
Abstract
Healthcare in the United States has reached a point where it is unsustainable for the long term, particularly for the poor, the elderly, and healthcare workers (HCWs) themselves. We propose a framework for making U.S. healthcare more sustainable, whereby the service returns to its core mission of healing. The framework casts that healing mission in broadly applicable, practical terms, whereby leaders of healthcare organizations and in the wider for-profit, not-for-profit, and governmental healthcare ecosystem take concrete steps to improve outcomes for patients and HCWs. Those steps involve aligning healthcare resources, incentives, and policies with the core mission of healing and then implementing change in specific ways that particular organizations have already shown are achievable and sustainable. We use those examples to illustrate how healing-oriented innovations in healthcare delivery get deployed and how progress toward sustainability then ensues. Lessons from these efforts can be tailored to individual healthcare contexts and institutions—and then applied on a national scale. The discussed initiatives can also guide the direction of future research on healthcare sustainability.
The U.S. healthcare system is ailing. Its purpose is to heal, but too often it harms patients with misdiagnosis, medication errors, over and undertreatment, medical debt, failing to address the social drivers of health, and other ills. It is a service we all need, but some population segments are served far better than others. An inherently stressful service to perform—physically, emotionally, mentally—it is plagued by severe, worsening staff shortages. It costs far more, per capita, than in any other country, with at least 25% of total spending estimated to be wasteful (Shrank, Rogstad, and Parekh 2019). It is often managed like a business and, increasingly, is controlled by for-profit companies. But caring for patients is not merely a business; it is a unique, sacred calling. Patients’ quality of life, and life itself, are at stake.
Many nations’ health systems are distressed, to be sure. We focus on the U.S. because its system differs from that of other industrialized nations in important ways, such as its very high administrative costs, its emphasis on specialty versus primary care, and its payment and reimbursement complexities. As it now exists, U.S. healthcare is unsustainable for the long term.
The Global Quest for Sustainability in Healthcare
The United Nations in its 2030 Agenda for Sustainable Development has identified as a top sustainable development goal (SDG) “good health and well-being” (United Nations 2015). Although just one of the UN’s 17 SDG goals, health and well-being is unique because it often strongly intersects with other SDGs such as poverty, hunger, education, and inequality (Aftab et al. 2020). In short, global health issues have strong spillover effects. After all, SDGs such as health focus on what long ago was described as “wicked problems” (Rittel and Weber 1973), whose multiple, interdependent causes complicate efforts to find and implement sustainable solutions.
Not surprisingly, then, progress on healthcare sustainability is frustratingly slow, related to a lack of alignment with desired sustainability outcomes. When alignment is present, it leads to balance, stability, and continuity; when it is absent and unaddressed, imbalances get amplified, creating a vicious cycle that makes solutions even more elusive. The emerging evidence suggests that three alignment types are central to achieving SDGs: (1) alignment of resources; (2) alignment of incentives; and (3) alignment of policies—each shaping the others (United Nations 2022). We now briefly describe each type, later showing precisely how they apply to healthcare.
Resources Alignment
Resources can be multifaceted—financial, technological, and human—although financial resources often shape the other two. Creating alignment requires, at minimum, that the available resources match the task at hand. The literature gives much attention to challenges stemming from a lack of financial resources. To appreciate the magnitude, consider the sobering statistics from the United Nations Commission on Trade and Development. UNCTAD estimates, globally, a need for $5 to $7 trillion per year to address all SDGs (Constanza et al., 2020). Recent trends suggest governments will provide only about 15% of those funds. Without additional, reliable funding sources, efforts to address SDGs are likely to remain seriously under-resourced.
Incentives Alignment
Incentives are, broadly, the motivational underpinnings of various stakeholders. In complex systems related to SDGs, stakeholders represent entities along the entire value chain (Koskela-Huotari et al. 2023). Incentives are aligned when stakeholders, using their own rational analysis, are sufficiently motivated to engage in activities that help to achieve SDGs. Evidence points to a lack of alignment on multiple fronts (Agarwal et al., 2020)—firms, consumers, and institutions. The status quo, unfortunately, encourages behaviors that run counter to SDGs. For instance, companies that profit from marketing products that harm the environment have incentives to continue doing so as long as possible. Consumers often resist changing accustomed buying patterns even when detrimental to themselves or others. Institutions, too, may find it difficult to make meaningful changes in the short run.
Policy Alignment
We use “policies” broadly to refer to the prevailing institutional (i.e., legal and regulatory) context and operating procedures that firms employ to structure their various activities. SDGs fundamentally are country-level outcomes, making it critical to deeply understand the policy infrastructure at that level. The regulatory context not only provides rules for proper governance, but also signals support for specific types of stakeholder behavior. For instance, taxation and subsidies can spur firms and consumers to continue or discontinue certain activities in the marketplace. Emerging literature indicates that the policies often remain misaligned with SDGs (United Nations 2022). This misalignment occurs primarily because SDGs require new policies, but the political process does not produce such policies in a timely manner. In addition, firm-level policy changes may be stymied by resource constraints, insufficient incentives, or both.
This article proposes how the U.S. healthcare system can deliver better outcomes more sustainably by aligning resources, incentives, and policies. We show how U.S. healthcare is straying from its core mission of healing, contributing to misaligned service to its diverse stakeholders. We focus on three stakeholder groups—the poor, the elderly, and the healers themselves—given their importance and the egregious misalignment in meeting their needs. For each group, we discuss the current state of underperformance and promising innovations for improvement. Figure 1 presents our framework for sustaining a more effective, equitable health system. The framework, though far from comprehensive, highlights especially salient opportunities for realignment. We offer a future research agenda in the Discussion section. A framework for sustainable healthcare through healing.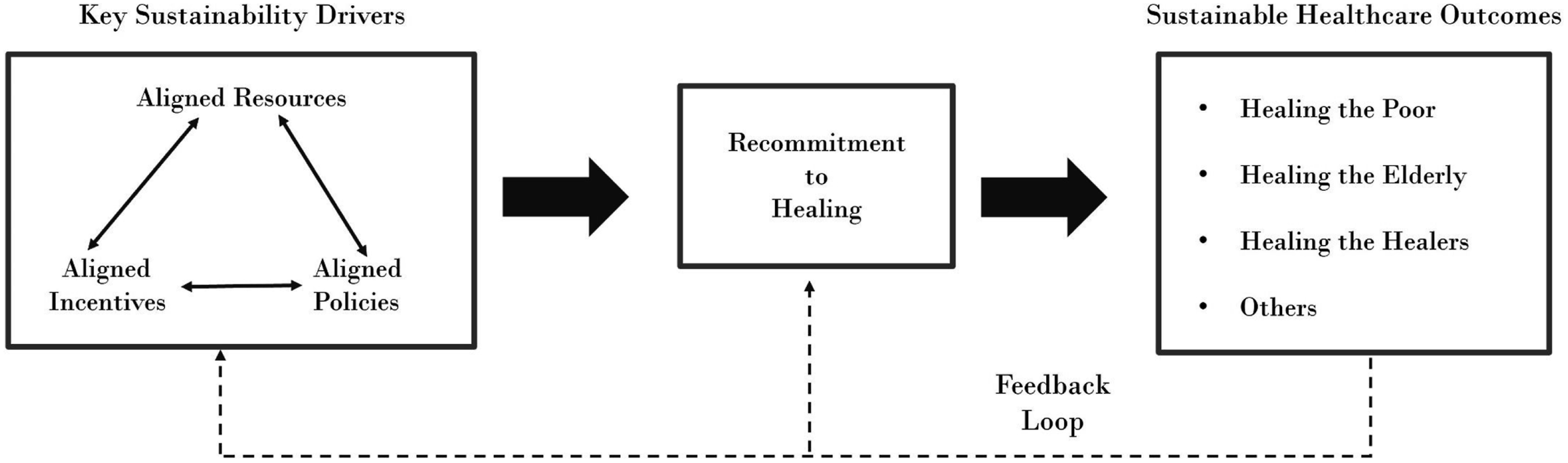
Re-Commit to the Mission of Healing
Healthcare’s primary aim is to heal in its broadest sense—physically, mentally, emotionally. Clinicians can heal even when they cannot cure by, for example, reassuring and calming a frightened patient; controlling pain and slowing progression of disease; and helping a patient decide whether to stop debilitating, costly treatment that is unlikely to be effective and start noncurative “comfort care.” Healing furthers a person’s well-being, which extends beyond medications, procedures, and hospitalizations. People need healing at different times in their lives, and when clinicians and their institutions offer it, they renew themselves, too (Awdish and Berry 2019).
Regrettably, healthcare’s healing mission is being trampled by a confluence of pressures, including burdensome documentation requirements (Rosenbaum 2022); a proliferation of for-profit companies that own and control healthcare delivery and prioritize short-term financial performance (Zhu and Polsky 2021); severe staffing shortages and clinician burnout (Auerbach et al. 2022); and general upheaval related to the COVID-19 pandemic (Prasad et al. 2021). Healing, healthcare’s “reason for being,” is in a state of imbalance. Although some health institutions hold firm to the healing mission, trends are in the wrong direction. Re-commitment to healing will require inspired leadership at every level (from individual clinicians to the federal government), starting with strengthening the primary antecedent of healing, which is trust.
