
Abstract
Background
The observation of fat accumulation in different organs at pediatric autopsy may help determine the cause of death. However, a comprehensive study on fat accumulation and related etiologies is still lacking.
Aim
To investigate the incidence of fat accumulation in different organs in pediatric autopsies and their relevance to the cause of death.
Methods
From February 2004 until March 2015, fat accumulation was assessed in 561 routinely performed pediatric autopsies in our center. Age at death ranged from 14 weeks of gestation for fetuses to 16 years. Samples of liver, heart, kidney, and muscle were stained with Oil-Red-O and scored for fat accumulation by one pediatric pathologist.
Results
Fat accumulation in ≥1 organ(s) was present in 132 (39.8%) of 332 prenatal cases. Only 3 (0.9%) had fat accumulation in all 4 organs. For postnatal cases, fat accumulation in ≥1 organ(s) was present in 106 (46.3%) of 229 postnatal cases. Only 12 (5.2%) had fat accumulation in all 4 organs. Fat accumulation was mostly seen in liver, both in prenatal and postnatal cases. Fatty acid oxidation disorders were the only cause of death associated with severe fat accumulation in all 4 organs. No other etiologies could be linked directly to distribution or severity of fat accumulation.
Conclusion
Severe fat accumulation in at least 4 organs is a rare finding in pediatric autopsies, whereas fat accumulation in only the liver is relatively common. Severe fat accumulation in both liver, muscle, kidney, and heart was only seen in cases with fatty acid oxidation disorders.
Introduction
Fat accumulation in parenchymal cells reflects an impairment of the transport and elimination of fat. Since the liver has a crucial role in whole body fat homeostasis, fat accumulation is predominantly observed in liver (steatosis). Common causes of fat accumulation in liver include alcohol consumption, obesity, toxins/medication, viral infections, inborn errors of metabolism, parenteral nutrition, protein malnutrition, diabetes mellitus, anoxia, and pregnancy.1–3 Autopsy studies4,5 have reported a prevalence of hepatic fat accumulation in children and young adults of 5.3% to 9.6%. A significant difference between ethnic groups is observed, and obesity is the most important risk factor.
Fat accumulation may also occur in kidney, heart, and skeletal muscle, but data on prevalence are limited with only one autopsy study reporting cardiac fat accumulation in 7% of all pediatric autopsies. 6 Factors that were associated with fat accumulation in kidney, heart, and skeletal muscle during autopsy studies are hypoxia, inherited metabolic disease, congenital heart disease, and infection.7–10
The distribution pattern of fat accumulation in liver and other organs may help determine the cause of death. Therefore, we investigated the occurrence of fat accumulation in different organs in a large series of pediatric autopsies and combined the data with the cause of death.
Methods
Patients
Between March 2004 and February 2015, 618 pediatric autopsies were routinely performed in one referral center (Department of Pathology, University Medical Center Utrecht). Autopsies included both prenatal and postnatal cases, with an age range from 14 weeks of gestation for fetuses to 16 years of age. Pregnancies were either terminated because of multiple congenital anomalies or due to unexpected intra uterine fetal death. In The Netherlands, legal termination of pregnancy is allowed up to 24 weeks of gestation.
For postnatal cases, the most common indication to perform an autopsy was sudden unexpected death in infancy (SUDI). In our cohort, all cases with a suspicion of nonnatural death, or homicide, were excluded, since these are carried out by the National Forensic Institute in The Netherlands. However, cases of unexpected and unexplained death without suspicion of homicide were included. If new findings during the autopsy procedure lead to suspicion of a nonnatural cause of death, the case was immediately handed over to the National Forensic Institute and excluded from this study. Our cohort included hospitalized children as well as children who died unexpectedly outside the hospital. Histologic data on fat accumulation in different tissues combined with age and cause of death were recorded anonymously and analyzed retrospectively.
Histologic Findings
Fat Accumulation Score.

