
Abstract
Lymphoma is the fourth most common tumor to display placental metastasis. This study aimed to report a case of high-grade lymphoma involving the placenta and review the literature on lymphomas metastatic to the placenta. A systematic review was performed following the PRISMA guidelines, using the keywords “lymphoma” AND “placenta.” All case reports and case series on lymphoma infiltrating the placenta were collected. Eight cases from 7 studies, including the present case, were synthesized. The mean patient age is 29.5 years. The clinical presentation is non-specific. Hematologic derangements included cytopenias or cytoses, and elevated prothrombin time. The mean gestational age (GA) when a diagnosis of lymphoma was rendered is 27 weeks. Five cases presented with either lymphadenopathy or visceral masses on imaging. Four of these cases eventually led to maternal demise. The mean GA when the fetus was delivered is 31 3/4 weeks. Grossly, most placentas had non-specific findings. Leukemic infiltrates were mostly seen within intervillous spaces. Intravillous infiltrates were associated with high-grade lymphomas, resulting in either maternal demise or stillborn fetuses. This study suggests that the placenta has mechanisms to guard against malignancies; however, these defense mechanisms are not foolproof and may be breached by tumor cells.
Introduction
The placenta is a transient organ that interfaces between 2 genetically unique individuals. It functions for nourishing the fetus, protecting against the maternal immune response, and secretion of hormones to support the pregnancy. 1 Although the placenta prevents maternal immunologic assault on the fetus, which is effectively an allograft, normal and malignant cells can cross over from the maternal circulation to the fetal circulation. 2
Like other organs, the placenta may harbor metastatic foci from maternal cancers. Placental metastasis of a maternal malignancy is rare.3,4 The most common metastatic process is a melanoma, whereas lymphoma is the fourth most common tumor type to display fetal and placental metastases. Diffuse large B-cell lymphoma and Burkitt lymphoma are the most common type of non-Hodgkin lymphoma affecting pregnancy. Pregnancy may be a special risk factor for patients with NHL, with a higher proportion of stage IV disease than in non-pregnant women. Pregnant patients with high-grade NHL have a 6-month mortality rate as high as 28.6%. 3 Involvement of the placenta in a pregnancy complicated by malignancy is of special interest. This may shed light on the mechanisms by which the placenta exerts its protective functions, that is, prevention of maternal-fetal transmission.
This study aimed to systematically review the literature for case reports or case series of lymphomas involving the placenta, focusing on the clinical aspects of the disease, histopathologic features, treatment modalities, and outcomes for both the mother and the child. We also report the case of a 31-year-old female with non-Hodgkin lymphoma who presented with placental metastasis during her second pregnancy.
Case Summary
A 31-year-old G2P1 (1001) presented at the obstetrics admitting section with uterine contractions at 34 weeks gestational age (GA) by ultrasound. One and a half years prior to admission, she presented with multiple neck masses. She was subsequently diagnosed as a case of non-Hodgkin B-cell lymphoma, favor diffuse large B-cell lymphoma, at another institution. She underwent chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) during the same year. Six months later, she underwent external beam radiation therapy (EBRT) and Rituximab therapy. The patient was allegedly well after her treatment, with no reported signs and symptoms related to her condition. However, there was no appropriate workup performed to determine whether the patient was in remission. The current pregnancy was unplanned and the patient had only 1 prenatal check-up 1 week prior to admission. Laboratory results were unremarkable except for mild leukocytosis and normocytic anemia (WBC: 12 × 109/L; normal: 4.50–11× 109/L; RBC: 4.01 × 1012/L; normal: 4.2–5.4 × 1012/L). No peripheral blood smear was performed.
The patient’s uterine contractions persisted, which prompted admission of the patient to the labor and delivery room. She eventually delivered a live baby girl who was small for her gestation age, via spontaneous vaginal delivery, at 34 weeks gestational age. No other complications were noted and the patient was discharged.
On the other hand, the neonate had an unremarkable in-hospital course and was discharged along with her mother. She was left to the care of her maternal grandparents. She has been on constant follow-up at the well-child clinic since her delivery, with no clinical and laboratory evidence of lymphoma.
Two months after delivery, the patient was brought to the emergency room due to high fever (39.5°C), associated with tachycardia and dyspnea. Diagnostic work-up at the time of admission showed sinus tachycardia, right-axis deviation, and non-specific ST-T wave changes on electrocardiogram; metabolic alkalosis with concomitant respiratory alkalosis on arterial blood gas; and low levels of albumin (31 g/L; normal: 35–50 g/L), sodium (135 mmol/L; normal: 137–145 mmol/L), potassium (3.3 mmol/L; normal: 3.5–5.1 mmol/L), chloride (84 mmol/L; normal: 98–107 mmol/L), and magnesium (0.67 mmol/L; normal: 0.70–1.00 mmol/L). The complete blood count showed normal WBC count (4.50 × 109/L; normal: 4.50–11 × 109/L) with predominance of neutrophils (0.78; normal: 0.50–0.70), normal RBC count (4.39 × 1012/L; normal: 4.2–5.4 × 109/L), normal hemoglobin (138 g/L; normal: 120–160 g/L), normal hematocrit (0.43; normal: 0.38–0.47), and adequate platelet count (358 × 109/L; normal: 150-450 × 109/L). Blood cultures taken showed no growth after 5 days of incubation. The patient’s condition, however, deteriorated in the emergency room, and she eventually expired 7 hours after admission. There was no consent for an autopsy.
