
Abstract
Objectives
To investigate the correlation between prenatal ultrasound (US) and autopsy findings in pregnancies terminated due to isolated congenital heart defects (CHDs), including CHDs associated with heterotaxy syndrome.
Materials and methods
The material consists of 67 fetuses with prenatally detected isolated CHDs or CHDs associated with heterotaxy syndrome at a tertiary center in Norway between 1985 and 2014. The main CHDs were categorized into subdiagnoses of CHDs in accordance with ICD-10. The US and autopsy findings were categorized according to degree of concordance.
Results
Gestational age at termination was 12 + 0–22 + 6 weeks. Hypoplastic left heart syndrome was the most common main diagnosis among the 67 fetuses (32.8%). There was full agreement between US and autopsy findings in 97.4% (222/228) of all subdiagnoses. The discrepant findings in three fetuses had no influence on the decision to terminate the pregnancy.
Conclusions
The correlation was high between prenatal US and postmortem findings in fetuses with isolated CHDs. Meticulous assessment of cardiac anatomy is particularly necessary when the decision to terminate relies on isolated CHDs. The trend of earlier termination challenges verification of diagnoses at autopsy. Consequently, the fetus should be examined at a tertiary center with fetal medicine specialists, pediatric cardiologists and perinatal pathologists.
Keywords
Introduction
A systematic assessment of the fetal anatomy at the second trimester ultrasound (US) examination has become an essential part of the prenatal examinations to locate disorders which may influence the care of the pregnancy. In certain cases, disorders detected are of such a severe nature that termination of the pregnancy (TOP) may be an option for the parents. It is then of utmost importance that the US diagnosis is correct.
Since the systematic examination of the fetal population was introduced in the eighties, the correlation between the prenatal US findings and autopsy results has been assessed over time with respect to the various organ groups.1–6 Some fetuses may have multiple anomalies, often with chromosomal aberrations as the dominant condition. In fetuses with multiple structural or chromosomal anomalies, the decision to terminate a pregnancy may be based on a platform of several severe diagnoses. Congenital heart defects (CHDs) have traditionally been difficult to detect and relatively often anomalies associated with the CHDs are located first.3,7
As a consequence of the focus on increasing the prenatal detection rate of CHD in general, cases with isolated CHDs are also being detected. 8 If this leads to TOP being an option, detailed prenatal and postmortem assessment of the cardiac anatomy is essential since the diagnosis relies on an isolated CHD without any associated anomalies.
The aim of this study was to investigate the correlation between prenatal US diagnoses and autopsy findings over a 30-year period, in pregnancies terminated because of isolated CHDs, including CHDs associated with heterotaxy syndrome in the fetus.
Materials and Methods
Included in the study were data from pregnant women who, during the period from 1985 until and including 2014, had a prenatal US examination performed at the National Center for Fetal Medicine (NCFM) that was followed by termination of pregnancy and a subsequent autopsy at the Department of Pathology; both institutions are located at St. Olavs University Hospital in Trondheim, Norway. The selected material comprised pregnant women from the catchment area of the hospital as well as referrals from all over Norway, as NCFM is a national referral center.
In Norway, the second trimester US examination is performed at 18 gestational weeks by Certified Nurse-Midwives with one-year university based Postgraduate Certificate in Obstetric Ultrasound and includes a detailed examination of the fetal anatomy. At NCFM, the prenatal US data, along with several variables including maternal age, obstetric history, detailed outline of congenital anomalies including karyotype, and results of fetal invasive procedures are prospectively registered in an extensive database which was designed at the introduction of routine US in Norway in 1986 to track the consequences of the national program at our center.
From an autopsy series of 1029 TOP cases with congenital anomalies including chromosomal aberrations, there were 320 fetuses with CHDs. 5 From the latter group, we included 67 fetuses with isolated CHDs for detailed evaluation. Ten of these fetuses had CHDs combined with heterotaxy syndrome and were included as none of these had extracardiac anomalies except for the abnormal arrangement of internal organs; this anomaly did not influence the decision for TOP and allowed an additional 10 cases to be part of the study group. Fetuses with CHDs and extracardiac and/or chromosomal anomalies were not included since the associated anomalies in this heterogeneous group could have had an impact on the decision for TOP.