How Trust Advances Healing
Trust, “... a willingness to rely on an exchange partner with whom one has confidence” (Moorman et al., 1993), opens the path to healing. No service depends more on trust than healthcare, given its emotional intensity, personal importance, variability, complexity, and intimacy. Whereas healthcare often is transactional and nonrelational (such as a one-time treatment at an urgent care center), much of it is relational, involving multiple encounters with the same clinicians or clinical team. Trust, the bedrock of strong relationships (Morgan and Hunt 1994), is paramount during serious illness because of the frequency and intensity of patients’ interactions with clinicians, informational complexity, the potential for high-stakes decisions, and the vulnerability and dependency that accompany serious illness (Berry et al. 2022). Without trust, will patients accept the opportunity to heal, especially if healing involves a doctor recommending halting futile treatment for incurable disease? Or, conversely, without trust and a sense of psychological safety, will patients be willing to say that they wish to stop “curative” treatment, that they do not want a third try at chemotherapy, that they wish to leave the hospital and go home (Berry et al. 2017)?
Competence-Influenced Trust
The most well-understood antecedent of trust in healthcare is competence. Patients’ perceptions of clinical competence can be influenced by whether a doctor seems rushed or deliberative, uncertain or assured, thorough or cursory (Bendapudi et al. 2006); by a doctor’s willingness to coordinate care with other clinicians (Lewis, Murry, and DeWalt 2023); and by the efficiency and professionalism of the service system, including encounters with nonclinical staff that “spill over” to influence assessment of the doctor (Dagger et al. 2013). Patients are likely to assume a physician is competent unless evidence to the contrary emerges (Bendapudi et al. 2006). Yet, trust is strengthened when perceived competence combines with perceived kindness. Given that patients and clinicians typically have such different levels of knowledge, patients have a tougher time judging technical competence than interpersonal behavior. Moreover, the circumstances of illness make patients especially sensitive and alert to the behavior they can see and understand, to infer what they cannot see and understand (Bendapudi et al. 2006).
Kindness-Influenced Trust
Kindness can offer a powerful emotional antidote to the uncertainty, worry, and fear that can accompany illness. Dean and Doty (2014) define kindness as “... purposeful, voluntary action undertaken with sensitivity to the needs or desires of another person and actively directed toward fostering their well-being or flourishing.”
Kindness in healthcare delivery has multiple dimensions. Extensive research with cancer patients (Berry et al. 2017) reveals the salience of six kindness dimensions that also apply to other illnesses: • Deep listening involves intently listening to patients (and family members), with infrequent interruption, to elicit their concerns and feelings. Active listening reduces the likelihood of unwanted or inappropriate treatment, demonstrates respect, and builds trust. • Empathy is viewing the situation from someone else’s perspective, avoiding judgment, recognizing the other person’s emotion, and responding to the emotion with caring (Wiseman 1996). • Generous acts go beyond standard, expected care by doing something extra and special to meaningfully help the patient. True generosity is voluntary. • Timely care involves focused effort to reduce needless delay for patients as they wait for appointments, vital information, and treatment. Although some delays are inevitable, more-timely care is often possible when service systems are redesigned, and their priorities recalibrated. • Gentle honesty is telling patients the truth about their condition in sensitive, well-chosen words that convey partnership and guide patients to decisions that are right for them (Sisk 2015). • Support for family members (or close friends) who care for ill loved ones at home is necessary and practical. These caregivers are often not prepared to perform the roles that are required (Aldridge and Bradley 2017).
In healthcare, trust is an antecedent to healing. Adding kindness-influenced trust to competence-influenced trust compounds their healing effects (Ballat & Campling, 2011; Barry & Edgman-Levitan, 2012; Berry et al., 2021).
How Clinicians Offer Healing
Healing takes four primary forms in addition to improving patients’ physical well-being:
Mitigating Fear
Clinicians heal when they defuse patients’ fears without resorting to telling falsehoods or quieting their concerns with unnecessary clinical treatments. Preparing patients for what actually lies ahead, by empathetically educating them with specifics, can minimize anxiety and fear. Asked in an interview about his first chemotherapy treatment, an adult cancer patient conveyed the healing power of preparation: “I felt armed with what the nurse had taught me. I remember feeling positive and strong. Being prepared made it much better” (Berry, Davis & Wilmet, 2015, p. 91). Some children’s hospitals allow pediatric patients to practice putting a soft toy through a full-scale mock MRI machine before their own actual scans. These practice sessions enable some children to undergo imaging without general anesthesia (McGuirt 2016).
Sustaining Hope When Cure is Not Possible
Clinicians heal when they sustain a patient’s hope regardless of the patient’s disease state. In healthcare, “hope” is usually framed as hope for cure, remission, or halting disease progression. This focused hope centers on achieving a future goal. However, when such a goal is unachievable, hope need not be abandoned. Clinicians who earn patients’ and families’ trust can help them navigate to intrinsic hope, which centers on living in the present with as much emotional resilience as possible. A day filled with intrinsic hope may include a visit with one’s grandchild, a walk in the sunshine, a family meal at home instead of the hospital, or playing cards with a good friend. The end-product of hope’s evolution is freedom hope. The time may come (for patients and families) to free themselves from the pain, suffering, fear, and life upheaval associated with advanced illness, or as one author puts it, “… the peace, the comfort, the joy and the sense of completion when a person chooses to live unencumbered by the demands of modern medical therapy” (Cripe 2016, p. 266). With gentleness and persistence, clinicians can help patients to be hopeful and, depending on the need at a given time, to heal (see Stuart et al. 2019 for greater detail on the three kinds of hope).
Anticipating Emotional Hardships
Clinicians heal when they anticipate patients’ emotional spikes during the course of illness and treatment—and then intervene to minimize adverse effects. Encouraging patients to express their concerns and fears can help in this endeavor. Consider how “Susan,” now healthy and in her twenties but diagnosed with brain cancer at age 14 years, described a nurse’s intervention before surgery: When Ava, my nurse, came by before surgery, she looked me in the eye and said, “Susan, I’m going to braid your hair back so that we only have to shave what we need.” What Ava did shaped how I viewed myself every time I glanced in the mirror during recovery, and when I walked into school surrounded by “normal” girls. Ava probably doesn’t remember braiding my hair, but that moment stuck with me for the past 6 years. (Berry et al., 2021, p. 1898)
Serving Holistically
Clinicians heal when they offer patients a seamless, frictionless, holistic healthcare experience. Serious disease upends normal life, and when healthcare’s moving parts are coordinated and made easier to access and navigate, the emotional upheaval of daily living lessens. Geisinger Health System’s Musculoskeletal (MSK) Institute uses the healing power of coordinated, holistic patient care. It equips each patient on the first visit with an iPad to track outcomes during treatment and for educational purposes. It prioritizes physical therapy and lifestyle changes as first options, with orthopedic surgery as the last alternative. Patients who do require surgery are seamlessly connected to their care team through a digital care-management platform that helps them prepare for surgery, track recuperation goals, record pain and activity, and contact the team with questions or concerns. A 3D knee kinesiography exam is administered to assess the knee in motion, helpful in customizing the care plan (Suk 2022). Geisinger’s high-touch, high-tech MSK service system is designed to heal in all its forms.
Figure 2 summarizes how integrating kindness with competence strengthens patients’ trust in their clinicians and the organizations they represent, paving the way for healing in its truest sense. Trust promotes healing and vice versa, a truism that applies demonstrably to the groups who need healing the most: the poor, the elderly, and the healers themselves. The figure depicts primary relationship and categorizations but does not capture how they intersect - for example, how thoroughness of care overlays with deep listening.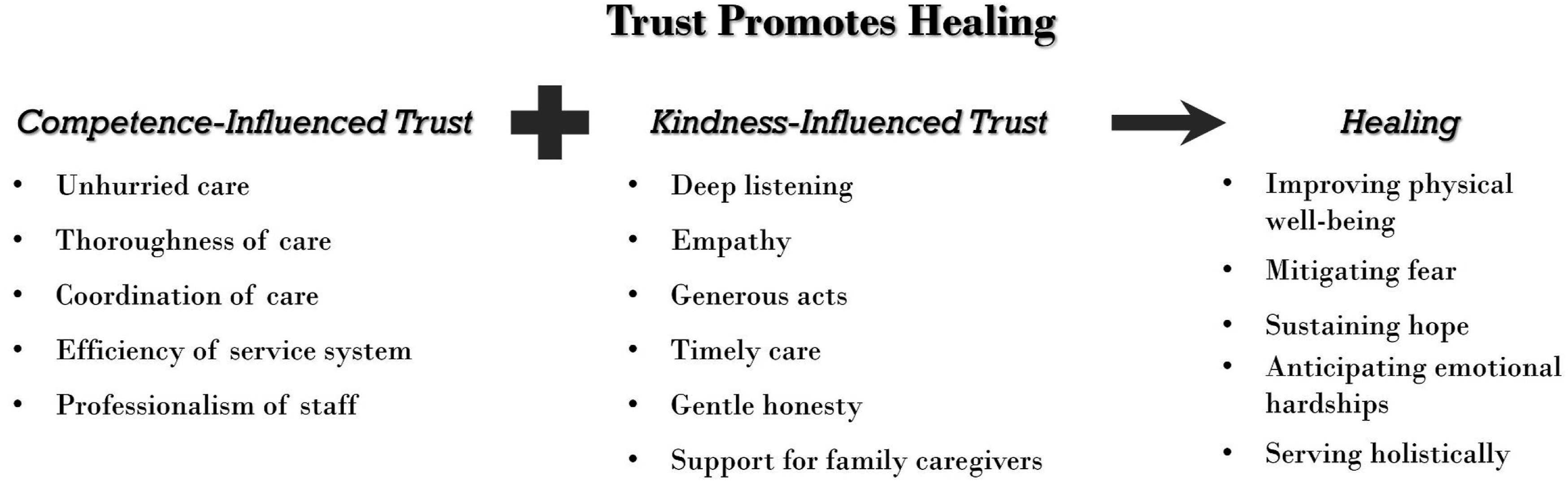
Healing the Poor
Chloe’s dad was in jail when she was diagnosed with cancer. Her mom, desperate for income, struggled to pay rent and started a third job. She sent Chloe to live with relatives near the U.S.–Mexico border, which meant missed medical visits and exposure to preventable infection. Chloe never made it to first grade.