Because of the high-risk nature of pregnancy (preterm labor in a known case of B-cell lymphoma), the placenta was submitted for routine histopathologic examination.
Pathologic Findings
The ovoid singleton placenta measured 14.0 × 10.0 × 1.5 cm3. The trimmed placental weight was 290 g, which is less than the expected placental weight at 34 weeks (300–460 g). The cotyledons were complete. Cut sections revealed a dark, red-brown, firm parenchyma with focal, pale, cream-white areas, which occupy less than 10% of the parenchyma. The paracentrally attached umbilical cord measured 41.0 cm in length and 1.0 cm in diameter and contained 3 vessels, while the extraplacental membranes were shiny, translucent, thin, and gray.
Microscopic examination (Figure 1) showed terminal villi full of capillaries and lined by syncytial knots, which were appropriate for the GA of 34 weeks. Intermediate to large neoplastic lymphoid cells were seen infiltrating the intervillous spaces in all the sections evaluated, that is, in more than 95% of the placental parenchymal tissues examined. The nuclear:cytoplasmic ratio was high. Coarse, granular chromatin was present. Occasional nucleoli were seen. Mitotic figures were also abundant; in some sections, as many as 5 mitotic figures were seen in 1 high-power field. Histologic examination of the pale areas seen on gross examination revealed infarcted villi. The neoplastic lymphocytes are present in the intervillous spaces of both infarcted and viable villi. No lymphocytes are seen within the villous stroma and blood vessels, indicating the absence of chronic villitis.
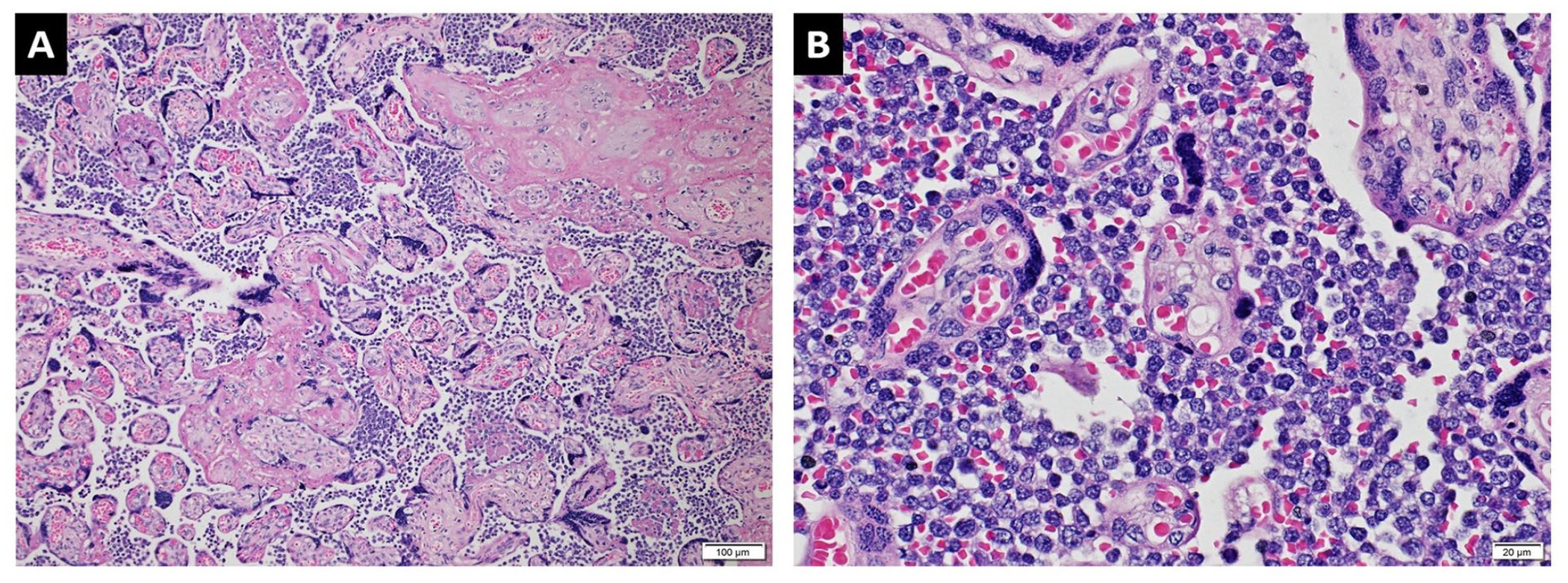
Lymphomatous infiltrates in the placenta. (A) Focally infarcted mature villi are surrounded by atypical lymphoid cells (H and E, 10×). (B) Closer inspection of the villi reveals that the lymphomatous infiltrates are limited to the intervillous spaces (H and E, 400×). Syncytial knots are readily identified in both images.