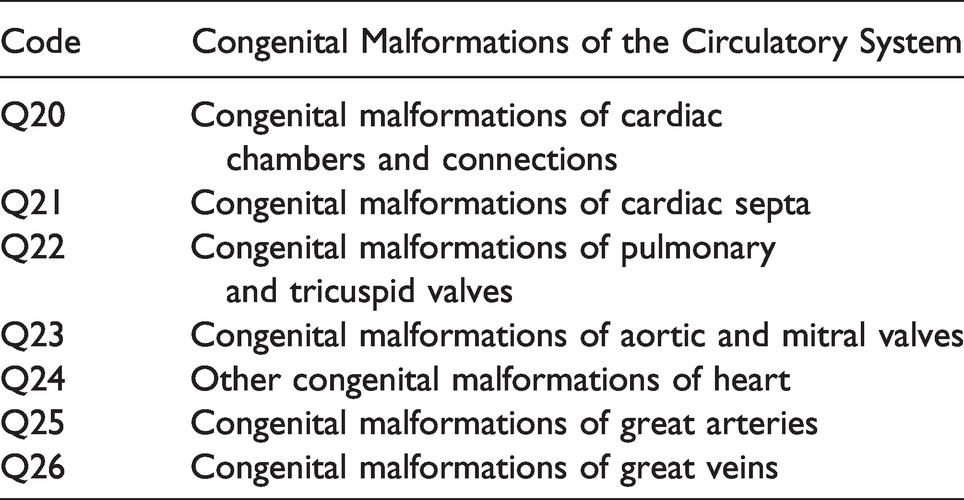
When the NCFM was established in 1990, a pathologist with experience in perinatal pathology was included in the team of experts, a practice which over time has been reinforced. Following termination of pregnancies, autopsies were classified according to affected organ groups. To facilitate a detailed comparison with the prenatally detected anomalies of the heart with the autopsy findings, each single anomaly, e.g. ventricular septal defect (VSD), and all subdiagnoses involved in a main diagnosis or syndrome, e,g. hypoplastic left heart syndrome (HLHS), were subcategorized and registered separately. The subcategorization of CHDs was based on the classification by the World Health Organisation, Clinical Modification codes (ICD-10) under the group, “Congenital malformations of the circulatory system” (Q20-Q26) (Table 1). 9
WHO Classification of Congenital Malformations of the Circulatory System, ICD-10 Codes. 9
Fetal medicine experts were responsible for the final US examinations at the NCFM. With few exceptions, a pediatric cardiologist was present during the US scans. Pregnancy length and expected day of delivery were mainly determined at the 18th week routine scan by measurement of biparietal diameter (BPD) in most fetuses or by femur length (FL) when BPD for various reasons could not be used. In early pregnancies, BPD or crown-rump length (CRL) was used.
For all 67 cases, TOP was approved by the regional abortion committee. According to Norwegian law from 1975, with later revisions, 10 the upper limit for termination was based on the earliest gestational age for possible survival of newborns. Until the 1990s, the upper limit was 23 + 6 weeks, which, from 2001, was changed to 21 + 6 weeks. Termination of pregnancy was preferably performed the day after the decision for termination was made. All abortions were induced medically to preserve the completeness of the specimen.
The pathologists had regular meetings with the fetal medicine experts, and the prenatal US reports were available to the pathologist before postmortem examination. From 1991, the autopsy protocol was standardized to include whole-body radiography and photography, to document external and internal abnormalities. The heart was examined in situ before the arterial connections were cut. If more than one cardiac defect was found, the anomalies were classified according to the most serious defect.
CHDs were categorized as major or minor in accordance with Mitchell et al. 11 The heart defects were grouped as simple or complex. A simple heart defect was defined as one without additional cardiac defects, e.g. transposition of the great arteries (TGA) or atrioventricular septal defect (AVSD). A heart defect was defined as complex when additional heart defects were present, e.g. TGA with pulmonary atresia.
Correlations between US findings and autopsy findings were categorized in accordance with a modification of the method described by Isaksen et al.
12
Full agreement between ultrasound and autopsy findings Minor autopsy findings not seen or recorded at ultrasound examination Major autopsy findings not detected at ultrasound examination None of the autopsy findings suspected at ultrasound examination Ultrasound findings not confirmed or not possible to confirm at autopsy
SPSS 25.0 (SPSS Inc., Chicago, Ill., USA) was used in the statistical analysis, and correlation analyses were performed using independent samples t-test. P < 0.05 was considered statistically significant.
The study was approved by the Regional Committee for Medical and Health Research Ethics in Norway (REK 2009/790). Since this is autopsy material, the Regional Ethic Committee gave dispensation from informed consent.
Results
The present study included data from a total of 67 terminated pregnancies, 38 from the catchment area of the NCFM and 29 from referring hospitals. The pregnancies were terminated at mean gestational age 19 + 0 weeks (range: 12 + 0 to 22 + 6 weeks). Eleven (16%) of the pregnancies were terminated between weeks 12 + 0 and 16 + 6. The sex distribution was 44.8% females and 55.2% males. The mean maternal age was 29 years (range: 21–41 years).
Table 2 shows the main diagnosis after autopsy in all 67 pregnancies terminated due to isolated CHDs. The dominating group comprising 22 (32.8%) of the total 67 fetuses was HLHS, which includes hypoplastic left ventricle, aortic and mitral atresia/stenosis and aortic arch hypoplasia. LAI was the second most common main diagnosis (8.9%, 6/67).