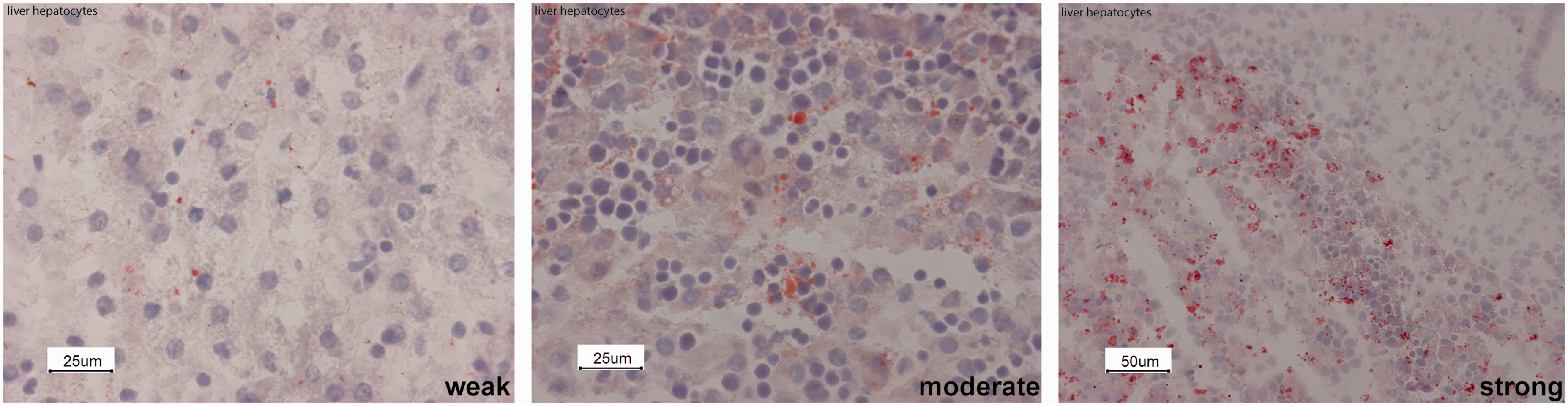
Fat accumulation score in liver hepatocytes.
Statistical Analysis
SPSS Statistical Software version 23 (IBM corp., Armonk, NY, USA) was used for descriptive analysis. The Mann–Whitney U test was used to compare mean gestational age at death for the prenatal cases and mean age at death for postnatal cases. A chi-square test was used to determine differences in gender and diagnoses. A P value < .05 was considered statistically significant.
Ethics
Parental consent including use of anonymous material and data for research was given in all cases.
Results
Prenatal Cases
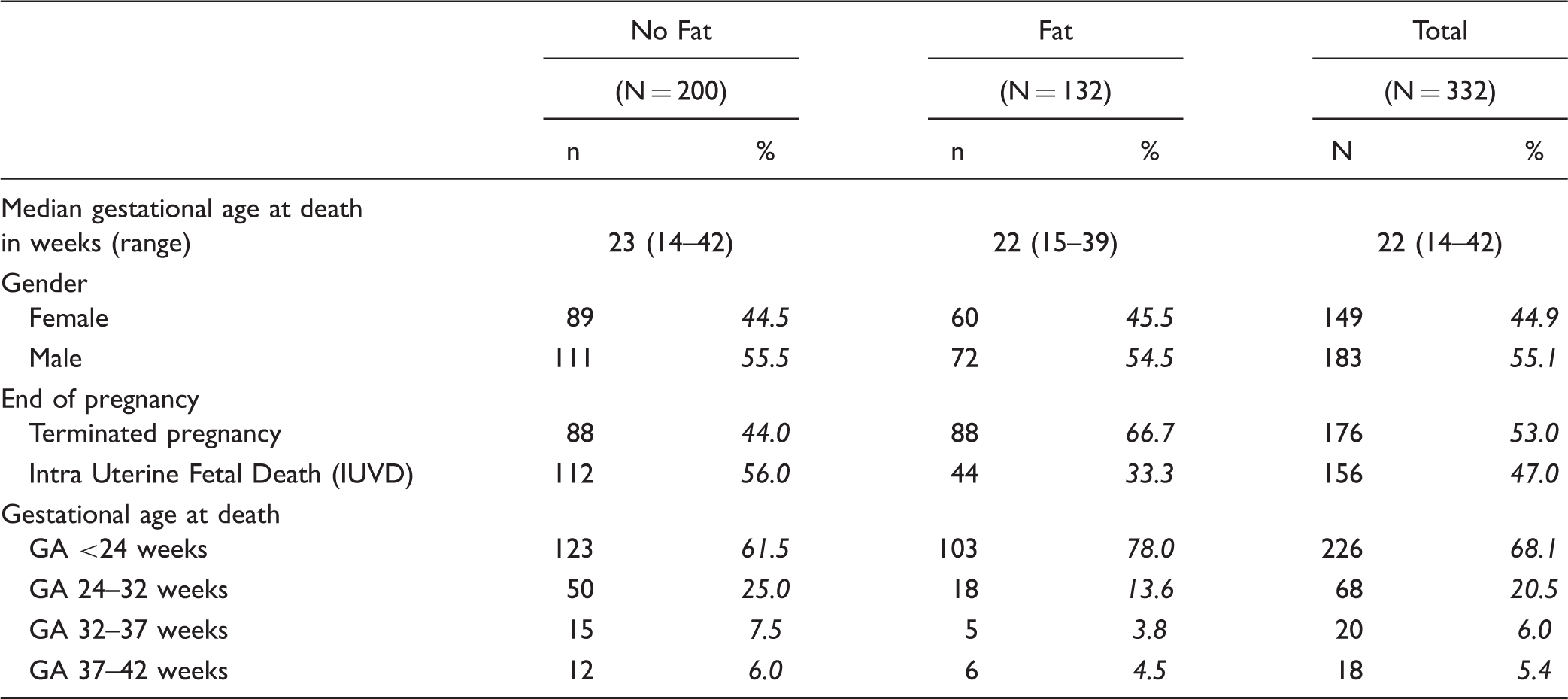
Of the 618 cases included in this study, 371 (60%) were prenatal. In 39 of them, information on fat accumulation in one or more organs was missing and they were excluded from the analysis (Figure 2). Table 2 shows characteristics of the remaining 332 prenatal cases. In total, there were 149 (44.9%) female cases, compared to 183 (55.1%) males. The pregnancy was terminated in 176 (53%) cases, following abnormal results found during prenatal diagnostics, either by genetic analysis or by ultrasound. The other 156 (47%) autopsies were done following intra uterine fetal death. Gestational age at death ranged from 14 weeks until 42 weeks with a median of 22 weeks.