An immunohistochemistry panel for lymphoma was done (Figure 2). The neoplastic cells showed strong and diffuse staining for leukocyte common antigen (LCA; CD45), CD5, CD10, CD79a, c-MYC, BCL2, and MUM1. Focal positivity for BCL6 was also seen. The neoplastic cells were negative for CD3, CD20, and cyclin D1. Efforts were exhausted to retrieve previous histopathologic material for side-by-side review; however, the authors were unable to retrieve the slides.
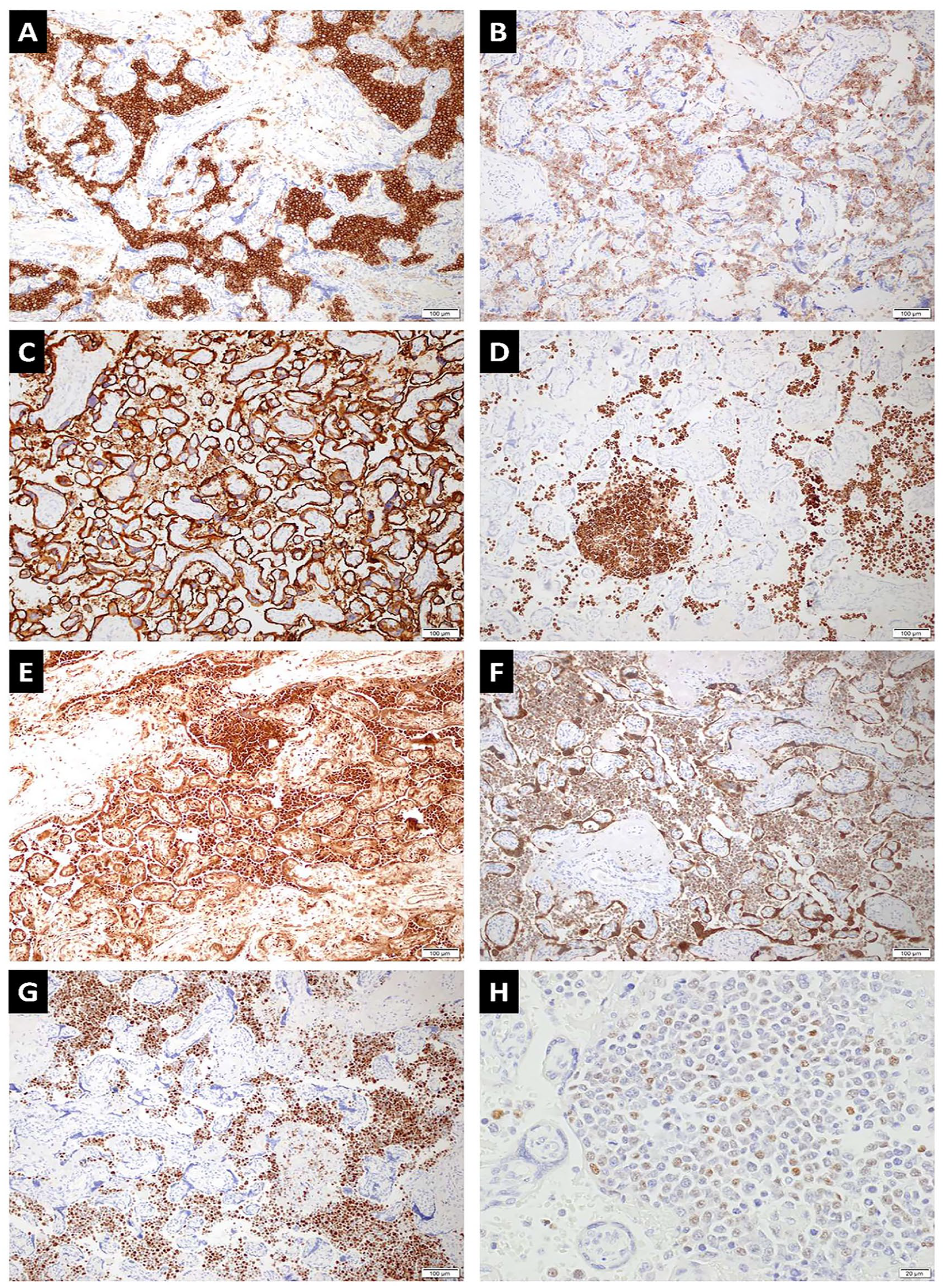
Immunohistochemistry studies show that the tumor cells are positive for (A) LCA/CD45, (B) CD5, (C) CD 10, (D) CD79a, (E) c-MYC, (F) BCL2, and (G) MUM1; focally positive for (H) BCL6; and negative for CD3, CD20, and Cyclin D1 (A–G, 10×; H, 400×).
