
Abstract
Introduction:
Laparoscopic gastrostomy (LG) tube placement is a minimally invasive technique increasingly used in pediatric patients requiring long-term enteral nutrition. While various approaches exist, technique standardization remains limited. This study aims to describe our institution’s standardized LG technique and evaluate its surgical outcomes.
Methods:
We conducted a retrospective review of pediatric patients who underwent LG tube placement at a tertiary care center between August 2017 and September 2022. All procedures were performed using a uniform laparoscopic technique involving a purse-string suture and multiple fascial anchoring sutures. Clinical and perioperative data, including patient demographics, operative time, and time to first feed, were analyzed. Statistical analyses included Spearman correlation and Mann–Whitney U tests.
Results:
Twenty-five patients (56% female) with a median age of 48 months (range: 7–204 months) underwent LG placement. Neurological impairment was present in 76% of cases. The median operative time was 71 minutes, and the median time to first feed was within the same postoperative day. Notably, no patients experienced intraoperative or postoperative complications. There were no conversions to open surgery, no aborted procedures, and no requirement for postoperative anti-reflux surgery. Mann–Whitney U analysis showed no statistically significant differences in operative time or time to first feed based on neurological status (P = .086 and P = .568, respectively).
Conclusion:
Our standardized LG technique is safe, reproducible, and effective, with no complications and favorable outcomes across pediatric subgroups. This approach may offer a reliable alternative to percutaneous endoscopic gastrostomy or open gastrostomy placement in children.
Introduction
Gastrostomy tube (GT) placement is an essential intervention in pediatric patients who are unable to meet their nutritional requirements through oral feeding. Indications for GT insertion include a wide range of medical conditions, such as failure to thrive, neurodevelopmental delays, congenital anomalies, and metabolic disorders. These patients often require long-term enteral feeding to prevent malnutrition and support growth and development. Gastrostomy feeding is generally preferred over nasogastric (NG) tube feeding when nutritional support is expected to exceed 3–6 months. 1
However, while GT placement provides a critical means of ensuring adequate nutrition, it is not without complications. Common complications associated with GTs include gastroesophageal reflux disease, hypergranulation tissue formation, leakage of gastric contents, wound infections, accidental dislodgement of the tube, and in rare cases, injury to adjacent organs necessitating re-intervention.1,2 Although many of these complications are not life-threatening, they contribute to significant morbidity and increase health care utilization and costs. Therefore, the choice of technique for GT insertion should aim to minimize these risks while ensuring effective and safe placement.
Several techniques have been described for GT insertion, each with specific advantages and disadvantages. The traditional open Stamm gastrostomy involves a formal laparotomy with direct access to the stomach, allowing secure placement of the tube under direct visualization. While reliable, this method is more invasive, requiring a large incision, prolonged recovery, and increased postoperative pain. Alternatively, percutaneous endoscopic gastrostomy (PEG) is a less invasive option that uses endoscopic guidance to facilitate tube insertion. Despite its minimally invasive nature, PEG carries notable risks, including inadvertent bowel perforation, creation of entero-enteric fistulas, and significant complications in patients with complex abdominal anatomy or prior surgeries. The major complication rate of PEG insertion is reported to be as high as 11%.3,4
In contrast, minimally invasive laparoscopic gastrostomy (LG) has gained increasing favor in the pediatric population due to its unique advantages. Laparoscopic placement allows for direct visualization of the stomach and surrounding structures, reducing the risk of injury to adjacent organs. It also facilitates optimal tube positioning and offers a safe alternative in patients with hostile abdomens or altered anatomy. Furthermore, LG is associated with shorter hospital stays, faster recovery, and earlier initiation of feeding, often on the same day as the procedure.2,4
Various LG techniques have been described in the literature, which can broadly be divided into two main approaches: the Seldinger technique and the mini-open technique (MOT).1,3 The Seldinger technique typically involves puncture of the stomach under laparoscopic guidance, followed by guidewire insertion, dilation, and tube placement—a method that is relatively simple but may carry a higher risk of dislodgement in some patients. On the contrary, the MOT involves direct suturing of the stomach to the abdominal wall, creating a more secure gastropexy and reducing the risk of leakage and dislodgement. Each technique has its proponents, and the choice often depends on surgeon preference, patient-specific factors, and institutional protocols.
At our tertiary care center, we have developed and standardized a specific technique for LG tube placement that we have successfully applied in a series of pediatric patients. The aim of this case series is to describe in detail our operative technique, report on clinical outcomes, and compare our experience to what is reported in the current literature. By sharing our method and outcomes, we hope to contribute to the ongoing efforts to optimize GT placement in children and improve patient care.
Our adopted technique is a variation of the mini-open approach, designed to be simple, reproducible, and safe. The procedure begins by defining and marking the gastrostomy site in the epigastric region, aligned with the left rectus muscle. An umbilical incision is used to introduce a 5 mm trocar under direct vision, with insufflation of the abdomen using CO2. A 5 mm 30-degree laparoscope is then inserted to inspect the abdomen. The stomach is identified and insufflated with approximately 15 mL of air via an NG tube, confirming its location. A stab incision is made at the predetermined gastrostomy site under direct visualization. Using an atraumatic grasper, the stomach is brought to the abdominal wall without tension. A figure-of-eight suture is applied for traction. Four 3-0 absorbable sutures are passed through the fascia to secure the stomach. A purse-string suture is then placed on the anterior gastric wall, and an enterotomy is created at its center using electrocautery. A GT of desired caliber is inserted, and the balloon is inflated with 5–10 mL of sterile water based on the manufacturer’s recommendations. The purse-string suture is tied snugly around the tube, ensuring a tight seal. After confirming the position of the tube and secure gastropexy laparoscopically, the abdomen is deflated, and additional fascial sutures are placed to anchor the stomach to the abdominal wall (Figs. 1–4).
