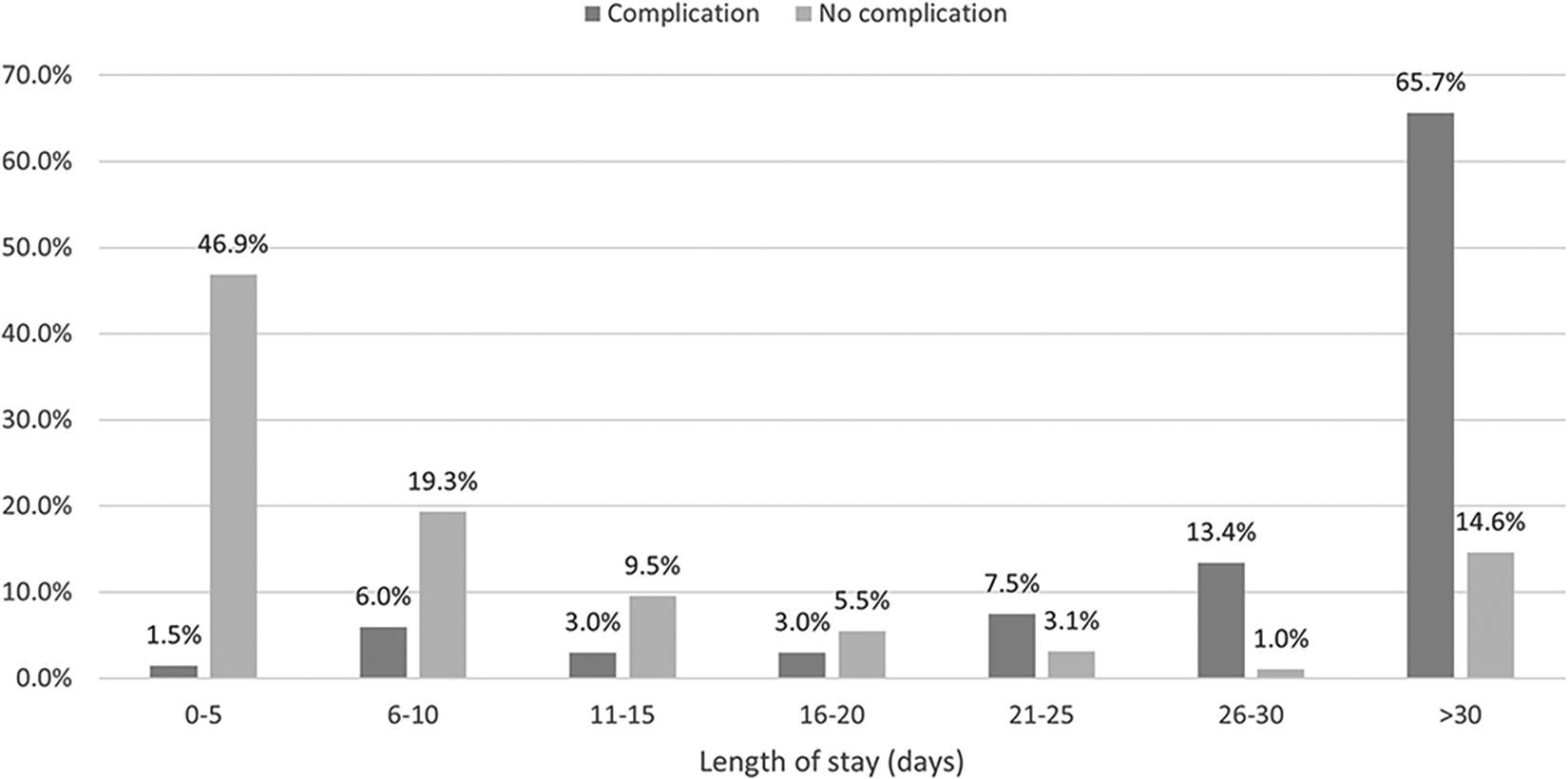
Length of inpatient stay (days) with and without complications following orthopedic surgery.
Discussion
The burden of SSCs in the UK is a significant concern for patients, healthcare providers, and the healthcare system as a whole. SSCs contribute to increased morbidity, prolonged hospital stays, and additional healthcare costs.8,13,25
The outcomes of the two SSC prevalence days in the UK and Ireland in 2022 reinforce many of these messages; overall, 8% of patients surveyed were indicated as having had a complication.
Although the two prevalence days here did not comprise costings, they do demonstrate significant burdens of extended length of stay and patient readmission. Both factors significantly increase the financial burdens on the health system but also present potential problems with patient throughput and ward capacity.