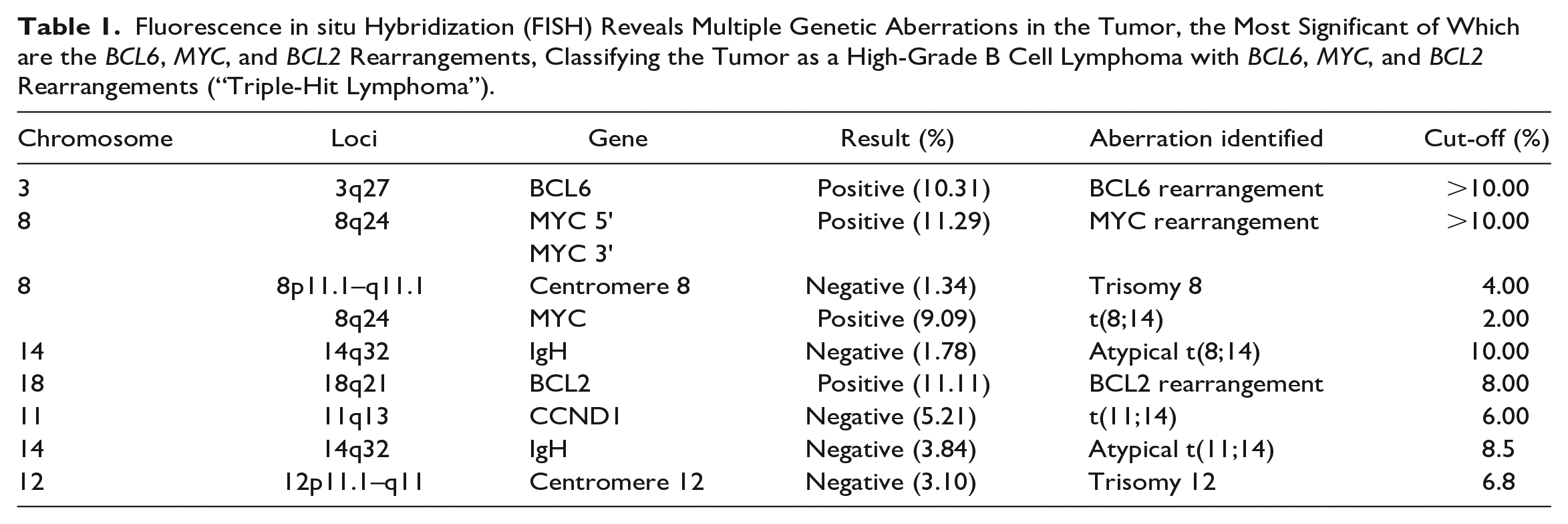
Fluorescent in situ hybridization (FISH) was done for this case, which revealed multiple genetic aberrations in the tumor, the most significant of which were BCL6, MYC, and BCL2 rearrangements (Table 1). Given these findings, the case was signed out as high-grade B-cell lymphoma (HGBL) with MYC, BCL2, and BCL6 rearrangements, or triple-hit lymphoma.
Fluorescence in situ Hybridization (FISH) Reveals Multiple Genetic Aberrations in the Tumor, the Most Significant of Which are the BCL6, MYC, and BCL2 Rearrangements, Classifying the Tumor as a High-Grade B Cell Lymphoma with BCL6, MYC, and BCL2 Rearrangements (“Triple-Hit Lymphoma”).
Materials and Methods
A systematic search was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The PubMed and SCOPUS databases were searched using the keywords “lymphoma” AND “placenta.” The search included articles from 1947 to 2021. The references of each article were also screened for similar studies. All case reports and case series on patients with histopathologic documentation of lymphoma infiltrating the placenta were collected. Inclusion criteria for the articles are (1) case reports or case series with individual descriptions of cases; (2) gross and microscopic examination of the placenta was performed; and (3) a diagnosis of lymphoma metastatic to the placenta was rendered after histopathologic evaluation, with or without ancillary studies. A study was excluded if there was no detailed description of the histopathologic findings in the placenta.
Data collected included patient age, pertinent clinical and imaging findings, laboratory results, GA at the time of pregnancy, histologic subtype of the lymphoma, ancillary tests done to confirm the diagnosis, treatment given to the mother and fetus, and maternal and fetal outcomes.