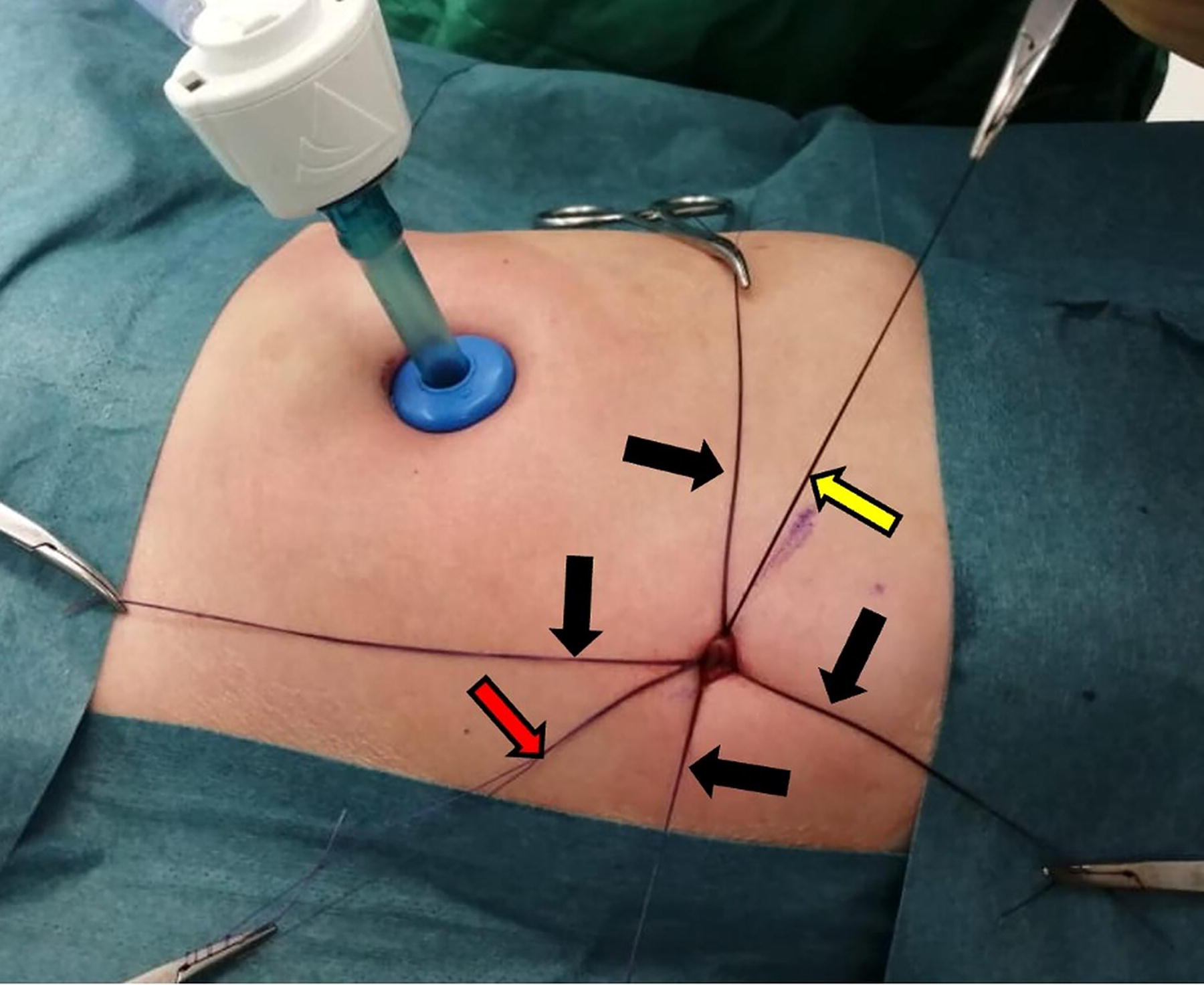
External view of the abdomen showing the 5 mm trocar placed through the umbilical incision. The yellow arrow indicates the figure-of-eight suture applied to provide traction on the stomach. The red arrow highlights the purse-string suture placed on the anterior gastric wall in preparation for gastrostomy tube insertion. The black arrows point to the four 3-0 absorbable