Main Diagnosis Based on Autopsy Results in 67 Pregnancies Terminated due to Isolated CHDs.
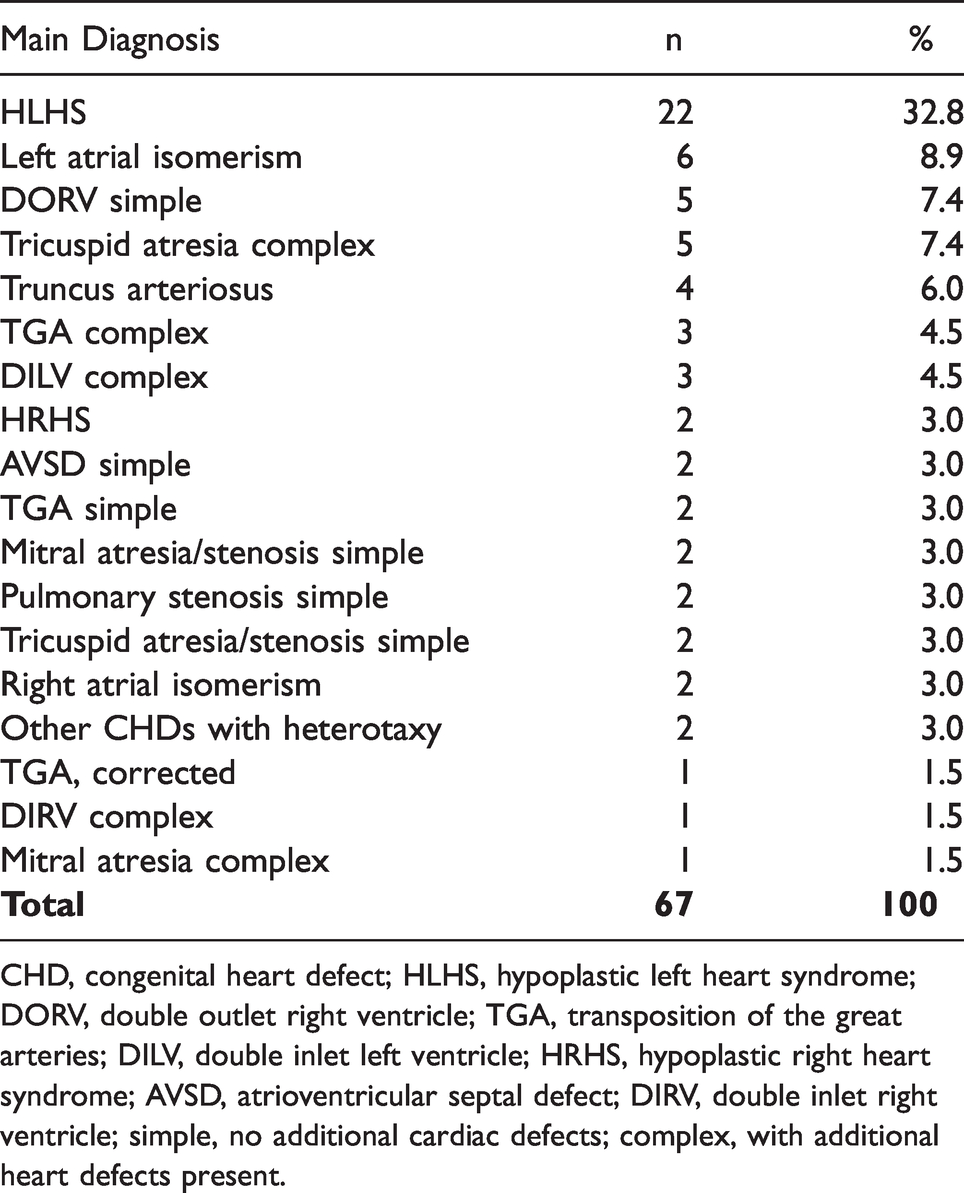
CHD, congenital heart defect; HLHS, hypoplastic left heart syndrome; DORV, double outlet right ventricle; TGA, transposition of the great arteries; DILV, double inlet left ventricle; HRHS, hypoplastic right heart syndrome; AVSD, atrioventricular septal defect; DIRV, double inlet right ventricle; simple, no additional cardiac defects; complex, with additional heart defects present.
Table 3 shows a detailed postmortem distribution of all subdiagnoses of CHDs among the 67 fetuses, altogether 228 CHDs, categorized according to ICD-10. Anomalies of the cardiac chambers and connections (Q20) comprised the largest category, 91/228 (39.9%), including TGA, 17/228 (7.5%) and double outlet right ventricle (DORV), 13/228 (5.7%). Hypoplastic right ventricle and hypoplastic left ventricle were also part of this category, comprising 11/228 (4.8%) and 38/228 (16.6%), respectively. Two of the 11 fetuses with hypoplastic right ventricle had hypoplastic right heart syndrome (HRHS), and 22 of 38 fetuses with hypoplastic left ventricle had HLHS.