Chloe’s story is too common. People with low incomes are sicker, with increased risk for disease and shorter lifespans, than those with more money. Outcomes are worst for people in poverty, but income-related health disparities exist at levels above the poverty threshold. Improving people’s financial health is a moral imperative that boosts their physical and mental health. But it’s also a practical goal: America’s health system and taxpayers eventually pay the cost of poor health among people experiencing poverty who don’t get preventive and early-stage care.
Poverty’s Definition and Scope
In the U.S., a state of poverty is when someone lacks sufficient income to meet basic needs. The government determines the poverty threshold, which is adjusted annually for inflation and was originally developed in the 1960s based on a family’s food budget. In 2021, the poverty line for a family of four was $26,500 in annual income.
The extent of U.S. poverty is significant, affecting 38.1 million people (11.4% of the population) in 2020. Demographic groups experience poverty at different rates—for example, 19.5% among Blacks, more than twice the rate of 7.3% among white Americans. Poverty rates are higher among children than adults: 14.4% versus 9.9% (U.S. Census Bureau 2021).
U.S. poverty is concentrated in regions, such as rural areas, where the poverty rate was 18.4% in 2019. Poverty varies widely by state: highest in Mississippi at 19.8%, lowest in New Hampshire at 6.6% (U.S. Census Bureau 2021).
Poverty is multifaceted, can persist for generations, and is caused by systemic problems that go beyond income thresholds. Indeed, it underlies most social, environmental, and community drivers of health, hindering access to healthcare, education, food, housing, and other needs (Desmond 2023).
Poverty’s Health Effects
Poverty has wide-ranging influences on health throughout a person’s life. People in poverty are at greater risk for chronic conditions such as heart disease, diabetes, and asthma (Artiga and Hinton 2018). Environmental factors disproportionately affecting the poor, such as exposure to pollutants, poor nutrition, and inadequate housing, are linked to worse health (Braveman and Gottlieb 2014). People in poverty face limited access to healthcare, impeding their link to preventive services and exacerbating existing illness (Artiga and Hinton 2018). The richest American men live 15 years longer than the poorest, and the richest American women live 10 years longer than the poorest (Chetty et al. 2016). During the COVID-19 pandemic, the life expectancy gap by income level increased, disproportionately affecting racial and ethnic minorities (Schwandt et al. 2022).
Children in poverty are especially vulnerable to negative health outcomes. They face higher risk for developmental delays and cognitive impairments (Blair and Rivera 2016). Poverty is associated with poor educational outcomes, which can have lasting influences on health. For example, people with less education are more likely to smoke, be sedentary, and have worse mental health compared with people who have more education (Assari 2017).
Children in poverty are more likely to have adverse childhood experiences, like abuse or neglect, and experience toxic stress, which is prolonged or repeated exposure to stressful situations that can harm physical and mental health (Shonkoff et al. 2012; Center on the Developing Child at Harvard University 2021). Toxic stress can damage children’s developing brains, increase their risks for depression and cardiovascular disease (Shonkoff et al. 2012), and cause heightened emotional reactivity and difficulty regulating emotions, even into adulthood (Center on the Developing Child at Harvard University 2021). Health systems and their partners must address the social drivers of health, such as poverty, to improve the health of children, America’s future workforce.
Healthcare’s Role in Addressing Poverty
America’s healthcare system has traditionally viewed poverty as a social problem outside its scope. It has screened patients for poverty’s downstream effects, such as food and housing insecurity, and then used social workers to provide case management and connect patients with community resources, such as food banks, housing assistance, and financial support. However, this approach has limitations, including a lack of coordination between healthcare providers and community-based organizations, as well as access barriers (e.g., inadequate access to transportation, limited literacy, complex applications for benefits) that result in low follow-through rates on referrals (Crumley, Houston and Bank 2023). Strong evidence also shows that poverty affects biology, thus meriting direct treatment as a medical problem (Marcil et al. 2021).
To that end, more healthcare providers are seeking to help heal patients in poverty by anticipating their hardships and more holistically meeting their needs. Professional associations like the American Academy of Family Physicians (AAFP) and the American Academy of Pediatrics have called for health providers to address poverty directly (AAFP 2021; Council on Community Pediatrics 2016). As such, healthcare systems are building partnerships with nonmedical agencies and in-house strategies to address patients’ financial insecurity as a path toward better health, thereby aligning needed resources with better health outcomes.
Antipoverty medicine is an emerging field addressing patients’ financial strain via medical-financial partnerships (MFPs)—cross-sector collaborations in which health systems and financial services organizations align resources to improve health by reducing patients’ financial strain. MFPs, which leverage the trust between patients and their healthcare providers, offer services in health settings that are tied to improved financial outcomes, including financial coaching, free tax preparation, budgeting, debt reduction, savings support, and job assistance (Marcil et al. 2021).
Many MFPs focus on increasing patients’ income and savings. Consider StreetCred, a program of Boston Medical Center, which helps low-income families file taxes, claim tax refunds, and open 529 children’s savings accounts during visits to clinics and hospitals (Hole, Marcil, and Vinci 2017). The organization has returned over $14 million to over 6,000 families, free of charge (StreetCred 2023). And Early Bird, a program launched by The Impact Factory at The University of Texas at Austin, offers job-search assistance and enrollment in savings accounts and pre-kindergarten to families with young children (Bennett et al. 2022).
Other MFPs focus on anticipating patients’ hardships and reducing their expenses and liabilities. Examples include the Harbor-UCLA Medical-Financial Partnership, which offers medical bill arbitration and financial coaching that helps patients build cost-conscious budgets (Marcil et al. 2021); “Dollar For,” which has eliminated over $25 million of medical debt by helping people access Charity Care, an Affordable Care Act provision that reduces or eliminates medical bills for income-eligible individuals (Dollar For 2023); and Boston Medical Center’s (BMC) community investment, which committed $6.5 million over 5 years, starting in 2017, to improving access to stable housing for its most vulnerable patients. This BMC effort aimed to reduce medical costs and address health issues tied to housing insecurity, such as asthma, lead exposure, and depression (McCluskey 2017). Examples of BMC’s investment include grants to community-based organizations to help families avoid eviction, and to community partners to create a housing stabilization program for people with complex medical problems, including substance use disorder (Metro Housing Boston 2020).
Innovative efforts are bringing medical care directly to the poor, especially where geographic, transportation, financial, and other barriers prevent patients from traveling to medical clinics. For example, an estimated 2,000 mobile clinics in the U.S. are doing 7 million visits annually. The clinics provide medical care, including primary and specialized care, to populations in hard-to-reach areas, including many low-income communities, and they can be equipped with advanced diagnostic equipment for on-site testing and diagnosis. Mobile Health Map, a Boston-based nonprofit, offers a directory of U.S. mobile clinics, collaborates with researchers to evaluate clinics’ health effects, provides mobile clinic leaders with resources to communicate their impact, and advocates for health equity (Mobile Health Map 2023).
Other innovators bring medical care into nonmedical brick-and-mortar sites accessible to the poor. For example, the Stewart B. McKinney Homeless Assistance Act of 1987 authorized Health Care for the Homeless (HCH), which provides federal money to establish medical clinics, staffed with medical and social services providers, in homeless shelters. In 1996, Congress combined HCH with Community Health Centers, Migrant Health Centers, and Primary Care in Public Housing under the Consolidated Health Center Program. Then, the Patient Protection and Affordable Care Act (ACA) of 2010 provided additional resources to expand services and health-delivery sites (National Association of Community Health Centers 2023).
Big retailers like Walmart and CVS Health are bringing medical care to the poor, often in rural communities where healthcare access is limited. Walmart opened its first Health Center in September 2019—offering primary care, vision tests, dental exams, counseling, fitness and diet classes, and more—at affordable prices without insurance (Japsen, 2019). CVS Health has opened nearly 1,000 in-store HealthHubs across America, offering primary care, sports physicals, sleep assessments, immunizations, chronic care management, and health insurance navigation (CVS Health 2023).