Through the database search, 262 articles possibly related to the study were identified. After screening the abstracts for relevance, 239 articles were excluded. In addition to the remaining 23 articles, 6 more studies were identified by reading through the reference list of each article. After removing duplicates (2) and studies in which the full text is not available (8), the full text of the remaining 19 papers was assessed. Twelve papers were eventually excluded, as shown in Figure 3. These papers were excluded because of the following reasons: the metastasis was not a lymphoma, there was no breakdown of the cases, the placenta was not involved, the histology of the placenta was not described, and 1 was a response to another paper. A total of 7 articles were included for qualitative analysis.
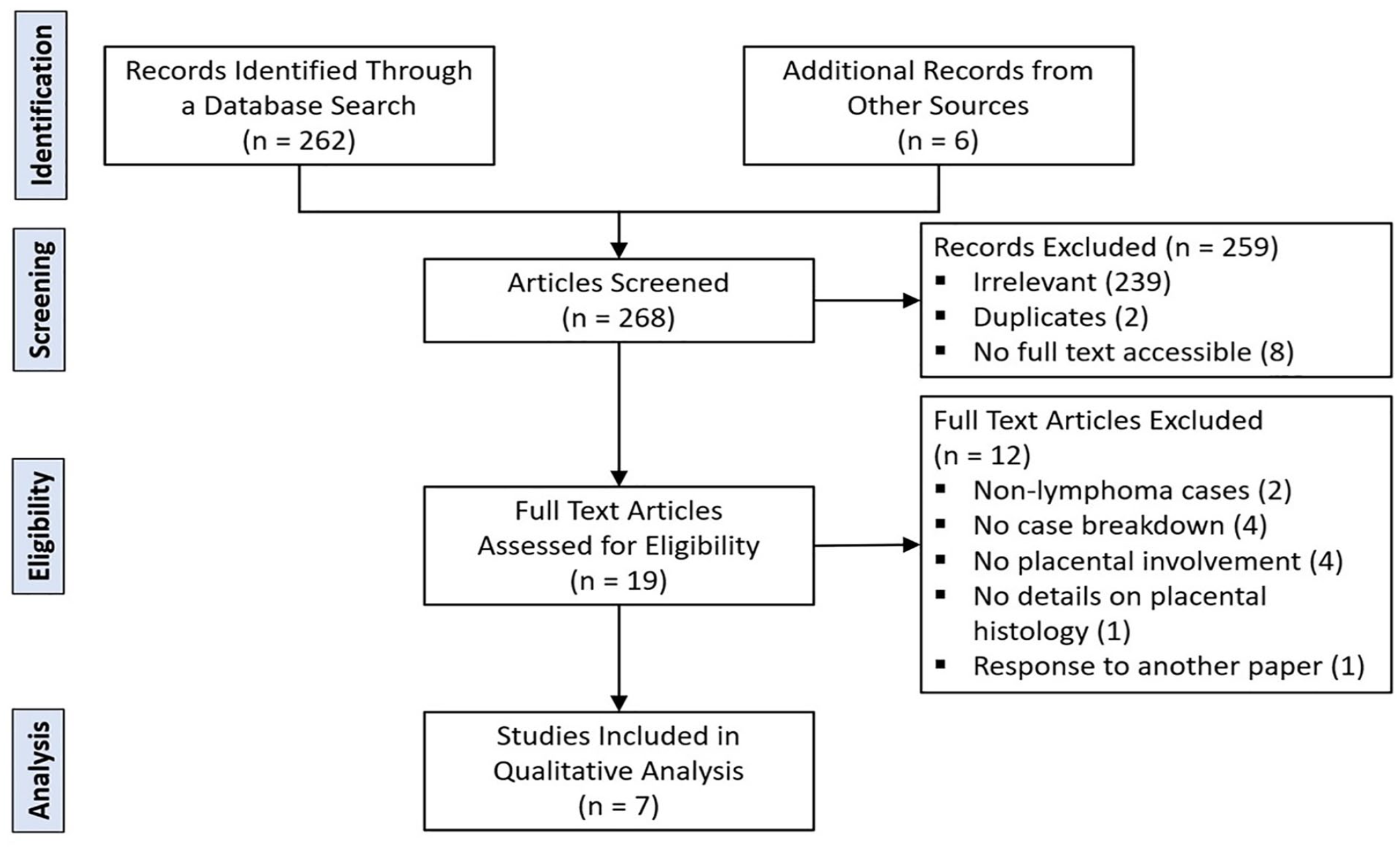
Systematic review based on the PRISMA guidelines.
Results
Eight cases from 7 studies, including the present case, were synthesized.5–11 The data collected from each study are presented in Table 2. All cases from the literature were newly diagnosed during pregnancy, except the present case. The patients’ age ranged from 15 to 35 years, with a mean of 29.50 years.
Clinico-Pathologic Features of the Eight Cases Included in this Systematic Review, Including the Current Case.