Detailed Postmortem Distribution of All Subdiagnoses of CHDs Among the 67 Terminated Pregnancies, According to ICD-10. 9
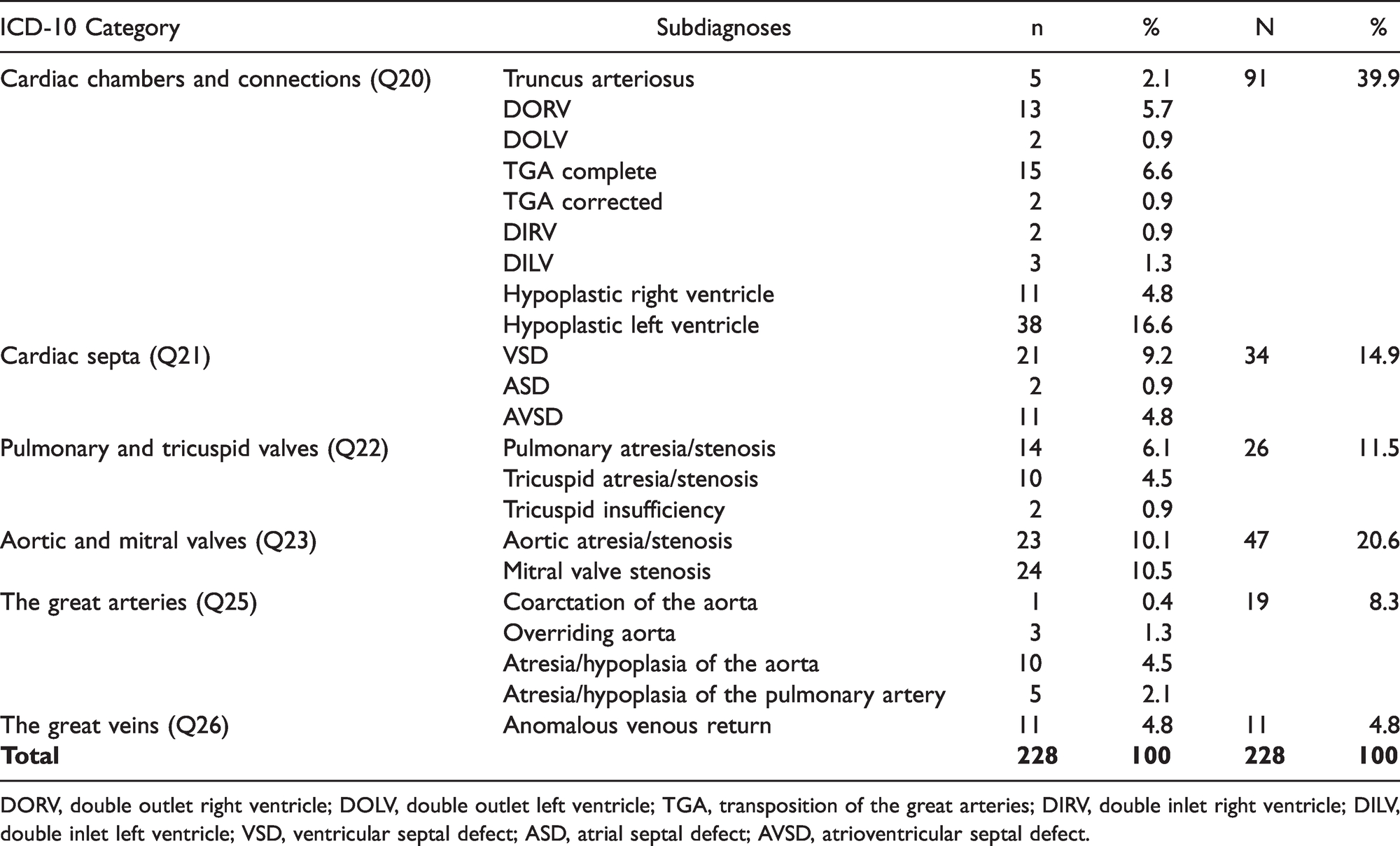
DORV, double outlet right ventricle; DOLV, double outlet left ventricle; TGA, transposition of the great arteries; DIRV, double inlet right ventricle; DILV, double inlet left ventricle; VSD, ventricular septal defect; ASD, atrial septal defect; AVSD, atrioventricular septal defect.
Among the 10 fetuses with heterotaxy syndrome, there were six fetuses with left atrial isomerism (LAI), two fetuses with right atrial isomerism (RAI) and two fetuses defined as “Other CHDs with heterotaxy” (Table 2). Table 4 shows an overview of the 10 cases with heterotaxy syndrome after autopsy examination, including subdiagnoses of the CHDs. In the fetuses with LAI, heart defects such as AVSD, TGA and hemiazygos continuation were common, while both fetuses with RAI had hypoplastic left ventricle and DORV. Overall, five fetuses (50%) with heterotaxy syndrome had hypoplastic left or right ventricle.