sutures that are passed through the fascial layer to anchor the stomach to the abdominal wall.
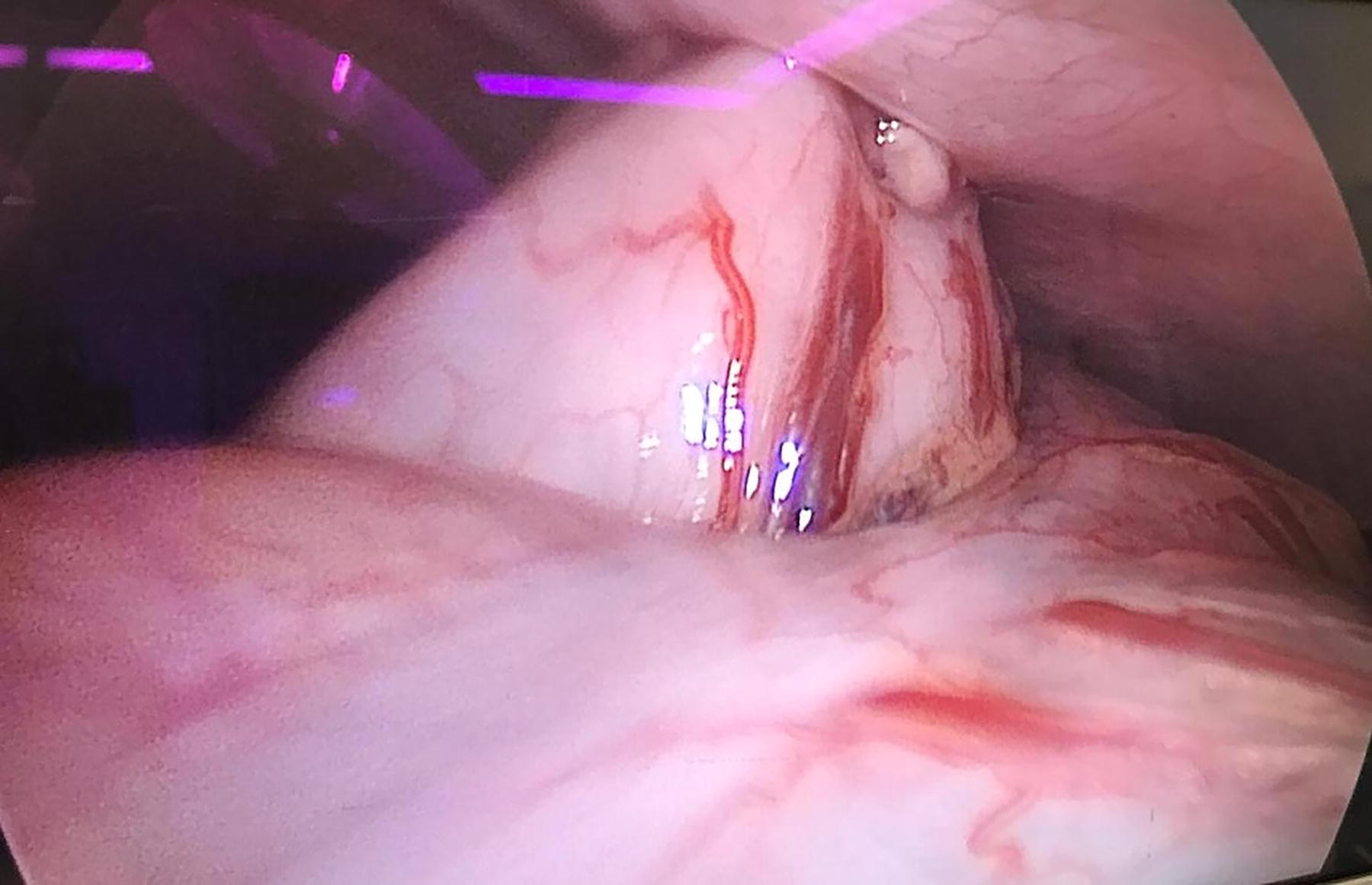
The stomach is visualized laparoscopically as it is gently elevated and approximated to the anterior abdominal wall using an atraumatic grasper.
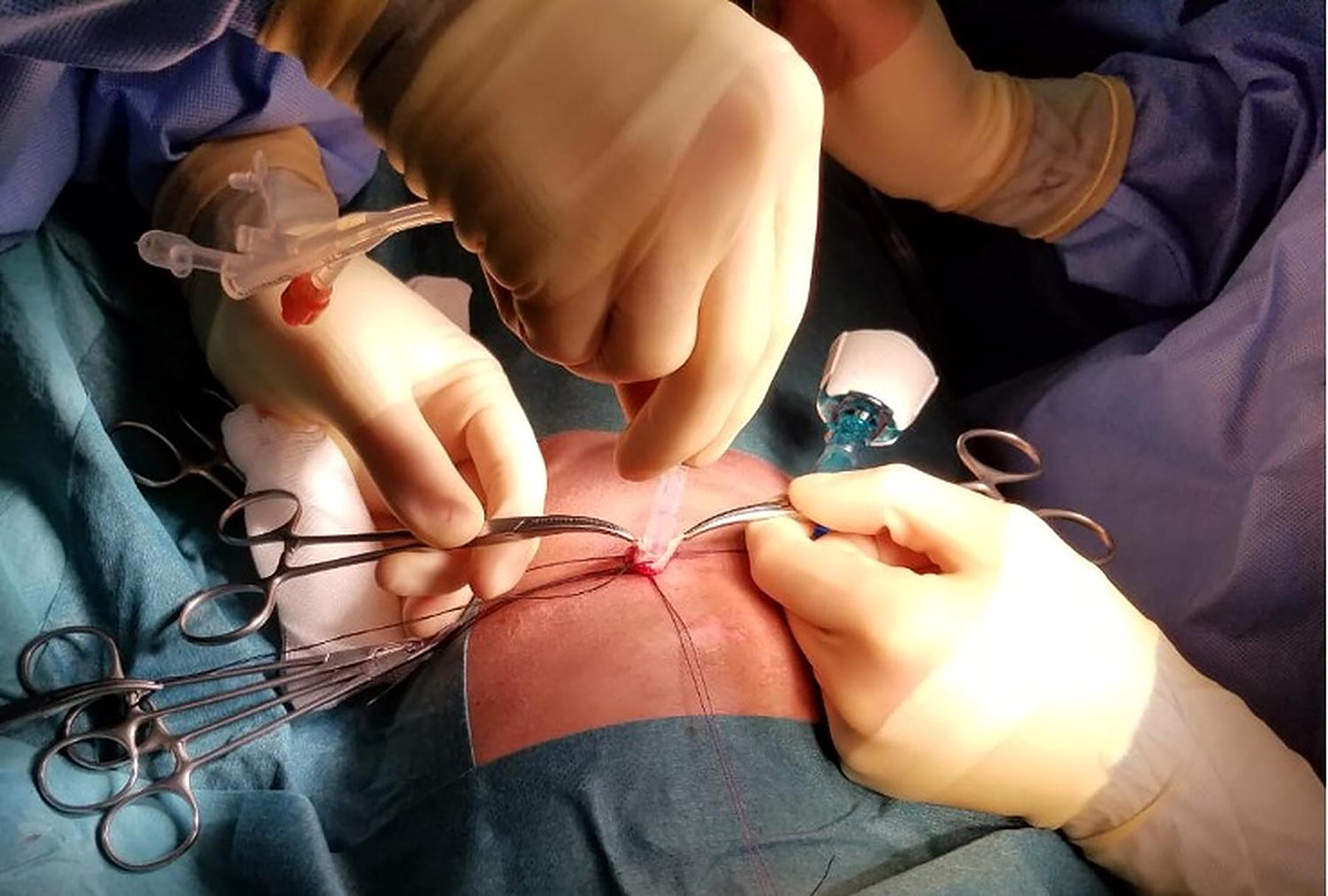
Insertion of the gastrostomy tube of the appropriate caliber through the prepared gastrotomy site.