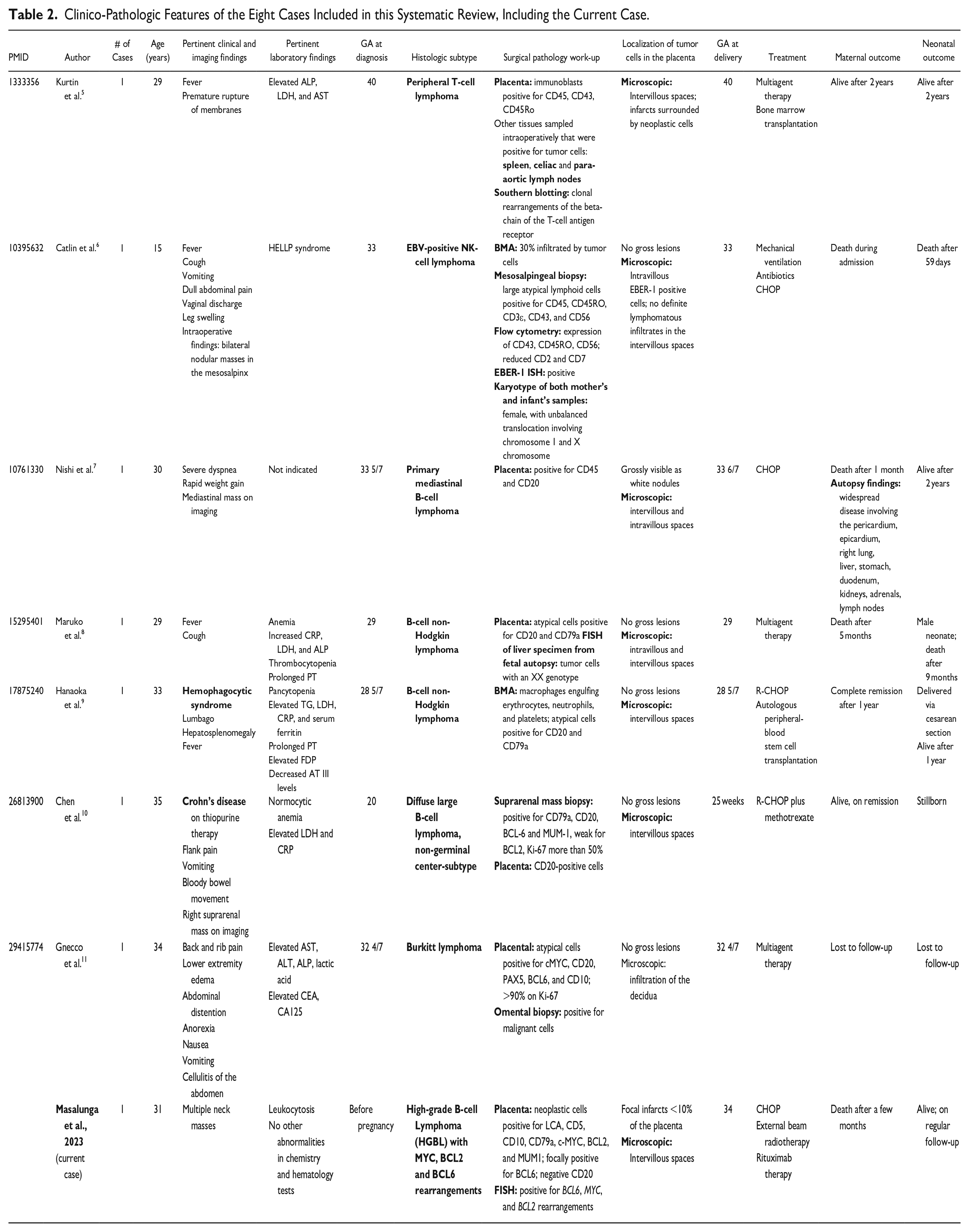
The clinical presentations of the patients are varied and non-specific. Most of them are related either to the current pregnancy, such as gastrointestinal symptoms, or to other co-morbidities, that is, hemophagocytic syndrome and Crohn’s disease. Derangements in hematologic parameters included cytopenias or cytoses, and elevated prothrombin time (PT). Most of the lymphomas were diagnosed during pregnancy, at a mean GA of 27 weeks. The present case was diagnosed before pregnancy.
Five cases presented with either lymphadenopathy or visceral enlargement on imaging, of which 4 are mature B-cell neoplasms. Four of these cases with either enlarged lymph nodes or visceral masses eventually led to maternal demise. The mean GA when the fetus was delivered is 31 3/4 weeks.
Grossly, most of the placentas were either unremarkable or had non-specific findings. One exception was a case of primary mediastinal B-cell lymphoma, which presented with white nodules in the placenta. Microscopically, most of the leukemic infiltrates were noted within the intervillous space. Three cases presented with intravillous infiltration, including the case where EBER-1-positive cells were detected within the villi. All were associated with high-grade lymphomas and resulted in either maternal demise or stillborn fetuses.