Overview of the 10 Cases With Heterotaxy Syndrome After Autopsy Examination, Including Subdiagnoses of the CHDs.
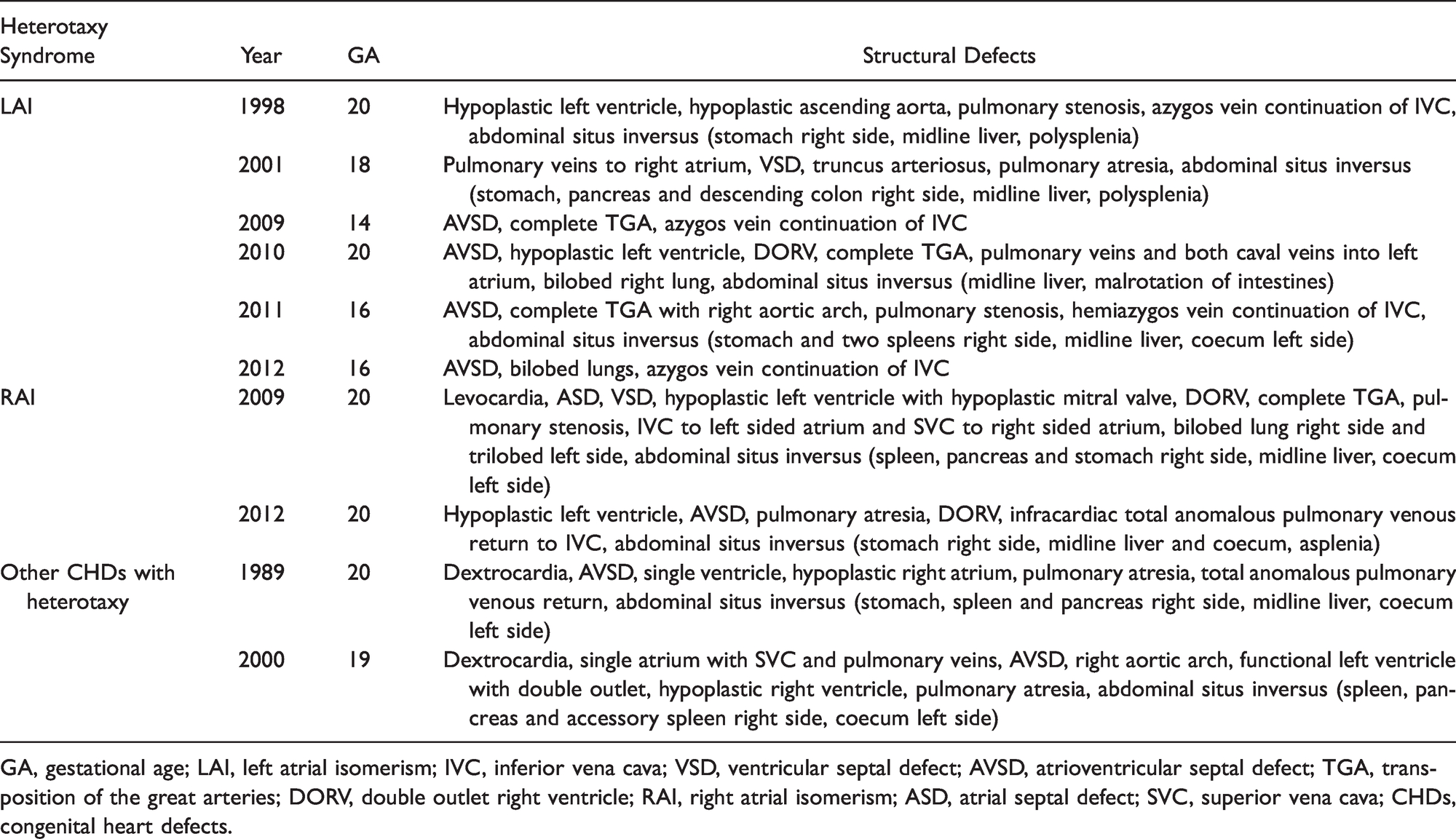
GA, gestational age; LAI, left atrial isomerism; IVC, inferior vena cava; VSD, ventricular septal defect; AVSD, atrioventricular septal defect; TGA, transposition of the great arteries; DORV, double outlet right ventricle; RAI, right atrial isomerism; ASD, atrial septal defect; SVC, superior vena cava; CHDs, congenital heart defects.