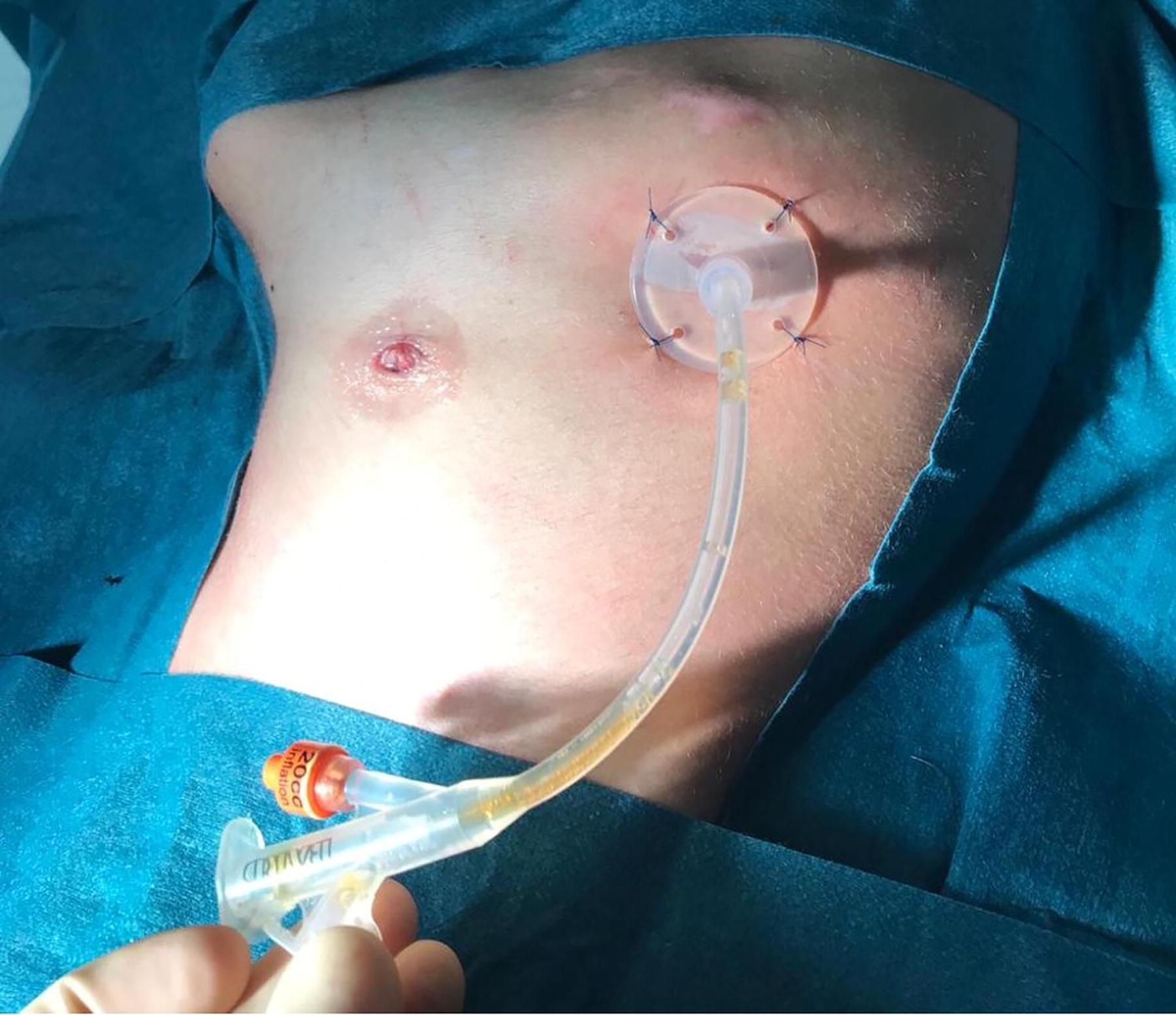
Final view following the placement of additional fascial sutures securing the stomach to the abdominal wall, demonstrating the completed laparoscopic gastrostomy setup.
Although LG placement offers several advantages, including reduced invasiveness, shorter recovery time, and improved visualization, it is important to acknowledge potential drawbacks. These may include technical challenges in patients with extensive intra-abdominal adhesions and the need for general anesthesia. Nevertheless, compared to PEG, LG is associated with fewer major complications, a lower rate of tube dislodgement, and avoids the need for a second procedure under general anesthesia to exchange the initial tube for a button. 5 Additionally, LG may contribute to an overall improvement in quality of life for patients and caregivers by providing a more durable and secure feeding route. 5
In this case series, we report our experience with 25 pediatric patients who underwent LG tube placement using this standardized method. We analyze intraoperative and postoperative outcomes, emphasizing complication rates and recovery, with the goal of supporting broader adoption of this technique in pediatric surgical practice.
Objective and Hypothesis
The objective of this study is to evaluate the clinical outcomes of pediatric patients who underwent minimally invasive LG tube placement and to provide a detailed description of the surgical technique adopted at our center. We hypothesize that LG tube placement is a safe and effective minimally invasive approach that facilitates rapid postoperative recovery, allows for same-day initiation of enteral feeding, and is associated with a low rate of complications.
Patients and Methods
This retrospective case series was approved by the Institutional Review Board of the American University of Beirut (Protocol number: BIO-2020-0345). Oral consent was obtained from the patients’ guardians prior to the procedure. A total of 25 pediatric patients, ranging in age from 7 months to 17 years, underwent LG tube placement at our tertiary care center between August 2017 and September 2022. All procedures were performed using a standardized minimally invasive “keyhole” technique. Patients included in this study were those who required GT placement for long-term enteral nutrition due to various underlying medical conditions. Exclusion criteria consisted of patients who underwent open surgical gastrostomy or PEG. Data on patient demographics, indications for gastrostomy, intraoperative findings, postoperative complications, and recovery outcomes were collected and analyzed.