Discussion
This case presents the first fully documented case of a high-grade, B-cell, “triple-hit” lymphoma complicating a pregnancy, documented by immunohistochemistry and cytogenetic studies. The case also shows loss of CD20 expression after treatment with rituximab, a common but potentially perplexing finding in the evaluation of hematolymphoid neoplasms.
High-grade B cell lymphoma (HGBL) is a heterogeneous group of aggressive, mature B-cell lymphomas that resemble DLBCL, NOS, or Burkitt lymphoma (BL), or both DLBCL and BL morphologically but are classified separately due to biological and clinical reasons. HGBL can be subcategorized based on the presence of MYC, BCL2, and BCL6 rearrangements. Aggressive mature B-cell lymphomas characterized by a MYC rearrangement at chromosome 8q24 can either have a rearrangement in BCL2 (at chromosome 18q21) and/or in BCL6 (at chromosome 3q27). Coexistence of either the MYC rearrangement as well as BCL2 or BCL6 rearrangements would qualify the tumor as a “double-hit” lymphoma (DHL), whereas the presence of both BCL2 and BCL6 rearrangements in addition to the MYC rearrangement would classify it as a “triple-hit” lymphoma. 12
The presence of the double-hit or triple-hit status carries a poor prognosis. They both predict poor response to standard chemoimmunotherapy and increased risk of progression and central nervous system involvement. 4 DHLs also typically present at a more advanced stage and have a higher risk for extranodal and bone marrow involvement, as well as leukemic or circulating disease. 13
HGBL consists of a heterogeneous group of B-cell lymphomas with various histologic features. This case features the classic DLBCL histologic picture: large, atypical lymphoid cells whose nuclei are the same size as or larger than twice the size of normal lymphocytes, with relatively few small, non-neoplastic lymphocytes present. 12
Pregnancy-Associated Malignancies
The incidence of different types of cancer in pregnancy mirrors the incidence of cancer seen in nonpregnant women of the same age. The most common types, in decreasing frequency, are carcinomas of the breast, cervix, and lung, melanoma, lymphoma, and leukemia. Despite the relatively high incidence of pregnancies with malignancy, metastatic lesions to the placenta continue to be a rare occurrence. In terms of frequency, the leading subtypes of cancer involved in placental metastasis are reported to be melanoma, followed by breast cancer, lung cancer, leukemia, and lymphoma. 14
Although the clinical features of malignancy occurring in the setting of pregnancy may initially be non-specific, certain findings might alert the physician to the possibility. In the case documented by Hanaoka et al, 9 in which the patient presented with hemophagocytic syndrome, the marked hepatosplenomegaly and the lack of response to glucocorticoid therapy were suspicious for an underlying malignancy. Aside from the non-specific features, clinicians may be reluctant to pursue clinical investigations during pregnancy. 11
It is suggested that physiologic attributes during pregnancy, such as pregnancy-associated immunodeficiency and a higher concentration of sex hormones, may contribute to transplacental or fetal metastasis. Higher levels of estrogen and progesterone during pregnancy may lower both innate and adaptive immune system activity, 3 thereby allowing a higher chance for immune evasion by cancer cells.
It is hypothesized that the same physiologic mechanisms that allow for maternal tolerance of paternal antigens on the fetal cells within the placenta may be utilized by maternal tumor cells. 2 In particular, the placenta induces epigenetic silencing of T-cell-attracting cytokine genes in the maternal decidua. 15 In addition, embryonic trophoblasts at the maternal surface do not express classical and polymorphic HLA-A and B proteins, but rather, express non-polymorphic HLA-G, C, and E molecules. 16 These have been found to block NK cell and dendritic cell activity and promote invasiveness. 17 This may explain why highly aggressive lymphomas are more prevalent in pregnant women than in nonpregnant women of the same age, where highly aggressive NHL accounts for 5% of cases.18-20
Maternal Complications of NHL During Pregnancy
In a systematic review by Horowitz et al, 3 they classified the patients into 3 groups, wherein indolent lymphomas make up 5% of cases, aggressive lymphomas (DLBCL and T-cell lymphomas) made up 48% of cases, and highly aggressive lymphomas (immunoblastic lymphoma, Burkitt lymphoma, and unspecified highly aggressive lymphomas) accounted for 47% of cases. Those with aggressive and highly aggressive histologic groups had 15.7% and 52% 6-month mortality rates, respectively. Among the histologic types, Burkitt lymphoma was associated with the highest 6-month mortality rate (61.5%), followed by unspecified high-grade NHL (28.6%), peripheral T-cell lymphoma (25%), DLBCL (12.8%), and immunoblastic lymphoma (4%). Furthermore, diagnosis before the year 2000 (pre-rituximab era), highly aggressive histology, and advanced clinical stage were all associated with an independent adverse effect on short-term maternal survival. 3
In general, metastatic disease to the products of conception confers a poorer prognosis for the mother, with 93% dying shortly after delivery. 21 Among those with pregnancy-associated NHL, the proportion of those diagnosed with stage IV disease is higher than those reported in non-pregnant women. 3
Fetal Complications of NHL During Pregnancy
Most cases of placental involvement are associated with minimal fetal complications. 4 In pregnancies involved with NHL, 100 of 120 of the pregnancies ended in live births, 11 pregnancies were electively terminated, 5 ended in spontaneous abortion, and 1 resulted in intrauterine fetal death. Of those delivered, 3 died after delivery, 2 were born preterm, and 1 died of lymphoma. 3 Massive placental infiltration by maternal metastasis can lead to intrauterine fetal demise, probably due to limitations in the supply of blood and nutrients to the developing fetus. 4 In the present case, microscopic examination revealed that most of the intervillous spaces (>95% of tissues processed) are infiltrated by the neoplastic cells. Other possible causes for the low fetal weight could be the previous chemotherapy and radiotherapy undertaken by the mother close to the pregnancy.