Table 5 demonstrates the correlation between prenatal US findings and autopsy findings in all 228 subdiagnoses of the CHDs amongst the 67 fetuses. There was full agreement between US and autopsy findings in 222 of the 228 CHDs (97.4%). The discrepant findings were found in three fetuses (Table 6). In the first fetus from 2004, a VSD was not seen at US (category 2: minor autopsy findings not seen or recorded at US examination) and a suspected truncus arteriosus at US was diagnosed at autopsy as a complete TGA, VSD and left ventricle outflow tract obstruction (LVOTO) (category 3: major autopsy findings not detected at US examination). In the second fetus from 2011, all US findings were verified at autopsy, except DORV (category 5: US findings not confirmed or not possible to confirm at autopsy, false positive). In the third fetus from 2014, prenatal findings were recategorized at autopsy. Overriding aorta and pulmonary artery smaller than aorta at US examination were not confirmed at autopsy (category 5, false positive). Moreover, postmortem findings of aortic stenosis, interrupted aortic arch and left subclavian artery rising from pulmonary artery were not seen at US (category 3: major autopsy findings not detected at US examination) (Table 6).
Correlation Between Prenatal US and Autopsy Findings in All Subdiagnoses of CHDs in 67 Fetuses.
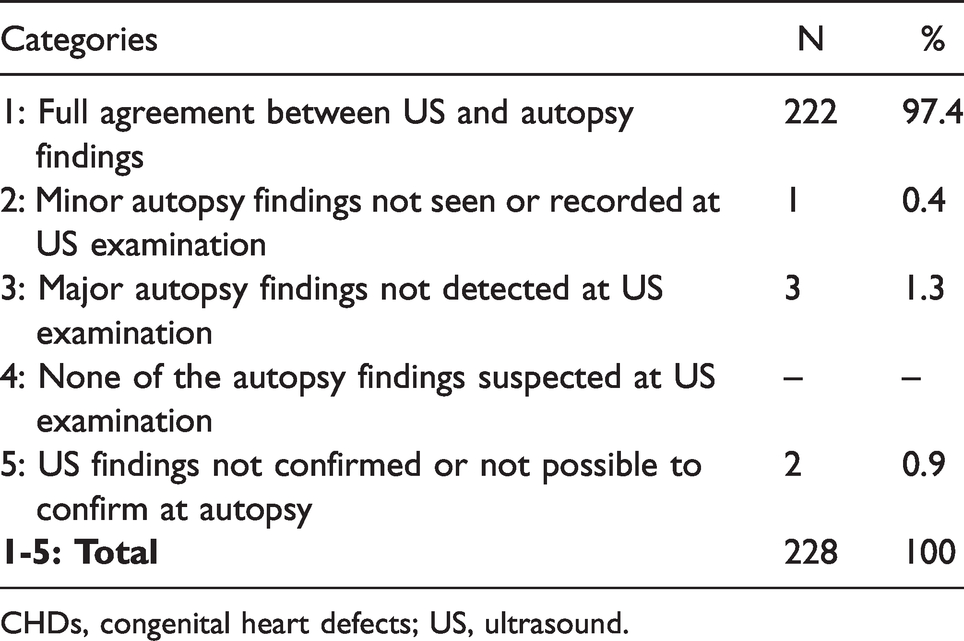
CHDs, congenital heart defects; US, ultrasound.
Cases With Disagreement Between Ultrasound and Postmortem Findings.
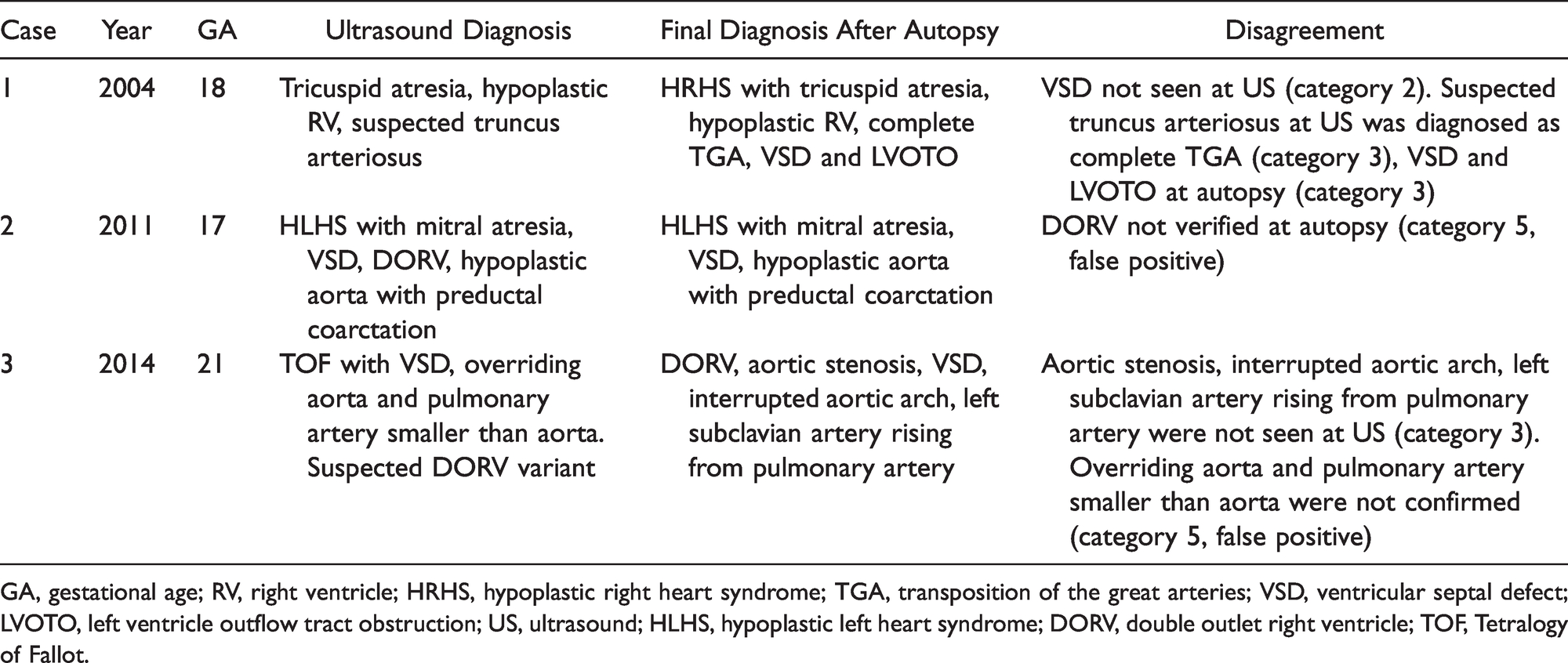
GA, gestational age; RV, right ventricle; HRHS, hypoplastic right heart syndrome; TGA, transposition of the great arteries; VSD, ventricular septal defect; LVOTO, left ventricle outflow tract obstruction; US, ultrasound; HLHS, hypoplastic left heart syndrome; DORV, double outlet right ventricle; TOF, Tetralogy of Fallot.
Discussion
When a pregnancy is terminated due to congenital anomalies detected by US, verification of those findings by autopsy is important.5,13–15 In the present study, there was full agreement between US and autopsy findings in 97.4% of 228 subdiagnoses of the CHDs among 67 fetuses. Previous studies addressing the correlation between US findings and verification at autopsy have addressed multiple organ groups,4,5,16–18 or included all cases with cardiac pathology, irrespective of the main cause of death.19–21 We are not aware of other studies comparing prenatal US and postmortem findings in pregnancies terminated due to isolated CHDs or CHDs associated with heterotaxy syndrome. It is therefore difficult to compare our correlation rates with other studies.