Statistical analysis
Clinical and demographic data were retrospectively collected from the medical records of pediatric patients who underwent LG tube placement. Due to the retrospective design, no formal sample size calculation was performed. All analyses were conducted using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA).
Continuous variables were assessed for normality. Since the data were not normally distributed, results are reported as medians with corresponding ranges, in addition to means ± standard deviations (SD) where appropriate. Categorical variables are expressed as frequencies and percentages, and comparisons between groups were performed using the chi-square test or Fisher’s exact test, as applicable.
To assess the impact of neurological impairment on surgical outcomes, the Mann–Whitney U test was used to compare operative time and time to first feed between patients with and without neurological impairment. A P value <.05 was considered statistically significant for all applied tests.
Results
Between August 2017 and September 2022, a total of 25 LG tube placements were performed at our institution. Among the 25 patients, 14 (56%) were female, and 11 (44%) were male (Table 1). The primary indication for gastrostomy placement was feeding difficulties, accounting for 22 cases (88%), while other indications included malignancies (4%) and propionic acidemia (4%). Neurological impairment was present in 19 patients (76%). Additionally, 10 patients (40%) had undergone a tracheostomy procedure and were capable of oral feeding (Table 1).
Baseline Clinical Characteristics of the Study Population
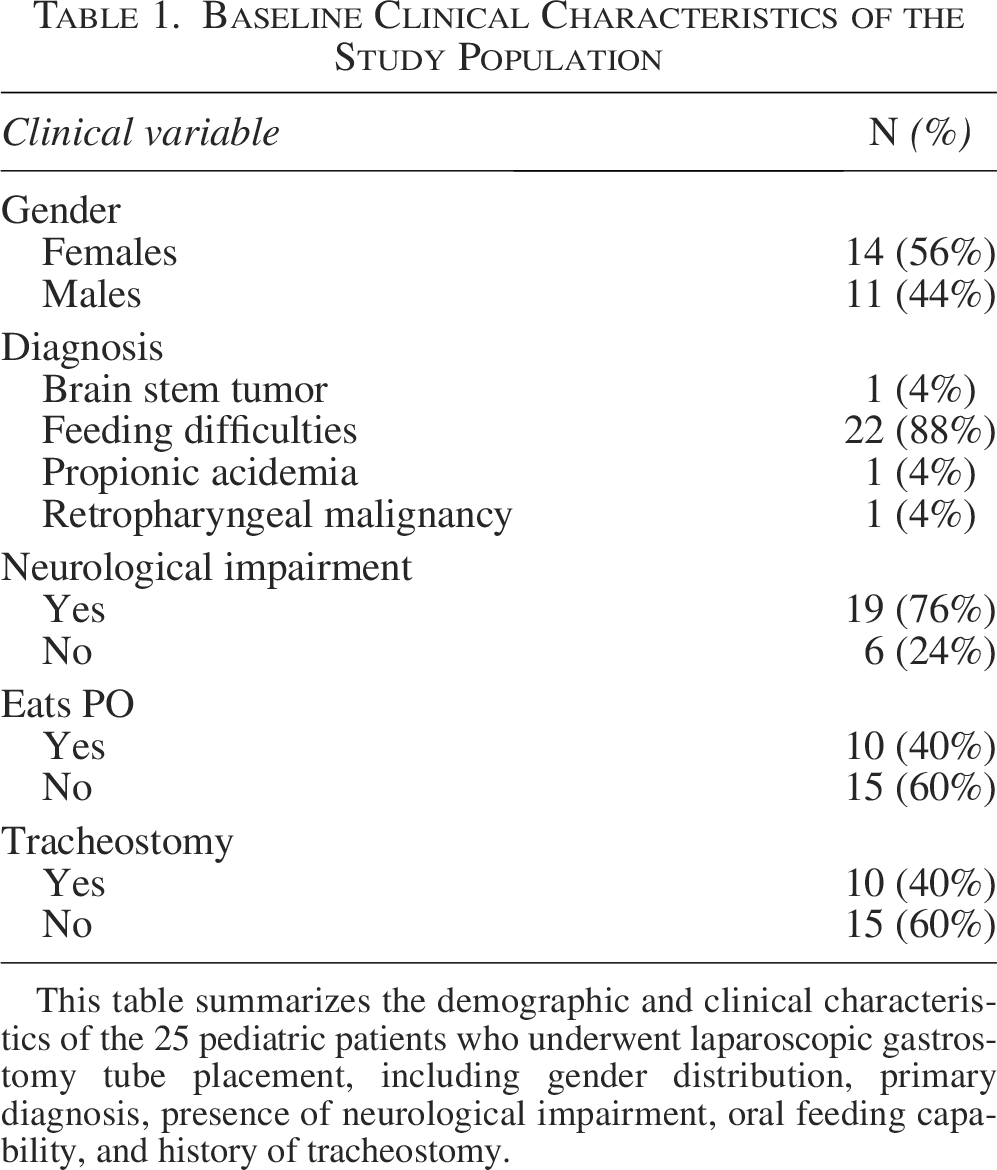
This table summarizes the demographic and clinical characteristics of the 25 pediatric patients who underwent laparoscopic gastrostomy tube placement, including gender distribution, primary diagnosis, presence of neurological impairment, oral feeding capability, and history of tracheostomy.
This table summarizes the demographic and clinical characteristics of the 25 pediatric patients who underwent LG tube placement, including gender distribution, primary diagnosis, presence of neurological impairment, oral feeding capability, and history of tracheostomy.
Regarding surgical outcomes, no patients experienced intraoperative or postoperative complications. There were no cases requiring conversion to an open procedure, no aborted surgeries, and no need for postoperative anti-reflux surgery. Importantly, no cases of tube dislodgement were observed prior to the first tube change or within the initial 30-day postoperative period.
The patients’ ages ranged from 7 months to 17 years (204 months), with a median age of 48 months (4 years) and a mean of 7.1 years at the time of gastrostomy placement. The median weight at the time of surgery was 13 kg, ranging from 4.5 kg to 66 kg. The median operative time was 71 minutes, and the median length of hospital stay was 4 day (Table 2).