The COVID-19 pandemic accelerated remote-based care, with telehealth adoption skyrocketing from 11% of U.S. consumers using telehealth in 2019 to 46% using it to replace canceled healthcare visits in 2020, especially for psychiatric and addiction treatment (McKinsey 2020). However, telehealth use during the pandemic was lower in communities with higher rates of poverty, suggesting that the digital divide is a barrier to widespread access to healing via telehealth for the poor (Patel, Mehrotra, and Huskamp 2021).
Drones delivering health supplies are a promising model for rural and remote U.S. communities such as Native American reservations, where poverty rates are especially high. UPS is even using drones to deliver critical medical samples, including blood and tissue. Likewise, Wing, a division of Google’s parent company Alphabet, has Federal Aviation Administration approval to make such deliveries for Walgreens and FedEx (Wing 2023). In the spirit of healing, such innovations offer hope, anticipate patients’ hardships, and aim to serve people more holistically.
Health systems are working to improve health and reduce costs in partnership with health insurers and philanthropists. For instance, Factor Health, a program at Dell Medical School at The University of Texas at Austin, uses a model whereby philanthropists provide upfront capital to fund a pilot intervention run by a community-based organization, researchers track the intervention’s effects on health outcomes, and insurers agree to fund the project moving forward if previously agreed-upon changes to health outcomes are met by the pilot intervention.
Policy Opportunities to Reduce Poverty
Programs that aim to address poverty in health systems, like MFPs, have so far faced limited scalability (Berkowitz et al., 2018), making policy change crucial in extending the reach of poverty-reduction initiatives. Policy opportunities to reduce poverty and improve health take various forms.
First, policies tied to work garner more bipartisan support. For instance, expanding the Earned Income Tax Credit (EITC), a refundable tax credit for low to moderate-income working individuals and families, can increase employment rates and reduce poverty levels (Hoynes and Patel 2016). Studies show the EITC improves health and education outcomes, such as birth weights, maternal depression rates, and K–12 school performance (Hole, Marcil, and Vinci 2017). In addition, improving childcare subsidies and scaling promising training and employment programs, such as WorkAdvance, can help low-income individuals find and maintain stable employment, which can improve economic security and health (Crumley, Houston and Bank 2023).
Second, policies tied to existing safety-net programs can reduce financial strain and improve health outcomes for low-income people. Protecting programs like the Supplemental Nutrition Assistance Program (SNAP) and Supplemental Security Income (SSI) can ensure access to nutritious food and financial support for millions of people experiencing financial hardship (Keith-Jennings, Llobrera, and Dean 2019). Expanding Medicaid improves access to healthcare (Artiga, Orgera, and Damico 2020) and boosts children’s mental health (Weissman et al. 2023). As of May 2023, 10 U.S. states continue to decline available federal funds to expand healthcare coverage to 138% of the federal poverty level (Weissman et al. 2023). Improving paid family leave opportunities is known to help people with low incomes balance work and family responsibilities, leading to less poverty, increased parental engagement with their children, reduced hospital admissions for abuse-related head trauma in children, and other improved health outcomes for both parents and children (Prenatal-to-3 Policy Impact Center 2023; Han, Ruhm, and Waldfogel 2017). Only 13 U.S. states have adopted paid family leave programs, as of May 2023, leaving much opportunity for boosting Americans’ health (Prenatal-to-3 Policy Impact Center 2023).
Finally, new policies such as extending the federal child tax credit to a more widely accessible child-allowance program have been proposed to reduce poverty and improve health (National Academies of Sciences, Engineering, and Medicine 2019). Other policies known to directly reduce poverty include increasing the minimum wage and expanding access to affordable housing (National Academies of Sciences, Engineering and Medicine 2019).
Society’s health cannot be sustained without sustaining the poor. To save the lives of people like Chloe and improve the health of others in poverty in the U.S., health systems and their partners must address patients’ financial strain head-on, through medical-financial partnerships, innovative care models in conveniently located and trusted places, technology-driven services, and policy change at the local, state, and federal levels. Advancing health equity depends on it.
Healing the Elderly
Early on an October morning, Niki Tone, a Henry Ford Health Home Hospice nurse, received a call that her elderly patient, Mrs. K, just died. Niki had cared for Mrs. K for several months and was close to her and her family. She quickly went to their home, washing and dressing Mrs. K while comforting the family. Niki documented the death, arranged for the funeral home pickup, and informed local police of the paperwork already on file, making their visiting the home unnecessary. Hospice service is sacred; when delivered with Niki’s grace, compassion, and competence, it is beautiful. It heals by helping patients and families make the transition from life to death with dignity and as much physical and emotional comfort as possible (Bruera and Hui 2010). Hospice, performed well, enables more people to die a “good death,” which Parkins (2017) describes as “…free from pain, at peace, and surrounded by loved ones....”
Unfortunately, hospice is grossly underutilized. Underperformance in end-of-life care is but one piece of American healthcare’s failure to serve the elderly equitably, accessibly, and empathetically (Field et al. 2021). Most older people will live for years before needing hospice, but they will need healthcare that is more attuned to their preferences, values, and needs; better coordinated among the multiple clinicians that may be treating them; and based on evidence specifically for an older population.
The Slippery Slope of Overtreatment
People age 65 or older need care that considers their common reality of having multiple chronic illnesses (“multimorbidity”). Patients with multimorbidity account for almost 80% of physician visits and hospitalizations (Blumenthal 2012). These patients often get suboptimal care, however, due in part to poor coordination among the various clinicians who treat them. Poor care coordination contributes to medical test duplication, incompatible medications, lack of follow-up care, and overtreatment that can include unnecessary hospitalizations (Berry et al. 2013; Fulmer et al. 2021).
Unnecessary or unwanted treatment is all too common in older patients, resulting from a confluence of factors in the fragmented care they often receive. Factors include fee-for-service payment that encourages more treatment, patients or family members asking doctors to “do everything,” and clinicians hesitating to candidly discuss the patient’s prognosis for fear of destroying hope (Stuart et al. 2019; Berry et al. 2022). These factors do not always lead to overtreatment, of course, but they are susceptible to it.
Overtreatment, when it occurs, wastes resources and can harm patients. As Gawande (2014, p. 9) writes, “The waning days of our lives are given over to treatments that addle our brains and sap our bodies for a sliver’s chance of benefit. They are spent in institutions—nursing homes and intensive care units—where regimented, anonymous routine cut us off from all things that matter to us in life.”
The Failure of Nursing Homes
Nursing homes as an industry have failed in their central purpose of providing for the safety, health, and overall well-being of residents. The facilities often are stale, foul-smelling, barren, impersonal, and devoid of nature; they don’t feel anything like a home should feel. Residents have little autonomy and safety is at risk, as documented by the disproportionately high number dying from COVID-19 (Yourish et al. 2020). An innovative nursing home leader, Dr. Bill Thomas, confronted what he called the “three plagues” of nursing home living—boredom, loneliness, and helplessness—by placing green plants in the living quarters, adding vegetable and flower gardens for residents to tend, and bringing in dogs, cats, and parakeets to be adopted and named by residents. Residents then used less medication and lived longer (Gawande 2014).
Severe staffing shortages and high staff turnover undermine nursing home quality. Nursing staff levels are commonly well below the standard set by the Centers for Medicare and Medicaid Services (CMS; Grabowski 2022) with annual nurse turnover exceeding 100% (Gandhi et al., 2021). Staff shortages and turnover rates are worse for nursing homes owned by for-profit companies that control about two-thirds of U.S. nursing homes (Grabowski 2022).
Social Isolation and Loneliness
Older people commonly deal with “losses” such as the death of a spouse, relatives, and close friends; their own declining health; diminished mobility and relocating from their home of many years. These events can heighten social isolation and loneliness (SIL), which increase their health risks (Holt-Lunstad and Perissinotto 2023). Before the pandemic, clinicians rarely addressed patients’ social isolation (having few social connections) or loneliness (subjective feelings of distress about a lack of social connections), as these were considered to be outside the scope of medical management (Aronson and Kotwal 2022; Holt-Lunstad and Perissinotto 2023). Although the pandemic clearly accelerated SIL, its presence and health risks have long been known (Murthy 2020).
Risks associated with SIL include coronary heart disease, stroke, diabetes, depression, dementia, infectious disease, and premature mortality (Office of the U.S. Surgeon General 2022). About half of U.S. adults report loneliness (Cigna Corporation 2021; Shovestul et al. 2020), so SIL is clearly an important health issue. SIL can strike at any age, with younger and older adults particularly susceptible (Cigna Corporation 2021). Clinicians, especially in primary care, can help to mitigate SIL by educating patients about it, regularly assessing them for it, documenting their risk in the health record, and offering needed referrals to local community resources or other supports (Holt-Lunstad and Perissinotto 2023).