If the cardiac diagnosis is a false positive finding when other lethal or serious extracardiac anomalies are present, the false positive diagnosis will not determine the management of the pregnancy in the same way as if the termination is performed based on a false positive isolated major CHD only.4,5,13,14 In cases with isolated CHDs, high agreement is especially important as there are no other associated organ anomalies that would justify TOP.
The fetal heart is considered the most challenging organ to examine prenatally. 8 In a non-selected population, 51% of the CHDs will be isolated; this emphasizes the necessity of a verification of the prenatal diagnosis. 8 To validate the quality of the US examinations, we chose to divide each major CHD into subdiagnoses as these constitute the main diagnosis and may also be important for the prognosis. Despite the false positive subdiagnosis (category 5) in two cases in our study, both had other serious subdiagnoses confirmed at autopsy, thus management had not been affected by the false positive subdiagnoses. The false positives illustrate the complexity of isolated CHDs.
One factor for the high correlation in our study may be a result of improved detection of minor CHDs. Traditionally, conditions with hypoplastic heart chambers and large VSDs and AVSDs have been easier to detect than minor VSDs and atrial septal defects.22–24 Even though minor anomalies do not change the management of the pregnancy with regard to TOP, detecting these minor findings is important as they may indicate the presence of a more serious anomaly and are essential in evaluating the severity of the CHD.5,13 Another factor that may contribute to the high correlation rate in our study, is that all 67 fetuses were intact after medical abortion and were not macerated or traumatized prior to verification at autopsy.
HLHS was the most common main diagnosis among all pregnancies terminated due to isolated CHDs and was found in 22 of the 67 fetuses (Table 2). It is considered a serious or lethal condition constituting 1–2% of all major CHDs, 25 and generally occurs in children without other anomalies. 26 Previous studies have reported TOP in 60–80% of cases in which HLHS was detected prenatally.25,27 In antenatally diagnosed cases, detailed parental counseling is important, with a discussion of options of termination or continuation of pregnancy, including the choice of postnatal interventions such as compassionate care and cardiac surgery.28,29
Anomalies of the aortic and mitral valves (Q23) together with anomalies of cardiac chambers and connections (Q20) comprised 60% of all 228 subdiagnoses of CHD (Table 3). Cardiac septal defects (Q21) are traditionally the most common CHDs, but in our study they constituted only 14.9%. This finding correlates with the literature, where most septal defects in autopsy populations are related to abnormal karyotype;30,31 such cases were excluded from the present study.