Overview of autopsy cases. Prenatal Cases.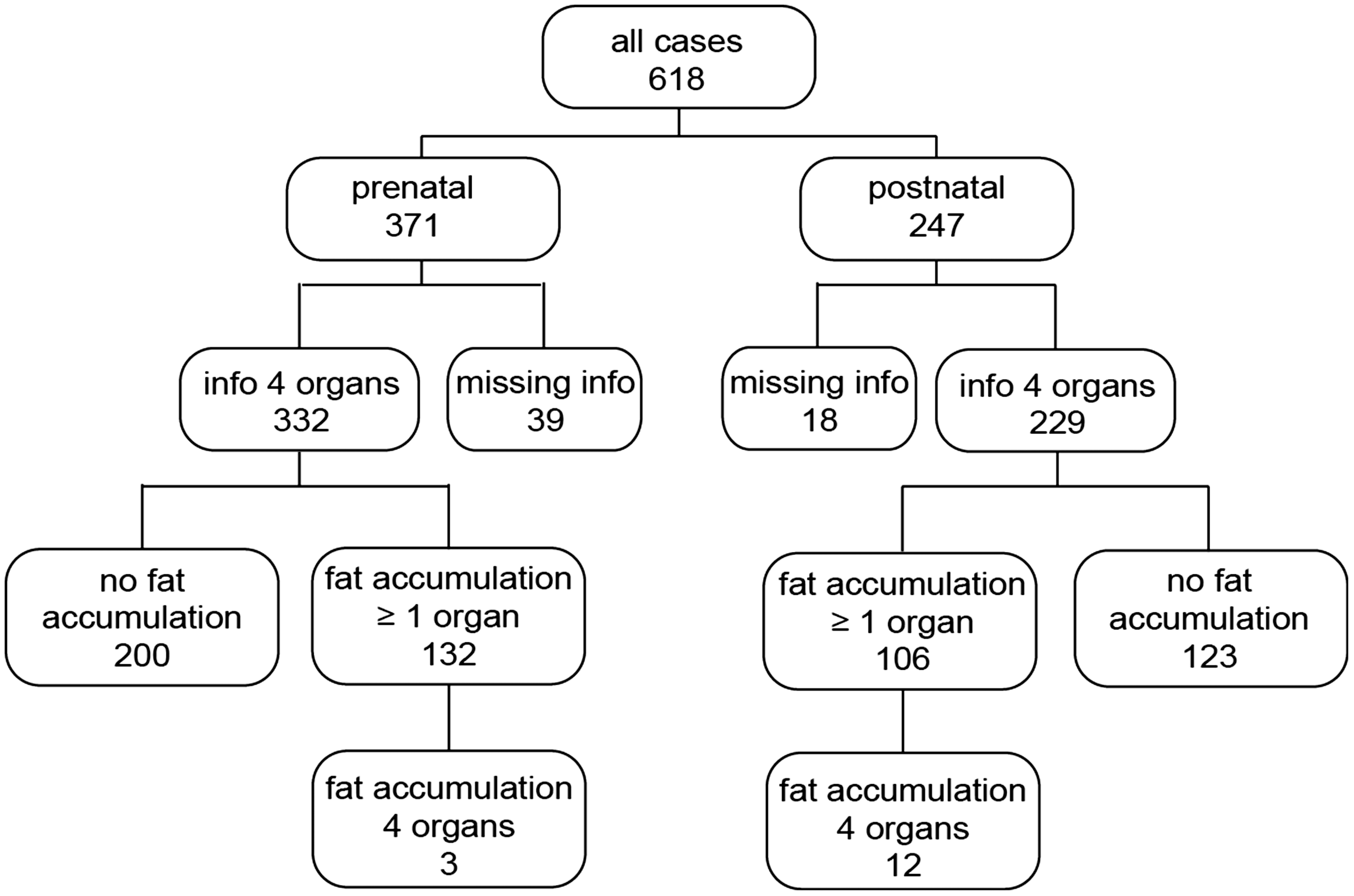
Fat accumulation
Of the 332 prenatal cases, 132 (39.8%) had fat accumulation in one or more organs. There was no significant difference in gender distribution compared to the 200 prenatal cases without fat accumulation. However, mean gestational age at death was significantly lower in the presence of fat accumulation (22 vs 23 weeks, P = .04).