Recognizing the impact of SSCs, the NHS and other healthcare organizations in the UK have implemented various preventive measures. 28 The National Institute for Health and Care Excellence (NICE) publishes evidence-based guidelines to promote best practices in infection prevention and control. These include appropriate patient and staff theater wear, antibiotic prophylaxis, and the use of gloves, drapes, and antiseptic preparations. 2
NICE also recommends intervention of medical technologies, such as the consideration of PICOTM (Smith and Nephew, UK) single-use negative pressure wound therapy (sNPWT) as an appropriate technology, because of its association with fewer SSCs in patients who are considered to be at risk. 29
In the context of prophylactic use on closed surgical incisions, sNPWT systems utilize a sealed and airtight dressing that connects to a pump, which applies sub-atmospheric pressure to the incision. 30 Mechanisms, by which healing is accelerated and the subsequent rate of complications is reduced, consist of removal of wound exudate, stimulation of neovascularization, and the reduction of interstitial edema. 31 Evidence for the prophylactic use of incisional NPWT compared with standard dressings for the prevention of SSI in adults undergoing any surgical procedure is compelling. 32
Many of these recommendations are made for high-risk patients only; these recommendations are generally made because of the increased cost of some interventions as a way to ensure hospitals achieve cost-effectiveness when implementing initiatives.
The findings of the SSC prevalence days further demonstrate the predictability of complications and support the feasibility of risk-based mitigation strategies. These data reinforce that using factors such as BMI and various comorbidities can help ascertain the post-operative risk of a patient developing a complication; the presence of some risk factors increased the likelihood of complication by up to an OR of 3.37. The finding that malnourishment lowers overall risk is intriguing and may stimulate further need for investigation.
Although these prevalence data demonstrate the importance of risk factors and their assessment, patient demographics, and the consequences of complications, they also further highlight the need for overall visibility of the issue. Challenges persist with national surgical site surveillance16,22 (leading to a lack of reporting and significant inconsistencies in observed complication rates). Overall, the difference between reported and actual rates of SSCs highlights the need for standardized surveillance methods, consistent definitions, and improved data collection practices. 28 Efforts to enhance reporting culture, promote accurate documentation, and implement comprehensive follow-up systems can help bridge the gap between reported and actual rates, providing a more accurate understanding of the burden of SSCs and enabling targeted infection prevention strategies.8,13,26
The success of this prevalence day initiative can be extended to provide a rolling national opportunity to better understand the burdens of complications and to monitor any future positive or negative trends in their occurrence. Notably, these data also only consider orthopedic inpatients; there remain significant possibilities to extend this initiative to consider patients suffering complications in the community and to better understand the burden and impact of risk on patients across other surgical specialties and within other countries and healthcare systems.
Limitations
The nature of this multi-site prevalence study inevitably leads to differences in data accuracy because of potential varying diligence in the accuracy of reported variables. Furthermore, the authors had no control over the availability of data around comorbidities or patient characteristics, nor the accuracy of any diagnosis of complications. No formal guidance was provided to the sites on formalized diagnostic criteria of SSCs. All these factors were considered in the design of the initial data capture form; comorbidities, patient BMI, and complications were all categorized in such a way to give reporting individuals the best opportunity to accurately reflect each individual patient.
Although not a limitation in the study itself, it is important to reinforce that this article does not suggest the incidence of inpatient SSCs is 8%. As indicated, the complication prevalence is calculated to be this high, yet it is important to recognize that this rate will inflate the incidence because patients suffering complications are likely to have extended their length of stay or experienced readmission. This finding is of significance because of the impact these 8% of patients have on factors such as patient throughput and workforce planning.
Other methodologies for calculating the rate of complications exist, such as an incidence-based study or the calculation of prevalence across an overall local or national population.
Again, both methods were dismissed to ensure simplicity and reduce the burden. These data highlight and reinforce the burden of complications, but their use in any population-based modeling should be handled appropriately.
Conclusions
The burden of SSCs in orthopedic inpatients in the UK and Ireland is high. Considering the challenges surgical site surveillance initiatives present, many positives were found in the initiative of prevalence days as a way to help hospital sites understand their own burden, benchmark against national averages, and contribute to a better national understanding of the burden of SSCs both to healthcare systems and, most importantly, patients.
Authors’ Contributions
All authors contributed to the study conception and design, material preparation, data collection, and analysis. The article was written by D.B. and T.S., and all authors commented on previous versions of the article. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors would like to extend their thanks to all the sites that took part in these prevalence days. In addition, they would like to thank Jennifer Gale for setting up data collection and Amy Glasswell for support with article preparation.
Author Disclosure Statement
R.M.J. is on the advisory board and receives consulting fees from Smith and Nephew, Zimmer Biomet, and Tecres, and receives consulting fees from Molnlycke and Biocomposites. R.M.J. is president of the Bone and Joint Infection Society and a Trustee of the British Orthopaedic Association. D.B. and T.S. are employees and shareholders of Smith and Nephew.
Funding Information
No funding was obtained for this study.