All CHDs in the 10 cases with heterotaxy syndrome (Table 4) were major anomalies. CHD is an important component of heterotaxy syndrome, resulting in significant mortality. 32 However, the prognosis of patients with heterotaxy varies, as they represent a heterogeneous group, and surgery is often complex. 33 In these cases, the choice leading to termination of pregnancy was based on findings of serious/lethal CHDs while the abnormal arrangement of organs was of subordinate importance when deciding to terminate the pregnancy. However, when heterotaxy is suspected during prenatal examination, further search for other anomalies, including CHDs, is necessary.
The complexities of CHDs emphasize the necessity of a referral center with specialists in fetal medicine. 34 Collaboration with a pediatric cardiologist is of great value, particularly when there are no associated anomalies. 35 In Table 6, which shows the disagreement between US and postmortem findings, it should be noted that in addition to fetal medicine specialists, a pediatric cardiologist evaluated cases 2 and 3, but not case 1. When the fetal medicine specialist was not sure about the details in the cardiac diagnosis, the prenatal findings were defined as “suspected” (Table 6). The broad range of CHDs without associated anomalies is challenging for the prenatal detection of CHDs, also when the heart is evaluated in detail by experts in fetal medicine and pediatric cardiologists. Moreover, classifications and categorizations of CHDs have evolved during the last decades, resulting in differences in terminology.
Fetal autopsy is not mandatory in Norway, but the involved parents are informed about the value of autopsy and the importance of quality control in diagnosing and verifying congenital anomalies detected at US prior to termination of pregnancy. To terminate a pregnancy is a difficult decision for the parents and a verification of the prenatal findings may ease their grief. 36 The information parents gain can be a positive confirmation of the choice they have made and may also provide them with additional knowledge of recurrence in a future pregnancy. 37 Such verification is also essential for clinicians in order to provide proper counselling. Despite the high correlation between the prenatal findings and the autopsy findings in our study, we still believe an autopsy is of value. However, an autopsy is not an option in all cases, and it is then reassuring to be aware of the high expertise of the fetal medical examiner.
Even though studies have shown that autopsy helps to establish the cause of death and can provide additional clinically significant information, autopsy rates are falling in the western world.37–39 Dislike for the invasiveness of traditional autopsy and cultural and religious beliefs have been raised as possible causes leading to falling autopsy rates. 40 However, alternatives to traditional invasive postmortem examination of congenital anomalies have been developed that include less-invasive methods and a variety of imaging modalities, that may alleviate this falling trend. 41 Postmortem magnetic resonance imaging has shown promising results in general, including fetal hearts.40,42,43 Micro-focus CT imaging with virtual dissection of the fetal heart may become a good alternative to conventional autopsy; 44 postmortem two-dimensional US may also be an alternative to invasive autopsy, although the results for the fetal heart still need to be improved. 45
During the last decade there has been a move towards the use of US in the first trimester.46,47 This has led to detection of congenital anomalies and, in selected cases, TOP at an earlier gestational age, making the verification of anomalies at autopsy difficult. The autopsy verification is particularly challenging when CHDs are the only prenatal finding leading to TOP. Opening the heart in situ and dissection with a stereomicroscope improves the visualization at autopsy 3 and requires an experienced perinatal pathologist. Postmortem imaging methods may be of particular help for the smaller fetuses. By performing medical abortion, the fetus is kept intact which makes the valuable verification at autopsy by a perinatal pathologist possible.
Conclusively, in this autopsy material of 67 fetuses with isolated CHDs, detailed prenatal assessment and postmortem examination revealed 228 subdiagnoses of CHDs, with 97.4% full agreement between prenatal US and autopsy findings. The two false positive subdiagnoses did not affect the basis for the TOP. Even though our study demonstrates a high degree of correct prenatal cardiac assessment, we cannot ignore the serious consequences of a misdiagnosis, especially when the decision to terminate a pregnancy is based on abnormalities in one organ only. We believe it is important to inform the parents of the option of autopsy given the benefit reassurance might represent for the couple. However, an autopsy is not an option in all cases, and we appreciate the expertise of fetal medicine specialists performing prenatal examinations with high accuracy. Consequently, the fetus should be examined at a tertiary medical center with fetal medicine specialists in collaboration with a pediatric cardiologist and an experienced perinatal pathologist.
Footnotes
Acknowledgment
Nancy Lea Eik-Nes revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.