Surgical Outcomes and Baseline Laboratory Parameters
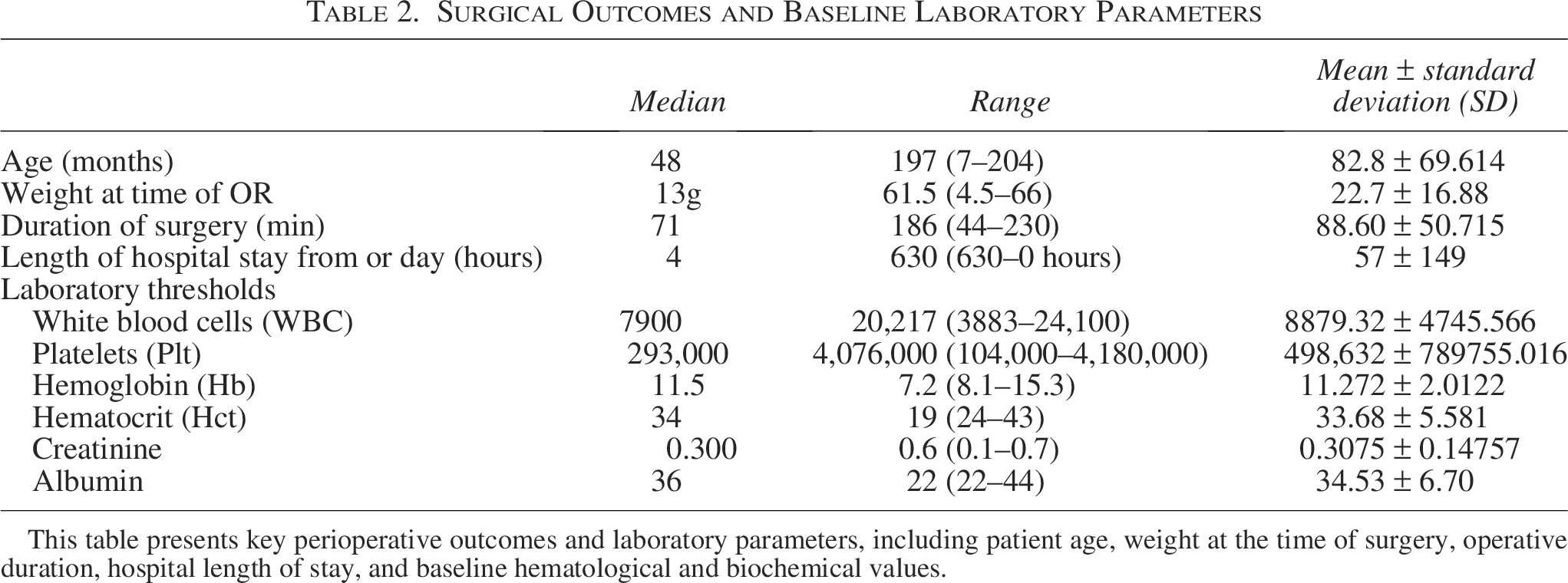
This table presents key perioperative outcomes and laboratory parameters, including patient age, weight at the time of surgery, operative duration, hospital length of stay, and baseline hematological and biochemical values.
This table presents key perioperative outcomes and laboratory parameters, including patient age, weight at the time of surgery, operative duration, hospital length of stay, and baseline hematological and biochemical values.
Baseline laboratory values showed a median white blood cell count of 7900/μL, platelet count of 293,000/μL, hemoglobin level of 11.5 g/dL, and hematocrit of 34%. Additionally, median creatinine and albumin levels were 0.3 mg/dL and 36 g/L, respectively. The full range, mean, and SD of these parameters are detailed in Table 2.
Spearman’s correlation analysis (Table 3) revealed non-significant negative associations between age at the time of surgery and time to first feed (ρ = –.165, P = .441), as well as between weight at the time of surgery and time to first feed (ρ = –.156, P = .468). These findings suggest that neither patient age nor weight had a statistically significant influence on the timing of postoperative enteral feeding initiation.
Spearman Non-Parametric Correlation
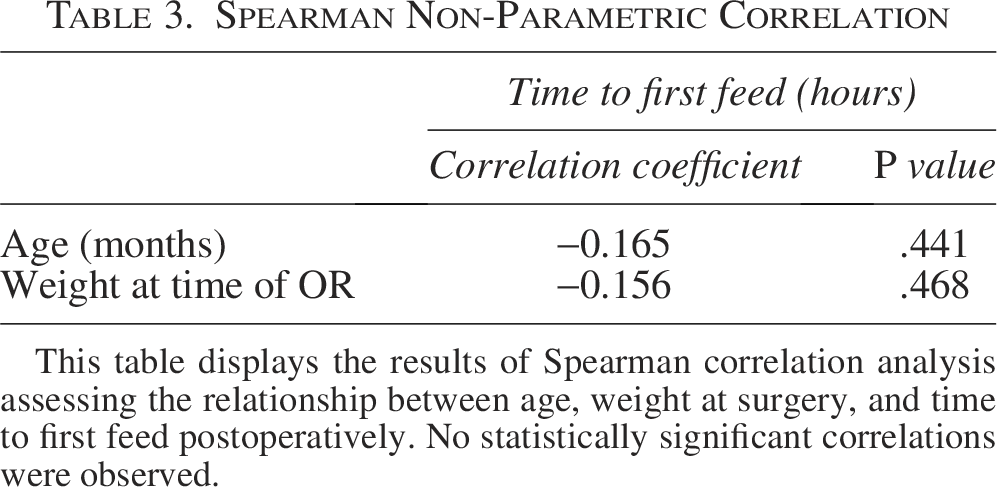
This table displays the results of Spearman correlation analysis assessing the relationship between age, weight at surgery, and time to first feed postoperatively. No statistically significant correlations were observed.