Reimagining Elder Care
By 2030, an estimated 20% of Americans will be age 65 or older (Czaja et al. 2019). Imagine the societal benefits if more healthcare organizations commit to becoming “age-friendly” by using the best-available evidence to prioritize coordinated, whole-person care, prevention of avoidable disease, and reduced overtreatment harms. Still in its nascent stage, such a movement is actually happening with the growth in the number of age-friendly health systems (AFHSs)—systems that follow the 4 Ms framework (Mate et al. 2021): What
Implementing the 4 Ms starts with deep listening. Listening well to learn patients’ goals and preferences—and the practical realities they face—has value that transcends the financial and productivity pressures of modern medicine. Those benefits include understanding what matters most to patients, recognizing and sensitively acknowledging when patients’ and families’ hopes are unrealistic, and avoiding overtreatment (Barry & Edgman-Levitan, 2012). Simple questions that invite patients’ candor in genuine conversation can reveal otherwise undisclosed information (Berry et al. 2017). Palliative care physician Susan Block facilitates such dialogue with seriously ill patients by asking questions such as “What are your concerns about what lies ahead?”; “What trade-offs are you willing to make?”; and “How do you want to spend your time if your health worsens?” (Gawande 2014).
Physicians’ goals-of-care (GOC) conversations with seriously ill patients can improve outcomes, including pain and symptom control, reduced hospital readmission rates, reduced acute-care utilization, earlier hospice enrollment, and greater patient satisfaction (Casarett et al. 2022; Temel et al. 2010). Duke Health, which committed in 2016 to the goal of having a GOC conversation with patients in the last 6 months of their lives, improved the occurrence of these conversations from 3% of cases in 2016 to 50% by May 2022. The initiative included developing templates to guide the conversations, educating clinicians, instituting reminder triggers in the EHR, and tracking results (Casarett et al. 2022).
Technology-Aided Home Care
Giving older people more of the care they need in their homes facilitates healing. The pandemic showed how swiftly healthcare delivery can move to the home when funding for telehealth is made available (i.e., by aligning incentives for a particular mode of service delivery). Indeed, the CMS’s Hospitals Without Walls program led to a more than 2,000% increase in telehealth use (Patel et al. 2021). In addition, a CMS waiver offers payment for acute hospital care at home (Levine et al. 2021).
Telehealth cannot accommodate patients who need in-person medical care or who lack the requisite technology literacy or infrastructure. Yet, well-executed telehealth can foster healing. Kaiser Permanente (KP), a provider and insurer, pays itself on a capitated basis (a fixed annual risk-adjusted amount per patient) rather than a fee-for-service basis. Capitation incentivizes KP to invest resources to keep patients as healthy as possible, and KP has become a leader in virtual care, given its speed of delivery, comparably lower cost, and opportunity for remote patient monitoring. Consider, for example, hypertension (high blood pressure), a leading risk factor for stroke, heart disease, and other serious illnesses. KP’s patient control rate for hypertension is more than 90%, well above the 50% control rate in the U.S. overall, an outcome aided by virtual care (Pearl and Wayling 2022). KP patients can check their blood pressure at home with a wearable device connected to the electronic health record (EHR) system, enabling timely medication adjustments and better disease control (Pearl and Wayling 2022). KP offers more than 100 online services to its patients, including telehealth visits and email exchanges with their clinicians (Pearl 2014).
Hospitals, primarily serving a geriatric population, can be scary places. They are full of stressors (noisy, hard to sleep in, bright lights, screaming) and prone to medication errors, patient falls, and hospital-acquired infections. Receiving hospital-level care in the comfort of one’s home can be an appealing option under certain conditions. Hospital at home (HaH) is not a new idea, but it has new momentum. The pandemic—and CMS funding—have generated interest in HaH in U.S. health systems. Boston’s Mass General Brigham has provided home-based hospital care to more than 2,000 patients since 2016. Initially focused on home care for patients discharged from the emergency room, the program has evolved to include more conditions (e.g., post-surgical patients) and more entry pathways (e.g., transfers from inpatient status; Conley et al. 2022). In a randomized control trial, both costs and 30-day readmission rates were lower for HaH patients than for similar patients who were treated in the hospital facility (Levine et al. 2020).
Technology plays an essential role in HaH. Mass General Brigham uses it for telehealth, remote patient monitoring, clinical team coordination, and other applications. Patients are cared for with a hybrid model of in-person and video-based remote visits. Advanced practice providers (APPs), registered nurses, and paramedics perform, for example, in-person physical exams, medication management, physical therapy, and wound care—collaborating with physicians, as necessary, remotely or at the bedside. Physicians and APPs deliver up to 50% of acute-care visits via telehealth. Patients’ individualized needs dictate the ratio of in-person to remote care. A key lesson learned is that telehealth visits are more effective after one or more in-person visits are completed, as starting in-person familiarizes the patient and family with the care team and enhances creation of baseline information. Mass General Brigham uses multiple technologies to remotely monitor a patient’s vital signs and a cloud-based task management system that enables team coordination, ordering of supplies for the next home visit, electronic clinical reminders, scheduling of care visits, and other applications (Conley et al. 2022). HaH will not replace conventional hospitals, but it is an important opportunity to implement the 4 Ms more effectively for some patients.
The Power of PACE
Perhaps no healthcare initiative better aligns with the 4 Ms and epitomizes the spirit of healing than a national program, first developed in 1973, called PACE: Program for All-Inclusive Care for the Elderly. PACE members (called “participants”) require nursing home-level care but can continue living in their homes supported by PACE holistic services. Ninety percent of PACE participants are dual-eligible for both Medicare and Medicaid, which together pay for PACE services. As of May 2023, 150 PACE programs operated in 32 U.S. states. The PACE model offers what matters most to its core population of elderly, chronically ill, poor people. It helps these patients live safely at home through a combination of (1) care and assistance (e.g., in-home medical care as needed, helping people take a bath or shower); (2) PACE facility daycare (e.g., group breakfasts and lunches, group games, physical rehabilitation); and (3) home upkeep (e.g., fixing porches, improving lighting, replacing heaters). PACE provides transportation to and from its facilities, operates an onsite medical clinic and pharmacy, and sends participants home with evening and weekend meals.
Evidence shows that PACE reduces hospitalizations, emergency room visits, and other healthcare costs, compared with similar populations (Arku et al. 2022). Aside from saving money, PACE adds dignity, social interaction, and joy to people’s lives. It is an antidote to SIL. With approximately 60,000 participants as of May 2023 (out of more than 12 million dual-eligible people in the U.S.), PACE is underutilized and represents a prime opportunity not only to serve many more elderly poor, but also to serve chronically ill older people in general.
Living Well to the End
Helping people live as well as possible until they die is a cornerstone of healing. There is much to improve in caring for people with life-limiting disease. Two core services for this population are hospice and palliative care. Hospice provides pain management and other comfort-care services for dying patients while also emotionally supporting family members. Hospice reimbursement requires a physician’s referral confirming that the patient is likely to die within 6 months. It also requires patients to forgo further “curative” treatment. Palliative care similarly focuses on relieving physical and emotional suffering but can be offered at any disease stage and does not require patients to forgo curative treatment.
Hospice and palliative care offer genuine healing when they are delivered well. They can improve the quality of daily living, reduce unneeded or unwanted medical interventions, and assist family caregivers (Al-Abdin et al. 2020). Palliative care has also been shown to extend patients’ lives (Temel et al. 2010). Both services, regrettably, are underutilized. About 50% of dying patients do not receive any hospice care, and of those who do, about 25% die within 3 days of joining (National Hospice and Palliative Care Organization [NHPSO] 2020). Research estimates that about 60% of patients who could benefit from palliative care do not get it (Gittlen, 2019).
Increasing the utilization of hospice and palliative care is complex and cannot be fully addressed in this article. However, three ideas merit consideration: 1. Improve the frequency and rigor of quality measurement for hospice. For-profit companies control nearly three-quarters of the hospice sector in the U.S. and, in the aggregate, offer fewer services with less-skilled staff to patients who are less costly to serve, compared with nonprofit hospices (Span 2023; Stevenson and Sinclair 2018; Berry, Connor, and Stuart 2017). Family caregivers of hospice patients report worse care experiences from for-profit compared with not-for-profit hospices (Anhang Price et al. 2023). Unannounced, comprehensive quality-measurement visits by state agencies, coupled with potent enforcements for below-standards performance, are essential. U.S. hospice care will not improve unless delivering high-quality care becomes more profitable than delivering low-quality care. 2. Improve palliative care branding. “Palliative care” is a suboptimal brand name, contributing to its underuse. The clinical name can be used internally for reimbursement without negative consequences, but a name with more appeal is needed for the public and referring clinicians. Indeed, referring clinicians are an important branding audience, as they must convey to patients that this service is about living life to its fullest, not a “death sentence” (Berry, Castellani, and Stuart 2016). Multiple health systems have achieved more and earlier patient use of palliative care by rebranding it as “supportive care” (Fadul et al. 2009; Dalal et al. 2011). Enhancing the patient and family experience with palliative care also strengthens the brand. Palliative care delivered in-person and virtually in the home, by interdisciplinary teams on an as-needed basis, offers the best opportunity to improve the experience (Berry, Castellani, and Stuart 2016). 3. Fuse hospice and palliative care. The word “hospice” connotes death to many people. This perception, coupled with the requirement of ceasing curative treatment, prevents many patients from enrolling in hospice, despite its healing properties at the end of life. Hospice and palliative care services could be beneficially merged into one renamed overall service (such as “supportive care”), with several levels of care available as patients’ needs change. Fusing the two services could eliminate the demand-destroying elements of hospice and strengthen continuity of care, as at least some members of the palliative care team could continue on the service throughout the rest of a patient’s life (Berry et al. 2022). Neither hospice nor palliative care is realizing its healing potential as a separate service, in part reflecting poor understanding of what matters most to older patients and their families—at its core, a marketing failure that misaligns the way the service is “sold” with the value that patients actually seek.