Fat accumulation was predominantly seen in liver hepatocytes. Only 5 cases (1.5%) showed fat accumulation in kidney (proximal tubules), muscle, or both without fat accumulation in liver (Figure 3). Fat accumulation in the heart was not seen without liver involvement.
Prenatal fat accumulation per organ.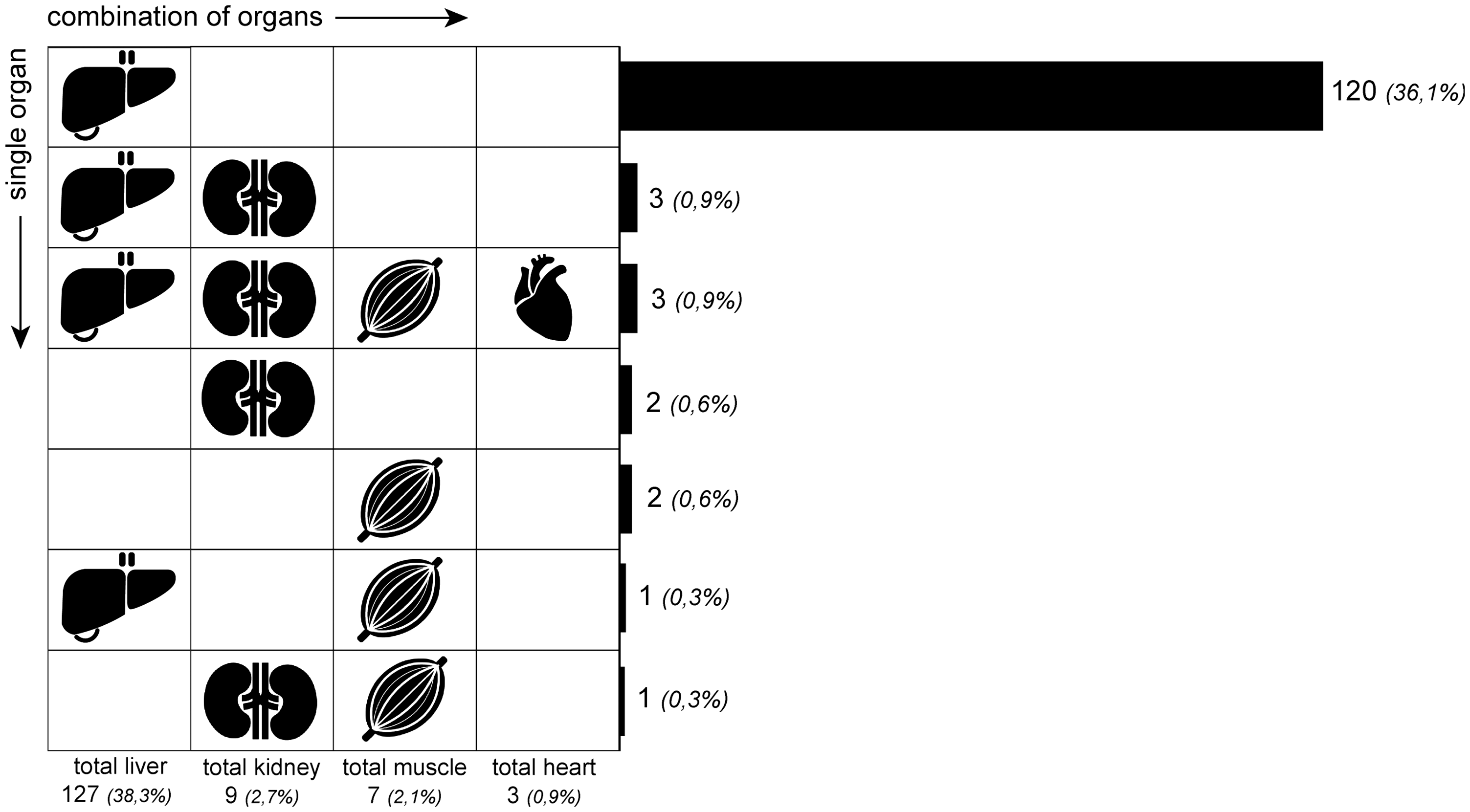
Prenatal Cases With Fat Accumulation in 4 Organs.