Mann–Whitney U test analysis (Table 4) demonstrated that operative time did not significantly differ between patients with neurological impairment (n = 19, mean rank = 14.42) and those without impairment (n = 6, mean rank = 8.50; U = 30.000, P = .086). Similarly, the time to first feed was not significantly different between neurologically impaired patients (n = 18, mean rank = 12.06) and those without impairment (n = 6, mean rank = 13.83; U = 46.000, P = .568).
Mann–Whitney Test
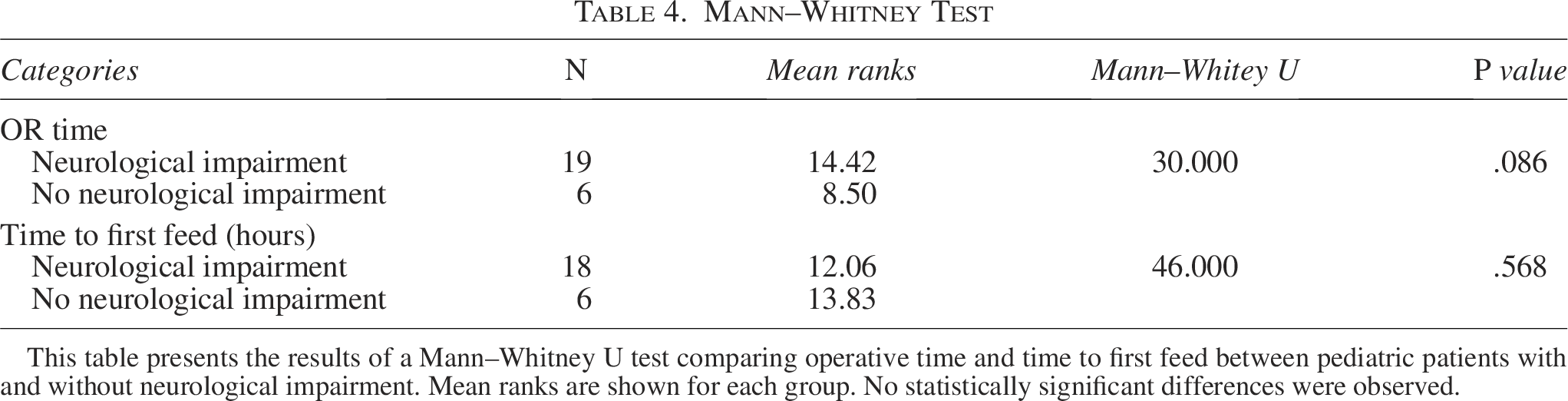
This table presents the results of a Mann–Whitney U test comparing operative time and time to first feed between pediatric patients with and without neurological impairment. Mean ranks are shown for each group. No statistically significant differences were observed.
Discussion
LG tube placement was first described by Georgeson in 1993 and has since evolved into a widely accepted technique with favorable recovery outcomes. As surgical approaches continue to advance, efforts have focused on identifying the safest and most effective method to ensure optimal nutritional support and improve quality of life in pediatric patients.
The laparoscopic approach has gained prominence due to its enhanced visualization of the peritoneal cavity and safer placement of the GT, particularly in children with small or distorted abdominal anatomies—such as those with spinal anomalies or hepatomegaly. 6 This visualization reduces the risk of intra-abdominal injury and facilitates precise tube placement. However, laparoscopic surgery may be less favorable for patients with respiratory compromise or significant intra-abdominal adhesions due to prior surgeries. 7
A commonly cited drawback of LG is the longer operative and anesthesia time compared to PEG. Nevertheless, the laparoscopic approach is associated with fewer major complications, reduced tube dislodgement, and the elimination of the need for a second procedure to replace the initial tube with a button device. 10 This can be especially beneficial in medically complex or high-risk pediatric patients.
Several laparoscopic techniques have been described, including the mini-open, Seldinger, and modified Seldinger approaches. The MOT uses a Stamm-like method with fascial sutures to anchor the stomach, while the Seldinger approach employs external suspension sutures and guidewire dilation. The modified Seldinger technique retains sutures subcutaneously for ongoing fixation. 10 Another approach, LAPEG, combines endoscopy and laparoscopy and uses T-fasteners for stomach fixation, although these may migrate or lead to complications if not properly expelled postoperatively.11,12
Comparative studies have examined laparoscopic versus PEG gastrostomy placement. One systematic review found similar complication rates between the two approaches, with time to first feed ranging between 0.7 and 0.8 days. 13 However, PEG is associated with a higher risk of bowel injury and early tube dislodgement, particularly when anatomical landmarks are unclear. In contrast, LG demonstrated a lower rate of major complications (1% versus 5.4%) and avoided unrecognized injuries. 7 In our series, no patient experienced a procedural complication, supporting the safety profile of our approach.