Placental Involvement by Lymphoma
When maternal hematologic malignancies involve the placenta, the involvement is usually seen on microscopic examination. 22 In this literature review, only 1 of the cases presented with grossly visible nodules. 7 The current case showed pale areas that proved to be infarcts on microscopic examination, but there were no grossly distinct nodules. Furthermore, the lymphoma cells are limited to the intervillous space rather than extending into the actual villi. This suggests that the tumor has not invaded the placental parenchyma and consequently, fetal tissues. This raises the possibility that the placenta has defense mechanisms that prevent the spread of maternal cancer to the fetus. 21
Walker et al 21 postulated that physiologic and immunologic barrier mechanisms are responsible for the low rates of placental and fetal invasion by maternal tumor cells. Physical barriers such as the positive pressure gradient from fetal capillary to intervillous space and complete separation of chorionic villi and fetal trophoblast prevent the passage of cellular components from the mother to the fetus. Immunologic barriers include the elaboration of interferon-gamma (IFN-y) by immune cells and cell-mediated responses, including natural killer cells. 9
While the exact mechanisms remain to be elucidated, the cases included in this review suggest that a more adverse fetal outcome occurs when the malignant cells infiltrate the villi. Careful examination of the placenta is therefore essential in the prognostication of the neonate. It is suggested that at least 3 sections of the placental disk be taken for histopathologic evaluation. 22 Additional sections may be taken for grossly suspicious areas. It is suggested that 1 of the reasons for the transmission of tumor cells to the fetus may be the immaturity of the fetal immune system in early gestation, as well as there being available space in the early fetal bone marrow for engraftment of the tumor cells. 9 Other authors suggested that HLA homozygosity may play a role in the non-rejection of maternal tumor cells. 8
Downregulation of CD20 Expression With Rituximab Therapy
Rituximab has been widely used for the treatment of relapsing or advanced-stage B-cell neoplasms with a 50% efficacy rate, and a 40–50% recurrence rate among treated patients. In a study by Chu et al, 23 they reported that 37% (13 of 35 cases) of Rituximab-treated recurrences were associated with loss of expression of CD20 by immunohistochemical or flow cytometric studies. The aberrant loss of CD20 antigens, as in our case, has been suggested as a mechanism of resistance. A panel of other B-cell markers is suggested for the diagnosis of recurrent B-cell lymphomas post-rituximab therapy. 23
Conclusion
The underreporting of placental metastases may be because many placentas appear normal upon gross examination and therefore are not adequately examined histologically. In our case, only focal infarcts were present in the placenta, and microscopic examination was needed to yield evidence of placental involvement. For pregnancies associated with malignancy, all placentas must be submitted to rule out any microscopic metastasis. The placenta can provide valuable material for further testing to confirm a malignant diagnosis.
The presence of MYC, BCL6, and BCL2 rearrangements seen in triple-hit lymphomas, as confirmed by cytogenetic studies, confers an aggressive clinical course and a poor prognosis for the patient. The diagnosis of these tumors requires a combination of histomorphology, immunochemistry, and cytogenetic studies.
There is still a lack of data regarding the mechanisms facilitating placental metastases from maternal cancer, as well as the protective factors that limit the incidence of both placental and fetal metastasis. However, the presence of neoplastic cells within the intravillous spaces is suggestive of a poorer prognosis for both the mother and the fetus. Further molecular studies may be able to elucidate the mechanisms involved in how malignancies breach the placental barrier.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Informed consent was secured for the case report portion of this study. In accordance with the World Medical Association Declaration of Helsinki, an ethics statement does not apply to the systematic review because the study is based exclusively on published literature.