Healing the Healers
Dr. Emily Silverman (2021, p. 2503) writes: “The pager, a black box, sits on my waistband. When I’m writing a note, it beeps; when I’m thinking about someone’s renal failure, it beeps; when I’m telling someone their cancer has spread to their brain, it beeps. … At any point, the pager could beep.… My adrenals squirt adrenaline and cortisol into my bloodstream. My breathing grows shallow; my chest grows tight. Sometimes, when I’m writing notes, I stop breathing altogether.”
Clinicians’ primary role is to heal. However, if they themselves are suffering physically, mentally, or emotionally, they cannot perform this role effectively—or at all. Healers need healing, too. To do this very challenging work requires highly trained, motivated, committed professionals. Being a doctor or nurse is a “dream job” for many, but it is increasingly difficult, resulting in rising healthcare worker (HCW) burnout, moral distress, moral injury, and concern for personal safety. The pandemic worsened these realities but did not create them.
Burnout
Healthcare worker burnout is a crisis, contributing to severe clinical and nonclinical staffing shortages as abnormally high numbers of staff quit their jobs or healthcare entirely. Indeed, more than 40% of U.S. doctors and advanced practice clinicians surveyed in 2021 intend to leave their professions (Linzer et al. 2022), and the U.S. healthcare system is short hundreds of thousands of nurses (Berlin et al. 2022). Burnout, influenced by ongoing stress, is characterized by a high level of emotional exhaustion and detachment, and a low sense of personal accomplishment at work (U.S. Surgeon General’s Advisory 2022). Physician burnout rates have risen from 27% in 2000 to nearly 50% during the pandemic (Prasad et al. 2021)—and are higher still in 2023 (Kuehn 2023).
Healthcare worker burnout has complex causes, including many HCWs believing that their organizations’ leaders prioritize profit over people and productivity over quality, at odds with their personal values (Shanafelt et al. 2021). Clinician performance is increasingly assessed by measures associated with personal productivity and revenue generation, rather than the quality of patient care (Berry et al. 2022). Administrative burdens are a culprit. In one study, outpatient physicians spent nearly 2 hours on “desk work” (including EHR documentation) for every 1 hour with patients (Tai-Seale et al. 2017).
Perceived lack of control and the digitization of care in poorly designed EHRs compound the administrative burden. Clinicians are losing their authority to insurers in determining the appropriateness of treatments—and losing their time to EHRs designed primarily for capturing payment-related data rather than improving care (Shanafelt et al. 2021). The demands of reimbursement and regulatory documentation—and the effort required to search through charting, clinical ordering, and billing information within the EHR—are, in the words of Wachter and Goldsmith (2018), “. . . a disaster for the clinical user.” Burnout is strongly associated with poor EHR usability (Melnick et al. 2020).
Burnout negatively affects the health of HCWs, results in lower quality of care and more medical errors and undermines preparedness for public health crises (U.S. Surgeon General’s Advisory 2022). Burnout also is costly to health systems. The direct costs of replacing a physician, which can exceed $500,000 (Shanafelt, Goh, and Sinsky 2017), include recruiting, onboarding, relocation, sign-on bonuses, and lost payment revenue before a new physician is on the job (Berry and Awdish 2021). Potential indirect costs include disruption for patients and the care team. Staff shortages have led many nurses to join travel-nursing agencies, at twice or more than their usual pay. Use of travel nurses undermines pay equity, team cohesion, and morale (Hilgers 2022).
Moral Distress, Residue, and Injury
Burnout intersects with moral distress, residue, and injury. Moral distress can occur when clinicians cannot deliver the quality of care they wish to give, as when limits are imposed on time spent with patients and insurers deny care claims. Moral residue ensues when unresolved instances of moral distress accumulate. Moral injury can occur from a single egregious violation or persistent moral distresses (Dean, Talbot, and Caplan 2020). Moral injury can result from witnessing overtreatment that benefits the bottom line but not the patient or from being required to care for more patients than is safe (Linzer and Poplau 2021).
Becoming an Employer of Choice
To heal HCWs, employers must embrace a “good-jobs” mindset (Ton 2023). After all, healthcare is a labor- and skill-intensive service whose quality depends on the quality of those who serve.
Values Alignment
Extrinsic factors, such as pay, are important but insufficient to address burnout and create a “good job.” Intrinsic factors, such as organizational values and culture, matter most (Shanafelt et al. 2021). In the randomized control trial study, Healthy Work Place (HWP), values alignment between physicians and organizational leaders, an emphasis on quality, good internal communications, and clinician cohesion were significantly associated with clinician–organization trust and patient–clinician trust (Linzer et al. 2021). In another study of 410,000 HCWs during the pandemic, employees who rated their organization low on its commitment to patient-centered care and quality were more than six times as likely to be planning to quit (Ryan and Lee 2023).
Mayo Clinic annually surveys all staff to assess managers on five kindness dimensions: • • • • •
These behaviors are associated with higher employee satisfaction and job fulfillment and lower burnout rates among Mayo Clinic staff at all levels (Berry, Awdish, and Swensen 2022).
Teamwork needs to be a cultural pillar. It facilitates work cohesion, nurtures reciprocal learning, spurs discretionary effort, and promotes feeling valued. A teamwork culture is built on respect for all, which includes getting input from people closest to the work, communicating transparently, embracing nondiscrimination and fairness, and sharing power (Berry and Awdish 2021).
Protection
Healthcare work can be physically dangerous, emotionally intense, and financially insecure. Healing the healers includes protecting them, to the degree possible. Aside from COVID-19, which cost more than 100,000 HCWs their lives (World Health Organization 2021), workplace violence is on the rise. According to 2022 data gathered by Press Ganey, 57 nurses are physically attacked by patients and visitors every day in the U.S. (two nurses every hour; Riney 2023). Some health systems are responding with training for staff in de-escalation techniques, EHR alerts for patients abusive in the past, wearable alarm technology for HCWs (e.g., a panic button on ID badges), and standardized processes for collecting and analyzing incident data and handling incidents, such as discharging threatening patients (Butkowski, Duncan, and Martinez 2023).
The emotional intensity of healthcare work is easily underestimated. Although the pandemic escalated emotional strain (including the fear of getting sick and bringing the virus home to the family, seeing patients die every day), caring for acutely ill people is inherently hard emotionally. Healthcare workers need “timeouts.” In a study of 80,000 HCWs from 40 U.S. health systems, decompression (being able to disconnect from work, recharge, and find enjoyment away from the job) was found to be a strong source of resilience and an antidote to burnout (Mylod and Lee 2018). Organizations that offer temporary leaves of absence, reduced hours, and temporary role changes for those needing a break or a change help to retain staff and keep them healthy. Employers can also offer flexible work hours, childcare, work transportation solutions, cross-training opportunities, career planning, and more.
Access to emotional support resources is essential. The Providence Health System, with more than 50 hospitals, sponsors a “No One Cares Alone” program whereby behavioral clinician, social worker, and chaplain teams consult with employees in high-stress units (e.g., ICU, emergency department). Providence trains managers to monitor employees for indicators of distress; encourages peer-to-peer support in a “buddy” system; and annually administers an anonymous mental health checkup survey, enabling confidential care for those who need and seek it (Berry, Awdish, and Swensen 2022).
Physical, emotional, and financial stability are intertwined. The healthcare sector must do better in providing fair, equitable pay and benefits to HCWs. Clinicians are often compensated well, and healthcare CEOs may earn millions, but many nonclinical staff are paid poorly (Tyan and Cohen 2020). More than one million HCWs lack health insurance (Berwick 2020). It need not be this way. Providence offers above-minimum wages across its system and free or reduced-cost healthcare to lower-income employees (Berry and Awdish 2021). The University of Arkansas Medical Center guarantees a regional living wage for all hourly workers (Berwick 2020).
Minimize Waste, Measure Progress
Clinicians’ well-being is directly influenced by how much time they spend on meaningful work. Tasks perceived as unnecessary, bureaucratic, or easily delegated contribute to burnout (Linzer and Poplau 2021). A team approach whereby medical and administrative assistants handle administrative and logistical tasks, such as starting the documentation template and preparing anticipated orders, gives physicians a more efficient start when entering an exam room.
More effectively managing clinicians’ online communications and phone calls can materially reduce physicians’ “desk work” (often requiring after-hours attention). The University of California San Francisco Medical Center has created “triage playbooks” for various medical specialties, enabling nonphysician staff to handle much of the desk work for the doctors they support. Henry Ford Health, in Michigan, uses nonphysician specialists to secure insurer approval of treatments requiring it (Berry, Awdish, and Swensen 2022).