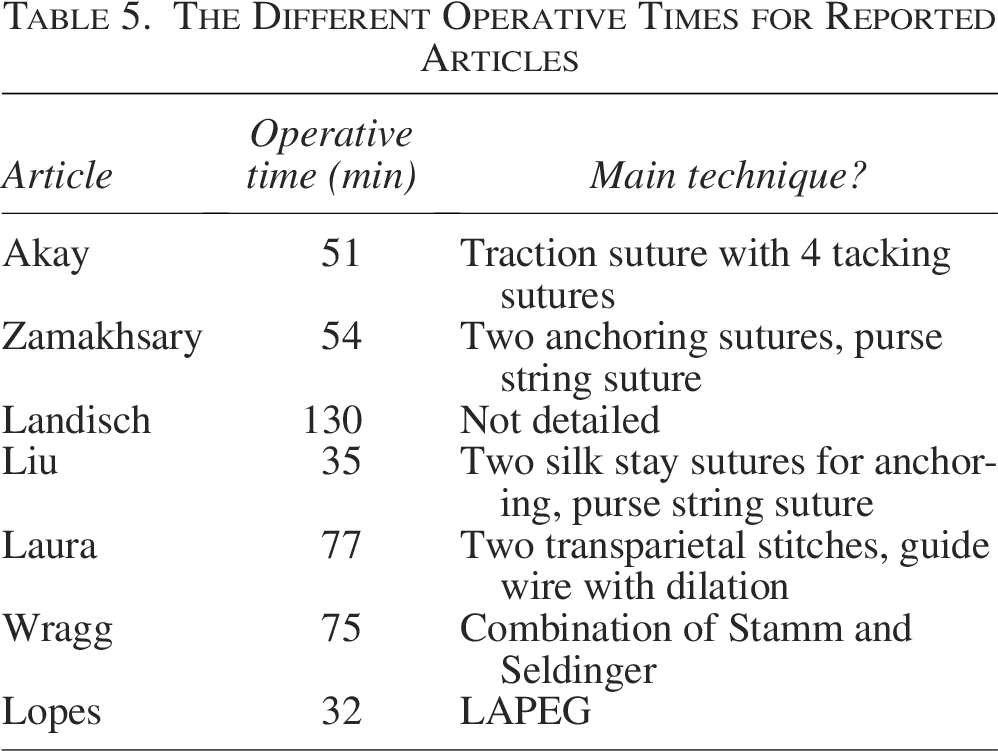
Operative time is a key metric in evaluating technique efficiency. Our reported median operative time was 71 minutes, which is longer than that reported in several other studies. For instance, Akay et al. (2010) reported a mean operative time of 51 minutes using a traction and tacking suture method, 8 while Zamakhsary et al. (2005) achieved 54 minutes using a technique similar to ours. 14 The extended duration in our series is likely attributable to the added steps of placing a figure-of-eight suture and four fascial sutures, which we believe enhance gastropexy integrity and reduce tube dislodgement.
Additional support for the robustness of our findings is provided by the Mann–Whitney U analysis. Although patients with neurological impairment tended to have longer operative times and delayed initiation of feeding, these differences did not reach statistical significance (P = .086 and P = .568, respectively). This suggests that our standardized approach performs consistently across different patient subgroups, including those with neurological comorbidities.
Other studies have reported comparable operative times and feeding outcomes. Laura et al. (2016) utilized a guidewire and dilator technique with a mean operative time of 77 minutes and a median time to first feed ofpexy 1.7 ± 0.9 days, 15 closely matching our data. Kyle et al. (2022) also reported a mean operative time of 85 minutes using the modified Seldinger technique, 16 while Bitar et al. achieved faster times with fewer suturing steps.
When compared to literature-reported techniques (Table 5), our method falls on the higher end of the operative time spectrum. However, this trade-off is balanced by reduced procedural risk, elimination of the need for a second surgery, and high tube security. The use of a primary GT rather than an interim button also simplifies follow-up and reduces procedural burden for both the patient and caregiver. Moreover, Our reported operative time was longer than that of several comparable series. Two factors may explain this difference. First, our recorded duration included anesthesia induction and patient positioning in addition to the operative steps, which inherently prolongs the total time. Second, all procedures were performed at an academic tertiary-care center where residents carried out the surgeries under direct supervision of attending pediatric surgeons. The teaching environment, while essential for training the next generation of surgeons, inevitably lengthens operative times. Despite these considerations, the operative duration remained within a safe range and did not adversely affect postoperative recovery or complication rates.
The Different Operative Times for Reported Articles
As for the learning curve, although we did not formally evaluate it in this study, our institutional experience suggests that the technique is highly reproducible and easy to teach. Most surgical trainees are able to perform the procedure independently after 2–3 supervised cases. The simplicity of the operative steps, along with minimal dissection and clear anatomical landmarks, contributes to its accessibility. Additionally, the technique is well-suited for use in resource-limited settings, as it does not require advanced laparoscopic equipment, energy devices, or specialized instruments. This makes it a practical and cost-effective option for centers with limited surgical resources.
Study limitations
This study has several limitations that should be acknowledged. It is a retrospective analysis conducted at a single tertiary care center with a relatively small sample size, which may restrict the statistical power and limit the generalizability of the findings. Furthermore, the absence of a comparator group, such as patients undergoing PEG or open gastrostomy, precludes direct comparison of outcomes across different techniques. Although appropriate statistical methods were applied, the retrospective nature of the study and the small cohort size reduce the ability to detect meaningful differences between subgroups. Consequently, the absence of statistically significant associations should be interpreted with caution, as the study may have been underpowered to identify subtle but clinically relevant effects. Future research should focus on prospective, multicenter studies with larger cohorts and control groups to validate our findings and better define the relative advantages of the laparoscopic approach.
Conclusion
This case series highlights the safety, feasibility, and clinical effectiveness of our standardized LG tube placement technique in a pediatric population. Despite a slightly longer operative time compared to other reported methods, the approach demonstrated a low complication rate, reliable tube fixation, and facilitated timely initiation of enteral feeding. Notably, outcomes remained consistent across patient subgroups, including those with neurological impairment. Our findings support the broader adoption of this reproducible technique as a durable and minimally invasive alternative to open or PEG gastrostomy, with the potential to enhance patient care and reduce the need for additional interventions.
Despite the limitations of sample size and the longer operative times observed, our findings demonstrate that LG tube placement using this standardized technique is safe, reproducible, and associated with low complication rates. The approach is particularly well suited to academic and resource-limited settings, where operative efficiency must be balanced with safety and training needs. These results support the broader adoption of a structured laparoscopic technique for pediatric gastrostomy in diverse clinical environments.
Authors’ Contributions
B.H.: Conceptualization, methodology, investigation, writing—original draft. H.F.: Data curation, writing, visualization, review and editing. M.N.: Data curation, writing, visualization, review and editing. J.H.: Formal analysis. H.A.T.: Writing—review and editing. M.E.E.: Supervision, validation, writing—review and editing. A.Z.: Conceptualization, methodology, supervision, writing—review and editing, corresponding author.
Footnotes
Acknowledgments
The authors would like to thank the Department of Surgery at the American University of Beirut Medical Center for their support throughout the study. We also express our gratitude to the nursing and operating room staff for their assistance in patient care and data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.