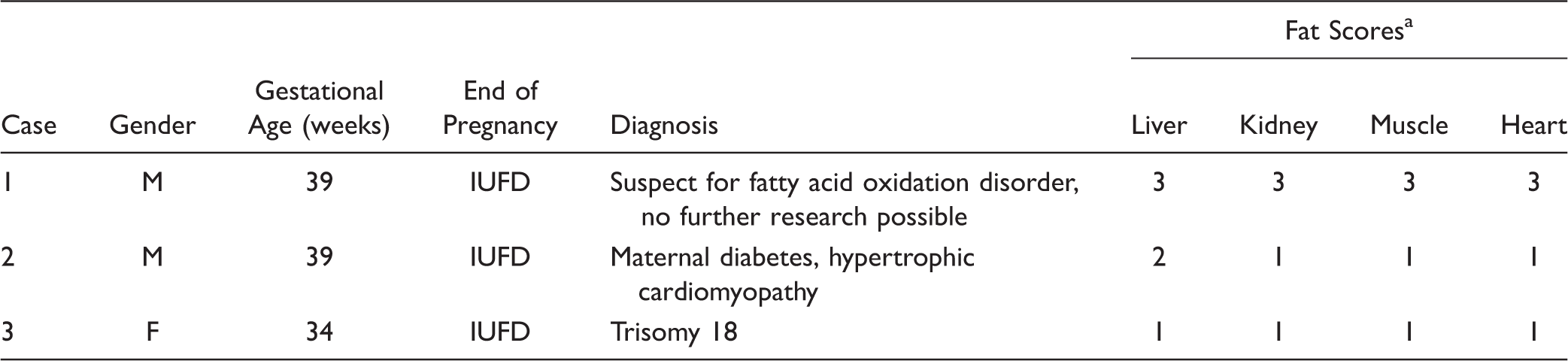
IUFD = intra uterine fetal death.
a1 = weak; 2 = moderate; 3 = strong.
Asphyxia, congenital heart disease, and severe infection were found equally frequent in the group without as in the group with fat accumulation.
Postnatal Cases
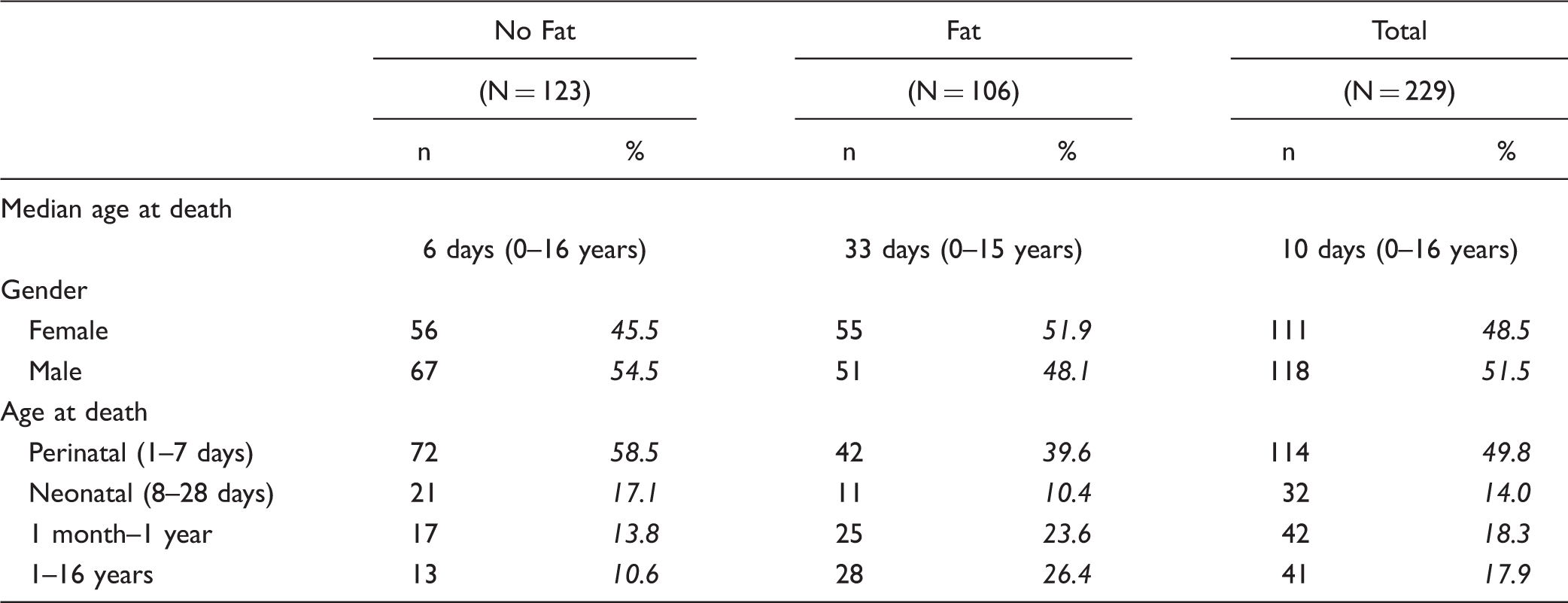
Postnatal Cases.