Eliminating activity that offers minimal benefit also helps. Hawaii Pacific Health has a “Getting Rid of Stupid Stuff” program whereby staff nominate processes that should be changed or dropped. Among many wins was ceasing to require hospital nursing staff to record hourly rounds in the EHR, saving 1,700 nursing hours monthly at four hospitals (Ashton 2018). The American Medical Association (AMA) has issued a “De-implementation checklist” that includes minimizing alerts, streamlining the login process, and eliminating order requirements for low-risk activities (e.g., fingerstick glucose check) that don’t need physician signoff (AMA 2022).
Redesigning the EHR is a major opportunity. Presenting the patient’s current medical situation clearly and succinctly should be the EHR’s primary function. Commonsense EHR design changes (e.g., a highlighted section displaying tasks needing completion) could save clinicians time and improve care (Berry et al. 2022). Moreover, technology is available for clinicians to enter EHR notes by voice command rather than keyboard. The EHR needs to clarify, not confuse; save time, not waste it; improve patient care, not undermine it; and align a useful technological resource with its real potential value.
Healthcare organizations should include burnout and moral injury data on their performance dashboards, which would signal its importance and enable monitoring (Linzer and Poplau 2021). In addition to using published, validated burnout and moral injury scales (see Rotenstein, Sinsky, and Cassel 2021), data from open-ended questions—such as “What prevents you from doing a job that you are proud of?”—could be included (Palamara & Sinsky, 2022).
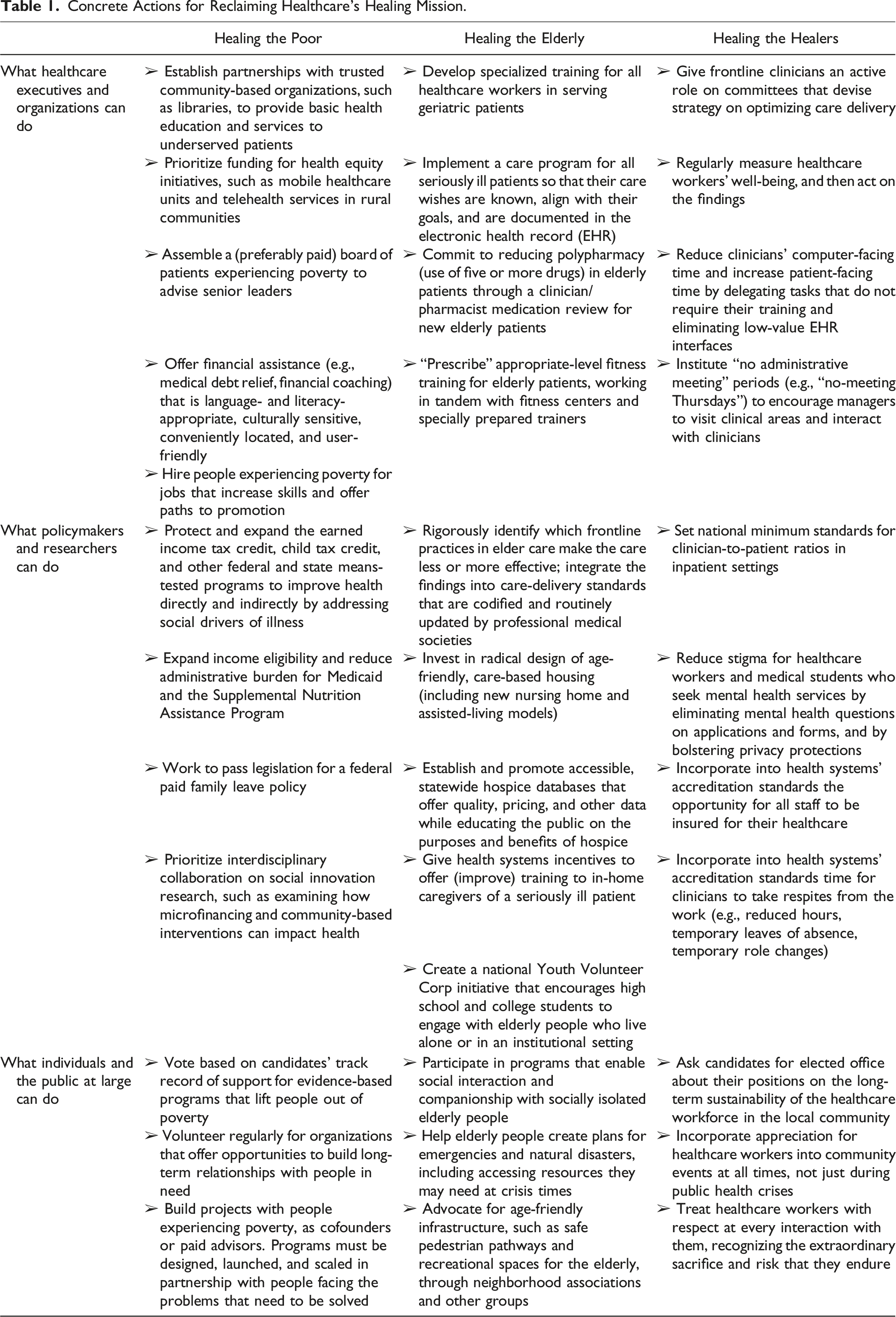
Concrete Actions for Reclaiming Healthcare’s Healing Mission.
Discussion
Framework and Research Opportunities
Our proposed framework aims to facilitate progress toward sustainable healthcare by restoring this service’s healing mission. Given the number and breadth of the challenges, progress will be complex and gradual, perhaps making it seem impossible. Our analysis leaves us optimistic, however, by revealing many creative, practical initiatives that have yielded concrete results, even when small in scale. Those efforts come from a broad spectrum of organizations—hospital-based health systems, NGOs, corporations, and government agencies. The most promising efforts all share an important conceptual thread—alignment, which encompasses three dimensions: resources that are available and deployed, plus incentives and policies that shape and influence the stakeholders’ work.
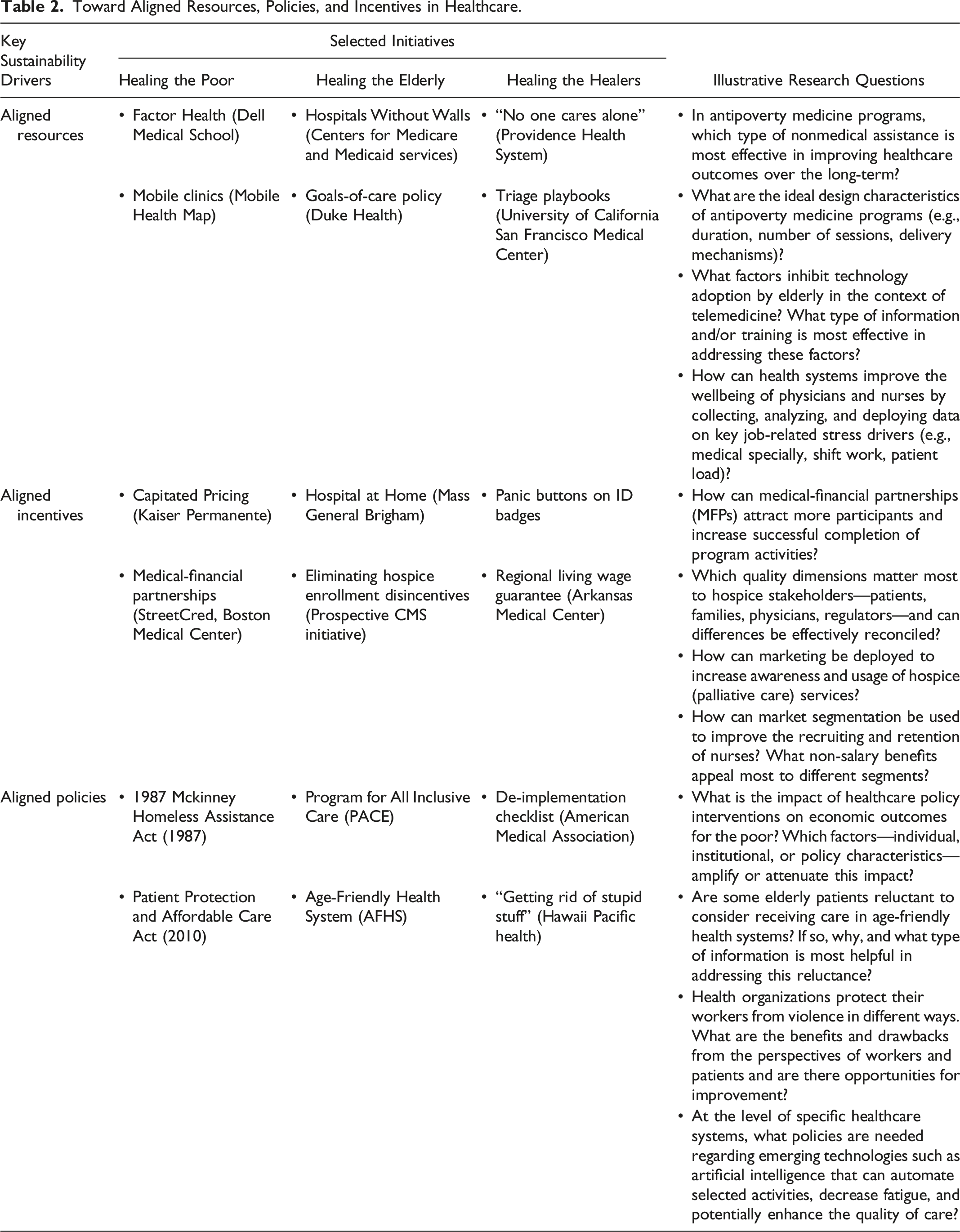
Toward Aligned Resources, Policies, and Incentives in Healthcare.