Fat accumulation
Of the remaining 229 postnatal cases, 106 (46.3%) had fat accumulation in one or more organs. There was no significant difference in gender distribution compared to the 123 cases without fat accumulation. However, median age in the group with fat accumulation was significantly higher compared to the group without fat accumulation (33 days vs 6 days, P = .02).
Hepatic fat accumulation was seen in 99 (43.2%) postnatal cases (Figure 4). In one third of this group, hepatic fat accumulation was accompanied by involvement of other organs. Four cases showed fat accumulation only in kidney and in 2 cases, fat accumulation was only found in skeletal muscle. Similar to the prenatal group, fat accumulation in the heart was only seen in combination with fat accumulation in other organs. Eighteen cases showed fat accumulation of both liver and kidney without involvement of other organs. The combination of fat accumulation in liver and muscle or muscle and kidney was rare with only 2 cases and 1 case, respectively.
Postnatal fat accumulation per organ.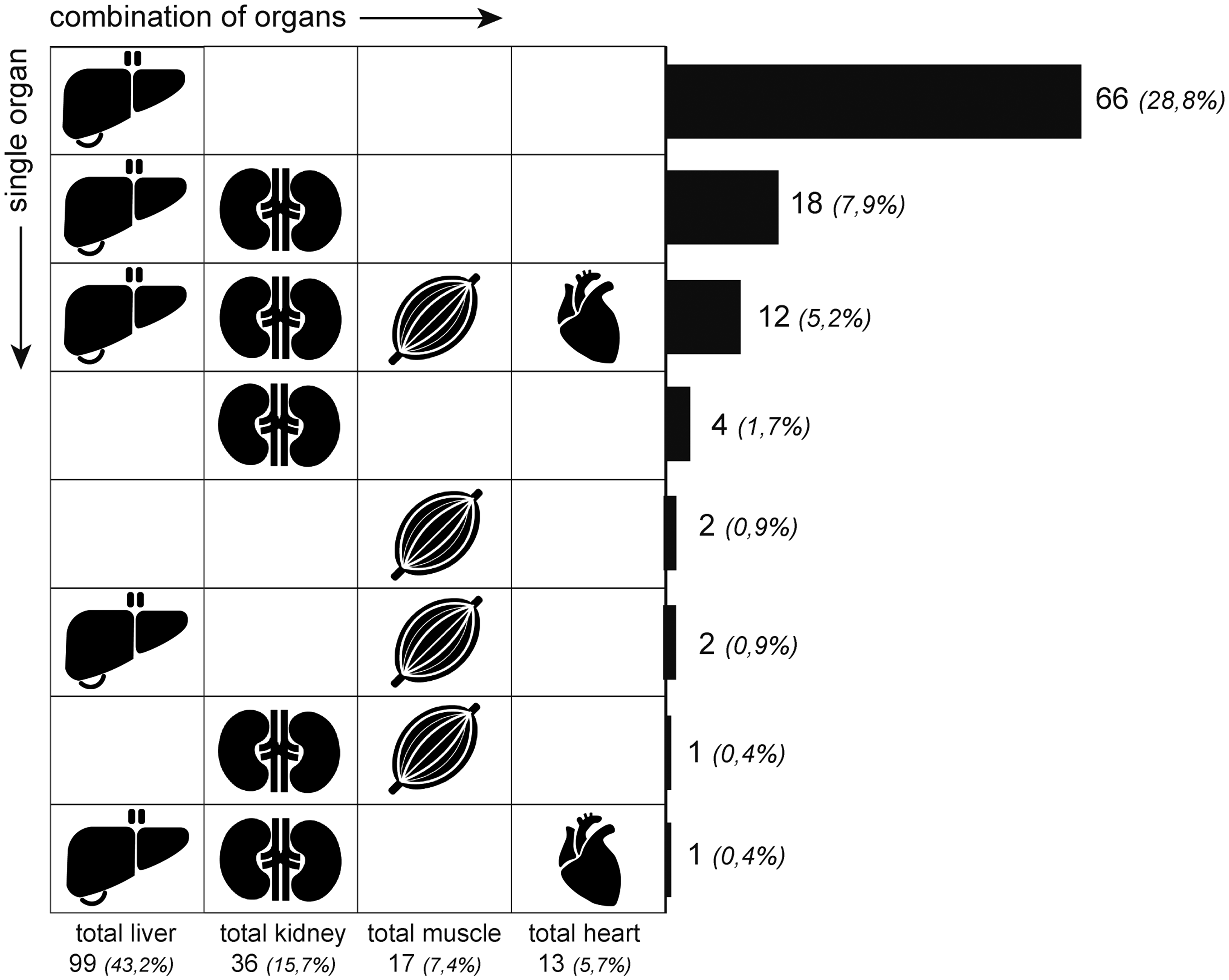
Postnatal Cases With Fat Accumulation in All 4 Organs.
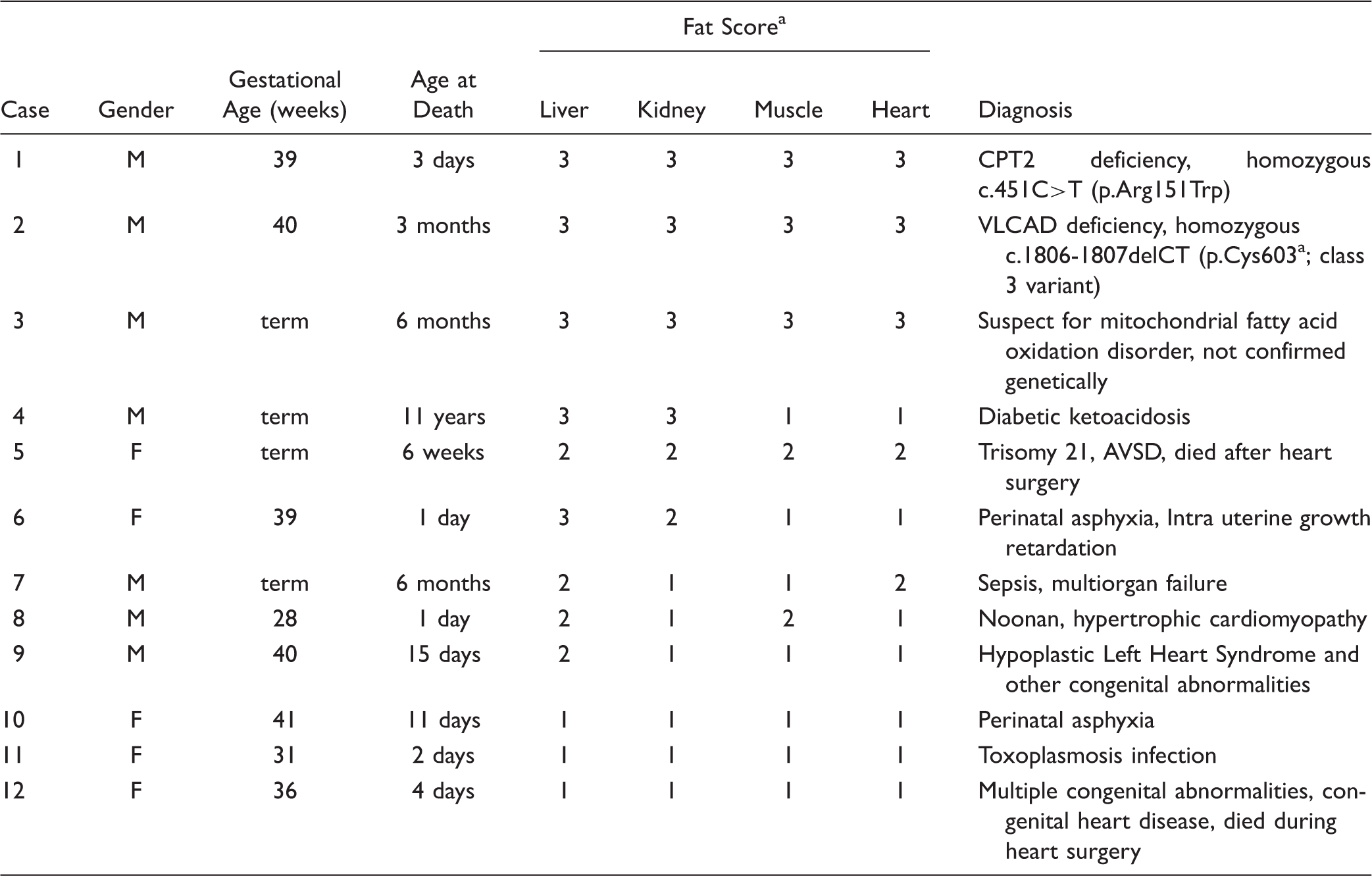
a1 = weak; 2 = moderate; 3 = strong.