Before resources can be aligned with desired outcomes, research must elucidate the full scope of resources that different stakeholders in healthcare need. The literature often focuses on financial resources (Makarenko et al. 2021), but human, technological and other resources also matter. Researchers should examine the overlooked role of such nonfinancial resources from the perspectives of providers and recipients of healthcare. For example, we know very little about what coping mechanisms are triggered for clinicians and patients when resources are inadequate. In addition, research should focus on how to align available resources with desired outcomes in different healthcare contexts that vary in size and complexity.
With respect to alignment of incentives—the motivational drivers of behavior—research can leverage extant work from service, consumer behavior, psychology, and marketing more broadly. Consider the “value-centered marketing” framework that Agarwal et al. (2020) have proposed for work in healthcare. Using this framework, the authors argue that the fee-for-service systems that often dominate healthcare are misaligned with patients’ needs and lead to “…unintended overprovision of services” (p. 10). Learning more about how such a counterproductive fee-for-service system evolved and became so firmly entrenched institutionally could clarify and chart the optimal path forward.
Concerning alignment of policies, Aftab et al. (2020) recommend that health policy should inform all other major national policies—what the authors call “health-in-all policies.” Their central rationale is that poor coordination with other national development agendas often hampers health policy—and without such coordination, even well-conceived healthcare policies fail in their stated objectives. Beyond macro-level institutional coordination, various types of entities in the healthcare ecosystem are likely to have their own firm-level policies. These micro-level policies often interact substantially with regional and national policies (Idowu, Schmidpeter, and Zu 2020), suggesting that policy-related work should adopt a hierarchical approach, with a focus on policy interrelationships. Such an integrated examination is likely to uncover where and why policy misalignments occur, potential remedies to consider, and the facilitating role that various stakeholders can play.
Healthcare is a service all people need. It, therefore, will always exist in one form or another. But it is not a given that it will deliver true physical, mental, and emotional healing to patients—especially the poor and the elderly—and to HCWs. These groups are currently underserved because misalignment of healthcare resources, incentives, and policies is undermining U.S. healthcare’s core mission to heal. Healthcare quality can mean the difference between illness and wellness, between life and death.
For-profit companies are greatly impacting healthcare. The largest pharmacy chain, CVS Health, operates in-store medical clinics and owns a major health insurer, home healthcare businesses, a pharmacy benefit manager firm (PBM), and large medical practices. United Health Group, America’s largest health insurer and employer of approximately 70,000 physicians, owns Optum, a $186 billion health services company in 2023 that operates a wide array of businesses, including urgent care, home care, and data analytics companies. Eight of the largest 25 U.S. companies by revenue are healthcare firms (Arpan and Fry 2023). The corporatization of healthcare risks that pursuit of profit over healing will dominate healthcare delivery. However, not-for-profit health systems are not immune from this risk, given that many face extreme financial pressures, particularly rural and “safety net” health systems. For all healthcare organizations, sustaining healthcare means getting mission and margin to be in equilibrium. Leaders who are adept at aligning resources, incentives, and policies can make high-quality, equitable healthcare more profitable than low-quality, inequitable healthcare.
Leaders Who Heal
Healthcare needs exceptional leaders to navigate its myriad pressure points and to reclaim its healing mission. Our focus is on health system leaders, but bold leadership is needed in all parts of the healthcare ecosystem, including NGOs, government, and corporations. Healthcare leaders must perform in the short term to keep the organizations functioning well operationally and financially while transforming it for the long-term (Taylor 2022). To perform and transform, leaders must: • Define what matters. What are the indicators of success? How is organizational and individual performance assessed? What kind of people get promoted? Is caring for the underserved valued? Is quality of care valued? The best leaders shape organizational culture by continually demonstrating the meaning of success. • Stay connected to the work—and the workers. Leaders who interact with frontline service providers better understand the reality of their work and what’s required to make it more effective, efficient, and joyful. They earn trust by being present, by listening and learning, by solving problems. Taylor (2023) describes programs at the dialysis company DaVita—called “Adopt-A-Center” and “Reality 101”—in which senior managers spend time in the treatment facilities performing various jobs and engaging with the staff. In those programs, front-line caregivers teach the executives. • Cultivate “middle” leadership. Most HCWs report to middle managers. Superb leadership in the middle of the organization is critical, and senior leaders make few decisions more important than whom to promote into these middle leadership posts. The CEO may embrace improving care for the poor, but if the manager of the hospital’s pediatrics unit has other priorities, misalignment pushes away the ideas, brainstorming, and trial programming that could lead to high-value innovation. And when HCWs’ passions are squelched, when their voices are unheard, they have more reason to quit, emotionally or literally. • Model generosity. A healing organizational culture is a generous one. Generosity is an input to success, not just an output, because it inspires an organization’s stakeholders and strengthens its reputation. Generosity is needed to align resources, incentives, and policies in ways that inspire HCWs to give their best efforts and health systems to stay true to their healing mission. Generosity—going beyond what is required to help others, allocating resources to serve those in need without expectation of commensurate payment, giving of oneself—is an essential leadership quality. Its absence deflates everything that matters in healthcare. Generosity must start at the top of the organization for it to make its way down through the ranks, for it to be a core value, a primary way of doing business.
A Government That Facilitates Healing
The U.S. government must do better in coordinating and aligning resources, incentives, and policies to reclaim and sustain healthcare’s healing mission. It is not an easy path politically, but it is an essential one. Our primary focus is on the federal government, but state and local governments also play key roles in supporting bold, creative health-sector transformations. Government often provides an unwieldly thicket of uncoordinated mandates, contributing to massive bureaucracy, red tape, waste, and gaps in enforcement. Different agencies do different things (e.g., the Centers for Disease Control and Prevention focuses on population health, the Centers for Medicare and Medicaid on payment), but no agency has the overall responsibility and authority to plan, coordinate, and implement a comprehensive, cohesive, aligned partnership with the organizations that actually deliver healthcare services.
Consider, for starters, what such an omnibus agency, if it existed, could do: • Move reimbursement more completely to a capitated system, wherein healthcare service is pre-paid, incentivizing prevention and early detection of disease, along with greater efficiency in delivery of care. • Redesign government payment protocols to better identify and prosecute cheating—for example, up-charging by inflating patients’ illnesses. Artificial intelligence systems can greatly assist in spotting improperly inflated charges. Catching financial cheating and implementing strong penalties for repeat offenders, including revocation of certifications and operating licenses, and possibly jail time, will save billions of dollars (Berwick 2023). • Create a national, online healthcare-performance dashboard that the public can easily use. The dashboard would present comparative information for individual health organizations on the services they offer, prices, quality metrics, and more. Users would be able to drill down to specific health systems in their local area. • Focus special attention and investment on improving access and care to underserved populations. The PACE model, for example, offers a superior alternative to nursing homes for many, and yet PACE has fewer than 100,000 members in the U.S. The government would improve the lives of the chronically ill elderly while saving money by investing in new ways to pay for and expand PACE. Similarly, both hospice and palliative care are underperforming in terms of usage and, particularly in the case of for-profit hospices, quality (Price et al. 2023). Trials that fuse palliative care and hospice (with reconsideration of hospice provisions, such as giving up curative care, that make it unattractive to many) need to be sponsored. Hospices providing low-quality care should face license revocation if they do not improve to an acceptable level. • Require all Medicare-participating hospitals to follow uniform fair pricing, billing, and debt-collection policies. One hundred million U.S. adults hold medical debt, and many face aggressive debt-collection practices (Berwick 2023). This is not the face of healing. Moreover, nonprofit hospitals should offer measurable benefits to their communities, commensurate with the taxes they avoid because of their nonprofit status (Crowley, Atiq, and Hinton 2021). Local hospitals should be local leaders in marshaling community resources to improve healing.
Conclusion
Health and well-being is a global priority that affects every facet of human activity. U.S. healthcare has an obligation to examine itself, rectify its structural flaws, and reclaim its mission of true healing so that all people, most notably the underserved, benefit and thrive. Leaders from the for-profit, not-for-profit, and government sectors must make it a top priority to fulfill this mission in the broad sense and to figure out, on both the macro and micro levels, precisely how to align resources, incentives, and policies to achieve better health outcomes that are sustainable. As our analysis shows, practical progress is afoot at an array of well-meaning, results-focused organizations. The imperative is for other institutions to learn from those exemplary efforts and step boldly forward to act. Without such action, healthcare runs the risk of becoming less mission-driven and less sustainable for the long term, and that is a dangerous prospect for all of us.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (September 2023):
This article has been updated with minor corrections since its original publication.