Discussion
This study demonstrates that fat accumulation in multiple organs (liver [hepatocytes], heart, kidney [proximal tubules], and muscle) is a rare finding in pre- and postnatal pediatric autopsies. Furthermore, we show that in our cohort, severe fat accumulation in all 4 organs was often found in combination with inherited disorders of mitochondrial fatty acid oxidation.
Little is known about distribution of fat accumulation in multiple organs on autopsy studies, and fat accumulation is usually reported only in liver. In our study, hepatic fat accumulation was present in 38.3% of prenatal cases and in 43.2% of the postnatal cases. This is considerably more than the prevalence reported in previous studies on pediatric autopsies.4,5 However, these studies selected a population-based group, consisting of children who died due to trauma or unknown origin. Cases that had been hospitalized prior to death, or died from known pathology, were excluded. In our center, no autopsies are performed on children who died with a suspicion of nonnatural death or homicide, since these are carried out by the National Forensic Institute in The Netherlands. However, cases of unexpected and unexplained death without suspicion of homicide were included in this cohort. Our cohort included both hospitalized children as well as children who died unexpectedly outside the hospital. These differences in study population could contribute to the observed differences with previous studies.
After the liver, fat accumulation was most frequently found in kidney. Fat accumulation in the kidney was seen in 2.7% of the prenatal cases and 15.7% of the postnatal cases and in the heart in 0.9% of the prenatal cases and 5.7% of all postnatal cases. Strikingly, fat accumulation in the heart was only observed in combination with fat accumulation in liver, kidney, and muscle. As reported earlier, myocardial fat accumulation is uncommon in children and is associated with infection, metabolic disease, and hypoxia.6,7 The impact of hypoxia caused by myocardial infarction on fat accumulation has been studied extensively in autopsy studies and various animal models. Duration of the hypoxia is closely related to the severity of fat accumulation in the myocardium,7,11 as a result of decreased mitochondrial fatty acid oxidation and increased triglyceride synthesis in this tissue due to the hypoxia.12–15 This mechanism may also play a role in myocardial fat accumulation observed in congenital heart disease, as the increased working load on the heart will lead to an increased demand on β-oxidation activity which cannot be met by the supply of oxygen. 7 Insulin resistance is also associated with cardiac fat accumulation, but there are only very limited data on its prevalence in children. 16 In adults, Nakanishi et al. 17 found myocardial fat accumulation in 9.5% of 72 studied autopsy cases, all of which were diagnosed with diabetes mellitus.
Relatively little is known about prenatal fat accumulation. Oey et al. 18 showed that the enzymes involved in mitochondrial fatty acid oxidation are already expressed in fetal tissues and fatty acids do play an important role in fetal development. 19 Two out of the three prenatal cases with fat accumulation in all 4 organs suffered from severe hypoxia and sepsis. Although hypoxia and sepsis are known causes for fat accumulation, these causes of death were found equally frequent in the group without fat accumulation. Maternal factors can also influence the lipid metabolism of the fetus. Patel et al. 20 showed a clear correlation between fat accumulation in liver of stillborn fetuses of mothers with diabetes mellitus. Brumbaugh et al. 21 confirmed this finding in newborns. We also found one prenatal case with severe fat accumulation in liver and mild fat accumulation in kidney, heart, and muscle of a mother with diabetes mellitus (Table 5).
FAODs are a known cause of SUDI.22–24 Although an increasing number of newborn screening programs worldwide includes disorders of mitochondrial fatty acid oxidation, there are still patients who may die before screening is performed, and it is not uncommon that the diagnosis is made based on the results of postmortem investigations. 25 Several studies show that most SUDI caused by FAOD occurred in the first week of life. 26 This was also the case in one of the FAOD cases in our cohort. The other case with confirmed FAOD was born before introduction of FAODs to the Dutch newborn screening program.
It is likely that the number of cases that died of FAODs in our cohort is an underestimation. Metabolic derangement is often triggered by another illness; therefore, it is possible that this illness, for example a viral infection, is stated as cause of death and without further metabolic investigation. In all cases diagnosed with FAOD, we found severe fat accumulation in all studied organs, but mild and moderate fat accumulation in less than 4 organs are also described in literature. For a comprehensive overview of histopathological features of FAODs reported in literature, see Supplementary Table S1.
In conclusion, the combination of severe fat accumulation in liver, as well as kidney, heart, and skeletal muscle is very rare in pediatric autopsies. In our study, mitochondrial FAODs were most often the cause of severe fat accumulation in multiple organs. When severe fat accumulation is found in multiple organs, further investigations including genetic and metabolic analysis are advisable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplements for this article are available online.